
Clinical observation of sinew-regulating and bone-setting manipulation combined with functional exercise to treat rotator cuff injury
2018-10-22 10:31:24ZhangWendi張文娣ChenZhaohui陳朝暉WangBo王波YaoMengli姚夢莉XuHan徐寒
Zhang Wen-di (張文娣), Chen Zhao-hui (陳朝暉), Wang Bo (王波), Yao Meng-li (姚夢莉), Xu Han (徐寒)
1 Graduate School, Anhui University of Chinese Medicine, Hefei 230038, China
2 College of Acupuncture and Massage, Anhui University of Chinese Medicine, Hefei 230038, China
Abstract
Keywords: Tuina; Massage; Exercise; Range of Motion, Articular; Rotator Cuff Injuries; Shoulder Pain
The rotator cuff injury (RCI) is a common shoulder soft tissue lesion caused by degenerative changes,insufficient blood supply, subacromial impact and/or trauma[1].Its prevalence increases with age[2].The incidence of RCI has risen significantly among people over 40, especially in people with shoulder injury,sprains, and do beating exercise such as badminton,swimming, and throwing, the incidence of RCI has remained high[3].The shoulder pain aggravates when the shoulder is flexed, abducted or extended on the internal rotation.The shoulder joint movement is limited and even leads to atrophy, which seriously affects the quality of life of patients.RCI is currently treated with conservative methods.In recent years, the author has followed his tutor and used sinew-regulating and bone-setting manipulation combined with functional exercise to treat RCI.The report is as follows.
1 Clinical Information
1.1 Diagnostic criteria
With reference to theCriteria of Diagnosis and Therapeutic Effects of Diseases and Syndromes in Traditional Chinese Medicine[4]andMuscle Injury Science of Traditional Chinese Medicine[5], the diagnostic criteria are as follows.
Clinical manifestations: a history of acute trauma,chronic cumulative strain or cold; shoulder pain,especially front shoulder pain aggravated during movement and at night; tenderness in the proximal great tubercles of humerus or subacromial space;motor dysfunction, generally abduction, flexion,external and internal rotation limited.
Positive signs: positive test of supraspinatus tendon rupture, positive Hawkins test, and positive pain arc test[6].
The presence of the above clinical features with any of the above positive signs should consider the possibility of RCI, shoulder joint MRI can confirm RCI diagnosis.
1.2 Inclusion criteria
In accordance with the above diagnostic criteria; age 18 to 60 years old; MRI examination of the shoulder joint revealed clear RCI, and Neer grading was below Grade 2; the patient did not receive surgery and other conservative treatment in the last month; it was better recognized in this study.Knowledge and degree of cooperation; signed informed consent.
1.3 Exclusion criteria
Patients with limited shoulder activity and muscle weakness due to central or peripheral nerve injury;those with shoulder fractures, dislocations, or surgical history; those with neck symptoms and positive signs;shoulder MRI indications of injury at level 2 and above according to Neer grading.
1.4 Statistical method
The SPSS version 23.0 statistical software was used for statistical analysis.All data were tested with a normal distribution.Measured data that line with normal distribution were expressed as mean ± standard deviation () and thet-test was used; data that did not meet the normal distribution were tested by rank sum test.Count data were analyzed using Chi-square test.α=0.05 was taken as the test level,P<0.05 indicated a statistical significance.
1.5 General information
All 40 patients were enrolled from the tendon injury clinic of the First Affiliated Hospital of Anhui University of Traditional Chinese Medicine and the Outpatient Department of the Guoyitang of Anhui University of Chinese Medicine.According to a random excel table,40 patients were divided into a treatment group and a control group, with 20 cases in each group.The age range of treatment group was 18 to 55 years old and the disease duration was 1 to 18 months.The age range of control group was 18 to 60 years old and the disease duration 1 to 17 months.Both groups of patients completed the relevant treatment and no dropout.There was no statistical difference in the general data between the two groups (allP>0.05), indicating that the two groups were comparable (Table 1).

