
Circulating thrombospondin-2 in patients with moderate-to-severe chronic heart failure due to coronary artery disease
2016-12-13 08:41:22AlexanderBerezinAlexanderKremzerTataynaSamura
Alexander E.Berezin,Alexander A.Kremzer,Tatayna A.Samura
Department of Internal Medicine;Department of Clinical Pharmacology,State Medical University,Zaporozhye 69035, Ukraine.
Circulating thrombospondin-2 in patients with moderate-to-severe chronic heart failure due to coronary artery disease
Alexander E.Berezin△,?,Alexander A.Kremzer△,Tatayna A.Samura
Department of Internal Medicine;Department of Clinical Pharmacology,State Medical University,Zaporozhye 69035, Ukraine.
Chronic heart failure(CHF)remains a leading cause of morbidity and mortality.In the current study,we aimed to evaluate the predictive value of circulating thrombospondin-2(TSP-2)for cumulative survival in patients with ischemic CHF due to coronary artery disease(CAD).The results showed that during a median follow-up of 2.18 years,21 participants died and 106 subjects were hospitalized repeatedly.The median circulating levels of TSP-2 in patients who survived and those who died were 0.63 ng/mL(95%CI=0.55-0.64 ng/mL)and 1.03 ng/ mL(95%CI=0.97-1.07 ng/mL)(P<0.001).Circulating TSP-2 independently predicted all-cause mortality (OR=1.27;95%CI=1.08-1.59;P=0.002),CHF-related death(OR=1.16;95%CI=1.02-1.50;P<0.001),and also CHF-related rehospitalization(OR=1.12;95%CI=1.07-1.25;P<0.001).In conclusion,among CAD patients with symptomatic CHF,increased circulating TSP-2 is correlated with increased 3-year CHF-related death,all-cause mortality,and risk for recurrent hospitalization.
thrombospondin-2,chronic heart failure,survival,hospitalization,prognosis
Introduction
Chronic heart failure(CHF)remains a leading cause of morbidity and mortality worldwide[1].The natural evolution of CHF is associated with endothelial dysfunction that results in shear stress disorders on endothelium which is exerted by several factors,such as angiotensin-aldosterone system activation,oxidative stress,proinflammatory response,exaggerated collagen synthesis and extracellular matrix(ECM)remodelling in vasculature,and degradation of vasodilators[2]. Thrombospondin-2(TSP-2)is an important component that influences the function of vascular smooth muscle cells,endothelial cells,fibroblasts and inflammatory cells,as well as modulates the survival of endothelial cells and myocytes with important implications for CHF evolution[3-4].Therefore,TSP-2 mediates an adaptive endothelial stress response,integrates endothelial function with ECM protein remodelling and,also protects the heart and the vessels from any injury[5]. Recent experimental studies have shown that TSP-2, as an essential inhibitor of angiogenesis,cardiomyocyte damage and extracellular matrix disruption,is able to increase age-dependently and modulates an interrelation between immunity and cardiovascular remodelling[6-7].Although TSP-2 may affect vascular function,thereby influencing tissue remodelling and promoting the generation of T regulatory cells that control the inflammatory response[8],the role ofTSP-2 in CHF is completely unknown.It has been reported that increased TSP-2 associates well with the severity of diastolic heart failure and predicts mortality in patients with preserved left ventricular ejection fraction[9].This suggests that TSP-2 might be considered as a marker of the natural evolution of CHF irrespectively related with worsening endothelial function.The objective of the study was to evaluate the predictive value of circulating TSP-2 for cumulative survival in patients with symptomatic CHF due to coronary artery disease(CAD).
Patients and methods
Patients
The study included 188 patients aged 42 to 63 years with ischemic(n=154)and non-ischemic(n=34) symptomatic moderate-to-severe CHF,and 44 patients with stable angiographically proven CAD.CHF was diagnosed according to current clinical guidelines[10]. The study was approved by the local ethics committee of State Medical University,Zaporozhye,Ukraine.The study was carried out in conformity with the Declaration of Helsinki.All the patients provided their written,informed consent for participation in the study. The study lasted up to 3 years.
Multi-spiral computed tomography angiography
Multi-spiral computed tomography(CT)angiography was carried out for all the patients prior to their inclusion in the study.When atherosclerotic lesions of the coronary arteries were verified,patients were subjected to conventional angiographic examination,provided indications for revascularization were available.CAD was considered to be diagnosed upon availability of previous angiographic examinations carried out no later than 6 months previously,provided that no new cardiovascular events occurred for this period and the procedures were available for assay.The coronary artery wall structure was measured by means of contrast spiral CT angiography[11]on the Somatom Volume Zoom scanner(Siemens, Erlangen,Germany)with two detector rows with patients holding their breath at the end of inspiration.After preliminary native scanning,non-ionic contrast Omnipak (Amersham Health,Ireland)was administered for the optimal image of the coronary arteries.To reconstruct the image,0.6-mm-width axial tomographic slices were used.
