
Improvement of gastric emptying by enhanced recovery after pancreaticoduodenectomy
2016-04-28 01:43:41EfstratiosZourosTheodorosLiakakosAnastasiosMachairasPaulosPatapisChristosAgalianosandChristosDervenisAthensGreece
Efstratios Zouros,Theodoros Liakakos,Anastasios Machairas,Paulos Patapis,Christos Agalianos and Christos DervenisAthens,Greece
?
Improvement of gastric emptying by enhanced recovery after pancreaticoduodenectomy
Efstratios Zouros,Theodoros Liakakos,Anastasios Machairas,Paulos Patapis,Christos Agalianos and Christos Dervenis
Athens,Greece
BACKGROUND:Enhanced recovery after surgery(ERAS)has improved postoperative outcomes particularly in colorectal surgery.This study aimed to assess compliance with an ERAS protocol and evaluate its effect on postoperative outcomes in patients undergoing pancreaticoduodenectomy.
METHODS:Fifty patients who had received conventional perioperative management from 2005 to 2009(conventional group)were compared with 75 patients who had received perioperative care with an ERAS protocol(fast-track group)from 2010 to 2014.Mortality,complications,readmissions and length of hospital stay were evaluated and compared in the groups.
RESULTS:Compliance with each element of the ERAS protocol ranged from 74.7% to 100%.Uneventful patients had a significant higher adherence to the ERAS protocol(87.5% vs 40.7%;P<0.001).There were no significant differences in demographics and perioperative characteristics between the two groups.Patients in the fast-track group had a shorter time to remove the nasogastric tube,start liquid diet and solid food,pass flatus and stools,and remove drains.No difference was found in mortality,relaparotomy,readmission rates and overall morbidity.However,delayed gastric emptying and length of hospital stay were significantly reduced in the fast-track group.The independent effect of the ERAS protocol in reducing delayed gastric emptying and length of hospital stay was confirmed by multivariate analysis.
CONCLUSION:ERAS pathway was feasible and safe in improving gastric emptying,yielding an earlier postoperative recovery,and reducing the length of hospital stay.
(Hepatobiliary Pancreat Dis Int 2016;15:198-208)
KEY WORDS:fast-track;
delayed gastric emptying;
compliance;
length of hospital stay;
morbidity
Author Affiliations:Department of Surgery,“Konstantopouleio” General Hospital,3-5 Agias Olgas Str.,14233 Athens,Greece(Zouros E,Agalianos C and Dervenis C);First Department of Surgery,Laiko University Hospital,Ag.Thoma 17,11527 Athens,Greece(Liakakos T);Third Department of Surgery,Attikon University Hospital,Rimini 1,12462 Athens,Greece(Machairas A and Patapis P)
? 2016,Hepatobiliary Pancreat Dis Int.All rights reserved.
Published online January 13,2016.
Introduction
E nhanced recovery after surgery(ERAS)pathways are best described as structured multidisciplinary care plans that consist of a number of evidencebased treatments covering the entire perioperative period.The combination of these elements reduces the surgical stress and organ dysfunction and therefore greatly shortens the time required for full recovery.[1]ERAS pathways have been shown in multiple studies to accelerate recovery,decrease the length of hospital stay(LOS)and streamline costs,without compromising patients’safety,particularly in the field of colorectal surgery.[1-5]
Pancreaticoduodenectomy(PD)is a technically challenging surgical procedure with high morbidity rates and prolonged LOS even in high volume hospitals.[6]In order to further improve short-term outcomes,ERAS protocols(also called “fast-track” protocols)have been developed.Relatively few studies have assessed the implementation of an ERAS program following PD with varying results in terms of delayed gastric emptying(DGE)and overall morbidity rate,while LOS was significantly shortened without compromising patients’safety.[7-13]Moreover,data about adherence to ERAS elements are limited.[14]Therefore,the true effect of the ERAS protocol on pancreatic surgery should be further investigated.
In order to evaluate the effect of these protocols on postoperative outcomes,the ERAS pathway must beverified prospectively.However,the number of patients undergoing PD per institution is limited.Moreover,a multicenter study needs standardization of the surgical procedure and widespread acceptance of ERAS protocols.Hence,our present study was undertaken as a singlecenter comparative study using a historical control.This study aimed to evaluate the feasibility,safety and outcomes of an ERAS protocol in a tertiary referral hospital with a unit specialized in pancreatic diseases.In addition we assessed compliance with the different elements of the ERAS protocol.
Methods
An ERAS pathway(Table 1)was implemented for PD at the “Konstantopouleio” General Hospital,Athens,Greece since January 2010.The fast-track group(FTG)consisted of 75 consecutive patients who received perioperative care with an ERAS protocol from January 2010 to December 2014.In order to evaluate the effect of the ERAS protocol on postoperative outcomes,the FTG was compared with a historical control group(conventional group;CG)which included 50 patients,operated on consecutively between January 2005 and December 2009,and received conventional perioperative care.Patients who had total or distal pancreatectomy were excluded from the study.Data for patients in the FTG were collected prospectively during the study period.Data for patients in the CG were collected and evaluated retrospectively.The Ethics Committee of our hospital approved the study according to the Declaration of Helsinki and Good Clinical Practice Guidelines and waived the need for written informed consent but oral consent was obtained.
Before surgery,demographics,body mass index(BMI),the American Society of Anesthesiologists(ASA)score,routine blood tests,comorbidities,nutritional status and primary diagnosis were recorded for all patients.All operations were performed by the same team of surgeons of the pancreatic unit.The procedure most commonly performed was pylorus-preserving PD with standard lymphadenectomy,end-to-side two-layer pancreaticojejunostomy,end-to-side hepaticojejunostomy,and antecolic duodenojejunostomy.In case of distal stomach or proximal duodenum involvement,a classical Whipple’s procedure was performed.All anastomoses were hand-sewn.One abdominal drain was placed adjacent to pancreatic and biliary anastomoses in both groups.
Preoperative biliary drainage was performed by endoscopic retrograde biliary drainage or percutaneous transhepatic catheter drainage when surgery had to be delayed because of additional diagnostic procedures or waiting lists,or in cases of cholangitis.Texture of the pancreatic remnant,diameter of the major pancreatic duct,operative time,intraoperative blood loss and blood transfusions were recorded for each patient.Moreover,we included the predictive prognostic score for major complications after PD,reported by Braga et al.[15]
Outcome measures were postoperative complications(both in-hospital regardless of total hospital stay and within 30 days following discharge to home),readmission rates(within 30 days from initial discharge),LOS and mortality.All patients were admitted the day before surgery.LOS was defined as the time interval,in full days,from the day of admission to discharge,during which the patient underwent PD.Mortality was defined as any death during hospitalization or within 30 days after surgery.Evaluated complications were pancreatic fistula(PF),DGE,postoperative hemorrhage,bile leak,intra-abdominal abscess,relaparotomy,wound infection and medical complications such as pneumonia and atrial fibrillation.PF was defined and graded according to the International Study Group on Pancreatic Fistula(ISGPF)criteria.[16]DGE was defined as prolonged nasogastric intubation lasting more than postoperative day 3(POD 3)or the need for reinsertion of a nasogastric tube due to persistent vomiting after POD 3,based on the definition of International Study Group of Pancreatic Surgery(ISGPS).[17]DGE was also classified into grades A,B and C according to the international definition.[17]Postoperative hemorrhage was defined and classified according to the definition of the ISGPS.[18]Postoperative complications were also graded according to the Clavien-Dindo classification,which was validated in pancreatic surgery.[19,20]Complications graded as IIIb to V were considered to be major.A follow-up for infectious and non-infectious complications was carried out for 30 days after hospital discharge.Interventions(CT-guided percutaneous drainage or endoscopy)were also recorded.