Table 1.Comparison of general information
2 Methods
2.1 Treatment group
2.1.1 Sinew-regulating and bone-setting manipulation combined with functional exercise[7]
Sinew-regulating manipulation: First, applied Diandigital pressing, Rou-kneading and Nian-twisting, and Gun-rolling manipulations to release the affected area(Figure 1-Figure 3).For patients with a long duration,manipulations for unblocking should be applied to the funicular or pain points that appeared at the corresponding muscle regions on the shoulder, such as Hand Taiyin, Hand Shaoyin, Hand Yangming and Hand Taiyang.Ten to fifteen minutes manipulation with moderate force will achieve the effect of antispasmodic pain and regulating sinew and blood.
Bone-setting manipulation: First, adjusting the scapula method was used, that is, the doctor stood on the patient’s shoulder side, put one hand in front of the shoulder and the other hand on the lower corner of the scapula.The two hands oppositely shook the shoulder and thorax joints several times, and then stretched the shoulder and thorax joints to correct the position of the scapula (Figure 4).
Then used the swinging shoulder method, that is, the doctor stood behind the affected shoulder of the patient, held the wrist with one hand, placed the thumb and forefinger on the shoulder, and Yao-rocked the patient’s upper limb with the shoulder as the pivot to loosen adhesions and increase joint mobility.The amplitude was from small to large and the speed should be slow to lubricate the joint (Figure 5).Finally,used the shoulder lifting method, that is, the doctor stood on the affected side of the patient, held the patient's wrist with both hands, and gently lifted it upwards so as not to cause pain (Figure 6).It took 5-10 min.
The above treatments were performed once every other day and 7 times as a course of treatment for a total of two courses.
Finishing manipulation: Finally, the patient's shoulder was naturally sagging, and the doctor used Dou-shaking and Lü-twisting manipulations to further relax the shoulder (Figures 7 and Figure 8), for 2-3 min.
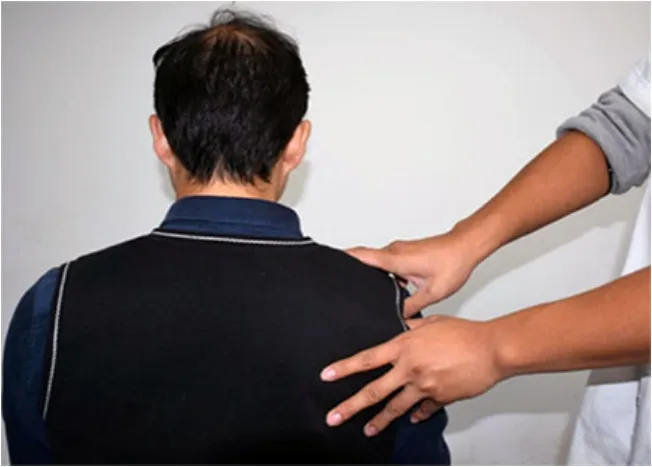
Figure 1.Dian-digital pressing

Figure 2.Rou-kneading and Nian-twisting

Figure 3.Gun-rolling

Figure 4.Adjusting the scapula

Figure 5.Yao-rocking the shoulder

Figure 6.Lifting the shoulder

Figure 7.Dou-shaking

Figure 8.Lü-twisting
2.1.2 Functional exercise[8]
Functional exercise played an extremely important role in the rehabilitation of RCI.We refer to the research of Escamilla RF,et al[9]and divide the RCI functional exercise into four phases: acute phase, joint activity phase, strength training phase, and functional training phase.
Acute phase: The aim of this phase is to avoid pain at the injury site and promote absorption of inflammation.The patient was told to avoid the cold and keep warm of the affected shoulders.Use triangles to suspend and protect the shoulder from excessive lifting and other painful postures.This period allows the patient to strengthen the hand, wrist and elbow training, such as empty hand fist training (Figure 9), wrist and elbow flexion and extension active training and resistance training (Figure 10-Figure 13).The joint activities and strength exercises at the distal extremities prevent muscle atrophy and soft tissue adhesion, promote blood and lymph flow in the upper extremities, and reduce swelling and pain.Each exercise set is 15 to 20 times, three sets a time, 2 to 3 times a day.
Joint activity phase: In this period, the inflammation of the patient gradually subsides and the pain is relieved.The purpose of the exercise is to maintain and expand the range of shoulder activities and prevent the occurrence of soft tissue adhesion around the joints.Instruct patients to use sandbags or dumbbells to perform pendulous swaying within the painless range of shoulder joints, and gradually increase the range of motion, including shoulder flexion, adduction,extension and rotation (Figure 14-Figure 17).The sandbag weighs 1 kg and dumbbell 1 kg (Hangzhou Sanhuan Sporting Goods Co., China).Instruct patients to conduct isometric contraction exercises at different angles in different directions, and each contraction was maintained for 10 s.Patients were asked to actively exercise the scapula elevation, depression, adduction,and rotation (Figure 18-Figure 21).Each exercise the above trainings contained 3 groups, 15-20 times in each group, and 2 to 3 exercises are performed daily.After each training, ice compress was used for 15-20 min to relieve pain.