Transthoracic echocardiography
Transthoracic ultrasonic echocardiography was performed conventionally on an ACUSON apparatus (SIEMENS)in B-mode regimen and tissue Doppler echocardiography regimen from parasternal,subcostal, and apical positions over the short axis and long axis with sensor P of 5 MHz.Left ventricular end-diastolic and end-systolic volumes were measured by modified Simpson’s planimetric method;they were measured by cylinder method if severe failure of local myocardial contractility was observed.Left ventricular ejection fraction (LVEF)was assessed in compliance with the requirements of American Society of Echocardiography[12]. Tissue Doppler echocardiography was carried out in 4-,3-and 2-chamber projections in each of 16 segments of the left ventricle and in 4 spots of the mitral annulus:at the base of the posterior septal,lateral,inferior,and anterior left ventricular walls[13].Peak systolic(Sm), early diastolic(Em),and late diastolic(Am)myocardial velocities were measured in the mitral annulus area, followed by calculating velocity of early diastolic left ventricular filling(E)to Am(E/Am)ratio and to Em (E/Em)ratio.
Calculation of glomerular filtration rate
Glomerular filtration rate(GFR)was calculated using MDRD-6 formula[14].
Measurement of TSP-2,galectin-3,NT-pro-BNP,total cholesterol and its fractions
To determine TSP-2,N-terminal pro-brain natriuretic peptide(NT-pro-BNP),total cholesterol(TC)and cholesterol fractions,blood samples were drawn in the morning(at 7-8 a.m.)into pre-chilled silicone test tubes.Samples were processed according to the recommendations of the manufacturer of the analytical instruments used.They were centrifuged at 6,000 rpm for 3 minutes.Then,plasma was refrigerated immediately and stored at a temperature not higher than-35°C. Circulating galectin-3(Gal-3)and TSP-2 levels were determined by ELISA(Bender MedSystems GmbH, Vienna,Austria).NT-pro-BNP content was measured by immunoelectrochemoluminescent assay using sets by R&D Systems(USA)on Elecsys 1010 analyzer (Roche,Mannheim,Germany).Concentrations of TC and high-density lipoprotein cholesterol(HDL-C)were measured by fermentation method.Concentration of low-density lipoprotein cholesterol(LDL-C)was calculated according to the Friedewald formula(1972).
Statistical analysis
Statistical analysis was carried out in the SPSS system for Windows,Version 22(SPSS Inc,Chicago,IL, USA).The data were presented as mean±SEM or 95%confidence interval(CI);median and interquartile range.Normal distribution was checked by means ofShapiro-Wilk test and Kolmogorov-Smirnov test.Twotailed Student t-test or Shapiro-Wilk U-test were used for comparison of the main parameters of patients′groups.Chi square test(χ2)and Fisher F exact test were used to compare categorical variables between groups. The circulating TSP-2 and NT-pro-BNP levels in the blood were not in normal distribution,while distribution of TC and cholesterol fractions had a normal character and was not subjected to any mathematical transformation.The factors,which could be associated potentially with circulating TSP-2,were determined by logistic regression analysis.Receiver operation curve(ROC) analysis was carried out to identify the optimal cut-off points of the TSP-2 concentration with predicted value. Net reclassification improvement(NRI)was used for comparison of AUC curves.Odds ratio(OR)and 95%CI were calculated for all the independent predictors of survival of the patients.A calculated difference of P<0.05 was considered significant.
Results
Demographic and baseline characteristics of the study patients
Table 1shows the general characteristics of the patients included in the study.No statistical differences in age and gender were found among study subjects. The patients were also comparable in baseline characteristics including body mass index(BMI),GFR, HbA1c,fasting blood glucose level,blood creatinine level,TC,LDL-C and HDL-C,and the number of damaged coronary vessels.
Hypertension was present in 32(72.7%)CAD subjects without CHF and in 73(47.4%)ischemic CHF subjects(P=0.002).No hypertension subjects in the non-ischemic CHF cohort were found.The proportion of patients with dyslipidemia in all cohorts was similar. Type 2 diabetes mellitus was present in 17(38.6%) CAD subjects without CHF,in 53(34.4%)subjects with ischemic CHF,and in 3(8.8%)subjects with non-ischemic CHF(P=0.003).CHF class distribution was similar between heart failure patients in the two cohorts.No difference was found between cohorts in systemic blood pressure(BP)and heart rate(HR).
The levels of circulating NT-pro-BNP and Gal-3 were significantly higher in patients with CHF than in CAD patients without left ventricular dysfunction. There was not a statistically significant change in left ventricular ejection fraction,E/Am and E/Em between the CAD cohort and ischemic CHF cohort,while decrease in the left ventricular ejection fraction and increase of diastolic performances were found in patients with non-ischemic CHF in comparison with other cohorts.
