
Ultrasonic integrated backscatter in assessing liver steatosis before and after liver transplantation
2014-05-04 07:37:09HanTengYangKeFeiChenQiangLuYongGangWeiBoLiYangQinandWenQingHuang
Han-Teng Yang, Ke-Fei Chen, Qiang Lu, Yong-Gang Wei, Bo Li, Yang Qin and Wen-Qing Huang
Chengdu, China
Ultrasonic integrated backscatter in assessing liver steatosis before and after liver transplantation
Han-Teng Yang, Ke-Fei Chen, Qiang Lu, Yong-Gang Wei, Bo Li, Yang Qin and Wen-Qing Huang
Chengdu, China
BACKGROUND:Liver steatosis affects 20%-30% of adults. Because of the increasing gap between graft supplies and demands, livers with steatosis are frequently used in liver transplantation. But severely steatotic liver grafts are associated with a high risk of intraoperative and postoperative complications. Accurate assessment of fat content of donor livers and monitoring of the extent of steatosis in recipients are required for liver transplantation. The present study aimed to determine the correlation between liver echogenicity and fat content, and to evaluate the use of an ultrasonic integrated backscatter system (IBS) in the assessment of changes in fat content after liver transplantation.
METHODS:Seventy-nine consecutive patients receiving liver grafts from living donors were evaluated in our center. Of these recipients, 67 survived for more than two years and were included in this study. Each liver graft was evaluated with IBS and ultrasound before operation and the fat content was estimated. The fat content of the grafts in the recipients was again assessed with ultrasound at 18 months after surgery.
RESULTS:A correlation was detected between each graft's IBS value and its fat content (P=0.001). The IBS value in fatty grafts with various degrees of steatosis was significantly decreased in 3 (P=0.02), 12, 15 and 18 (P=0.001) months after orthotopic liver transplantation. The IBS value returned to normal in all patients in 18 months after liver transplantation.CONCLUSIONS:Decreased fat content in steatotic grafts can be observed in all recipients. Ultrasonic IBS is useful in determining the steatotic degree of grafts in donors as well as in monitoring the grafts after liver transplantation.
(Hepatobiliary Pancreat Dis Int 2014;13:402-408)
fat content;
fatty liver;
liver transplantation;
ultrasonic integrated backscatter
Introduction
Liver steatosis affects 20%-30% of adults.[1-3]Because of the growing need for liver grafts and the shortage of liver donors, livers with steatosis are frequently used in liver transplantation. While grafts with a mild degree of steatosis are used and grafts with a moderate degree of steatosis are also used with caution in liver transplantation. Most surgeons hesitate to use a graft with severe steatosis, as severe steatosis is associated with higher rates of primary graft dysfunction, renal failure and major complications.[4]With the development of surgical techniques for living donor liver transplantation, more patients acquire the opportunity to receive a liver graft from their relatives. However, experimental animals and human studies demonstrated that a larger graft/recipient weight ratio is needed for a better chance of successful steatotic liver graft transplantation.[5,6]As such, accurate assessment of the fat content of donor livers and monitoring of the extent of steatosis in recipients are required for liver transplantation.
It has been reported that severely steatotic liver grafts are associated with a high risk of intraoperative and postoperative complications.[7]However, two casecontrol studies independently revealed that neither thegraft survival rate nor recipient survival was significantly different between the patients receiving the grafts with severe steatosis and those with moderate steatosis.[8,9]Moon et al[10]reported two cases of rapid resolution of severe graft steatosis following dual-graft living donor liver transplantation. If these observations are not by chance, the decrease of fat content may at least partially explain why steatotic grafts have a comparable survival rate.
In light of these findings, we used an ultrasonic integrated backscatter system (IBS) to evaluate the degree of the fat content of the grafts. IBS has been used over the past couple of decades as an innovative quantitative approach in ultrasonic assessment. Reflection occurs when the ultrasound waves hit an interface between two substances with different degrees of resistance. Thus, the ultrasound is scattered when the interface is significantly thinner than the wavelength of the ultrasound. The directly reversing scattered waves can be detected by a sensor. The conventional method used in the ultrasound diagnosis processes merely assesses the reversed wave signals. IBS, on the other hand, processes part of the ultrasound emitted and the circuit received. More precisely, the reversed highfrequency pulse ultrasound wave received by a sensor is filtered and amplified. IBS has been widely used in the assessment of liver, kidney and heart diseases.[11-13]
The present study was to investigate whether the resolution of steatosis also occurs in steatotic grafts in 18 months after liver transplantation, and also to verify that ultrasonic integrated backscatter is a good modality for detecting subtle pathological changes in fatty liver.
