
Monocyte chemoattractant protein-1,transforming growth factor-β1,nerve growth factor,resistin and hyaluronic acid as serum markers:comparison between recurrent acute and chronic pancreatitis
2016-04-28 01:43:43GaneshKamathGaneshPaiAshaKamathandAnnammaKurienManipalIndia
M Ganesh Kamath,C Ganesh Pai,Asha Kamath and Annamma KurienManipal,India
?
Monocyte chemoattractant protein-1,transforming growth factor-β1,nerve growth factor,resistin and hyaluronic acid as serum markers:comparison between recurrent acute and chronic pancreatitis
M Ganesh Kamath,C Ganesh Pai,Asha Kamath and Annamma Kurien
Manipal,India
BACKGROUND:Diagnostic parameters that can predict the presence of chronic pancreatitis(CP)in patients with recurrent pain due to pancreatitis would help to direct appropriate therapy.This study aimed to compare the serum levels of monocyte chemoattractant protein-1(MCP-1),transforming growth factor-β1(TGF-β1),nerve growth factor(NGF),resistin and hyaluronic acid(HA)in patients with recurrent acute pancreatitis(RAP)and CP to assess their ability to differentiate the two conditions.
METHODS:Levels of serum markers assessed by enzymelinked immunosorbent assay(ELISA)were prospectively compared in consecutive patients with RAP,CP and in controls,and stepwise discriminant analysis was performed to identify the markers differentiating RAP from CP.
RESULTS:One hundred and thirteen consecutive patients(RAP=32,CP=81)and 78 healthy controls were prospectively enrolled.The mean(SD)age of the patients was 32.0(14.0)years;89(78.8%)were male.All markers were significantly higher in CP patients than in the controls(P<0.001);MCP-1,NGF and HA were significantly higher in RAP patients than in the controls(P<0.001).Stepwise discriminant analysis showed significant difference(P=0.002)between RAP and CP for resistin with an accuracy of 61.9%,discriminant scores of ≤-0.479 and ≥0.189 indicating RAP and CP,respectively.The other markers had no differential value between RAP and CP.
CONCLUSION:Serum resistin is a promising marker to differentiate between RAP and CP and needs validation in future studies,especially in those with early CP.
(Hepatobiliary Pancreat Dis Int 2016;15:209-215)
KEY WORDS:biological marker;
cytokine;
nerve growth factor;
transforming growth factor
pancreatitis;
resistin
Author Affiliations:Department of Physiology(Kamath MG)and Department of Pathology(Kurien A),Melaka Manipal Medical College,Manipal University,Manipal,India;Department of Gastroenterology and Hepatology(Pai CG)and Department of Community Medicine(Kamath A),Kasturba Medical College,Manipal University,Manipal,India
? 2016,Hepatobiliary Pancreat Dis Int.All rights reserved.
Published online October 30,2015.
Introduction
C hronic pancreatitis(CP)is characterized by inflammation and fibrosis of the pancreas resulting in irreversible damage to the organ.CP usually manifests as abdominal pain and loss of exocrine and endocrine pancreatic function and eventually increasing the risk of pancreatic cancer.[1]Conceptually,patients with acute pancreatitis(AP)recover their pancreatic function completely,as do those with two or more episodes of AP without evidence of permanent damage to the organ,defined as recurrent AP(RAP).[2]A variable proportion of patients with AP or RAP may eventually progress to CP,thereby manifesting progressive pancreatic damage and loss of function.[3]The full complement of factors that determine the progression from RAP to CP are poorly understood,but a persistent insult to the organ as happens with continuing alcohol consumption is clearly one.However,not all patients with alcohol abuse eventually develop CP.[4]Patients with CP often presentwith recurrent episodes of pain due to acute inflammatory episodes similar to RAP,especially early in the course of the disease.By definition,such patients already have permanent damage to the organ,but easily identifiable features of CP such as ductal dilatation,calcification,diabetes mellitus or steatorrhea may not be evident in many of them.[5]On the other hand,a reversible reduction in exocrine function or transient hyperglycemia in a patient with AP is not necessarily to imply the presence of underlying CP.[6,7]
Imaging techniques for evaluating the pancreas,such as endoscopic retrograde cholangiopancreatography(ERCP),ultrasonography(US),computed tomography(CT)and magnetic resonance imaging(MRI)usually detect late stages of CP.Endoscopic ultrasonography(EUS)is reported to have a high sensitivity,but may be lack of specificity or tend to over-diagnosis of CP.[8,9]The secretinpancreozymin test is considered the gold standard,but is cumbersome,poorly standardized,hardly used outside of research protocols and the exact role of newer simplified versions is unknown.[10]The availability of diagnostic parameters that would predict CP in patients who present with recurrent pain from pancreatitis would be of immense help to direct the appropriate interventions.For example,the option of pancreatic surgery available for patients with severe pain of CP is not appropriate for those with idiopathic RAP.Appropriate timely intervention in RAP might also prevent progression to CP.