When analyzing details of pharmacotherapy,no substantial differences were found between CAD subjects without CHF and ischemic CHF patients with regard to administration of the majority of drugs.However,frequencies of statins and metformin prescribing in nonischemic CHF patients were lower when compared with CAD subjects without CHF and ischemic CHF patients.
Clinical events
During the median follow-up of 2.2 years,21 participants with ischemic CHF died and CHF-related death was defined in 18 patients of this cohort.Additionally, 106 subjects with ischemic CHF were re-hospitalized due to advanced CHF.Eleven subjects with nonischemic CHF were admitted to the hospital due to advanced CHF and 9 subjects died due to CHF-related reasons.Only three patients with CAD without CHF died due to myocardial infarction within the observation period.Four new cases of ischemic CHF were found in the CAD subjects.All clinical events for survival analysis were determined as cumulative.
Circulating TSP-2 levels
The median circulating levels of TSP-2 in ischemic CHF patients were 17.31 ng/mL(95%CI=14.10-19.13 ng/mL)and,in non-ischemic CHF patients,were 18.19 ng/mL(95%CI=15.25-20.1 ng/mL)(P=0.62). However,the median circulating TSP-2 in CAD patients without CHF was 12.13 ng/mL(95%CI= 10.10-15.23 ng/mL)(P=0.022).
Furthermore,TSP-2 plasma levels were directly correlated with galectin-3(r=0.599,P=0.001);NT-pro-BNP (r=0.493,P=0.001),NYHA functional class of CHF (r=0.46,P=0.001),multi-vessel lesion of coronary arteries(r=0.362,P=0.001),E/Am(r=0.362, P=0.001),E/Em(r=0.34,P=0.001),T2DM (r=0.34,P=0.003),TC(r=0.32,P=0.001),age (r=0.29,P=0.001),gender(r=0.212,P<0.001formale), smoking(r=0.26,P=0.001)and inversely to LVEF(r= -0.542,P=0.001)and estimated GFR value(P=-0.438, P=0.003).No significant association between the levels of circulating TSP-2 with fasting plasma glucose, HbA1c,mean systolic and diastolic BP,premature CAD in family history,and medications for both cohorts of the patients was found.
The TSP-2 concentration as predictor of CHF
ROC was constructed for TSP-2 concentrations among patients with and without cumulative clinical events,defined as combination of death and CHF-relatedhospitalization.ROC analysis indicated selected patients with cumulative clinical events had a lower TSP-2concentration than subjects who demonstrated clinical events. We found that the best balanced cut-off point of TSP-2 concentration for patients with cumulative events versus without cumulative events was 14.65 ng/mL.The area under cure(AUC)represented 0.823(SD=0.34; 95%CI0.575-0.889;P<0.001),and sensitivity and specificity were 89.6%and 63.3%,respectively.ROCs were created for ischemic CHF subjects,non-ischemic CHF patients and CAD persons without CHF.We used the previously obtained cut-off point of TSP-2 concentration of14.65ng/mL,with the aim of distinguishing subjects with ischemic CHF and with non-ischemic CHF(P<0.05). AUC obtained for CAD persons without CHF showed to be significantly smaller when compared with AUCs that were suitable for ischemic CHF and non-ischemic CHF subjects(P<0.05)(Fig.1).Thus,concentration of TSP-2>14.65 ng/mL demonstrated predictive value of expected cumulative clinical events among all selected patient population,while the overall ability of the cut-off point of TSP-2 to correctly identify CHF patients with unfavourable clinical outcomes was higher than for other cohorts.