Figure 9.Empty hand fist training

Figure 10.Waist flexion resistance training

Figure 11.Waist extension resistance training
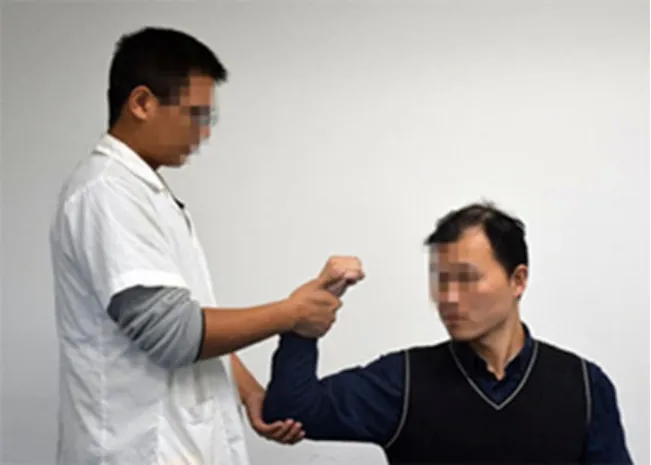
Figure 12.Elbow flexion resistance training

Figure 13.Elbow extension resistance training

Figure 14.Shoulder forward flexion

Figure 15.Shoulder backward extension

Figure 16.Shoulder adduction

Figure 17.Shoulder abduction

Figure 18.Scalupa elevation
Strength training phase: The purpose of this period of exercise is to enhance the muscle strength around the shoulder, including muscle strength and muscular endurance training.Using an elastic band, one end is fixed and the other end is tied to the patient's forearm.The shoulder joint resists to confrontation to complete shoulder flexion, abduction, adduction, internal rotation,and external rotation (Figure 22-Figure 27).

Figure 19.Scapula depression

Figure 20.Scapula adduction

Figure 21.Scapula abduction

Figure 22.Shoulder resists to flexion

Figure 23.Shoulder resists to extension

Figure 24.Shoulder resists to adduction
In addition, the scapula must be trained for exercise control and stability, and the closed-chain training of the scapula can be performed at the bedside (Figure 28).The shoulder flexion angle can be adjusted to avoid shoulder pain.The elastic ball can be used instead of the fixed support surface to increase the training difficulty.Muscle strength training should be high repetition, low load in a gradual progress, and the muscle does not feel fatigue for the next day.Each action exercise contains three groups, 15 to 20 times in each group, and practice 2 to 3 exercise a day.The elastic band is 1.5 m long, about 8 kg weight (Aoyang Flagship Store, China).
Functional training phase: The purpose of this period of exercise is to provide special exercise posture guidance for sports-induced RCI patients, including shoulder flexibility and coordination training during exercise, proprioceptive training and posture correction.
The above functional exercises were all performed after the treatment of sinew-regulating and bonesetting manipulation.
2.2 Control group
The patients in the control group received the same treatment as the treatment group.The time and course of treatment were the same as those in the treatment group.However, functional exercises are not performed.

Figure 25.Shoulder resists to abduction

Figure 26.Shoulder resists to internal rotation

Figure 27.Shoulder resists to external rotation

Figure 28.Scapula closed-chain movement
3 Results
3.1 Observational items
3.1.1 Pain/tenderness
Wagner Force TenTM-Model FDX digital dynamometer manufactured by WAGNER Company was used to measure the tenderness value of the patient's self-reported most painful point.The measurement was performed three times and averaged.
3.1.2 Shoulder motion
Angle rulers were used to measure the joint angels of flexion, abduction, internal rotation and external rotation of patients before and after treatment.
The patient was seated.The center of the ruler was located on the acromion of the humerus, the fixed arm was parallel to the trunk, and the moving arm was parallel to the humerus.The angle of the shoulder flexion was measured, normally between 0-180°.The patient took a seat, the center of the ruler was located at the back of the acromion, the fixed arm was parallel to the trunk, the moving arm was parallel to the humerus, and the angle of the shoulder abduction was measured, normally between 0-180°.The patient was seated, the shoulder extended 90°, elbow flexion 90°,forearm pronation, the center of the ruler was located on the olecranon, the fixed arm was parallel to the ground, the moving arm was parallel to the forearm,and the angles of internal rotation (normally 0-70°) and external rotation (normally 0-90°) were measured.
3.1.3 University of California at Los Angeles (UCLA)shoulder rating score
The UCLA shoulder rating score was adopted to evaluate the patient's pain, function, forward flexion activity, forward flexion strength, and patient satisfaction before and after treatment.The total score was 35 points, excellent: 34-35 points; good: 29-33 points; bad: less than 29 points.
3.2 Efficacy evaluation criteria
Refer toCriteria of Diagnosis and Therapeutic Effects of Diseases and Syndromes in Traditional Chinese Medicineas the standard for efficacy[4].
Cure: Shoulder pain disappears and function returns to normal.
Improvement: Shoulder pain is relieved and the function returns to normal, but pain may still occur after fatigue, cold or dampness attacks.
Failure: No improvement in shoulder symptoms.
3.3 Results
3.3.1 Efficacy comparison
After treatment, the total effective rate was 95.0% in the treatment group and 65.0% in the control group(P<0.05), (Table 2).