Irrespective of the etiology,injury to the pancreas results in hyperproliferation and differentiation of fibroblasts into myofibroblasts with excessive synthesis and secretion of the extracellular matrix(ECM).ECM constitutes of proteins(proteoglycan and hyaluronan),sugars,collagens(fibrillar and non-fibrillar),and elastic fibers,and is important for the healing of wounds,homeostasis and development of cells.[11]The simultaneous remodeling of the ECM,a consequence of the quiescent pancreatic stellate cells(PSCs)getting “activated”,lays down fibrosis.[12]Activated PSCs secrete the enzyme matrix metalloproteinases(MMPs),which degrades ECM and tissue inhibitor of matrix metalloproteinase(TIMP),inhibiting MMPs.[12]An imbalance between the degradation and formation of ECM contributes to the abnormal ECM synthesis.[12]The necro-inflammation occurring in pancreatitis releases proinflammatory cytokines,transforming growth factor-β1(TGF-β1),platelet derived growth factor(PDGF),tumor necrosis factor-α(TNF-α),monocyte chemoattractant protein-1(MCP-1),interleukin-1(IL-1),and IL-6 which activate PSCs and promote pancreatic fibrosis.[13]The synthesis of glycosaminoglycan hyaluronic acid(HA)and other ECM proteins is stimulated by the presence of TGF-β1.[12,14]Nerve growth factor(NGF)and its neurotrophin receptor p75 are expressed on the PSCs during CP.[12,15]The levels of TGF-β1,MCP-1 and resistin are increased during inflammation in CP.[16,17]HA is a useful predictor of liver fibrosis and is also increased in CP.[5,18]Evaluation of such markers in the serum of patients would offer an attractive option to differentiate RAP from CP.This study aimed to compare the serum levels of MCP-1,TGF-β1,NGF,resistin and HA in patients with RAP and CP and to assess their predictive ability in differentiating the two conditions.
Methods
Patients and controls
All consecutive patients aged 18 years and above with RAP and CP presenting to the Department of Gastroenterology and Hepatology,Kasturba Hospital,Manipal between March 2011 and February 2013 for initial evaluation were qualified for the study.The study was approved by the Ethics Committee of Manipal University.Written informed consent was obtained from each participant.An episode of pancreatitis was defined by the presence of any two of typical upper abdominal pain,raised serum amylase and/or lipase and imaging evidence of pancreatitis.CP was diagnosed by the presence of pancreatic calcifications and/or ductal changes,visualized by US,CT,EUS,ERCP or MRCP;RAP was defined as more than one episode of AP in the absence of changes of CP.Patients with pancreatic cancer were excluded.Patients consuming ≥50 g of alcohol/day were considered to have alcoholic pancreatitis.[19]Patients with gallstones,hypercalcemia and hypertriglyceridemia were excluded from this study.Healthy controls matched for age were included to compare the serum markers with those in the patient group.
Sample collection
Three mL of whole blood was drawn by venipuncture into sterile vacutainer tubes(Becton Dickinson,New Jersey,USA)with no additive or clot activator.The tubes were allowed to stand undisturbed at room temperature for 15-30 minutes,centrifuged at 2000×g for 10 minutes the supernatant(serum)pipetted,apportioned into 0.5 mL aliquots and stored at -80 ℃ until enzyme-linked immunosorbent assay(ELISA)measurement.Stool samples were collected and immediately stored in a -80 ℃ freezer until analysis.