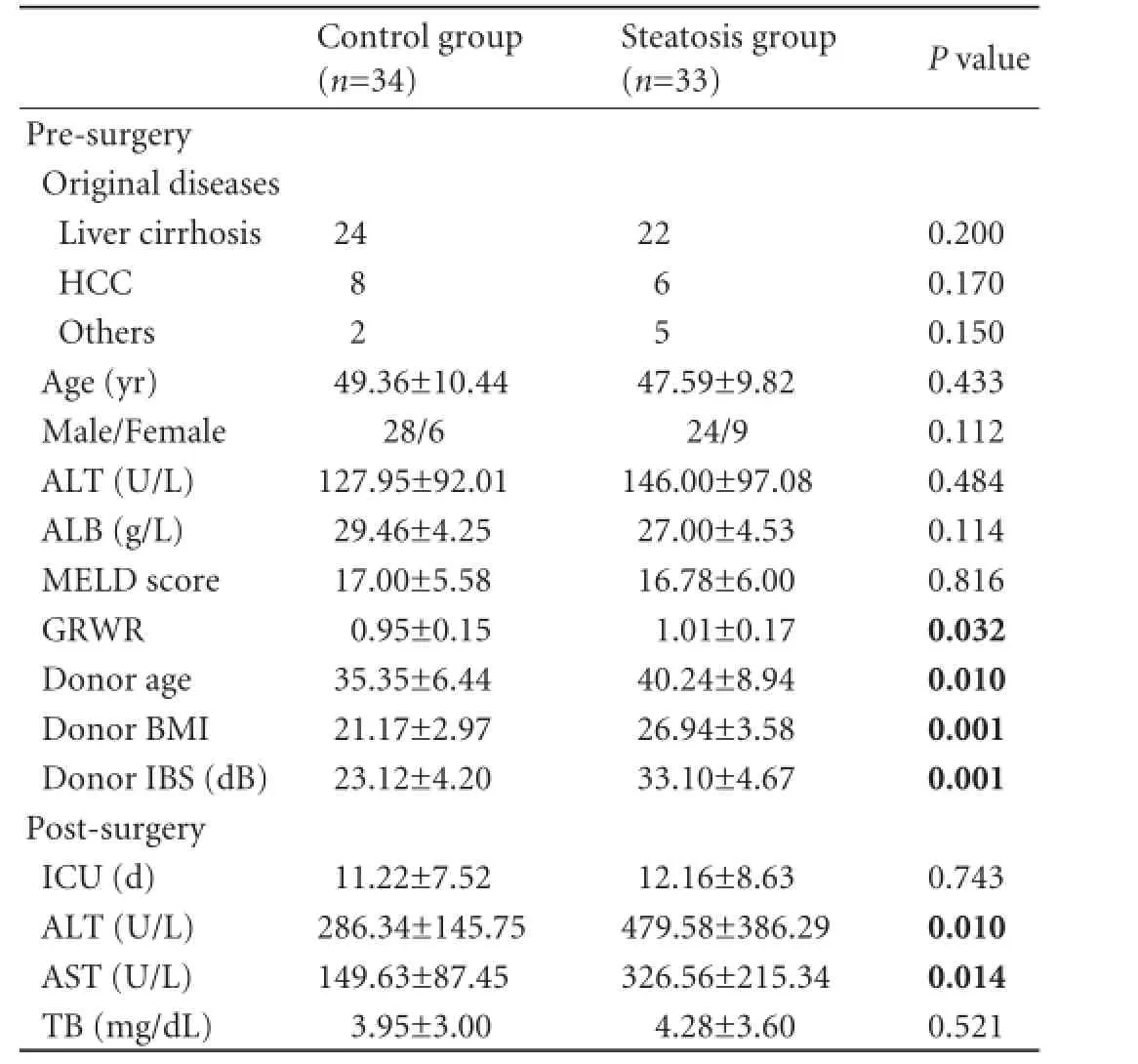
Table.Patients and graft status pre-surgery and one week posttransplantation
Methods
Patients and liver graft samples
Between May 2003 and April 2007, 79 consecutive patients received liver grafts from living donors for liver transplantation in our center. Of these recipients, 67 survived for more than two years were included in this study (Table). The age of the donors ranged from 20 to 65 years, with an average of 37.99±8.13 years, and that of the recipients ranged from 4 to 70 years, with an average of 48.31±10.09 years. Before a graft was implanted, one piece of liver tissue with a diameter of 0.5-1.0 cm (weighing 0.089-0.289 g) was removed from the front edge of the lateral leaf of the right liver lobe and was cut into two pieces of equal volume. One piece was immediately weighed, snap frozen in liquid nitrogen and stored at -80 ℃ for further staining with hematoxylin and Sudan III and pathological analysis of the steatotic type. The other was used for the assessment of fat content via the chloroform-methanol extraction method. The samples were analyzed at the same time under the same conditions. The grafts were divided into two groups according to their fat content: steatosis group (n=33) in which the grafts had fat content ≥5% and control group (n=34) in which the grafts had fat content <5% (Table).