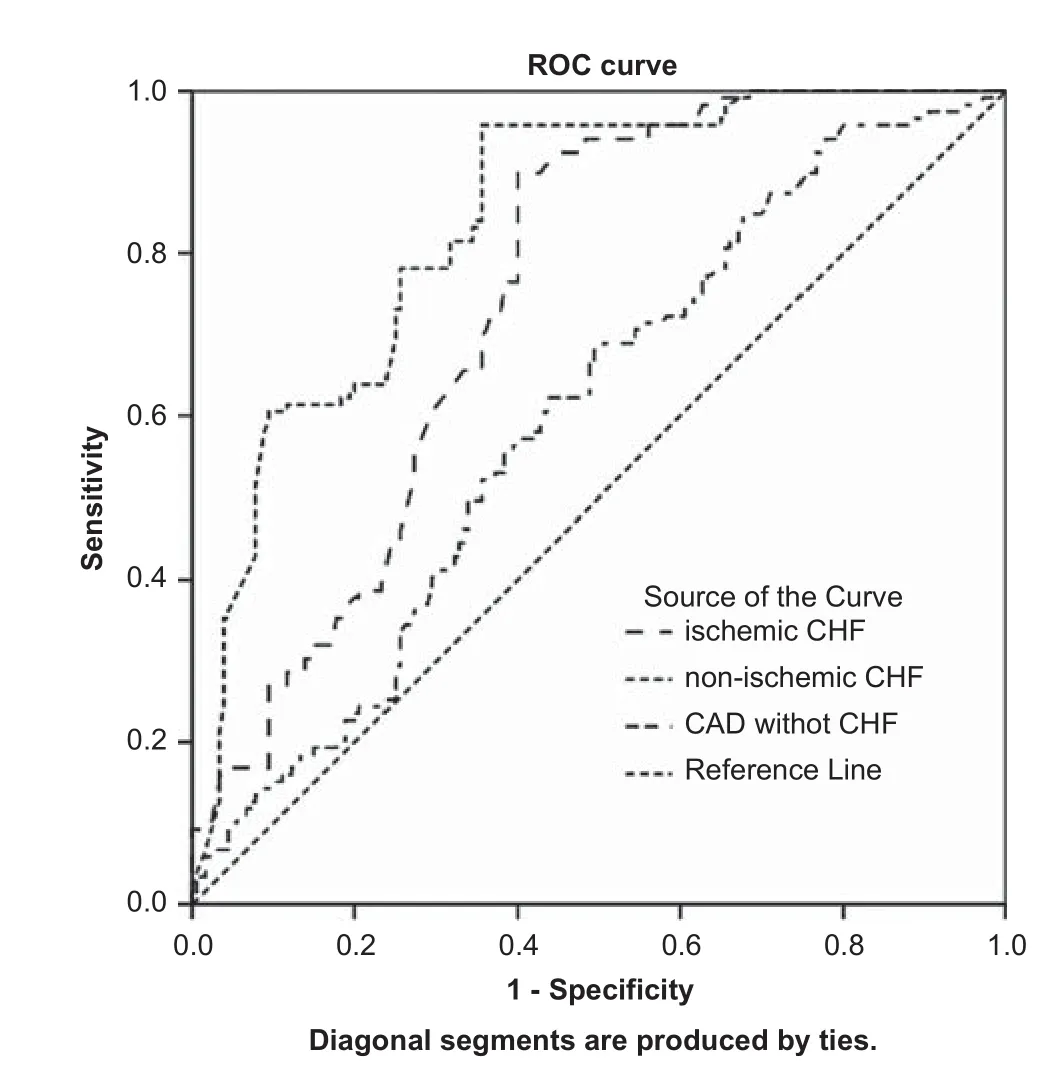
Fig.1Sensitivity and specificity of the model survival for patient study population based on circulating TSP-2 level.Results of the Receiver Operating Characteristic(ROC)analysis.
Iterations between sensitivity and specificity of TSP-2 cut-off point level for other clinical outcomes in the study patient population with CHF are presented in Table 2.For all occasions,the model was robust and provided significant results using the optimal cutoff point of TSP-2.However,there was a significant difference between AUCs(Std.error)calculated for CHF patients(Net reclassification improvement [NRI]index=0.34;95 CI=0.21-0.56;P= 0.012).NRI statistical analysis showed that a random event CHF subject had a higher predicted p value than a random non-event CHF subject,and that the predictive value of TSP-2 for ischemic CHF was statistically higher than for non-ischemic CHF.
Given the obtained data,we included further analysis of survival appropriate data for ischemic CHF patients.A significant divergence of Kaplan-Meier survival curves was found in patients with high(>14.65 ng/mL)and low(<14.65 ng/mL)concentrations of TSP-2(Fig 2).The curve divergence of event accumulation reached a statistical significance in week 22 of the observation period(P<0.001).
In the logistic regression analysis,the main factors independently related with cumulative mortality and CHF-related rehospitalization were TSP-2,NT-pro-BNP,galectin-3,LVEF,T2DM,and three-and multivessel lesion.Circulating TSP-2(over 16.65 ng/mL) independently predicted all-cause mortality (OR=1.12;95%CI=1.07-1.17;P=0.001),CHF-related death(OR=1.08;95%CI=1.02-1.11; P<0.001),and also CHF-related rehospitalization (OR=1.10;95%CI=1.02-1.15;P<0.001)within the 3 years of the observation period(Table 3).NT-pro-BNP,Gal-3 and LVEF remained statistically significant for all categories:all-cause mortality,CHF-related death,and CHF-related rehospitalizations,whereas T2DM and three-and multi-vessel lesions for all variables did not.