Exocrine and endocrine function tests
Fecal elastase-1 was assessed using the monoclonalantibody based commercial ELISA kit(ScheBo Biotech,Giessen,Germany)as per manufacturer’s instructions.Values less than 200 μg E1/g stool were considered as exocrine insufficiency.[20]Fasting blood glucose and glycated hemoglobin(HbA1c)levels were determined at index evaluation and diabetes mellitus was diagnosed based on the WHO criteria.[21]
Estimation of serum markers
The serum markers were determined by using commercially available ELISA kits for MCP-1(Yes Biotech Laboratories Ltd.,Canada),TGF-β1(Yes Biotech Laboratories Ltd.),NGF(Signosis,Inc.,Sunnyvale,CA,USA),resistin(Innovative Research,Novi,MI,USA)and HA(Echelon Biosciences Inc.,Salt Lake City,UT,USA)as per manufacturer.The normal range of serum markers was taken as per manufacturer:145-350 pg/mL for MCP-1,≤?200 ng/mL for TGF-β1,20-30 pg/mL for NGF,4-28 ng/mL for resistin,and ≤120 ng/mL for HA.
Statistical analysis
The SPSS version 15(SPSS South Asia,Bangalore,India)was used for statistical analysis.The continuous variables were expressed as mean(SD).Independent Student’s t test and the Chi-square test were used as appropriate.For skewed continuous variables,the data were expressed as median(interquartile range).The Kruskal-Wallis test was used to compare between the three groups and the Mann-Whitney U test was used to compare two groups.P<0.017 was considered as statistically significant with correction for type 1 error.Stepwise discriminant analysis was performed to identify the predictors differentiating RAP from CP.P<0.05 was considered as statistically significant.
Results
One hundred and twenty-two consecutive patients with pancreatitis were prospectively enrolled.Nine patients were excluded since blood samples could not be obtained,and finally 113 patients(RAP=32,CP=81)were left for analysis.The patient characteristics are shown in Table 1.The mean(SD)age of the patients was 32.0(14.0)years;89(78.7%)were male.The cause was alcohol in 8(25.0%)and 16(19.8%)patients with RAP and CP,respectively;no other cause was identified.The 78 healthy controls were at mean age of 32.4 years;65(83.3%)of them were male.

Table 1.Patient characteristics
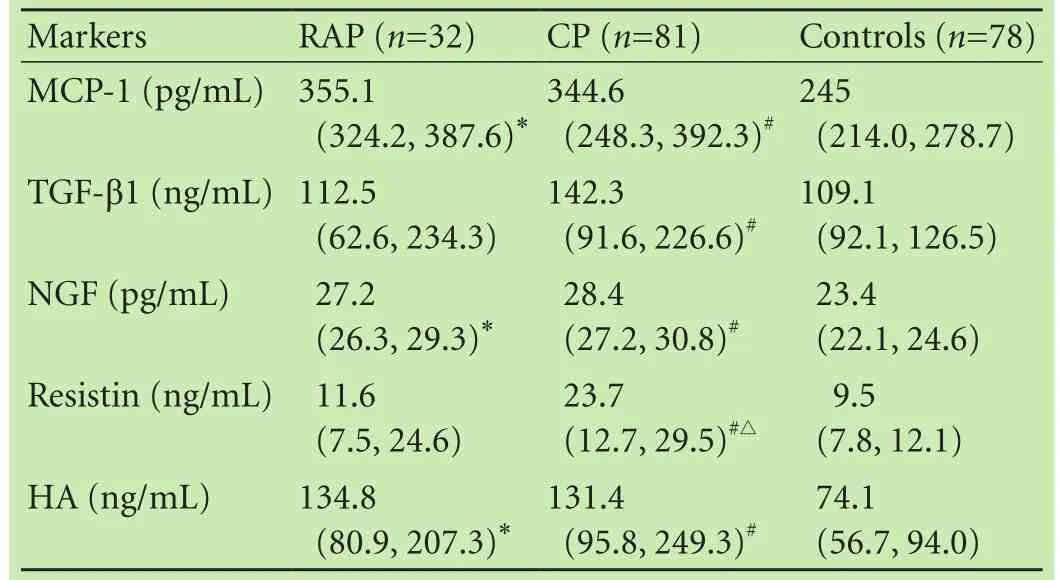
Table 2.Comparison of serum markers in RAP,CP and controls
Serum markers
The serum levels of MCP-1(P<0.001),TGF-β1(P=0.002),NGF(P<0.001),resistin(P<0.001),and HA(P<0.001)were significantly different between the controls,RAP and CP patients(the Kruskal-Wallis test).The median serum MCP-1 levels were significantly higher in the RAP and CP patients than in the controls(the Mann-Whitney U test,P<0.001);no significant difference was found between RAP and CP patients(P=0.133;Table 2).The median serum TGF-β1 showed no significant difference between the RAP patients and controls(P=0.481)and between RAP and CP patients(P=0.262),but it was significantly higher in the CP patients than in the controls(P<0.001 by the Mann-Whitney U test).Serum NGF levels were significantly higher in the RAP and CP patients than in the controls(P<0.001).Serum resistin levels showed no significant difference between the RAP patients and controls(P=0.080),but they were significantly higher in the CP patients than in the controls(P<0.001)and RAP patients(P=0.001).Serum HA levelswere significantly higher in the RAP and CP patients than in the controls(P<0.001).
