
Surgical treatment of synchronous colorectal liver and lung metastases:the usefulness of thoracophrenolaparotomy for single stage resection
2016-04-28 01:43:43DanieleDelFabbroMarcoAlloisioFabioProcopioMatteoCiminoMatteoDonadonAngelaPalmisanoLucaViganandGuidoTorzilliMilanItaly
Daniele Del Fabbro,Marco Alloisio,Fabio Procopio,Matteo Cimino,Matteo Donadon,Angela Palmisano,Luca Viganò and Guido TorzilliMilan,Italy
?
Surgical treatment of synchronous colorectal liver and lung metastases:the usefulness of thoracophrenolaparotomy for single stage resection
Daniele Del Fabbro,Marco Alloisio,Fabio Procopio,Matteo Cimino,Matteo Donadon,Angela Palmisano,Luca Viganò and Guido Torzilli
Milan,Italy
ABSTRACT:When suitable,surgery still remains the therapeutic option to be preferred for patients carrier of colorectal liver and lung metastases.Since thoracophrenolaparotomy should be helpful during liver resection for some of these patients,simultaneous removal of right lung metastases can be proposed through this approach.Eleven consecutive patients(median age of 53 years)carrier of colorectal liver and lung metastases,underwent single session surgical resection of both liver and right lung lesions by means of J-shaped thoracophrenolaparotomy.The median number of liver metastases removed was 5(range 2-30)and of lung metastases removed was 2(range 1-3).Lung metastases were located in the upper lobe in 1 patient,in the middle lobe in 2,in the lower lobe in 6,and in the upper and lower lobe in 2.Mortality and major morbidity were nil.Two patients had a minor morbidity:one had wound infection and bile leakage treated conservatively and the other had transient fever.Mean overall survival was 24.4 months.An aggressive surgical approach should be undertaken for colorectal metastases:in case of multifocal liver disease with complex presentations,J-shaped thoracophrenolaparotomy could be considered as safe approach for combined liver and right lung metastasectomies.
(Hepatobiliary Pancreat Dis Int 2016;15:216-219)
KEY WORDS:colorectal carcinoma;
liver metastases;
lung metastases;
thoracophrenolaparotomy
Author Affiliations:Department of Hepatobiliary Surgery(Del Fabbro D,Procopio F,Cimino M,Donadon M,Palmisano A,Viganò L and Torzilli G)and Department of Thoracic Surgery(Alloisio M),Humanitas Research Hospital,University of Milan School of Medicine,Rozzano,Milan,Italy
? 2016,Hepatobiliary Pancreat Dis Int.All rights reserved.
Published online September 17,2015.
Introduction
M ore than 50% of patients undergoing curative resection of a colorectal carcinoma will experience recurrent disease and liver and lung are the commonest sites of occurrence.The rationale for an aggressive surgical policy for both metastatic sites is well established and associated with improved prognosis,[1,2]leading to the extension of the indications for surgery.Staged or simultaneous resections accomplished by thoracic and/or abdominal approach have been proposed.[3,4]However,these approaches demand two or three(if bilateral lung metastases)operations,or otherwise a single operation by means of two separate incisions.Thoracophrenolaparotomy represents an established safe surgical approach in resective liver surgery[5,6]and through this incision synchronous liver and right lung metastases can be treated simultaneously in a single session.
Methods
Eligibility criteria
Indications for liver and lung metastasectomies were as follows:(i)controlled primary disease;(ii)no evidence of extrahepatic lesions other than resectable lung metastases;(iii)disregarding number and distribution of colorectal liver metastases(CLM),technical resectability leaving a remnant liver volume of at least 40%;(iv)dis-regarding number and distribution of lung metastases,all of the detected nodules could be removed preserving enough functioning remnant lung based on the results of the preoperative cardiopulmonary functional tests;(v)patients eligible for a J-shaped thoracophrenolaparotomy because carrier of CLM located at hepatocaval confluence,or in the paracaval portion of segment 1,or in the upper portion of segments 4a,7 and 8,or presenting strong-adhesion or infiltration of the diaphragm,irrespective of whether metastases in right lung are diagnosed throughout preoperative diagnostic workup.