Essential elements of the ERAS protocol were preoperative counselling,no bowel preparation,short preoperative fasting,no preanesthetic medication,epidural analgesia,avoidance of excessive intravenous fluids perioperatively,effective control of pain,early reinstitution of oral feeding and drain removal,and immediate mobilization.Main postoperative protocol targets were as follows:nasogastric tube removal(POD 1),early mobilization(POD 1),resumption of oral fluids and liquid diet(POD 2),initiation of regular solid diet(POD 4),and drain removal(POD 5).Planned discharge was on POD 6.Details of the fast-track protocol are given in Table 1.Differences between the ERAS pathway and the conventional perioperative care protocol are outlined in Table 2.
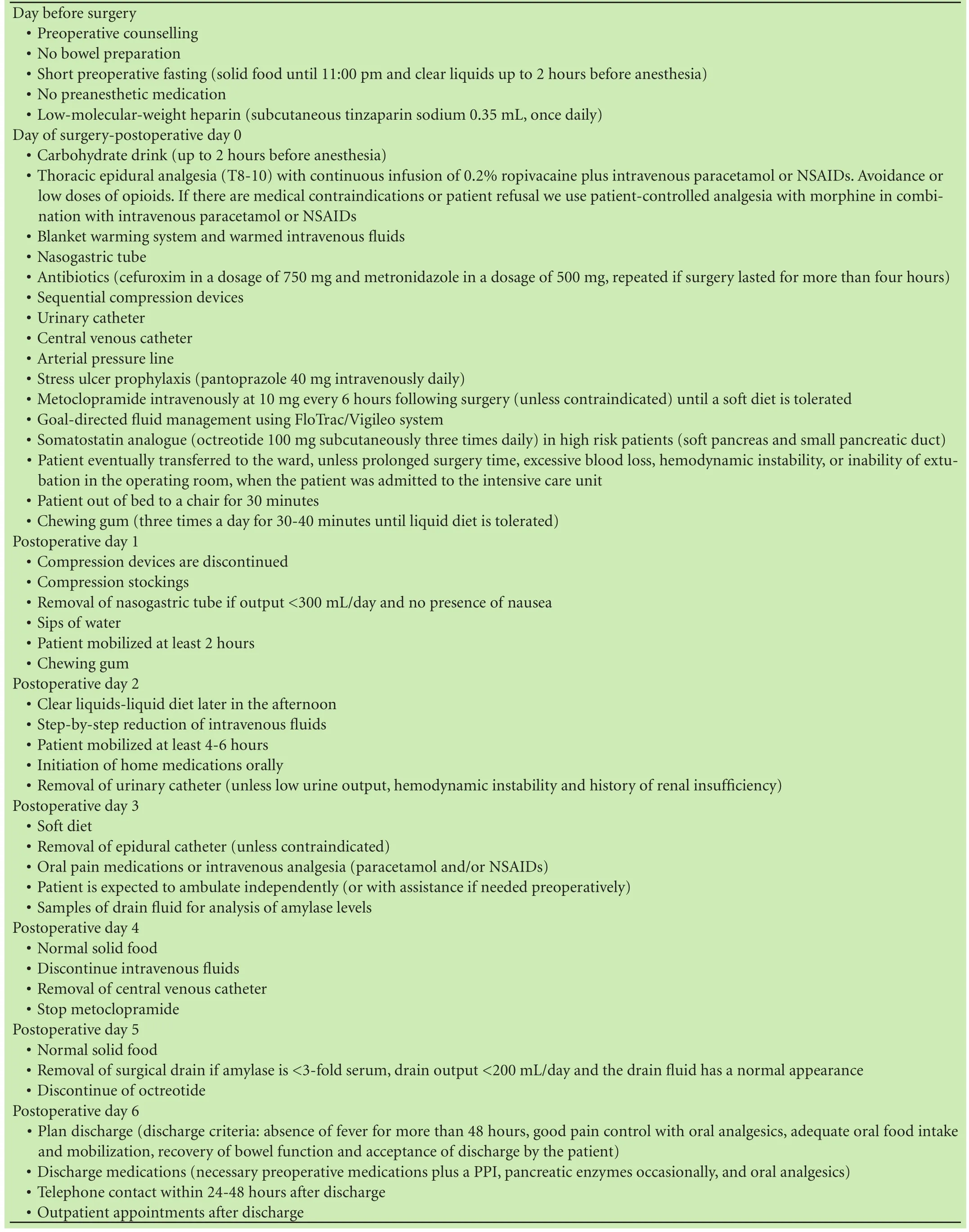
Table 1.Elements of ERAS protocol
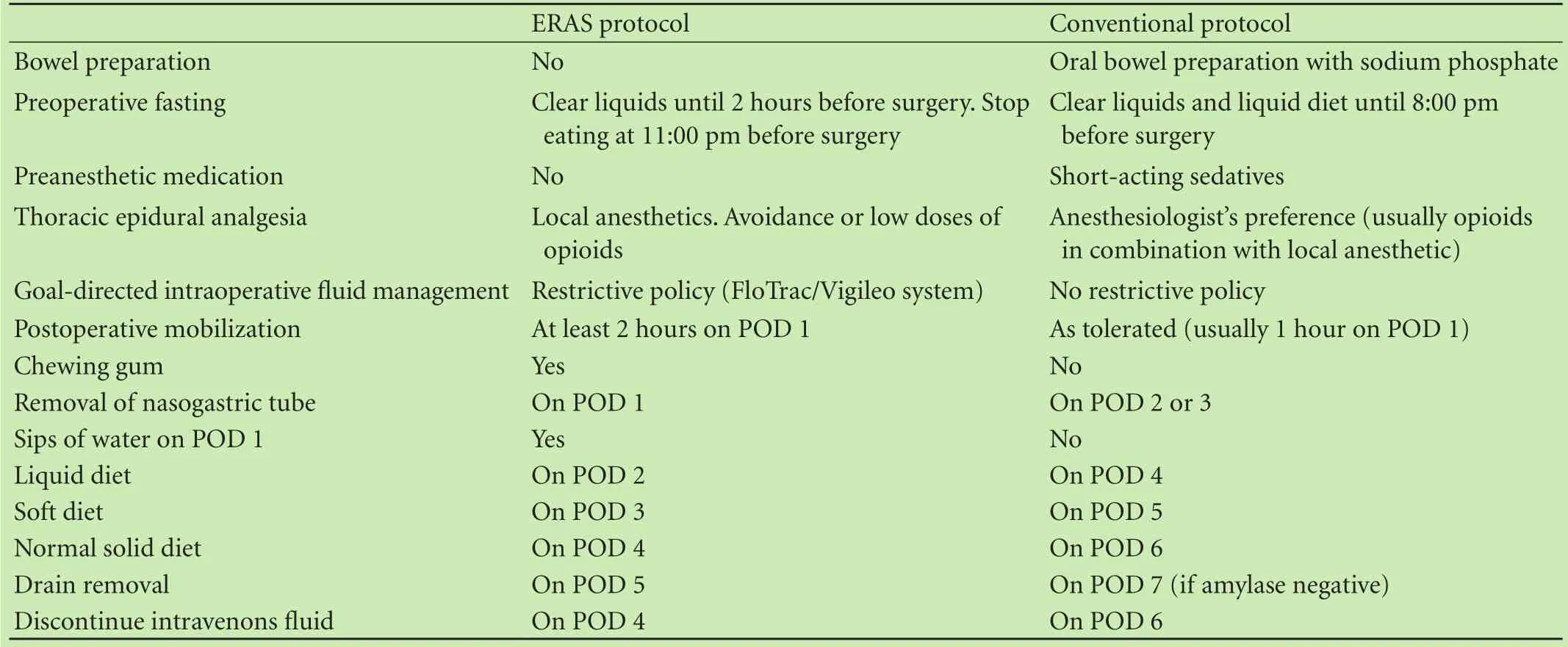
Table 2.Differences between ERAS and conventional protocol
Data are number(percent)of patients or mean± standard deviation(SD).SPSS version 19.0(SPSS,Chicago,IL)software was used for all analyses.Continuous variables were compared using the Mann-Whitney U test or the ANOVA test and categorical variables were compared using the Fisher’s exact test or the Chi-square as appropriate.Backward stepwise multiple logistic regression analysis used all those variables from the univariate analysis with P<0.1.Factors contributing to multicolinearity were excluded from the multivariate analysis.Adjusted odds ratios(aORs)and 95% confidence intervals(CIs)were calculated to evaluate the strength of any association.All statistic tests were two-tailed and P<0.05 was considered statistically significant.