Using a stepwise model selection method for multivariable prediction model,we investigated the summaryeffect of any combinations of TSP-2,NT-pro-BNP, galectin-3 and LVEF on all-cause mortality,CHF-related death,and CHF-related rehospitalizations. We found that TSP-2(Model 1)and the combination of TSP-2 with NT-pro-BNP(Model 2)remained statistically significant predictors for all-cause mortality (B-coefficient=1.22,P=0.001,and B-coefficient =1,34,P=0.001 respectively),CHF-related death (B-coefficient=3.56,P=0.001,and B-coefficient= 3,95,P=0.001 respectively),and CHF-related rehospitalizations(B-coefficient=2.90,P=0.001,and B-coefficient=2,86,P=0.001,respectively).Whereas, combination of TSP-2 with NT-pro-BNP and galectin-3 (Model 3),combination of TSP-2 with galectin-3 (Model 4)or with NT-pro-BNP and galectin-3 and LVEF(Model 5)were not significant predictors (B-coefficient=0.026,P=0.82,and B-coefficient= 0,025,P=0.82,and B-coefficient=0,015,P=0.78, and B-coefficient=0,013,P=0.58,respectively).In fact,a stepwise model selection method demonstrated that LVEF,T2DM and three-and multi-vessel lesions of coronary arteries added to combination of TSP-2 and NT-pro-BNP do not offer any additional information to discriminate between survived and dead patients with CHF(B-coefficient of 0.022,0.026,and 0.028, respectively;p-valuesof0.862,0.880and0.860,respectively).
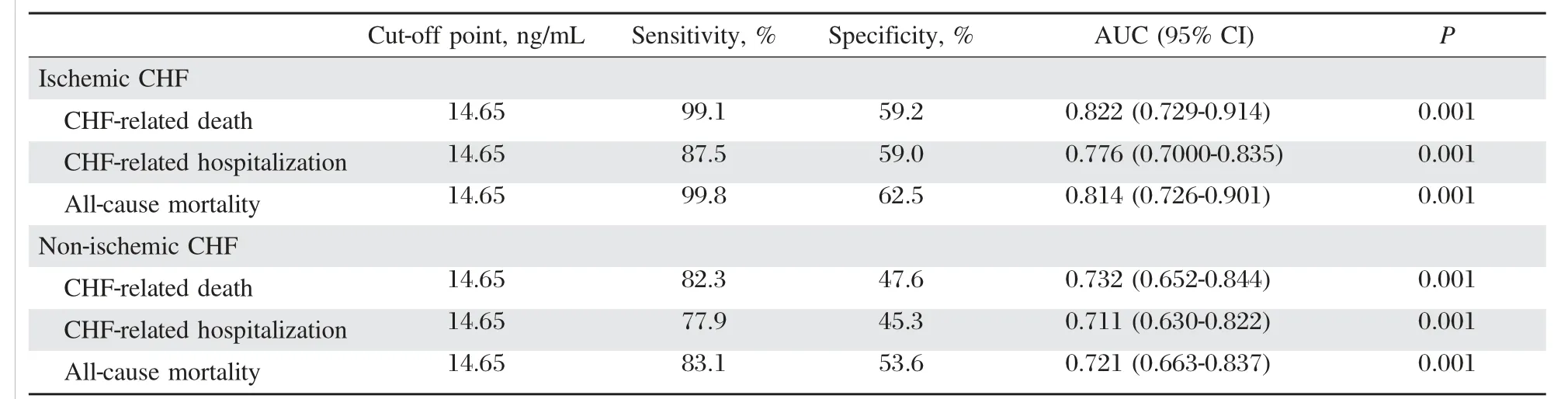
Table 2Iterations between sensitivity and specificity of TSP-2 cut-off point level for clinical outcomes in study patient population.
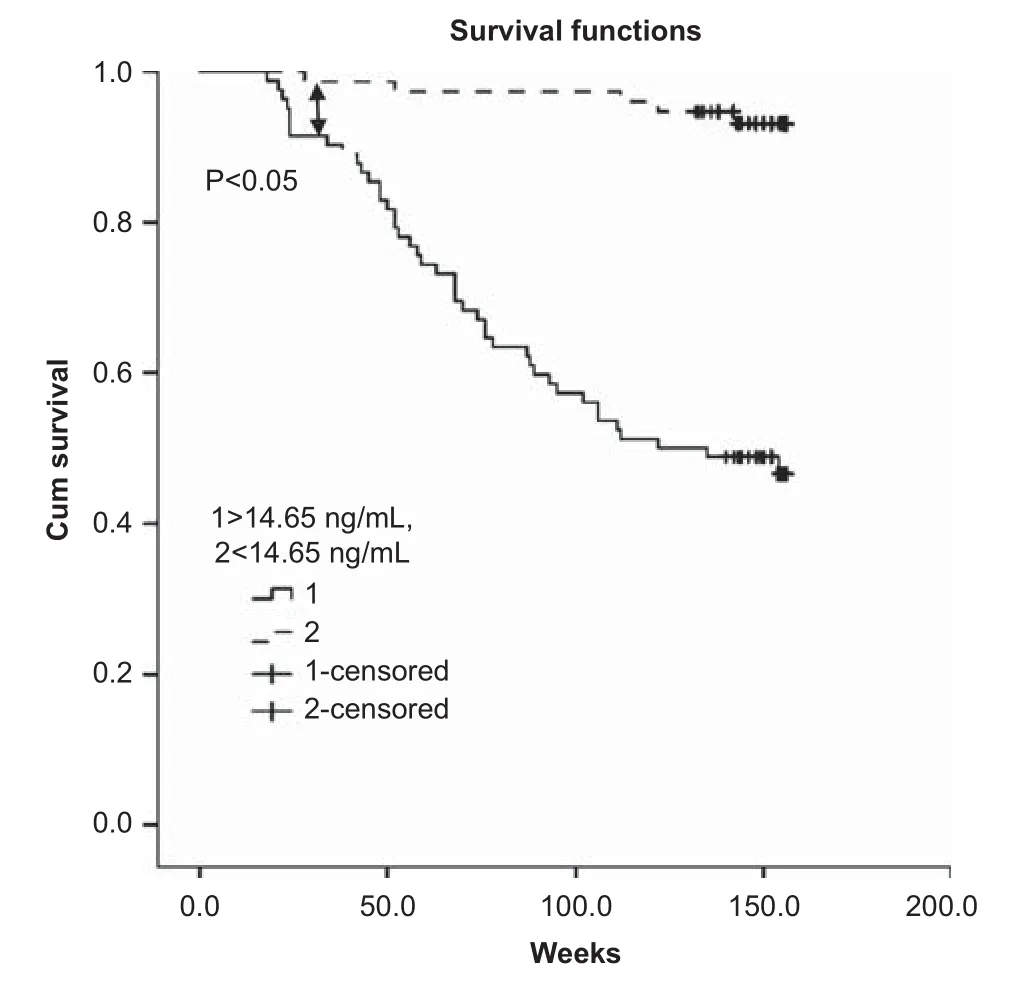
Fig.2The cumulative survival in two groups of patients with low(<14.65ng/mL)andhigh(>14.65ng/mL)circulatinglevels of TSP-2.Kaplan-Meier survival analysis shows achieving significantly divergence of survival curves in 22 weeks after baseline(P<0.05).
Discussion
TSP-2 is a non-structural glycoprotein belonging to the family of microcellular proteins regulating cellmatrix interactions[15].Currently,investigations indicate that TSP-2 produces a dual effect on tissue remodelling. First,TSP-2 activates the‘a(chǎn)nti-inflammatory’T-regulatory cells through the interaction with CD47 that results in preventing migration of endothelial cells,cell adhesion,cell death,apoptosis,and necrosis[16-17].Second, TSP-2 may modulate tissue inflammation by limiting the tissue damage caused by the immune response and hence,realizing an adaptive effect[18].Thirdly, TSP-2 can inhibit angiogenesis by limiting matrix-modulating activity,proliferation and inducing apoptosis of endothelial cells[19].After acute tissue injury such as ischemia and in a hypertension heart,increased circulating TSP-2 was found[20].However,an association between declined TSP-2 in blood and exaggerated inflammatory response are expected in patients with myocardial dysfunction[21].Really,according to Frangogiannis et al.