Study population
Between September 2004 and April 2013,298 patients underwent curative liver resection for CLM.Of these,20 patients had simultaneous lung metastases.Nine patients received a thoracoscopic resection subsequent to liver surgery,since the latter was carried out without the need of a thoracoabdominal approach.Right lung metastases were resected synchronously with CLM in the remaining 11 patients by means of a thoracophrenolaparotomy.Characteristics of patients are listed in Table.The preoperative staging included for all patients colonoscopy,thoracoabdominal contrast-enhanced CT,contrast-enhanced MRI of the liver,and 18-FDG PET scan.
Location of lung metastases is shown in Table.Liver metastases were located in all segments,ranging between 3 and 85 mm in diameter.Four patients had multiple(more than 4)bilobar CLM;among them,one had a preoperative diagnosis of 25 liver metastases and surgical exploration revealed 5 more lesions.Liver resections included major liver resections,limited resections and enucleations of small superficial nodules.Wedge resections of the right lung were performed in all patients.Two patients had bilateral lung metastases and they received supplementary operation for the clearance of the left lung one month after the first operation.
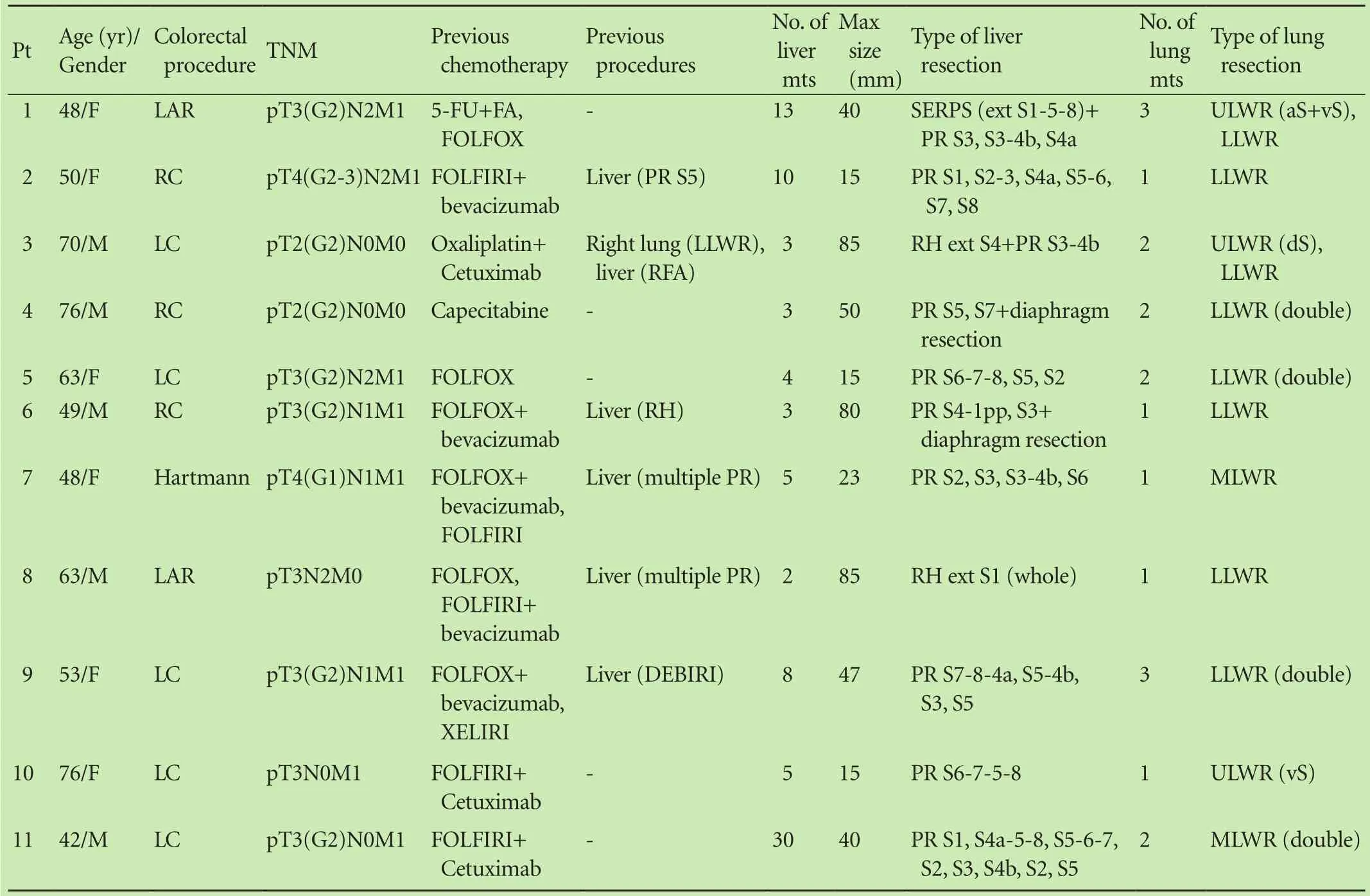
Table.Characteristics of patients and surgical procedures
Surgical procedures
The J-shaped abdominal incision conventionallyadopted for liver surgery is performed.If needed(see eligibility criteria),the incision is prolonged along the 9th right intercostal space allowing the access to the thoracic cavity.The incision of the skin and the external oblique muscle reaches the anterior axillary line.A small portion of the cartilaginous costal arch is removed and the lateral portion of the diaphragm is divided in a radial direction.The inner parietal incision,involving the pleura and intercostal muscles,is prolonged up to the posterior axillary line preserving the intercostal neurovascular bundle(Fig.).