Results
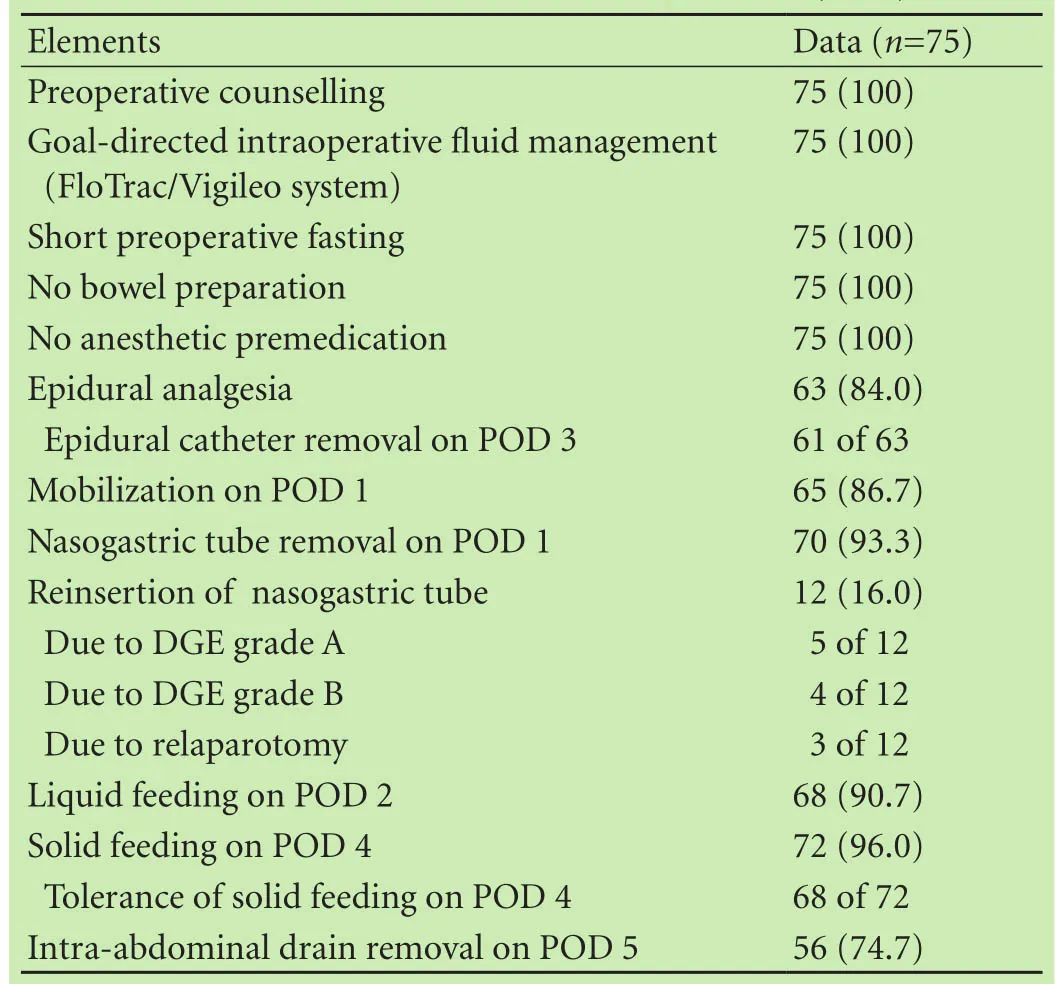
Table 3.Compliance with ERAS protocol(n,%)
Implementation of the ERAS protocol--compliance Compliance with preoperative counseling,goal-directed intraoperative fluid management,short preoperative fasting,and avoidance of bowel preparation and preanesthetic medication reached to 100%(Table 3).
Sixty-three(84.0%)patients received epidural analgesia.The epidural catheter was removed on POD 3 in 61 patients.In two patients who revealed prolonged prothrombin time,the catheter remained in situ until POD 4.Twelve(16.0%)patients were treated with patientcontrolled analgesia(PCA).In the latter group PCA was used as an alternative treatment modality because of medical contraindications(e.g.coagulopathy)or patient refusal.The nasogastric tube was removed on POD 1 in 70(93.3%)patients.Patients in whom the nasogastric tube was not removed on POD 1 had failed to meet the criteria of nasogastric tube removal(Table 1).The nasogastric tube was reinserted in a total of 12(16.0%)patients due to the occurrence of DGE grade A(5 patients),DGE grade B(4)and relaparotomy(3).Oral intake of clear liquids and liquid diet was resumed by POD 2 in 68(90.7%)patients and oral solid diet by POD 4 in 72(96.0%)patients.Early solid feeding was well tolerated in 68(94.4%)of 72 patients.Drain removal on POD 5 was carried out in 56(74.7%)patients.Delays were caused by not fulfilling the criteria for drain removal(Table 1)or by logistic problems(POD 5 was on a weekend day and drain removal was overlooked).Sixty-five(86.7%)patients achieved the target of mobilization on POD 1.Patients who failed to ambulate on POD 1 were weak(3 patients),hypotensive(5)or in pain(2).
Among the 75 patients of the FTG,53(70.7%)showed total adherence to the elements of the ERAS protocol,and the remaining 22(29.3%)had lower protocol compliance.The latter group,as compared with the former one,was associated with higher rates of postoperative complications in general(72.7% vs 20.8%;P<0.001).Hemodynamic instability due to epidural analgesia and early postoperative pain that resulted in delayed postoperative mobilization were also registered as complications in these subgroups.Patients with postoperative complications showed lower compliance with specific ERAS elements(Fig.).On the other hand,uneventful patients showed a significant higher adherence to the ERAS protocol(87.5% vs 40.7%;P<0.001).Moreover,patients with total adherence to the ERAS protocol also showed a shorter LOS(7.8±2.4 vs 14.4±7.8 days;P<0.001).Eight(10.7%)patients were discharged from our unit until POD 6,40(53.3%)until POD 7 and 49(65.3%)until POD 8.Discharge was delayed in a total of 23(30.7%)patients who were otherwise fit to leave the hospital due to social,transport or logistical issues(e.g.no discharge in weekends).

Fig.Compliance with postoperative ERAS elements with reference to the occurrence of complications.*:P<0.05,no complications vs complications.POD:postoperative day.