Discriminant analysis between RAP and CP patients
The level of serum resistin was significantly different(P=0.002)between RAP and CP patients,with an accurate rate of 61.9% for differentiation between RAP and CP.The formulae for calculating discriminant scores were:resistin value obtained by ELISA×0.132-1.725 for RAP and resistin value obtained by ELISA×0.193-2.908 for CP.Using these discriminant scores we classified 19(23.5%)of the 81 CP patients as having RAP and 15(46.9%)of the 32 RAP patients as having CP.The discriminant scores of ≤-0.479 and ≥0.189 suggested RAP and CP respectively.MCP-1(P=0.193),TGF-1(P=0.487),NGF(P=0.215),and HA(P=0.410)were not significantly different between RAP and CP.
The combination of serum resistin levels with other serum markers was not effective in differentiating RAP from CP.The canonical correlation was 0.31 as against 0.29 with serum resistin alone.We also looked at the canonical correlation individually,combining each marker with resistin.Resistin combined with MCP-1 was 0.31,with TGF-β1 0.31,with NGF 0.30,and with HA 0.30.
Serum markers and exocrine insufficiency
The serum levels of MCP-1(P=0.49),TGF-β1(P=0.86),NGF(P=0.94),resistin(P=0.72)and HA(P=0.95)were not different between patients with RAP with and without exocrine insufficiency.Patients with CP and exocrine insufficiency had lower serum levels of MCP-1 than those without [302.6(234.0,383.4)and 359.0(317.7,411.6),respectively;P=0.02 by Mann-Whitney U test].A similar difference was not seen for the other markers in patients with CP with exocrine or without exocrine insufficiency(data not shown).
Serum markers and diabetes mellitus
There was no significant difference in the levels of serum markers in patients with RAP with or without diabetes mellitus as was the case in patients with CP(data not shown).
Discussion
Serum levels of MCP-1,TGF-β1,resistin and HA have been studied earlier as potential markers for the diagnosis of CP.[5,22-24]Among them,only MCP-1 is a serum marker for RAP.[24]NGF is up-regulated in the pancreas of experimental animals with CP and mediates pain,but its serum levels have not been assessed earlier in patients with RAP and CP.[25]We found that all these markers were raised in patients with CP,and three of them(MCP-1,NGF and HA)in RAP too,compared to controls.TGF-β1 and resistin levels were not elevated in RAP compared to controls,but only the resistin level was significantly different between RAP and CP.However,on discriminant analysis,the only predictor between the two disease conditions was serum resistin.Combining the levels of serum resistin with those of the other markers did not improve the yield.To our knowledge,this is the first study to assess these serum markers simultaneously in a large number of patients with RAP and CP of idiopathic and alcoholic etiology,and to address their predictive ability to differentiate RAP from CP.
The elevation in the serum levels of the mediators evaluated in this study in patients with RAP and CP is thought to reflect the changes of tissues in the two pancreatic diseases.Since inflammation occurs in all patients with RAP presenting with pain and in most patients with CP except possibly those with advanced “burnt out” disease,markers of inflammation are expected to be elevated in most if not all patients with these diseases.On the other hand,fibrosis is a definite feature of CP which is absent in patients with RAP because mediators of fibrosis are expected to be raised only in the former condition.