[20],thrombospondins,as potent inhibitors of angiogenesis and activators of transform-ing growth factor,are induced in healing myocardial infarcts and play a pivotal role in suppressing the post-infarction inflammatory response,inhibiting local angiogenesis,and limiting expansion of granulation tissue into the non-infarcted area.On the other hand,an increase of TSP-2 level in CHF patients can be interpreted as a reflection of a non-adaptive response on proinflammatory activation that is essential for CHF and also appears to be critical for survival[22].The results of our investigation support this assumption. We found elevated TSP-2 level in the patients who died when compared with those who survived.However,an increase of TSP-2>14.65 ng/mL associates well with declined cumulative survival incidences at 22 weeks after baseline(P<0.05).Moreover,the significant divergence of Kaplan-Meier survival curves in patients with high(>14.65 ng/mL)and low(<14.65 ng/mL) concentrations of TSP-2 was able to continue without the tendency to convergence during all observation periods.We also found that elevated circulating TSP-2 independently predicted all-cause mortality,CHF-related death,and CHF-related rehospitalization in patients with CHF.Thus,our findings relate well with some of the recent clinical study data by Kimura et al.[9]and Hanatani et al[21].Their research revealed that TSP-2 may be considered as a useful biomarker in CHF patients with reduced LVEF.However,Hanatani et al.[21]found that circulating TSP-2 elevation was associated with cardiovascular mortality in elderly men. We also found a negative association for TSP-2 with the LVEF value in subjects who were enrolled in the study,but no profound correlations with age and the male gender were investigated.Taking into consideration the patients who were eligible for the study had preserved LVEF and elevated circulating level of both prognostic biomarkers in CHF:galectin-3 and NT-pro-BNP.Therefore,galectin-3 and NT-pro-BNP were significantly associated with circulating TSP-2,but the predicted model,after adding to TSP-2 several biomarkers,such as NT-pro-BNP and galectin-3 or the combination of NT-pro-BNP with galectin-3 and LVEF,did not improve cumulative prognostic value for combination TSP-2 and NT-pro-BNP.Similar data was obtained for the combination of TSP-2 and NT-pro-BNP versus TSP-2 and galectin-3.We believe that TSP-2 may be added to the prognostic model based on NT-pro-BNP and/or galectin-3 as a tool for reclassification of the patients with CHF at high risk of mortality and CHF-related unfavourable clinical outcomes.In conclusion, among CAD patients with symptomatic CHF, increased circulating TSP-2 is correlated with increased 3-year CHF-related death,all-cause mortality,and risk for recurrent hospitalization.
