
Samaritan donor interchange in living donor liver transplantation
2014-05-04 02:52:34SeeChingChanKennethSHChokWilliamSharrAlbertCYChanSimonHYTsangWingChiuDaiandChungMauLo
See Ching Chan, Kenneth SH Chok, William W Sharr, Albert CY Chan, Simon HY Tsang, Wing Chiu Dai and Chung Mau Lo
Hong Kong, China
Samaritan donor interchange in living donor liver transplantation
See Ching Chan, Kenneth SH Chok, William W Sharr, Albert CY Chan, Simon HY Tsang, Wing Chiu Dai and Chung Mau Lo
Hong Kong, China
BACKGROUND:In order to overcome ABO blood group incompatibility, paired donor interchange has been practised in living donor liver transplantation. Liver transplantations using grafts donated by Samaritan living donors have been performed in Europe, North America, South Korea, and Hong Kong. Such practice is clearly on strong biological grounds although social and psychological implications could be far-reaching. Local experience has been satisfactory but is still limited. As few centers have this arrangement, its safety and viability are still being assessed under a clinical trial setting.
METHODS:Here we report a donor interchange involving an ABO-compatible pair with a universal donor and an ABO-incompatible pair with a universal recipient. This matching was not only a variation but also an extension of the donor interchange scheme.
RESULTS:The four operations (two donor hepatectomies and two recipient operations) were successful. All the two donors and the two recipients recovered well. Such donor interchange further supports the altruistic principle of organ donation in contrast to exchange for a gain.
CONCLUSIONS:Samaritan donor interchange certainly taxes further the ethical challenge of donor interchange. Although this practice has obvious biological advantages, such advantages have to be weighed against the potential increase in potential psychological risks to the subjects in the interchange. Further ethical and clinical evaluations of local and overseas experiences of donor interchange should guide future clinical practice in utilizing this potential organ source for transplantation.
(Hepatobiliary Pancreat Dis Int 2014;13:105-109)
orthotopic liver transplantation; living donor liver transplantation; right lobe
Introduction
The purpose of donor interchange in living donor liver transplantation (LDLT) is to circumvent ABO incompatibility as the 5-year recipient survival rate of LDLT with ABO incompatibility is only 52% even in a very experienced center.[1]LDLTs with donor interchange have been performed in Asia at two liver transplant centers only, according to the literature.[2, 3]Here we describe a case of donor interchange in Hong Kong, in which one pair of donor and recipient was in fact ABO-compatible. In order to render another pair of donor and recipient who were ABO-incompatible suitable for LDLT, donor interchange was decided. The ethical, surgical, and logistical challenges of this arrangement are discussed.
Case report
Pair 1
The recipient was a 57-year-old man of blood group AB (recipient 1), a universal recipient. He weighed 78 kg. He was a carrier of hepatitis B virus and had Child-Pugh B cirrhosis. He had sustained multiple episodes of esophageal variceal bleeding. Surveillance computed tomography (CT) showed a 4.4-cm hepatocellular carcinoma (HCC) in liver segment 6/7. Hepatectomy was prohibited by significant portal hypertension.
His 56-year-old wife volunteered as the living liver donor (donor 1). She weighed 47.5 kg and had an unremarkable medical history. She, with blood group O, is a universal donor. Her right liver volume on CT was 670 mL, accounting for 46% of her husband's standardliver volume.[4]Donor workup was per protocol. The usual upper age limit is 60 years but the limit can be extended slightly for very healthy subjects.[5]
Pair 2
The recipient was a 53-year-old man of blood group A (recipient 2), weighing 61 kg. He suffered from acute fl are of hepatitis B due to withdrawal of entecavir on his own. He had grade-2 hepatic encephalopathy with episodes of hypoglycaemia. His serum total bilirubin level was over 300 μmol/L and the international normalized ratio rose to 1.9. His Model for Endstage Liver Disease score was 22. Emergency liver transplantation was indicated.
His 47-year-old wife volunteered as the living liver donor (donor 2). She weighed 63.5 kg and her right liver volume was 851 mL on CT. She was evaluated as suitable for the donation except being ABO-incompatible because her blood group is B (Fig. 1).