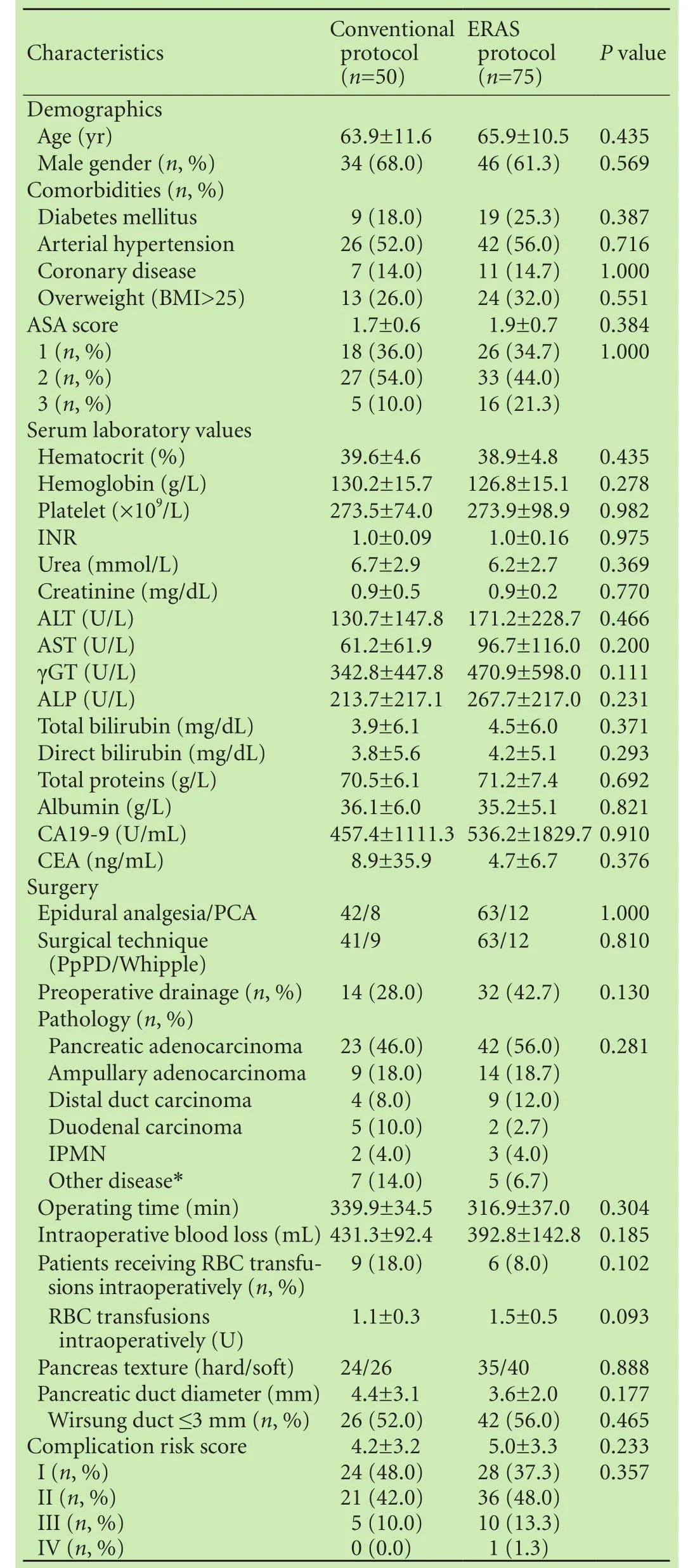
Table 4.Comparison of demographics,preoperative and intraoperative characteristics among the two groups
Postoperative outcomes
There was no significant difference in demographics,prognostic scores for complications after PD,preoperative and intraoperative characteristics between the FTG and CG(Table 4).Patients in the FTG had a shorter time to remove the nasogastric tube(1.1 vs 2.8 days;P<0.001),pass flatus(2.6 vs 3.8 days;P<0.001)and stools(3.5 vs5.2 days;P<0.001),and remove drains(6.9 vs 10.2 days;P<0.001).An oral diet was introduced earlier(liquid diet;2.4 vs 4.3 days;P<0.001 and solid diet;4.6 vs 6.1 days;P<0.001)in the FTG than in the CG(Table 5).
The rates of reoperation and intervention were similar between the two groups.But the mortality of the patients was not different significantly between the groups,nor the readmission rate(Table 5).Reoperation was necessary in four(5.3%)patients in the FTG and in two(4.0%)patients in the CG.Causes of reoperation were severe,late,intra-abdominal(grade C)hemorrhage(4 patients)and PF grade C(2)because of insufficiency of the pancreatojejunal anastomosis.Mortality occurred in three(4.0%)patients in the FTG and in two(4.0%)patients in the CG.Causes of death were PF grade C and multiple organ failure(1 patient)and severe,late,intraabdominal hemorrhage(grade C)(4).Overall,eight patients were readmitted in our unit within 30 days after initial discharge due to DGE grade B(3 patients),PF grade B(3),intra-abdominal abscess(1),and late(grade B)hemorrhage(1).
Overall morbidity rate,i.e.,the percentage of patients with at least one complication,was not different significantly between the two groups(36.0% FTG vs 50.0% CG;P=0.140).The occurrence of PF,postoperative hemorrhage,bile leak,intra-abdominal abscess,wound infection and medical complications(e.g.pneumonia and atrial fibrillation)were not changed significantly as time passed(Table 5).Moreover,the incidence of complications classified according to Clavien-Dindo classification was not different between the two groups.However,the DGE rate was significantly reduced in patients who received perioperative care with the ERAS protocol(12.0% vs 30.0%;P=0.019)(Table 5).LOS was also significantly reduced in the FTG(10.6 vs 14.3 days;P<0.001).LOS was different in the two groups because the patients who did not develop complications(7.3 vs 9.0 days;P<0.001),since the LOS of patients with complications was not different significantly among the groups(16.4 vs 19.6 days;P=0.211)(Table 5).
Since the percentage of patients who developed DGE was lower in the FTG,a second analysis was performed to determine the risk factors for DGE.The results of univariate analysis are shown in Table 6.Multivariate analysis revealed that the development of PF was significantly associated with DGE(P=0.048;aOR=2.9;95% CI:1.0-8.2),whereas the implementation of the ERAS protocol was a protective factor(P=0.022;aOR=0.34;95% CI:0.13-0.86).