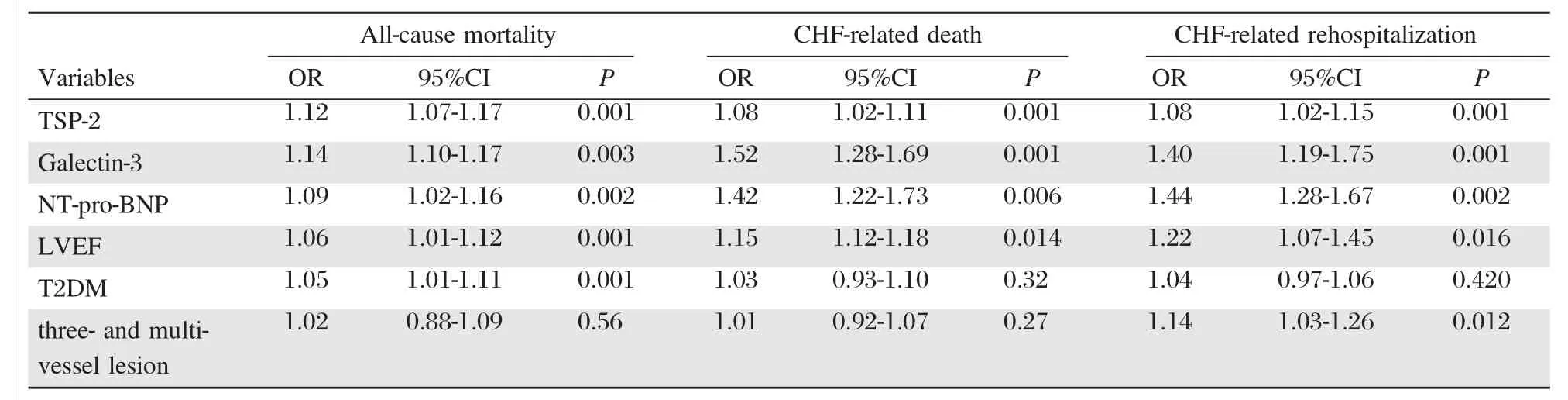
Table 3Variables independently related to 3-year all-cause mortality,CHF-related death,and CHF-related rehospitalization,obtained by logistic regression analysis.
The major limitation of this study was the small population size.However,this was not a randomized and controlled study.Authors believe that a greater cohort of patients with more incidences detected is desirable to improve the power of the study.Because survival analysis provides little additional information as there are too few deaths in the cohort,we use cumulative events to increase the statistical power.
Acknowledgments
We thank all patients for their participation in the investigation,staff of the Regional Zaporozhye Hospital (Ukraine)and the doctors,nurses,and administrative staff inCity hospital#6(Zaporozhye,Ukraine),general practices,and site-managed organizations that assisted with the study.
References
[1]Roger VL.The Heart Failure Epidemic[J].Int J Environ Res Public Health,2010,7(4):1807-1830.
[2]Matsuzawa Y,Sugiyama S,Sumida H,et al.Peripheral endothelial function and cardiovascular events in high-risk patients[J].J Am Heart Assoc,2013,2(6):e000426.
[3]Krishna SM,Golledge J.The role of thrombospondin-1 in cardiovascular health and pathology[J].Int J Cardiol, 2013,168(2):692-706.
[4]Bornstein P,Armstrong LC,Hankenson KD,et al.Thrombospondin 2,a matricellular protein with diverse functions[J].Matrix Biology,2000,19(7):557-568.
[5]Lynch JM,Maillet M,Vanhoutte D,et al.A Thrombospondin-Dependent Pathway for a Protective ER Stress Response[J].Article Cell,2012,149(6):1257-1268.
[6]Agah A,Kyriakides TR,Letrondo N,et al.Thrombospondin 2 levels are increased in aged mice:consequences for cutaneous wound healing and angiogenesis[J].Matrix Biology,2004,22(7):539-547
[7]van Almen GC.,Swinnen M,Carai P,et al.Absence of thrombospondin-2 increases cardiomyocyte damage and matrix disruption in doxorubicin-induced cardiomyopathy[J].J Mol Cell Cardiol,2011,51(3):318-328.