MCP-1,TGF-β1,NGF and HA have been shown to be increased in the pancreatic parenchyma when PSCs are activated during inflammation.[15,26]MCP-1,considered a serum marker of inflammation,especially in the liver,pancreas and other organs,is increased within the animal pancreas during acute inflammation and its serum levels appear to reflect the severity of pancreatitis.[27]Serum levels of MCP-1 have also been shown to increase in patients with RAP or CP in some but not all studies.[24,28]The elevation of MCP-1 in CP may also reflect the laying down of fibrosis,since the cytokine has been shown to mediate fibrosis by stimulating α smooth muscle actin in PSCs.[13,24,26]
TGF-β1,resistin and HA have been used as markers of fibrosis in patients with pancreatic disease.[5,22-24]In fact,these mediators also appear to have complex interactions among themselves and with other cytokines thus playing important roles in both inflammatory and fibrogenic processes directly or indirectly.For example,in vitro studies have shown that activated PSCs secrete TNF-α,MCP-1 and TGF-β1 among others during pancreatitis and thereby promote fibrosis.[13,29]Mice induced with recurrent episodes of AP showed evidence of TGF-β1 promoting fibrosis and providing valuable support to the necrosis-fibrosis hypothesis.[30]TGF-β1 exerts its fibrogenic effect in the pancreas by inducing the synthesis of ECM proteins specially laminin and HA.[12,14]Animal and human studies show increased expression of NGF in AP and during CP mediated by TGF-β1 and PSCs.[15,31]TGF-β1 induces NGF expression in PSCs.[15]Our resultsdocument a similar increase in the serum levels of NGF in patients with RAP and CP compared to the controls.
Peripancreatic fat necrosis has been shown to release several adipocytokines like visfatin,ghrelin,adiponectin,leptin,and resistin.[32]The adipocytokines augment the inflammatory process during AP and possibly RAP.[33]Resistin in particular is known to up-regulate MCP-1,IL-6,and most importantly TNF-α,which is activated via the NF-κB pathway.[34]TNF-α in turn activates the quiescent PSCs within pancreatic parenchyma resulting in laying down of fibrosis.[29]Human studies[23,35]have shown increased levels of serum resistin in patients with AP and CP.The resistin levels in RAP were found to be comparable to the controls in this study and the reason for this is not clear.One reason could be that the number of patients with RAP,and consequently the subgroup of those who are likely to progress to CP,was small.Further longitudinal studies are needed to clarify these issues in subgroups of patients with RAP who progress to CP and those who do not.
The reason for the significantly lower serum MCP-1 levels in patients with CP and exocrine insufficiency than in those without,is unclear.While the difference in exocrine function could be responsible,an alternative explanation is the difference in acute inflammation that is sometimes seen between the two subgroups.Patients with more advanced CP tend to have more functional impairment and less inflammation.Levels of TGF-β1 but not MCP-1 have previously been shown to be significantly different between early and late stages of CP and to correlate with exocrine function.[28]While exocrine and endocrine insufficiencies are not present in all patients with CP,transient abnormalities of these functions may be seen after an acute insult to the pancreas,and consequently in a variable proportion of patients with acute exacerbation of early chronic disease.Whether the different results between the two studies represent the fluctuating changes in pancreatic function due to varying inflammation relative to the time of drawing samples is unknown and needs further evaluation.Given the complex interactions discussed above,we found that resistin appears to be the best option for differentiating RAP from CP.However,the serum levels of the marker showed some overlap in the two conditions and the accuracy was only 61.9%.Further studies are needed to validate the clinical relevance of this finding in patients with RAP followed up prospectively for the development of early CP,and also to assess the usefulness of this marker in combination with other markers or imaging modalities such as EUS to differentiate the two conditions.
There is no gold standard for differentiating RAP from CP,we used imaging modalities including EUS to differentiate the two conditions.Secretin-pancreozymin test might be the better alternative to differentiate the two conditions,but it is expensive and invasive,and needs standardization and trained personnel.[10,36]
It cannot be forgotten that the progression of disease from RAP to CP may be a continuous process with time as an important variable,the division into the two categories thus being arbitrary and artificial.Nonetheless,it helps conceptually to classify patients in those whose pancreatic functions will recover completely and in those whose morphological,functional impairment is already established or is likely to appear in the near future.Thus interventions are considered to prevent such progression.