Table 2.Efficacy comparison (case)
3.3.2 Comparison of tenderness degree
There was no significant difference in tenderness degree between the two groups before treatment(P>0.05).After treatment, there was statistically significant intra-group differences (bothP<0.05).The between-group difference was also statistically significant (P<0.05), showing that the treatment group had better efficacy in improving tenderness degree than the control group (Table 3).
Table 3.Comparison of tenderness (, kg)
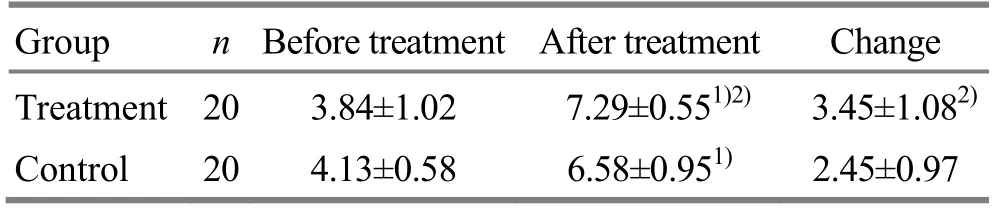
Table 3.Comparison of tenderness (, kg)
Note: Intra-group comparison, 1) P<0.05; compared with the control group, 2) P<0.05
Group n Before treatment After treatment Change Treatment 20 3.84±1.02 7.29±0.551)2) 3.45±1.082)Control 20 4.13±0.58 6.58±0.951) 2.45±0.97
3.3.3 Shoulder motion comparison
There was no significant difference in shoulder motion between the two groups before treatment(P>0.05).After treatment, the flexion, abduction,internal rotation and external rotation of the shoulder joints were significantly improved than those before the treatment (allP<0.05), and the improvement in treatment group was better than in the control group(allP<0.05), (Table 4).
Table 4.Shoulder motion comparison (, °)