Donor interchange workup
The two pairs underwent workup around the same time. The possibility of donor 1 donating to recipient 2 (blood group O to A) and donor 2 donating to recipient 1 (blood group B to AB) was raised and discussed with the two pairs. Pair 2 accepted the proposed arrangement of donor interchange readily as that rekindled their hope for a cure. The rationale of donor interchange was explained to Pair 1. After a day's pondering, they agreed to the proposal. The fact that the right liver graft from donor 2 would be larger than that from donor 1 was not disclosed.
The two pairs were interviewed and counselled by a clinical psychologist. Their ability to cope with this relatively novel arrangement was assessed. They were orientated to the idea that even though the wives intended to save their own husband, donating their liver to each other's husband was also altruistic, and that recipient 1's willingness to receive a liver not from his wife but from recipient 2's wife should also be reckoned as a Samaritan act despite the fact that he is an universal recipient. After the two potential LDLTs were approved by the local human organ transplant board, informed consent was obtained from the donor and the recipient of each potential LDLT, which was regarded as independent of the other LDLT as the donor interchange was supposed to be unconditional.
Early elective simultaneous LDLTs were arranged. Recipient 1 received donor 2's right liver. The graft which was 851 mL in volume on CT was 650 g as weighed on the back table. This weight was slightly less than expected, given the graft-volume-to-graft-weight conversion factor of 1.19 mL/g.[4]The graft-to-standardliver-volume (G/SLV) ratio was 45%. Histopathological examination of the liver excised from recipient 1 revealed an encapsulated HCC measuring 4.5×3.2× 4.0 cm with no evidence of vascular invasion. Recipient 2 received donor 1's right liver. The graft which was 670 mL on CT weighed 540 g. The G/SLV ratio was also 45%. The four people recovered satisfactorily. No recurrence of HCC was discovered in recipient 1 at one and a half year after transplantation.
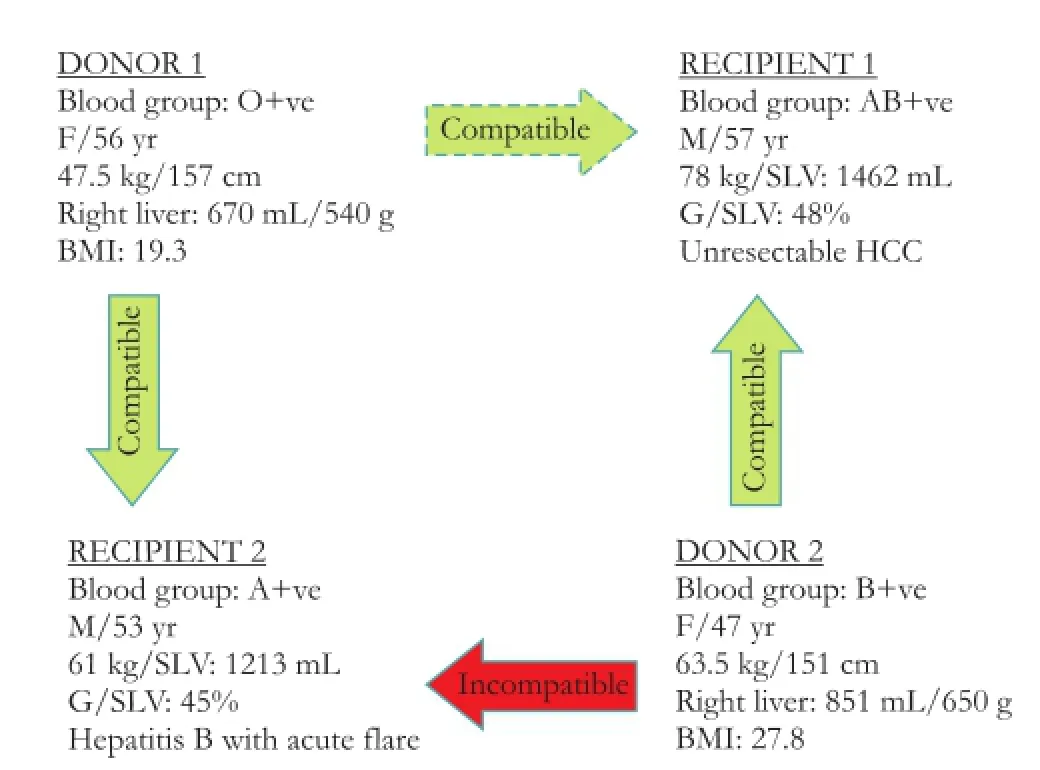
Fig. 1.Characteristics of the donors and recipients. G/SLV: graftto- standard-liver-volume.