There are some limitations in the present study.Blood samples were drawn after the pain subsided from an acute episode of pancreatitis.In similar studies,the time of drawing blood samples in relation to the episode of pain was not standardized in our patients,and some of the patients were evaluated during a long intervening period between two episodes of pain.The effect of this time interval from the acute inflammatory event to the time of obtaining serum samples was unknown but this did influence our results.Whether the interval for better discrimination between RAP and CP should be standardized is unknown,but it appears likely.Including patients with AP or RAP as a disease control group would be interesting.Different thresholds for the intake of alcohol varying from ≥40 to ≥80 g/day implicate the cause of pancreatitis.[19,37-39]We chose to use the one which has been used most often.[40]
In summary,we found that serum resistin is a promising marker to differentiate RAP from CP.Further studies are needed to prospectively follow up patients and validate the use of this marker by itself or in combination with other markers or imaging modalities such as EUS to differentiate RAP from early CP.
Acknowledgements:We thank Mr.Vijay Kumar,lab assistant at Manipal AcuNova for helping in with the ELISA of the serum markers and Dr.Narayanan,for helping us obtain the final results from optical density values.
Contributors:PCG proposed the study.KMG and PCG wrote the first draft.KMG performed the research and Kurien A helped in analyzing the lab parameters.KMG collected the data and analyzed the data along with Kamath A.All authors contributed to the design and interpretation of the study and to further drafts.PCG is the guarantor.
Funding:The study was supported by a grant from the Indian Council of Medical Research(ICMR),New Delhi,India(No.5/4/3-5/10-NCD-II).
Ethical approval:The study was approved by the Ethics Committee of Manipal University.
Competing interest:No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
References
1 Mayerle J,Hoffmeister A,Werner J,Witt H,Lerch MM,M?ssner J.Chronic pancreatitis--definition,etiology,investigation and treatment.Dtsch Arztebl Int 2013;110:387-393.
2 Kedia S,Dhingra R,Garg PK.Recurrent acute pancreatitis:an approach to diagnosis and management.Trop Gastroenterol 2013;34:123-135.
3 Mariani A,Testoni PA.Is acute recurrent pancreatitis a chronic disease? World J Gastroenterol 2008;14:995-998.
4 Vonlaufen A,Wilson JS,Pirola RC,Apte MV.Role of alcohol metabolism in chronic pancreatitis.Alcohol Res Health 2007;30:48-54.
5 L?hr JM.What are the useful biological and functional markers of early-stage chronic pancreatitis? J Gastroenterol 2007;42:66-71.
6 Pezzilli R,Simoni P,Casadei R,Morselli-Labate AM.Exocrine pancreatic function during the early recovery phase of acute pancreatitis.Hepatobiliary Pancreat Dis Int 2009;8:316-319.
7 Das SL,Singh PP,Phillips AR,Murphy R,Windsor JA,Petrov MS.Newly diagnosed diabetes mellitus after acute pancreatitis:a systematic review and meta-analysis.Gut 2014;63:818-831.
8 Kahl S,Glasbrenner B,Leodolter A,Pross M,Schulz HU,Malfertheiner P.EUS in the diagnosis of early chronic pancreatitis:a prospective follow-up study.Gastrointest Endosc 2002;55:507-511.
9 Raman SP,Fishman EK,Lennon AM.Endoscopic ultrasound and pancreatic applications:what the radiologist needs to know.Abdom Imaging 2013;38:1360-1372.
10 Laterza L,Scaldaferri F,Bruno G,Agnes A,Bo?koski I,Ianiro G,et al.Pancreatic function assessment.Eur Rev Med Pharmacol Sci 2013;17:65-71.
11 Cox TR,Erler JT.Remodelling of the extracellular matrix:Implications for cancer.In:Schatten H,ed.Cell and molecular biology of breast cancer.New York:Springer;2013:65-90.
12 Patel M,Fine DR.Fibrogenesis in the pancreas after acinar cell injury.Scand J Surg 2005;94:108-111.
13 Apte MV,Wilson JS,Lugea A,Pandol SJ.A starring role for stellate cells in the pancreatic cancer microenvironment.Gastroenterology 2013;144:1210-1219.
14 Shek FW,Benyon RC,Walker FM,McCrudden PR,Pender SL,Williams EJ,et al.Expression of transforming growth factorbeta 1 by pancreatic stellate cells and its implications for matrix secretion and turnover in chronic pancreatitis.Am J Pathol 2002;160:1787-1798.
15 Haas SL,Fitzner B,Jaster R,Wiercinska E,Gaitantzi H,Jesnowski R,et al.Transforming growth factor-beta induces nerve growth factor expression in pancreatic stellate cells by activation of the ALK-5 pathway.Growth Factors 2009;27:289-299.