Table 4.Shoulder motion comparison (, °)
Note: Intra-group comparison, 1) P<0.05; compared with the control group, 2) P<0.05
Group n Time Flexion Abduction Internal rotation External rotation Treatment 20 Before treatment 55.35±9.84 122.70±9.02 18.80±8.42 30.55±4.93 After treatment 131.55±12.571)2) 61.75±7.981)2) 58.45±8.961)2) 75.65±8.081)2)Control 20 Before treatment 53.10±8.70 57.80±5.70 17.80±8.83 28.05±6.58 After treatment 97.25±13.221) 94.10±8.901) 47.8±6.921) 69.15±5.141)
3.3.4 UCLA shoulder rating score
There was no significant difference in the UCLA shoulder rating score between the two groups before treatment (P>0.05).After treatment, the UCLA shoulder rating scores were significantly improved in both groups(P<0.05) compared with before treatment, and the improvement of the treatment group was better than that of the control group (P<0.05), (Table 5).
Table 5.UCLA shoulder rating score (, point)
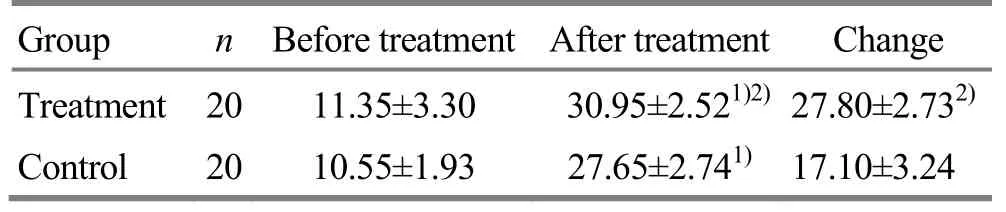
Table 5.UCLA shoulder rating score (, point)
Note: Intra-group comparison, 1) P<0.05; compared with the control group, 2) P<0.05
Group n Before treatment After treatment Change Treatment 20 11.35±3.30 30.95±2.521)2) 27.80±2.732)Control 20 10.55±1.93 27.65±2.741) 17.10±3.24
4 Discussion
RCI is an important cause of shoulder pain and dysfunction, accounting for about 17% to 41% of shoulder disease[10].The patient showed different degrees of pain under the acromion or around major nodules, aggravated when raising the arm or in a lying position on the affected side, and some patients are even awakened at night, the shoulder activity is severely limited.Patients with a course of more than 3 weeks could have muscle atrophy and the supraspinatus is the most severe.Because symptoms and signs are similar to those of scapulohumeral periarthritis, many RCI patients are clinically misdiagnosed and undergo a lot of shoulder joint activity in the early stages, resulting in worsened rotator cuff tears.The important identification point of rotator cuff tear and periarthritis is that the active joint activity of the former is limited but the passive joint activity is basically normal, while the latter has both active and passive activities limitation due to adhesion inside and outside the joint[11]; The range of pain and movement restriction are broader than the former, and most studies have shown that there is a clear correlation between periarthritis and diabetes[12].With the development of magnetic resonance, ultrasound and other imaging technologies, the position and degree of RCI can be clearly defined.Arthroscopy is often used as a ‘gold standard’ in the diagnosis of shoulder diseases as well as rotator cuff muscle injury[13].Therefore, when a patient develops symptoms of the shoulder joint, clear diagnosis should be made before treatment and functional exercise.
Studies have shown that RCI is closely related to scapular motility disorders, which refers to scapula malpositioning and movement disorders, and can be either the cause of RCI, or a compensatory change in the course of disease development[14].Excessive external rotation of the scapula causes a decrease in the strength of the rotator cuff muscles, increasing the chance of impact and injury to the rotator cuff[15-16].Kibler WB,et al[17]classified the abnormalities of the scapula position and movement into four types.Type I was the dorsiflexion of the scapular angle; Type II was the dorsiflexion of the medial scapula; the type III was the excessive elevation of the upper scapula; type IV is normal and the scapulas are relatively symmetrical.The normal scapular plane is about 30-45°.In clinical practice, we observed that due to prolonged posture during work and life, most patients suffer from an increase in angle of the scapular plane, an internal rotation of the scapula, and an inward dorsum of the shoulder blades.During the shoulder elevating process,the scapula was prematurely rotated.From the perspective of dynamics, RCI patients with scapular motility disorders often have weak serratus muscle strength, levator scapula, pectoralis minor muscle contraction and hypertonia, and excessive activation or premature activation of upper trapezius muscle,insufficient or late activation of trapezius muscle[18].Deng SM,et al[19]also pointed out that the imbalance between the mid-lower trapezius muscles, the subscapular and great round muscles is an important cause of type II scapula position and movement abnormalities.Therefore, in clinical practice, besides sinew-regulating manipulation, we emphasize the adjustment of the scapula position by means of the dynamic movement, and the correction of scapular strength and coordination disorders by means of the muscular force exercise of the scapular muscle to restore normal glenohumeral joint rhythm.In addition,proper neck and shoulder posture correction can restore its normal anatomical position, and fundamentally reduce the chance of shoulder impact and injury[20].