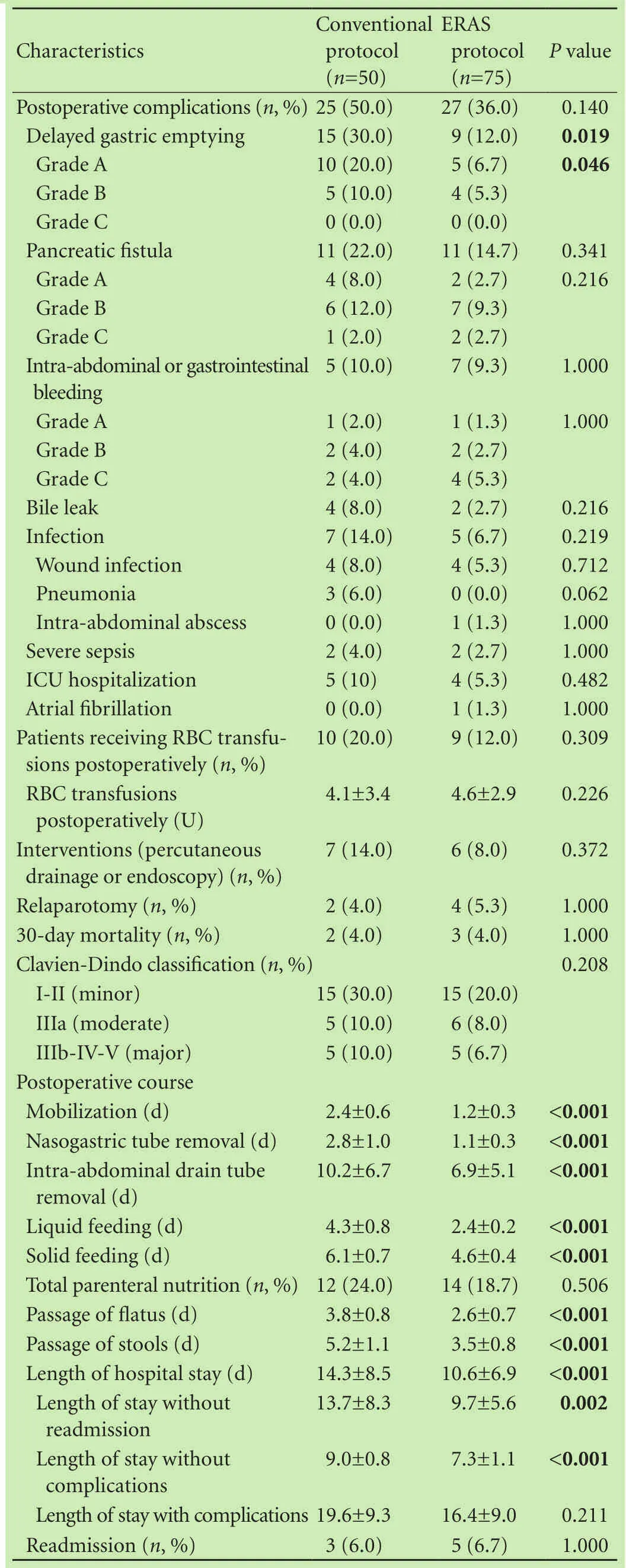
Table 5.Comparison of complications and outcomes among the two groups
Forty-seven(37.6%)patients had an LOS of more than 9 days.The results of univariate analysis of predictors for late discharge are shown in Table 7.Multivariate analysis revealed that the development of postoperativecomplications(P=0.001;aOR=9.2;95% CI:2.6-32.1)and the administration of total parenteral nutrition(P=0.004;aOR=11.7;95% CI:2.2-63.7)were significantly associated with a prolonged LOS,but the usage of the ERAS protocol(P=0.001;aOR=0.12;95% CI:0.04-0.42)was a predictor of a shorter LOS(Table 7).
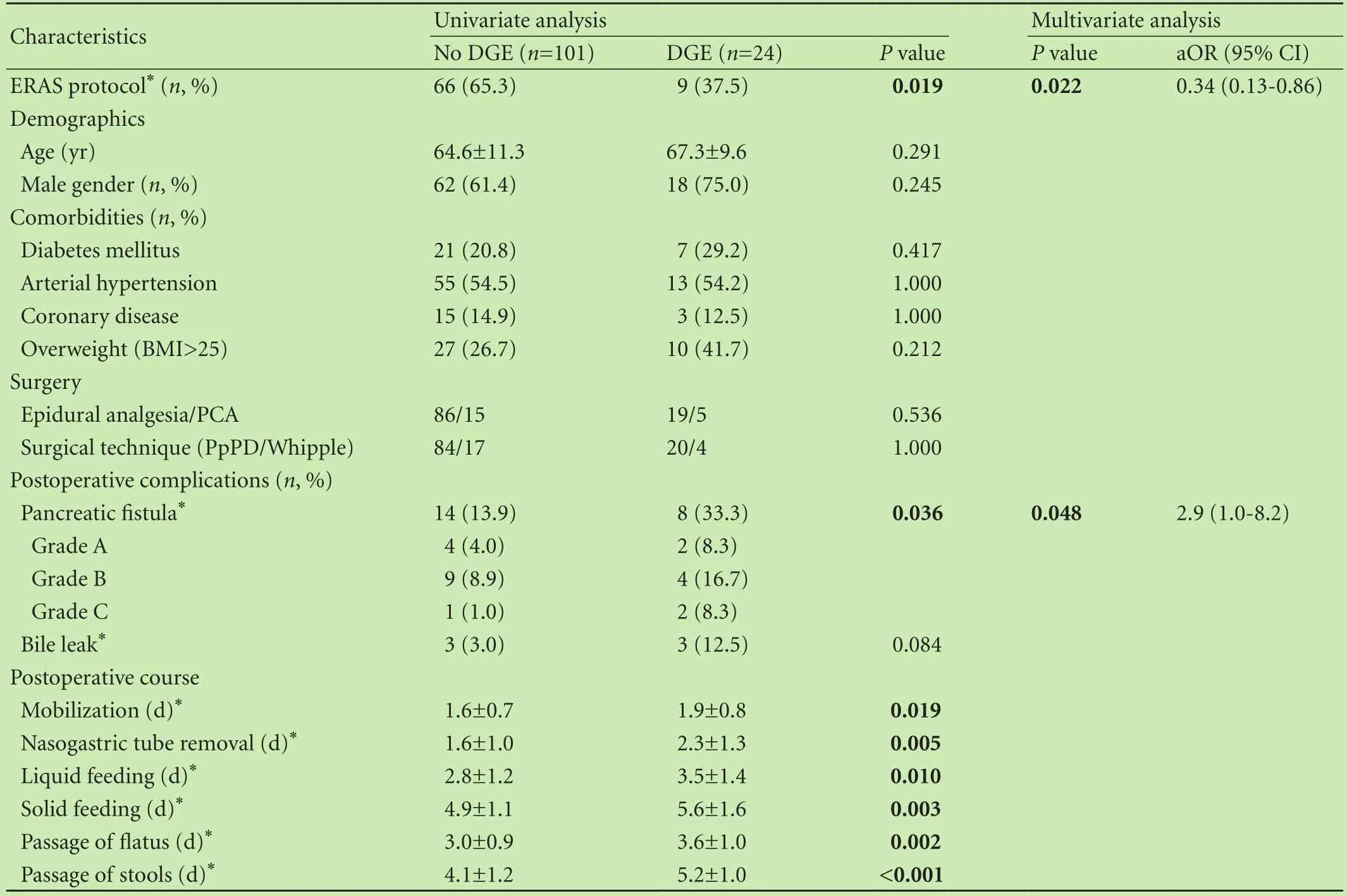
Table 6.Univariate and multivariate analyses of risk factors for the development of delayed gastric emptying
Discussion
PD is a complex surgical procedure that requires high standard perioperative care.Undoubtedly postoperative complications hamper the recovery after PD.However,several other factors delay convalescence after uncomplicated major abdominal surgery,including the need for parenteral analgesia(persistent pain)and bed rest(persistent lack of mobility and fatigue).Persistent gut dysfunction(postoperative ileus,nausea and vomiting)is another crucial factor that hinders recovery.[7,8]
On the plus side,hospitals are under increasing pressure to reduce costs without compromising quality and patient safety,which is also a crucial factor for the Greek health care system due to the recent financial crisis.The introduction of the ERAS(or fast-track)protocol is one approach to these challenges that has been adopted in different surgical procedures.[3,4,21,22]Relatively few studies have assessed the implementation of an ERAS program following PD,with varying results in terms of overall morbidity and DGE rate,whereas LOS and hospital costs were significantly reduced.[7,22-26]Moreover,a recent systematic review and meta-analysis reported that an ERAS program lowers LOS as well as costs and morbidity for PD.[14]
Inspired by the beneficial results of fast-track concepts in colon surgery and also by promising available data about the role of fast-track protocols in the setting of PD,we felt that the implementation of an ERAS pathway could improve outcomes at our center.Firstly,we would like to point out that the implementation of ERAS protocol was not associated with unpleasant consequences.On the contrary,preoperative counselling alleviates anxiety,facilitates patients’active participation during their perioperative period and helps to achievemain postoperative targets.