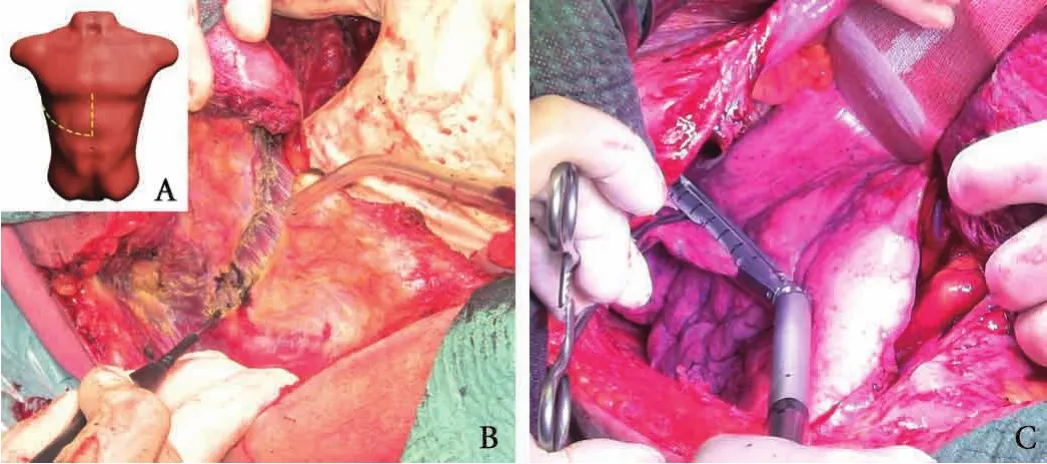
Fig.J-shaped thoracophrenolaparotomy.A:schematic view(yellow line:laparotomy;green line:thoracotomic extension);B:division of intercostal muscles along the 9th intercostal space;C:wedge resection of the upper lobe performed through thoracophrenolaparotomy.
Intraoperative ultrasound is performed in all patients to stage the liver involvement,to assess the relationships between tumors and vessels and to guide the dissection of liver parenchyma.For combining the abdominal and thoracic procedures the right liver has to be mobilized at least up to the hepatocaval ligament allowing an enlarged view field to the thoracic cavity.Careful manual palpation of the lung to detect the metastatic lesion is carried out.Pulmonary ligaments and lobar fissures are divided as needed.Then,wedge resection of the lung metastases is performed by using a disposable stapler(Fig.).
Liver resection is then started as previously reported.[7]Briefly,the resection area is defined with the surrounding of the tumor at its deepest portion combining the minimal parenchymal sacrifice and the flattest cut surface under intraoperative ultrasound guidance.Parenchymal transection is obtained under intermittent Pringle maneuver and accomplished using Kelly-clasia,ligating with sutures all the vessels but those thinner ones which are coagulated.Closed suction abdominal drains are inserted in every patient around the liver,in a variable number depending to the number and the size of liver cut surfaces.One or two chest tubes are placed in the pleural cavity.