Discussion
In Pair 1, there were a universal donor and a universal recipient. Such a pair of donor and recipient would allow donor interchange with another pair with any blood groups. Pair 1's Samaritan act enabled LDLT for Pair 2 who had blood groups A and B (Fig. 2). More commonly, both pairs in an interchange are ABO-incompatible, as in the example of 'A to B' and 'B to A' (Fig. 3). When the donor in one pair is a universal donor, the matchingis between the recipient in this pair and the donor in another pair (Fig. 4). For a pair with a universal recipient, the matching is that of the donor in this pair and the recipient in the other pair (Fig. 5).
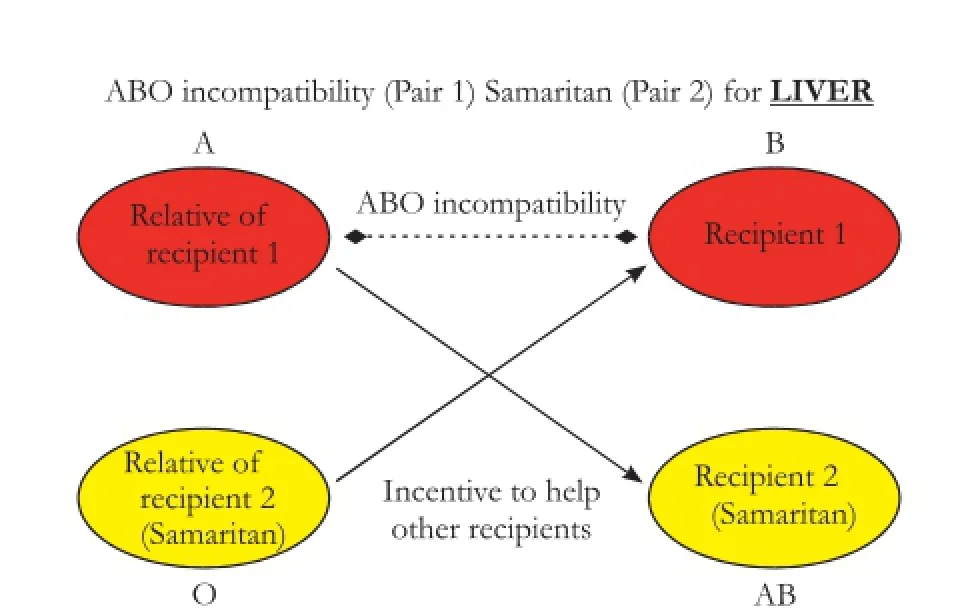
Fig. 2.Samaritan donor interchange with a universal donor and a universal recipient in one pair.
Donors are universally healthy. Nevertheless, donor risk could not always be equal in an interchange since remnant liver size and age of two donors are seldom identical though often comparable. The complication rate increases with the decrease in the size of the remnant liver.[6]Older donors tend to regret their donation afterwards.[7]On the other hand, recipients who suffer significant post-transplant complications tend to have poorer mental health after receiving the donation.[8]Equal survival of recipients cannot be achieved in every interchange. When a big survival difference between them is anticipated, particularly in short-term survival, it should be discussed in detail with all the four subjects in the interchange before they make their decision. Each of the two donations in an interchange should be taken as altruistic, and any failure regarding the transplantation of the recipient in a pair should not confer dissatisfaction to the original donor. A donation should be considered successful as the recipient survives. In the donor workup process in a regular LDLT, the potential donor is counselled to cope with failure of the recipient in case it happens, and his/ her ability in coping is assessed. In an LDLT with donor interchange, such counselling and assessment should be adjusted to the situation that the donor is facing two recipients, the original recipient whom he/she intends to donate to and the ultimate recipient receiving his/ her donation. Hoping that the two recipients in an interchange have exactly the same transplant outcome is unrealistic, but an exact estimation of discrepancy in recipient outcome should be strived for.