RCI is in the category of ‘tendon injuries’ in Chinese medicine and is also known as ‘upper arm joint tendon injury’.The soft tissues/tendons of the human body are attached to the bones.The main function of the tendon is to connect the joints and limbs to conduct joint movements.There is a close relationship between bones and tendons, long-term tendon injury will inevitably lead to the occurrence of bone staggered joints, that is, ‘the simultaneous tendon and bone disease’, so in the treatment, we should emphasize‘focus and treat the tendons and bones at the same time’[21].Local manipulations Dian-digital pressing,Rou-kneading and Nian-twisting, and Gun-rolling were performed to loosen the tendons knotting and pain points of the affected shoulder, to relieve pain and dredge the meridians.From syndrome differentiation perspectives of traditional Chinese medicine, the upper limbs of the Hand Yangming, the Hand Taiyang, the Hand Taiyin and the Hand Shaoyin Meridians are often affected in patients with long-term RCI, so the relaxing manipulation on the corresponding areas often gets satisfactory efficacy.The Hand Taiyin muscle region routine is equivalent to the muscle fascia chain formed by the large squid muscles, diaphragm, biceps long head, deltoid anterior and pectoralis major muscles in modern anatomy; The Hand Shaoyin muscle region routine is equivalent to the muscle fascia chain of the superficial flexor muscle, the biceps short head and the pectoralis major muscle in modern anatomy; the Hand Taiyang muscle region routine is similar to the muscle fascia chain formed by the middle and small thenar muscle group, lateral ulnar suture, the medial head of the triceps, the rotator cuff muscles, the scapular levator muscle and the rhomboid muscle; the Hand Yangming muscle region routine is similar to the fascia chain of the extensor muscle of fingers, the triceps lateral head, the deltoid anterior bundle, the trapezius muscle bundle, the supraspinatus muscle and the scapular levator muscle.According to the descriptions inLing Shu(Spiritual Pivot), the muscle regions are all originated from the end of the extremities, and pressing the origin and insertion of the above muscles of the upper limbs, painful points of the radialis side of the thenar eminence and the thumb, the antithenar muscles and the little fingers, can play a good relaxation effect on the whole muscle.Local orthopedic manipulations include adjustment of the scapula method, swaying method and lifting method to restore the anatomical position of the scapula and humerus,improve the scapular rhythm, relieve soft tissue adhesion, and increase the range of shoulder movement.The characteristics of the sinew-regulating manipulation are light and gentle, because the tendon and muscles ‘prefer gentleness rather than hardness’.Therefore, the manipulation needs to be gentle,uniform and infiltrated, and finally achieve the state of‘a(chǎn)djusted bones and smoothing muscles, and qi and blood flow’.
Functional exercise combines the shoulder joint and peripheral joint assist, active and anti-resistance methods to improve the range of shoulder joint movement, muscle strength and scapular rhythm.The closed-chain exercise training in which the scapula is extended and retracted can improve the stability and coordination of the scapular chest wall joints, especially the anterior serratus function.Studies have shown that shoulder immobilization can lead to insufficient and fatigue activation of the anterior serratus muscle, which makes the scapula upturned insufficiently to advances and lifts up the humeral head, resulting in abnormal subacromial space, and it is easy to cause secondary impact under the shoulder[22-23].Therefore, the scapula closed chain movement, especially the recovery of the anterior serratus function is crucial.In addition, the closed-chain movement of the scapula can improve the proprioception of the scapula and promote better recovery of the shoulder movement[24].
This study showed that after treatment, the symptoms of the two groups were significantly improved (P<0.05), the pain was relieved, the joint mobility and stability were enhanced, and the treatment effect of the treatment group was significantly better than that of the control group(P<0.05).These results revealed that sinew-regulating and bone-setting manipulation combined with functional exercise is effective for mild to moderate RCI and can achieve the purpose of restoring shoulder function, which is worthy of clinical application.
猜你喜歡
金秋(2023年4期)2023-05-23 10:11:18
小獼猴智力畫刊(2022年11期)2022-11-28 02:49:08
Acta Mathematica Scientia(English Series)(2022年3期)2022-06-25 02:12:18
花火·繪閱讀(2021年2期)2021-09-10 07:22:44
喜劇世界(2017年5期)2017-12-06 04:28:41
男生女生(金版)(2016年3期)2017-01-17 15:23:41
小小說月刊(2016年12期)2016-12-13 17:37:57
博客天下(2016年14期)2016-09-15 13:46:42
水動力學(xué)研究與進(jìn)展 B輯(2015年2期)2015-04-20 05:52:30
文藝論壇(2015年23期)2015-03-04 07:57:15
 Journal of Acupuncture and Tuina Science2018年5期
Journal of Acupuncture and Tuina Science2018年5期
- Journal of Acupuncture and Tuina Science的其它文章
- Clinical observation of Zhen’ai needling method in Nei Jing (Classic of Internal Medicine) on improving quality of life in patients with allergic rhinitis
- Effect of acupoint massage plus acupoint sticking therapy for the stress reaction during postoperative anesthesia recovery period in patients undergoing nasal endoscopic surgery
- Effect of modified Qing Long Bai Wei needling on the levels of IL-1β, IL-6 and INF-α in synovial fluid of knee osteoarthritis patients
- Therapeutic observation of acupuncture plus tuina for cervical vertigo
- Clinical experience of Xiangxi Liu’s infantile tuina for exogenous fever in children
- Experimental study on the influence of pressing force and time on thermal effect of An-pressing manipulation