16 Adrych K,Smoczynski M,Stojek M,Sledzinski T,Korczynska J,Goyke E,et al.Coordinated increase in serum platelet-derived growth factor-BB and transforming growth factor-β1 in patients with chronic pancreatitis.Pancreatology 2011;11:434-440.
17 Marra F.Renaming cytokines:MCP-1,major chemokine in pancreatitis.Gut 2005;54:1679-1681.
18 Rossi E,Adams LA,Ching HL,Bulsara M,MacQuillan GC,Jeffrey GP.High biological variation of serum hyaluronic acid and Hepascore,a biochemical marker model for the prediction of liver fibrosis.Clin Chem Lab Med 2013;51:1107-1114.
19 Lankisch MR,Imoto M,Layer P,DiMagno EP.The effect of small amounts of alcohol on the clinical course of chronic pancreatitis.Mayo Clin Proc 2001;76:242-251.
20 Mariani A,Di Leo M,Petrone MC,Arcidiacono PG,Giussani A,Zuppardo RA,et al.Outcome of endotherapy for pancreas divisum in patients with acute recurrent pancreatitis.World J Gastroenterol 2014;20:17468-17475.
21 Alberti KG,Zimmet PZ.Definition,diagnosis and classification of diabetes mellitus and its complications.Part 1:diagnosis and classification of diabetes mellitus provisional report of a WHO consultation.Diabet Med 1998;15:539-553.
22 Sri Manjari K,Nallari P,Vidyasagar A,Jyothy A,Venkateshwari A.Plasma TGF-β1,MMP-1 and MMP-3 levels in chronic pancreatitis.Indian J Clin Biochem 2012;27:152-156.
23 Adrych K,Smoczynski M,Sledzinski T,Dettlaff-Pokora A,Goyke E,Swierczynski J.Increased serum resistin concentration in patients with chronic pancreatitis:possible cause of pancreatic fibrosis.J Clin Gastroenterol 2009;43:63-68.
24 Cavestro GM,Zuppardo RA,Bertolini S,Sereni G,Frulloni L,Okolicsanyi S,et al.Connections between genetics and clinical data:Role of MCP-1,CFTR,and SPINK-1 in the setting of acute,acute recurrent,and chronic pancreatitis.Am J Gastroenterol 2010;105:199-206.
25 Zhu Y,Colak T,Shenoy M,Liu L,Pai R,Li C,et al.Nerve growth factor modulates TRPV1 expression and function and mediates pain in chronic pancreatitis.Gastroenterology 2011;141:370-377.
26 Michalski CW,Gorbachevski A,Erkan M,Reiser C,Deucker S,Bergmann F,et al.Mononuclear cells modulate the activity of pancreatic stellate cells which in turn promote fibrosis and inflammation in chronic pancreatitis.J Transl Med 2007;5:63.
27 Zhou GX,Zhu XJ,Ding XL,Zhang H,Chen JP,Qiang H,et al.Protective effects of MCP-1 inhibitor on a rat model of severe acute pancreatitis.Hepatobiliary Pancreat Dis Int 2010;9:201-207.
28 Yasuda M,Ito T,Oono T,Kawabe K,Kaku T,Igarashi H,et al.Fractalkine and TGF-beta1 levels reflect the severity of chronic pancreatitis in humans.World J Gastroenterol 2008;14:6488-6495.
29 Mews P,Phillips P,Fahmy R,Korsten M,Pirola R,Wilson J,et al.Pancreatic stellate cells respond to inflammatory cytokines:potential role in chronic pancreatitis.Gut 2002;50:535-541.
30 Van Laethem JL,Robberecht P,Résibois A,Devière J.Transforming growth factor beta promotes development of fibrosis after repeated courses of acute pancreatitis in mice.Gastroenterology 1996;110:576-582.
31 Toma H,Winston J,Micci MA,Shenoy M,Pasricha PJ.Nerve growth factor expression is up-regulated in the rat model of L-arginine-induced acute pancreatitis.Gastroenterology 2000;119:1373-1381.
32 de Ferranti S,Mozaffarian D.The perfect storm:obesity,adipocyte dysfunction,and metabolic consequences.Clin Chem 2008;54:945-955.
33 Franco-Pons N,Gea-Sorlí S,Closa D.Release of inflammatory mediators by adipose tissue during acute pancreatitis.J Pathol 2010;221:175-182.