In the situation where one recipient's indication for transplantation is unresectable HCC, the chance of tumour recurrence should be estimated as accurate as possible. The estimation can be aided by an up-todate imaging study and positron emission tomography. The size, number and pathology of tumor definitely have a bearing on the rate of tumor recurrence.[9]Use of dual-tracer positron emission tomography enables identification of more aggressive HCC.[10]Hepatitis C patients are also very likely to have disease recurrence after liver transplantation. On the other hand, very ill patients with liver failure may fail in their transplantation with sepsis. All these kinds of anticipation should be explained explicitly to the four subjects before they make their decision.
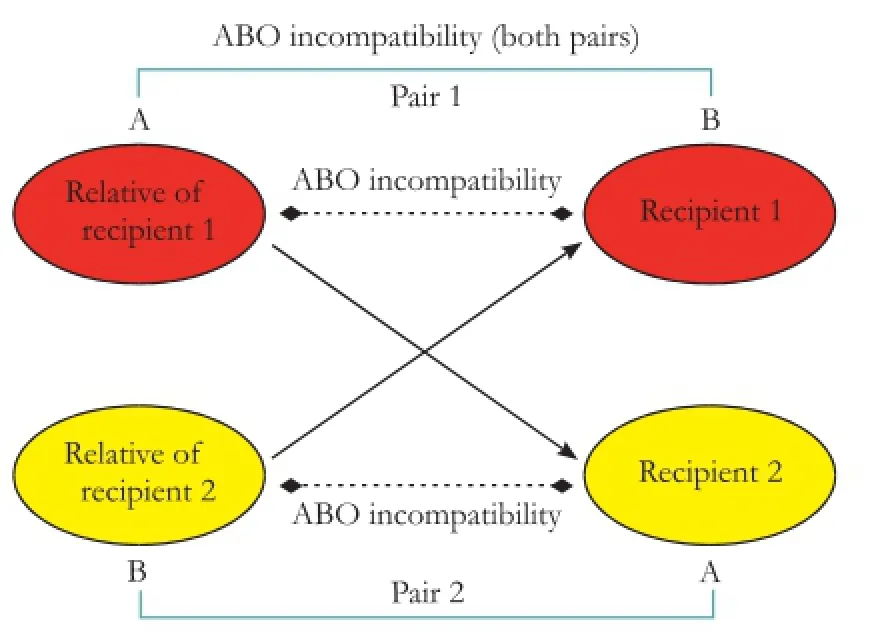
Fig. 3.Donor interchange between an A-to-B pair and a B-to-A pair.

Fig. 4.Samaritan donor interchange in which the universal recipient has an original donor whose blood group is the same as that of the recipient in the ABO-incompatible pair.
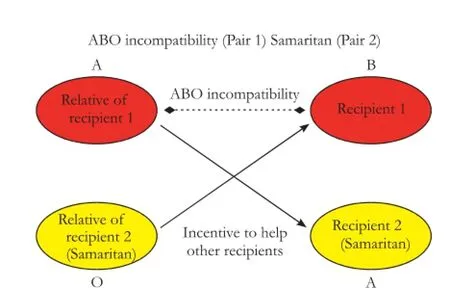
Fig. 5.Samaritan donor interchange in which the universal donor has an original recipient whose blood group is the same as that of the donor in the ABO-incompatible pair.
The local human organ transplant board regards LDLT with donor interchange as two separate cases and treats each of them independently. In the practical sense, once the two transplantations are commenced, albeit simultaneously, they are entirely independent. The progress of one should not affect the other. It could, however, be argued that the two transplantations need not be carried out simultaneously to minimize the logistical challenge to the surgical team. Non-simultaneous kidney transplantations have been performed sequentially for 10 recipients, started with an altruistic living donor. Provision was made for the possibility of the donor for the next kidney transplantation reneging. In such case, the recipient would enter another chain or paired donation.[11]This, however, should be less applicable to LDLT, which in most instances has to be done within a limited time frame. Moreover, the morbidity and mortality of donors and recipients in LDLT are many folds higher.