[27,28]Lack of bowel preparation was not correlated with adverse-effect.Besides,studies[27,28]have demonstrated that mechanical bowel preparation causes dehydration and electrolyte imbalance,particularly in the elderly,and increases the risk for anastomotic leak.Early removal of the nasogastric tube was well tolerated by the majority of patients in the FTG and only five patients needed immediate reinsertion of the nasogastric tube due to DGE grade A.These results suggest that early removal of the nasogastric tube is safeand justified.Studies[27,28]have also demonstrated that nasogastric tube placement is,in fact,unnecessary in elective abdominal surgery and leads to pulmonary complications.Early removal of intraabdominal drain was not associated with any harmful effects.Abdominal cavity drainage was reported not to improve the incidence and severity of postoperative complications(such as anastomotic leakage)in colorectal and PD surgery.[29,30]However,PF is a potentially disastrous event and justifies the placement of an abdominal drain after PD.Further,it has been reported that early removal of a drain after PD is indicated,since long-remaining drains are associated with significantly more abscesses or fistulas during the postoperative course.[31,32]Finally,our study demonstrates that early normal food intake can also be achieved in pancreatic surgery without compromising DGE and morbidity rates.Many surgeons are still reluctant to apply early feeding after PD.The rationale of “nil by mouth”is to prevent postoperative nausea and vomiting and to protect anastomoses.However,early oral intake in patients after PD has been shown to be feasible and safe.[24,33]
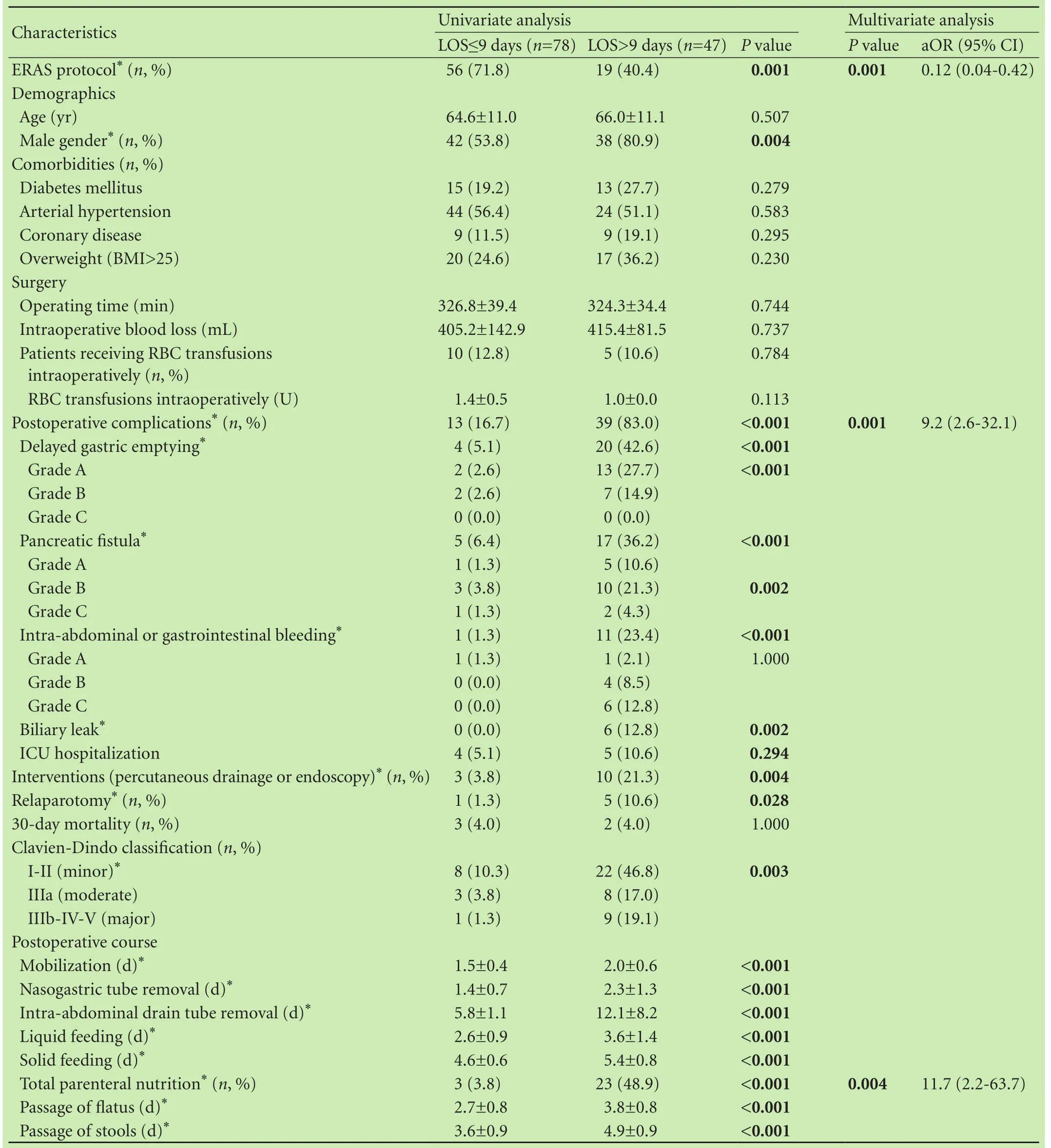
Table 7.Univariate and multivariate analyses of factors resulting in late discharge(length of hospital stay >9 days)
Data about adherence to ERAS items in PD are scarce.Most previous studies did not investigate compliance for each ERAS element.In our study,the rates of compliance with ERAS protocol elements suggest that fast-track management is feasible and safe.Moreover,the study demonstrates that patients with postoperative complications showed a significantly lower adherence to the ERAS protocol.In patients with a complicated postoperative course compliance to the postoperative elements of ERAS protocol is obviously less and sometimes even impossible.On the other hand,in uncomplicated patients compliance is easier and a shorter LOS seems feasible.