Results
The median operation time was 578 minutes(range 413-776).Median clamping time was 118 minutes(range 74-268).The overall median blood loss was 450 mL(range 200-1000).Three patients received blood transfusions.The median number of CLM removed was 5(range 2-30)and that of lung metastases was 2(range 1-3).Nine patients had multiple CLM;6 patients had bilateral CLM.The types of liver and lung resections are listed in Table.Only 2 patients underwent a liver resection.Wedge resections of right lung metastases were accomplished through the thoracoabdominal incision in all patients.In two patients,partial diaphragmatic resection was done because of liver tumor infiltration:the diaphragm was repaired in both cases by direct suture.
Mortality and major morbidity were nil;minor morbidity occurred in 2 patients:transient fever in one,wound infection and bile leakage in the other,and both of them were managed conservatively.No clinical complications due to phrenotomy or to the chest opening were observed.The median hospital stay was 9 days(range 8-39).The mean overall survival was 24.4 months(range 11.0-51.7).Tumor recurrence was observed in all patients and 3 patients received further operations,2 because of liver and lung recurrence and 1 because of liver recurrence alone.They all underwent chemotherapy.Similar outcome was observed in the 9 patients who received separate abdominal and thoracic surgery,whose mean overall survival was 20.5 months(range 13.4-30.5).
Discussion
Surgical resection is considered the “gold standard” treatment for CLM,with a reasonable long-term survival.[2]However,the management of patients with both liver and lung metastases is controversial,although several reports documented prolonged survival following staged or simultaneous resection to the liver and lung.[3,4]Resection of liver and lung metastases at various intervals after primary tumor surgery is feasible and safe,but sequential operations or combined but separated abdominal and thoracic approaches are required,increasing physical and psychological load for the patient and,at least theoretically,the surgical risk.Moreover,the essential time for recovery after surgery entails an unavoidable break before the restart of chemotherapy,which could be further prolonged in case of complications.This can be unhelpful especially for patients whose surgical program consists of multiple steps.
In our series we included carriers of liver and lung metastases in which the main load of disease was in the liver:3 patients had at least 10 bilateral CLM,3 had CLM larger than 8 cm(one of them having infiltration of the diaphragm),4 had CLM in contact with major hepaticveins at the caval confluence,and two among them had also CLM in contact with the 1st and 2nd order portal branches.They all received a one-stage procedure achieving the radical resection of liver disease.Safety and effectiveness of thoracophrenolaparotomy in surgery for liver tumors have been already reported in previous studies.[5,6]We performed thoracophrenolaparotomy(38% in our whole series of liver resections)for the aforementioned conditions to ensure liver exposure and vascular control,indispensable for carrying out safely conservative liver resections.We also adopted this approach in patients after repeated surgery or previous interstitial therapies,in which the presence of tight adhesions can make troublesome the dissection of the liver from the diaphragm and from the inferior vena cava.
To our knowledge,this is the first series detailing the feasibility and safety of combined complex liver resections and right lung resections,disregarding their lobar location,by means of a single surgical incision(that is one procedure less in case of bilateral lung metastases).
As alternative to thoracotomy,some techniques have been introduced.Video assisted thoracic surgery should limit the morbidity associated with thoracotomy,but its effectiveness to detect small intraparenchymal lesions is debated because of the lack of palpation.Transthoracictransdiaphragmatic approach,originally reported for the treatment of hepatocellular carcinoma[8]also for resection of CLM located at the dome of the liver together with right lung metastases,[9]is not indicated for bilobar CLM and,by this approach,the usefulness of intraoperative ultrasound for staging the liver involvement distant to the exposed area is very limited.[9]Transdiaphragmatic approach(uni- or bilateral)has been recently proposed for lung metastasectomies in patients with synchronous liver and lung metastases undergoing liver resections,[10]to avoid the combination of laparotomy and thoracotomy or thoracoscopy in a single stage procedure.Authors reported as limitation of this approach its narrow visual field in the thoracic cavity;conversely,thoracophrenolaparotomy,primarily performed for liver surgery,allows also a wide exposure of the lung without the need of any additional incision.
In conclusion,given that an aggressive surgical management of liver and lung metastases from colorectal cancer provide prognostic benefit,J-shaped thoracophrenolaparotomy should be considered as feasible and safe surgical approach for the treatment of both conditions,involving any oncological impairment in comparison with separate laparotomic and thoracotomic or thoracoscopic procedures.Further confirmation of our results in a larger series of patients is necessary to validate this policy.