In LDLT with donor interchange, the two recipients often have dissimilar G/SLV ratios. Recipient survival should be similar if both G/SLV ratios are over 40%. Experience has shown that a liver graft with a G/SLV ratio over 40% is adequate for smooth recovery of the recipient. On the other hand, a G/SLV ratio below 35% significantly increases hospital mortality[12]and entails the chance of compromised graft survival as well as recipient survival. If preoperative assessment reveals a G/SLV ratio of less than 35%, it should be brought to the knowledge of all the subjects in the interchange and the issue of small-for-size graft should be discussed with them. A consensus on embarking on the interchange despite any unequal chance of survival should however be strived for. In the case reported herein, recipient 1 received a larger right liver graft from donor 2. Considering that both recipients were having a G/SLV ratio above 35% (in fact, both ratios were 45%), the fact that the two liver grafts would be different in size was not disclosed in the donor workup process in order not to introduce the idea of secondary gain.
In a desperate situation, a pair may consider an interchange which does not appear to be fair. In Ganga Ram Hospital of India, a mother with blood group A was so anxious for securing a liver transplantation for her 18-month old child who has blood group B that she donated her right liver to a 44-year-old woman of blood group A in exchange for an ABO-compatible left lateral section liver graft for her child from the woman's husband. The substantial difference in magnitude of the two donor operations, albeit equally life-saving, is not easy to understand. They could be viewed as two Samaritan donor operations and were not bounded by the need for comparability in donor risks (Soin et al, The Times of India, August 20, 2009). Another situation in donor interchange is that one donor's left liver as a remnant would be too small (<30%) for the donor yet large enough for the recipient in the other pair. There may also be a situation where one pair has a universal donor with a small body size while the ABO-incompatible pair has a small-sized recipient. The universal donor's donated portion of liver would be a small-for-size graft for the original recipient but a graft big enough for the recipient in the other pair. Donor interchange benefits both recipients by exempting one recipient from the possibility of small-for-size syndrome and allowing another recipient a transplantation by circumventing ABO incompatibility (Fig. 6).
In conclusion, donor interchange in LDLT is feasible although it requires additional effort in the workup process. The logistical challenge of performing four operations simultaneously can be overcome with adequate preparation and expertise accumulated from previous LDLTs. Donor interchange is reserved for very enthusiastic patients and should be performed only at expert centers of LDLT. The subjects in a donor interchange could feel dissatisfied and even regretful if adverse transplant outcomes occur. In order to minimize such unfavourable feelings, each of the two donations in a donor interchange should be deemed as a Samaritan act. This is also consistent with the legal requirement of LDLT.
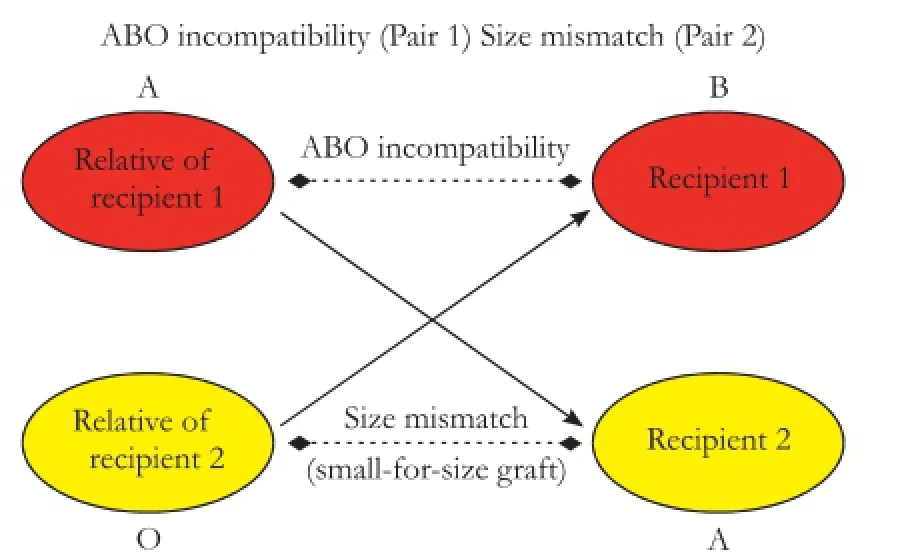
Fig. 6.Donor interchange between an ABO-incompatible pair and an ABO-compatible pair with a small-sized universal donor.
Contributors:CSC operated and drafted the manuscript. CKSH, SWW, CACY, DWC and LCM operated and revised the manuscript. TSHY revised the manuscript. CSC is the guarantor.
Funding:None.
Ethical approval:This study was approved by the local human organ transplant board. Informed consent was obtained from the donor and the recipient of each LDLT.