34 Jiang CY,Wang W,Tang JX,Yuan ZR.The adipocytokine resistin stimulates the production of proinflammatory cytokines TNF-α and IL-6 in pancreatic acinar cells via NF-κB activation.J Endocrinol Invest 2013;36:986-992.
35 Daniel P,Le?niowski B,Jasińska A,Pietruczuk M,Ma?ecka-Panas E.Usefulness of assessing circulating levels of resistin,ghrelin,and IL-18 in alcoholic acute pancreatitis.Dig Dis Sci2010;55:2982-2987.
36 Von Schassen H,Keller J,Layer P.Methods and principles of pancreatic function tests.In:Yang HC,Yeh WK,McCarthy JR,ed.Enzyme technologies:pluripotent players in discovering therapeutic agents.New Jersey:John Wiley &Sons;2013:336-337.
37 Yadav D,Whitcomb DC.The role of alcohol and smoking in pancreatitis.Nat Rev Gastroenterol Hepatol 2010;7:131-145.
38 Braganza JM,Lee SH,McCloy RF,McMahon MJ.Chronic pancreatitis.Lancet 2011;377:1184-1197.
39 Midha S,Singh N,Sachdev V,Tandon RK,Joshi YK,Garg PK.Cause and effect relationship of malnutrition with idiopathic chronic pancreatitis:prospective case-control study.J Gastroenterol Hepatol 2008;23:1378-1383.
40 Layer P,Yamamoto H,Kalthoff L,Clain JE,Bakken LJ,DiMagno EP.The different courses of early- and late-onset idiopathic and alcoholic chronic pancreatitis.Gastroenterology 1994;107:1481-1487.
Received January 27,2015
Accepted after revision July 3,2015
News
Zheng and Li’s innovative research group awarded At the annual National Science and Technology Award Conference held on January 8,2016 in the People’s Great Hall,Beijing,the Comprehensive Diagnosis and Treatment of End-stage Liver Disease Innovative Research Group from the First Affiliated Hospital,Zhejiang University School of Medicine,led by Professors Shu-Sen Zheng and Lan-Juan Li,was awarded the First prize for progress in science and technology.
In the past thirty years,the group has done remarkably in treating and conquering liver diseases.The application of Li’s Artificial Liver System has improved the survival of patients with end-stage liver diseases.The mortality of acute and subacute severe hepatitis decreased from 88.1% in the 1990s to 21.1% at the present,and that of chronic severe hepatitis from 84.6% to 56.6%.The finding of gut microflora changes in patients with end-stage liver diseases promotes the development of micro-ecology of liver diseases,and enriches the theory about the pathogenesis of the diseases.The Hangzhou criteria for selecting patients with hepatocellular carcinoma for liver transplantation,proposed by Professor Zheng,has been highly recognized by scientists from other countries,for instance,UCLA and Cleveland Clinic from USA.The 1-and 3-year survival rates of patients after liver transplantation are 88% and 78%,respectively.
Reported by Lei SY
Email:hbpdint@126.com
Representatives of the Innovative Research Team,the First Affiliated Hospital,Zhejiang University School of Medicine at the Tian’anmen Square,Beijing,January 9,2016.
doi:10.1016/S1499-3872(15)60029-7 10.1016/S1499-3872(16)60082-6)
Corresponding Author:C Ganesh Pai,MD,Department of Gastroenterology and Hepatology,Kasturba Medical College,Manipal University,Manipal 576014,India(Tel:+91-820-2922385;Fax:+91-820-2571934;Email:cgpai@yahoo.co.in)
 Hepatobiliary & Pancreatic Diseases International2016年2期
Hepatobiliary & Pancreatic Diseases International2016年2期
- Hepatobiliary & Pancreatic Diseases International的其它文章
- OIder age at first birth is a risk factor for pancreatic cancer:a meta-anaIysis
- Pathologic response to preoperative transarterial chemoembolization for resectable hepatocellular carcinoma may not predict recurrence after liver resection
- Role of microRNA in liver regeneration
- An unusual case of prolonged post-endoscopic retrograde cholangiopancreatography jaundice
- Surgical treatment of synchronous colorectal liver and lung metastases:the usefulness of thoracophrenolaparotomy for single stage resection
- Improvement of gastric emptying by enhanced recovery after pancreaticoduodenectomy