Patients in the FTG had also a significant shorter time to remove nasogastric tube,pass flatus,pass stools and remove drain.Mortality,readmissions and reoperations were not different significantly between the two groups.These results are in line with other reports on fast-track and PD.[7,11,23,26]We strongly believe that epidural analgesia with local anesthetics and lower doses of opioids in combination with goal-directed perioperative fluid management,early removal of nasogastric tube,early feeding and chewing gum is associated with an enhanced return of bowel activity as reported previously.[27,28,34,35]
Even though overall morbidity was not statistically significant between the two groups,there was a trend towards less complication rate in the FTG(36.0% vs 50.0%;P=0.140),which can be attributed to the statistically lower incidence of DGE in that group.Several reports on ERAS and PD also did not show an increase in morbidity after implementing an ERAS protocol,[11,13,23,26]whereas,two other reports showed a decrease in morbidity rates.[7,25]
DGE is a specific problem after PD occurring in 15%-30% of patients.[7,17]The majority of published studies on ERAS and PD failed to show a significant improvement in the rates of DGE.In the present study,patients in the FTG had less DGE than traditionally treated patients.The independent effect of the ERAS protocol in reducing DGE was confirmed by multivariate analysis.The present results are in line with a previous report by Balzano et al,[7]who demonstrated that an ERAS protocol with early mobilization,metoclopramide and removal of nasogastric tube on POD 1 or POD 2 decreased the rate of DGE.We applied this strategy to our ERAS protocol with favorable outcomes.A policy of standard use of metoclopramide in combination with dexamethazone and/or a serotonin receptor antagonist,especially in high risk patients,[28]to prevent postoperative nausea and vomiting after PD should be further investigated in PD surgery.Since then,the suggestions for patients undergoing colorectal surgery should be applicable to those undergoing PD as recommended by recently reported guidelines for perioperative care in patients undergoing PD.[28]
Multivariate analysis showed that prolonged LOS was independently associated with postoperative complications,whereas the use of ERAS protocol was a predictor of shorter LOS.Studies[7,11,25]on ERAS and PD have also reported improved LOS compared to historical controls.In our study,reduction in LOS was mainly due to patients without complications,where the difference between the FTG and CG was more profound.A recent retrospective study[9]has also demonstrated that fasttrack recovery was associated with shorter LOS after uncomplicated PD.However,Coolsen et al[11]reviewed 230 patients and found that improved LOS was probably a result of ERAS protocol and increased hospital volume over time rather than an effect of ERAS alone.Centralization of patients in specialized centers and higher hospital volume have significantly improved postoperative outcomes after PD.[11]In our center,the PD resection volume has increased significantly over the years.Hence,apart from the implementation of an ERAS protocol,another factor that might have contributed to shorter LOS was the increase in hospital volume of PD over the years and accompanying experience.
Inspired by the significant reduction of LOS after the introduction of ERAS protocols in colonic surgery,we considered that the established goal for patients to be discharged from hospital on POD 6,after the implementation of our protocol,could be reached.However,the proportion of patients who managed to discharge from hospital on POD 6 was low(10.7%).Moreover,none of the previous studies on ERAS and PD managed to reach such an ambitious LOS reduction.[7-13,23-26]We believe that higher morbidity rate in PD is the most crucial fac-tor that hampers the improvement of LOS in relation to colorectal surgery.Nevertheless,ERAS protocols have significantly reduced LOS after PD compared with historical controls.
Following this study and according to previously published data,[31,32]we should consider reducing the duration of drainage further in our hospital,especially in patients at low risk of PF.Furthermore,compliance rates to the ERAS protocol were good for nasogastric tube removal,nasogastric tube replacement and liquid as well as solid feeding.This gives some evidence that the nasogastric tube could be removed directly postoperatively,that liquid should be started as early as 6 hours postoperatively,and that solid food may be started on POD 2.[11,26]
The most important limitations of the present study include the fact that the study was not prospectively designed and also data from patients in the CG were collected retrospectively.However,the two groups were similar for all demographics,perioperative characteristics and prognostic scores for complications after PD.Studies[7,11,25]have also evaluated historical control groups of patients operated on years before fast-track groups.Moreover,the introduction of the ERAS pathway was the only change in the management of patients undergoing PD in our department and any differences in outcome can therefore be attributed to this variable.However,reduction in LOS might not solely be attributable to the introduction of the ERAS protocol,since the increase in volume and accompanying experience probably also has had its influence.On the other hand,data for patients in the FTG were collected prospectively during the study period and a prospective evaluation of compliance to ERAS protocol was performed.
The groups of patients in our study are relatively small.As far as we known our unit is the highest volume center for pancreatic diseases in Greece.Besides,the number of patients undergoing PD per institution is limited.Moreover,the study aimed to prove the safety and feasibility of an ERAS protocol in a unit specialized in pancreatic diseases.The results from this single-center study will be the base for future implementation of ERAS protocols in our department as well as multicenter studies in our country.The best evidence would be a randomized control trial comparing ERAS pathways with traditional care in PD,but this would be hard to do since the majority of ERAS elements have already been separately proven to be safe and effective in randomized control trials.[27,28,30,31,33,35]However,the role of ERAS pathways in the setting of PD remains ambiguous due to the heterogeneity of the implemented protocols.Moreover,feasibility must be ensured.Guidelines for perioperative care in patients undergoing PD have recently been published,[28]promoting the formation of a unified protocol that can be used in order to assess the feasibility and outcomes of ERAS protocol in multicenter studies.
In conclusion,the present study showed that DGE rates and LOS after PD were significantly reduced in our center within the last five years.A safe procedure in high volume centers still remains the most important factor for low mortality rates and early discharge.However,implementation of an ERAS protocol seems also to promote earlier discharge,particularly in patients with uneventful postoperative course,without compromising other outcomes,such as mortality,morbidity and readmissions.Hence,our results contribute to a growing body of evidence that a fast-track recovery protocol in PD is feasible,safe and plays a crucial role in patient recovery.
Acknowledgements:We thank Papadimitriou-Olivgeris Matthaios,MD,PhD,for his valuable work in statistical analysis and input in this article.
Contributors:ZE,LT,MA,PP and DC contributed to the conception and design.ZE and AC collected data.ZE wrote the manuscript.LT,MA,PP and DC did the critical revisions of the manuscript.ZE is the guarantor.
Funding:None.
Ethical approval:This study was conducted according to the Declaration of Helsinki and Good Clinical Practice Guidelines and was approved by the Ethics Committee of our hospital.
Competing interest:No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
References
1 Kehlet H.Fast-track colorectal surgery.Lancet 2008;371:791-793.
2 Gillissen F,Hoff C,Maessen JM,Winkens B,Teeuwen JH,von Meyenfeldt MF,et al.Structured synchronous implementation of an enhanced recovery program in elective colonic surgery in 33 hospitals in The Netherlands.World J Surg 2013;37:1082-1093.
3 Sammour T,Zargar-Shoshtari K,Bhat A,Kahokehr A,Hill AG.A programme of enhanced recovery after surgery(ERAS)is a cost-effective intervention in elective colonic surgery.N Z Med J 2010;123:61-70.
4 Adamina M,Kehlet H,Tomlinson GA,Senagore AJ,Delaney CP.Enhanced recovery pathways optimize health outcomes and resource utilization:a meta-analysis of randomized controlled trials in colorectal surgery.Surgery 2011;149:830-840.
5 Varadhan KK,Neal KR,Dejong CH,Fearon KC,Ljungqvist O,Lobo DN.The enhanced recovery after surgery(ERAS)pathway for patients undergoing major elective open colorectal surgery:a meta-analysis of randomized controlled trials.Clin Nutr 2010;29:434-440.
6 Ho CK,Kleeff J,Friess H,Büchler MW.Complications of pancreatic surgery.HPB(Oxford)2005;7:99-108.
7 Balzano G,Zerbi A,Braga M,Rocchetti S,Beneduce AA,Di Carlo V.Fast-track recovery programme after pancreaticoduodenectomy reduces delayed gastric emptying.Br J Surg2008;95:1387-1393.
8 Robertson N,Gallacher PJ,Peel N,Garden OJ,Duxbury M,Lassen K,et al.Implementation of an enhanced recovery programme following pancreaticoduodenectomy.HPB(Oxford)2012;14:700-708.
9 Nikfarjam M,Weinberg L,Low N,Fink MA,Muralidharan V,Houli N,et al.A fast track recovery program significantly reduces hospital length of stay following uncomplicated pancreaticoduodenectomy.JOP 2013;14:63-70.
10 Abu Hilal M,Di Fabio F,Badran A,Alsaati H,Clarke H,Fecher I,et al.Implementation of enhanced recovery programme after pancreatoduodenectomy:a single-centre UK pilot study.Pancreatology 2013;13:58-62.