Competing interest:No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
1 Egawa H, Teramukai S, Haga H, Tanabe M, Fukushima M, Shimazu M. Present status of ABO-incompatible living donor liver transplantation in Japan. Hepatology 2008;47:143-152.
2 Hwang S, Lee SG, Moon DB, Song GW, Ahn CS, Kim KH, et al. Exchange living donor liver transplantation to overcomeABO incompatibility in adult patients. Liver Transpl 2010;16:482-490.
3 Chan SC, Lo CM, Yong BH, Tsui WJ, Ng KK, Fan ST. Paired donor interchange to avoid ABO-incompatible living donor liver transplantation. Liver Transpl 2010;16:478-481.
4 Chan SC, Liu CL, Lo CM, Lam BK, Lee EW, Wong Y, et al. Estimating liver weight of adults by body weight and gender. World J Gastroenterol 2006;12:2217-2222.
5 Chan SC, Fan ST, Liu CL, Lo CM, Lam BK, Lee EW. Working up donors for high-urgency and elective adult-to-adult live donor liver transplantation. Liver Transpl 2007;13:509-515.
6 Taner CB, Dayangac M, Akin B, Balci D, Uraz S, Duran C, et al. Donor safety and remnant liver volume in living donor liver transplantation. Liver Transpl 2008;14:1174-1179.
7 Chan SC, Liu CL, Lo CM, Lam BK, Lee EW, Fan ST. Donor quality of life before and after adult-to-adult right liver live donor liver transplantation. Liver Transpl 2006;12:1529-1536.
8 Kim-Schluger L, Florman SS, Schiano T, O'Rourke M, Gagliardi R, Drooker M, et al. Quality of life after lobectomy for adult liver transplantation. Transplantation 2002;73:1593-1597.
9 Mazzaferro V, Llovet JM, Miceli R, Bhoori S, Schiavo M, Mariani L, et al. Predicting survival after liver transplantation in patients with hepatocellular carcinoma beyond the Milan criteria: a retrospective, exploratory analysis. Lancet Oncol 2009;10:35-43.
10 Cheung TT, Chan SC, Ho CL, Chok KS, Chan AC, Sharr WW, et al. Can positron emission tomography with the dual tracers [11 C]acetate and [18 F]fludeoxyglucose predict microvascular invasion in hepatocellular carcinoma? Liver Transpl 2011;17:1218-1225.
11 Rees MA, Kopke JE, Pelletier RP, Segev DL, Rutter ME, Fabrega AJ, et al. A nonsimultaneous, extended, altruisticdonor chain. N Engl J Med 2009;360:1096-1101.
12 Fan ST, Lo CM, Liu CL, Yong BH, Wong J. Determinants of hospital mortality of adult recipients of right lobe live donor liver transplantation. Ann Surg 2003;238:864-870.
Received November 19, 2012
Accepted after revision June 4, 2013
Author Affiliations: Department of Surgery (Chan SC, Chok KSH, Sharr WW, Chan ACY, Tsang SHY, Dai WC and Lo CM); and State Key Laboratory for Liver Research (Chan SC and Lo CM), The University of Hong Kong, 102 Pokfulam Road, Hong Kong, China
See Ching Chan, Li Shu Fan Medical Foundation Professor in Surgery, Department of Surgery, The University of Hong Kong, 102 Pokfulam Road, Hong Kong, China (Tel: 852-22553025; Fax: 852-28175475; Email: seechingchan@gmail.com)
? 2014, Hepatobiliary Pancreat Dis Int. All rights reserved.
10.1016/S1499-3872(14)60016-3
 Hepatobiliary & Pancreatic Diseases International2014年1期
Hepatobiliary & Pancreatic Diseases International2014年1期
- Hepatobiliary & Pancreatic Diseases International的其它文章
- lntrahepatic Glissonian approach and outflow vascular occlusion during partial hepatectomy
- Complex hepatic outflow reconstruction in domino liver transplantation
- Novel en-bloc resection of locally advanced hilar cholangiocarcinoma: the Rex recess approach
- KAI1 inhibits lymphangiogenesis and lymphatic metastasis of pancreatic cancer in vivo
- Effect of CD74 on the prognosis of patients with resectable pancreatic cancer
- Blood group type antigens in pancreatic intraductal papillary mucinous neoplasms