This work was carried out in accordance with theDeclaration of Helsinki(2000) of the World Medical Association. All patients involved in the study offered written informed consent.
Ultrasound
All study data were acquired using a Hewlett-Packard Sonos 5500 (Hewlett Packard, Brooklyn, NY, USA) ultrasonic system equipped with ultrasonic IBS analysis software with a 2-4 MHz phased array transducer. A conventional ultrasound system was used as a control. The maximal section of a liver sample obtained from an operation was sought in the conventional plane image. Then Photoshop 7.0 (Adobe Systems, San Jose, CA, USA) was used for ultrasound image processing of the maximal section of the liver. Finally, acoustic densitometry (AD) was initiated to automatically measure the IBS value of an area of interest in a 21× 21pixel oval frame within 2-4 cm of the surface of the left or right liver. The mean of the data was used for semiquantitative analysis. A satisfactory IBS image was obtained in the AD-IBS state. With the single convex probe, all grafts were examined at the same anatomical location (the largest horizontal section of the right liver) at the same depth. Time gain compensation (TGC) was fixed during the scanning process. The lateral gain compensation curve was chosen as the level of the last line and with the average image intensity of the IBS parameter for comparison. All images and data were recorded using an ultrasonic diagnosis apparatus in CDs (Fig. 1).
An experienced sonographer who was unaware of the individuals' disease status scanned the liver specimens, which were obtained from partial resection of the liver and preserved with University of Wisconsin (UW) solution before implantation into a recipient, and the digital images were recorded for off-line assessment. All ultrasound examinations of the patients during the follow-up were performed by the same sonographer. All patients receiving steatotic grafts were followed for 18 months after surgery, and the IBS values in the middle field of the liver parenchyma were recorded at 1, 3, 6, 9, 12, 15, and 18 months after surgery.
The radiofrequency signal obtained by the sensor is inevitably affected by the equipment used. As a result, one must standardize the data collected so that the IBS values collected from different research subjects or from the same subject at different times can be compared. We adopted the TGC standardization in which the TGC curves of each examinee were averaged and each IBS value was multiplied by this TGC mean value at the same depth and then divided by the corresponding TGC value to get the standardized IBS value: the standardized IBS value=actual IBS value×TGC mean value/TGC intrinsic value.

Fig. 1.Ultrasonic image of steatotic graft before implantation.
Measuring fat content via the chloroform-methanol extraction method
A modified chloroform-methanol extraction method was used to measure fat content in the grafts. With this method, lipids were completely extracted from the final tissue residue (0.058-0.192 g). Four mL methanol, 2 mL chloroform, and 1 mL distilled water were added to each sample tube. After homogenizing (T 10 basic; IKA, Germany), the resultant mix was transferred to a 10 mL tube. The homogenate tube was rinsed with 1 mL chloroform, which was then added into the same 10 mL tube. After centrifuging at 4000 rpm for 5 minutes, 2 mL of the lower portion of the chloroform section was transferred into an aluminum dish with constant weight, and further dried at 4 ℃ for 6 hours. Finally, the fat in the resultant residue was removed after the residue had been placed in an oven with a constant temperature of 105 ℃ for 2 hours. Afterwards, the dish was removed for weighing. The following formula was used to calculate the fat content: fat content (%)=(total weight of sample in the dish—weight of dish)×100× 1.5/weight of the sample, in which 1.5 reflects that only 2 mL of 3 mL chloroform in the final homogenate was used in the above procedure. All the reagents used in the chloroform-methanol extraction were purchased from Chengdu Newsun Biochemistry (Chengdu, China).