11 Coolsen MM,van Dam RM,Chigharoe A,Olde Damink SW,Dejong CH.Improving outcome after pancreaticoduodenectomy:experiences with implementing an enhanced recovery after surgery(ERAS)program.Dig Surg 2014;31:177-184.
12 di Sebastiano P,Festa L,De Bonis A,Ciuffreda A,Valvano MR,Andriulli A,et al.A modified fast-track program for pancreatic surgery:a prospective single-center experience.Langenbecks Arch Surg 2011;396:345-351.
13 Nussbaum DP,Penne K,Stinnett SS,Speicher PJ,Cocieru A,Blazer DG 3rd,et al.A standardized care plan is associated with shorter hospital length of stay in patients undergoing pancreaticoduodenectomy.J Surg Res 2015;193:237-245.
14 Coolsen MM,van Dam RM,van der Wilt AA,Slim K,Lassen K,Dejong CH.Systematic review and meta-analysis of enhanced recovery after pancreatic surgery with particular emphasis on pancreaticoduodenectomies.World J Surg 2013;37:1909-1918.15 Braga M,Capretti G,Pecorelli N,Balzano G,Doglioni C,Ariotti R,et al.A prognostic score to predict major complications after pancreaticoduodenectomy.Ann Surg 2011;254:702-708.
16 Bassi C,Dervenis C,Butturini G,Fingerhut A,Yeo C,Izbicki J,et al.Postoperative pancreatic fistula:an international study group(ISGPF)definition.Surgery 2005;138:8-13.
17 Wente MN,Bassi C,Dervenis C,Fingerhut A,Gouma DJ,Izbicki JR,et al.Delayed gastric emptying(DGE)after pancreatic surgery:a suggested definition by the International Study Group of Pancreatic Surgery(ISGPS).Surgery 2007;142:761-768.
18 Wente MN,Veit JA,Bassi C,Dervenis C,Fingerhut A,Gouma DJ,et al.Postpancreatectomy hemorrhage(PPH):an International Study Group of Pancreatic Surgery(ISGPS)definition.Surgery 2007;142:20-25.
19 Dindo D,Demartines N,Clavien PA.Classification of surgical complications:a new proposal with evaluation in a cohort of 6336 patients and results of a survey.Ann Surg 2004;240:205-213.
20 DeOliveira ML,Winter JM,Schafer M,Cunningham SC,Cameron JL,Yeo CJ,et al.Assessment of complications after pancreatic surgery:A novel grading system applied to 633 patients undergoing pancreaticoduodenectomy.Ann Surg 2006;244:931-939.
21 Lemanu DP,Singh PP,Berridge K,Burr M,Birch C,Babor R,et al.Randomized clinical trial of enhanced recovery versus standard care after laparoscopic sleeve gastrectomy.Br J Surg 2013;100:482-489.
22 Porter GA,Pisters PW,Mansyur C,Bisanz A,Reyna K,Stanford P,et al.Cost and utilization impact of a clinical pathway for patients undergoing pancreaticoduodenectomy.Ann Surg Oncol 2000;7:484-489.
23 Kennedy EP,Rosato EL,Sauter PK,Rosenberg LM,Doria C,Marino IR,et al.Initiation of a critical pathway for pancreaticoduodenectomy at an academic institution--the first step in multidisciplinary team building.J Am Coll Surg 2007;204:917-924.
24 Berberat PO,Ingold H,Gulbinas A,Kleeff J,Müller MW,Gutt C,et al.Fast track--different implications in pancreatic surgery.J Gastrointest Surg 2007;11:880-887.
25 Kobayashi S,Ooshima R,Koizumi S,Katayama M,Sakurai J,Watanabe T,et al.Perioperative care with fast-track management in patients undergoing pancreaticoduodenectomy.World J Surg 2014;38:2430-2437.
26 Braga M,Pecorelli N,Ariotti R,Capretti G,Greco M,Balzano G,et al.Enhanced recovery after surgery pathway in patients undergoing pancreaticoduodenectomy.World J Surg 2014;38:2960-2966.
27 Gustafsson UO,Scott MJ,Schwenk W,Demartines N,Roulin D,Francis N,et al.Guidelines for perioperative care in elective colonic surgery:Enhanced Recovery After Surgery(ERAS?)Society recommendations.Clin Nutr 2012;31:783-800.
28 Lassen K,Coolsen MM,Slim K,Carli F,de Aguilar-Nascimento JE,Sch?fer M,et al.Guidelines for perioperative care for pancreaticoduodenectomy:Enhanced Recovery After Surgery(ERAS?)Society recommendations.Clin Nutr 2012;31:817-830.29 Karliczek A,Jesus EC,Matos D,Castro AA,Atallah AN,Wiggers T.Drainage or nondrainage in elective colorectal anastomosis:a systematic review and meta-analysis.Colorectal Dis 2006;8:259-265.
30 Conlon KC,Labow D,Leung D,Smith A,Jarnagin W,Coit DG,et al.Prospective randomized clinical trial of the value of intraperitoneal drainage after pancreatic resection.Ann Surg 2001;234:487-494.
31 Bassi C,Molinari E,Malleo G,Crippa S,Butturini G,Salvia R,et al.Early versus late drain removal after standard pancreatic resections:results of a prospective randomized trial.Ann Surg 2010;252:207-214.
32 Kawai M,Tani M,Terasawa H,Ina S,Hirono S,Nishioka R,et al.Early removal of prophylactic drains reduces the risk of intra-abdominal infections in patients with pancreatic head resection:prospective study for 104 consecutive patients.Ann Surg 2006;244:1-7.
33 Lassen K,Kjaeve J,Fetveit T,Tran? G,Sigurdsson HK,Horn A,et al.Allowing normal food at will after major upper gastrointestinal surgery does not increase morbidity:a randomized multicenter trial.Ann Surg 2008;247:721-729.
34 Lobo DN,Bostock KA,Neal KR,Perkins AC,Rowlands BJ,Allison SP.Effect of salt and water balance on recovery of gastrointestinal function after elective colonic resection:a randomised controlled trial.Lancet 2002;359:1812-1818.
35 Purkayastha S,Tilney HS,Darzi AW,Tekkis PP.Meta-analysis of randomized studies evaluating chewing gum to enhance postoperative recovery following colectomy.Arch Surg 2008;143:788-793.
Received May 17,2015
Accepted after revision September 11,2015
doi:10.1016/S1499-3872(16)60061-9
Corresponding Author:Efstratios Zouros,MD,Department of Surgery,“Konstantopouleio”(Agia Olga)General Hospital,3-5 Agias Olgas Str.,14233 Athens,Greece(Tel:+30-213-2057539;Fax:+30-213-2057541;Email:stratiszouros@gmail.com)
 Hepatobiliary & Pancreatic Diseases International2016年2期
Hepatobiliary & Pancreatic Diseases International2016年2期
- Hepatobiliary & Pancreatic Diseases International的其它文章
- OIder age at first birth is a risk factor for pancreatic cancer:a meta-anaIysis
- Pathologic response to preoperative transarterial chemoembolization for resectable hepatocellular carcinoma may not predict recurrence after liver resection
- Role of microRNA in liver regeneration
- An unusual case of prolonged post-endoscopic retrograde cholangiopancreatography jaundice
- Surgical treatment of synchronous colorectal liver and lung metastases:the usefulness of thoracophrenolaparotomy for single stage resection
- Monocyte chemoattractant protein-1,transforming growth factor-β1,nerve growth factor,resistin and hyaluronic acid as serum markers:comparison between recurrent acute and chronic pancreatitis