Contributors:DFD proposed the study and wrote the first draft.All authors contributed to data collection.VL and TG contributed to further drafts.TG is the guarantor.
Funding:None.
Ethical approval:This study was approved by the Ethics Committee of our hospital.
Competing interest:No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
References
1 Ambiru S,Miyazaki M,Ito H,Nakagawa K,Shimizu H,Kato A,et al.Resection of hepatic and pulmonary metastases in patients with colorectal carcinoma.Cancer 1998;82:274-278.
2 Minagawa M,Makuuchi M,Torzilli G,Takayama T,Kawasaki S,Kosuge T,et al.Extension of the frontiers of surgical indications in the treatment of liver metastases from colorectal cancer:long-term results.Ann Surg 2000;231:487-499.
3 Miller G,Biernacki P,Kemeny NE,Gonen M,Downey R,Jarnagin WR,et al.Outcomes after resection of synchronous or metachronous hepatic and pulmonary colorectal metastases.J Am Coll Surg 2007;205:231-238.
4 Brouquet A,Vauthey JN,Contreras CM,Walsh GL,Vaporciyan AA,Swisher SG,et al.Improved survival after resection of liver and lung colorectal metastases compared with liver-only metastases:a study of 112 patients with limited lung metastatic disease.J Am Coll Surg 2011;213:62-71.
5 Xia F,Poon RT,Fan ST,Wong J.Thoracoabdominal approach for right-sided hepatic resection for hepatocellular carcinoma.J Am Coll Surg 2003;196:418-427.
6 Tsugita M,Takasaki K,Ohtsubo T,Yamamoto M,Maruyama C,Katsuragawa H,et al.Right side hepatic resection under right thoracoabdominal incision with special reference to a highly anatomical systematized method.Int Surg 1995;80:242-246.
7 Torzilli G,Procopio F,Botea F,Marconi M,Del Fabbro D,Donadon M,et al.One-stage ultrasonographically guided hepatectomy for multiple bilobar colorectal metastases:a feasible and effective alternative to the 2-stage approach.Surgery 2009;146:60-71.
8 Ko S,Nakajima Y,Kanehiro H,Aomatsu Y,Yoshimura A,Taki J,et al.Transthoracic transdiaphragmatic approach for hepatectomy of Couinaud’s segments VII and VIII.World J Surg 1997;21:86-90.
9 Delis SG,Madariaga J,Bakoyiannis A,Avgerinos C,Touloumis Z,Vasileios V,et al.Combined liver and lung metastasectomy through an exclusive transthoracic approach.J Surg Oncol 2007;96:178-182.
10 Mise Y,Mehran RJ,Aloia TA,Vauthey JN.Simultaneous lung resection via a transdiaphragmatic approach in patients undergoing liver resection for synchronous liver and lung metastases.Surgery 2014;156:1197-1203.
Received November 28,2014
Accepted after revision July 2,2015
doi:10.1016/S1499-3872(15)60422-2
Corresponding Author:Guido Torzilli,MD,PhD,FACS,Department of Hepatobiliary Surgery,Humanitas Research Hospital,University of Milan School of Medicine,Via A.Manzoni,56,20089,Rozzano,Milan,Italy(Tel:+39-02-8224-4083;Fax:+39-02-8224-4590;Email:guido.torzilli@ humanitas.it)
 Hepatobiliary & Pancreatic Diseases International2016年2期
Hepatobiliary & Pancreatic Diseases International2016年2期
- Hepatobiliary & Pancreatic Diseases International的其它文章
- OIder age at first birth is a risk factor for pancreatic cancer:a meta-anaIysis
- Pathologic response to preoperative transarterial chemoembolization for resectable hepatocellular carcinoma may not predict recurrence after liver resection
- Role of microRNA in liver regeneration
- An unusual case of prolonged post-endoscopic retrograde cholangiopancreatography jaundice
- Monocyte chemoattractant protein-1,transforming growth factor-β1,nerve growth factor,resistin and hyaluronic acid as serum markers:comparison between recurrent acute and chronic pancreatitis
- Improvement of gastric emptying by enhanced recovery after pancreaticoduodenectomy