[8]Lawle J.The functions of thrombospondin-1 and-2[J]. Curr Opinion Cell Biology,2000,12(5):634-640.
[9]Kimura Y,Izumiya Y,Hanatani S,et al.Circulating Thrombospondin-2 Levels Correlate with Disease Severity and Predict Mortality in Patients with Diastolic Heart Failure[J].J Cardiac Failure,2013,19(10):S155
[10]McMurray JJV.,Adamopoulos S,Anker SD,et al.ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2012[J].Eur Heart J,2012,33:1787-1847
[11]Bluemke DA,Achenbach S,Budoff M,et al.Noninvasive coronary artery imaging:magnetic resonance angiography and multidetector computed tomography angiography:a scientific statement from the American Heart Association Committee on Cardiovascular Imaging and Intervention of the Council on Cardiovascular Radiology and Intervention,and the Councils on Clinical Cardiology and Cardiovascular Disease in the Young[J].Circulation, 2008,118:586-606
[12]Schiller NB.,Shah PM.,Crawford M,et al.Recommendations for quantitation of the left ventricle by twodimensional echocardiography.American Society of Echocardiography Committee on Standards,Subcommittee on Quantitation of Two-Dimensional Echocardiograms[J]. J Am Soc Echocardiogr,1989,2:358-367.
[13]Pellerin D.,Sharma R.,Elliott P.,et al.Tissue Doppler, strain,and strain rate echocardiography for the assessment of left and right systolic ventricular function[J].Heart, 2003,89(90003):iii9-17
[14]Levey AS,Stevens LA,Schmid CH,et al.for the CKDEPI(Chronic Kidney Disease Epidemiology Collaboration).A New Equation to Estimate Glomerular Filtration Rate[J].Ann Intern Med,2009,150(9):604-612.
[15]Schroen B,Heymans S,Sharma U,et al.Thrombospondin-2 is essential for myocardial matrix integrity:increased expression identifies failure-prone cardiac hypertrophy[J]. Circ Res,2004,95:515-522.
[16]Rebres RA,Kajihara K,Brown EJ.Novel CD47-dependent intercellular adhesion modulates cell migration[J]. J Cell Physiol,2005,205:182-193.
[17]Lamy L,Foussat A,Brown EJ,et al.Interactions between CD47 and thrombospondin reduce inflammation[J]. J Immunol,2007,178:5930-5939.
[18]Vila V,Mart?′nez-Sales V,Almenar L,et al.Inflammation, endothelial dysfunction and angiogenesis markers in chronic heart failure patients[J].Int J Cardiol,2008,130(2):276-277.
[19]Krady MM,Zeng J,Yu J,et al.Thrombospondin-2 Modulates Extracellular Matrix Remodeling during Physiological Angiogenesis[J].Am J Pathology,2008,173 (3):879-891.
[20]Frangogiannis NG,Ren G,Dewald O,et al.Critical role of endogenous thrombospondin-1 in preventing expansion of healing myocardial infarcts[J].Circulation,2005,111:2935-2942
[21]Hanatani S,Izumiya Y,Araki S,et al.Thrombospondin-2 is a Useful Biomarker in Patients with Reduced Left Ventricular Ejection Fraction[J].J.Cardiac Failure, 2013,19(10):S139.
[22]LichtmanAH.The heartof the matter:Protection of the myocardium from T cells[J].J Autoimmunity,2013,45:90-96.
△The authors have contributed equally to this paper.
?Alexander E.Berezin,Professor,MD,PhD, Department of Internal Medicine,State Medical University,26, Mayakovskyav.,Zaporozhye,69035,Ukraine,E-mail:dr_berezin@mail.ru
24 February 2014,Revised 14 April 2014,Accepted 26 December 2014,Epub 02 March 2015
R541.6,Document code:A
The authors reported no conflict of interests.
 THE JOURNAL OF BIOMEDICAL RESEARCH2016年1期
THE JOURNAL OF BIOMEDICAL RESEARCH2016年1期
- THE JOURNAL OF BIOMEDICAL RESEARCH的其它文章
- Molecular docking simulation analysis of the interaction of dietary flavonols with heat shock protein 90
- Myocardin-related transcription factor A cooperates with brahmarelated gene 1 to activateP-selectin transcription
- Assessment of malathion and its effects on leukocytes in human blood samples
- Manifestations of type 2 diabetes in corneal endothelial cell density, corneal thickness and intraocular pressure
- Impact of IL28Bgene polymorphisms rs8099917 and rs12980275 on response to pegylated interferon-α/ribavirin therapy in chronic hepatitis C genotype 4 patients
- Emerging targets for glioblastoma stem cell therapy