Classification of liver steatosis
Based on fat content in the liver measured by the chloroform-methanol extraction method, liver steatosis was divided into three categories: light, 5%-10%; moderate, 10%-25%; and severe, >25%.[14]Observation of the pathomorphology of the fatty grafts was further analyzed via hematoxylin and Sudan III staining.
Data collection
The length of stay at a postoperative intensive care unit (ICU) and the levels of total bilirubin (TB), alanine aminotransferase (ALT) and aspartate aminotransferase (AST) in the first week as well as the IBS values of the patients receiving steatotic grafts at 18 months were recorded and analyzed.
Statistical analysis
The data were expressed as the mean±standard deviation or median with a range. SPSS software for Windows (version 15.0; SPSS, Chicago, IL, USA) was used for statistical analysis. Student'sttest was usedto detect differences between the groups. Pearson's correlation coefficient and paired samplesttests were used to analyze the relationship between IBS values in the middle field and fat content. All tests performed were two-tailed. APvalue <0.05 was considered to be statistically significant.
Results
Fat content and pathological features of liver graftsBased on the fat content measured with the chloroformmethanol extraction method, we identified 23 patients with light steatosis (34%), 10 patients with moderate (15%), and no patients with severe steatosis among the 67 patients receiving liver grafts. By hematoxylin and Sudan III staining, we identified 23 pateints with light steatosis with small or micro-vesicular types (34%) (Fig. 2B), 8 patients with moderate steatosis with small or a mix of macro- and micro-vesicular types (12%) (Fig. 2C), and 2 patients with severe steatosis (3%), of which one was of micro-vesicular type and the other of macrovesicular type (Fig. 2D).
Relationship between echogenic intensity and fat content in steatotic grafts
The attenuation of backscatter intensity was found in the B-scan images of the fatty liver. The IBS value was significantly different between normal and steatotic grafts (23.12±4.20 dB vs 33.10±4.67 dB,t=8.296,P=0.001). In contrast to the control grafts (Fig. 2E), an increase of echogenicity was observed in the steatotic ones. With the increase of fat content, echogenicity increased proportionally, accompanied with fine and bright spots (Fig. 2F, G). Severe steatotic livers also showed a posterior attenuation of the deep liver parenchyma (Fig. 2H). To further establish thequantitative correlation between IBS values and fat content, we performed Pearson's correlation analysis. As shown in Figs. 3 and 4, a correlation between echogenic intensity and fat content was detected (r=0.898,P=0.001). Furthermore, we found that significantly increased IBS values were associated with BMI (r=0.922,P=0.001).
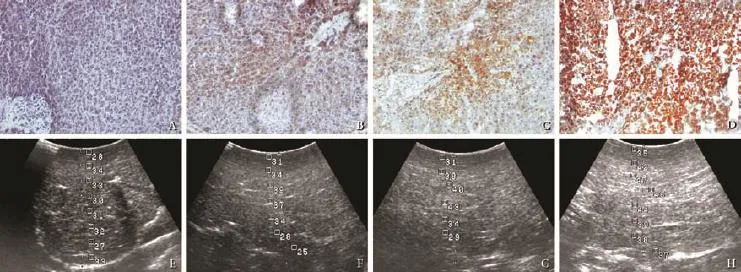
Fig. 2.Liver slices subjected to hematoxylin and Sudan III staining. A set of representative micrographs for normal (A) and steatotic grafts of different degrees: light (B), moderate (C), severe (D) (original magnification ×100), are presented with matched sonographic photographs: normal (E), steatotic grafts of different degrees: light (F), moderate (G), and severe (H).
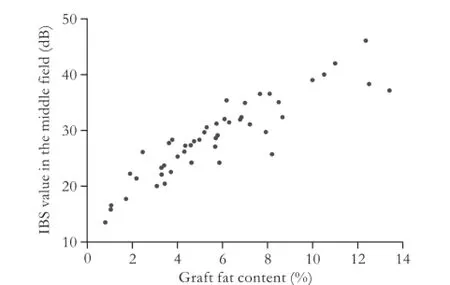
Fig. 3.Correlation between graft fat content and ultrasonic IBS values. With the increase of fat content, the echogenicity increases accordingly (r=0.898,P=0.001).

Fig. 4.Correlation between ultrasonic IBS values and BMI. Significantly increased IBS values were associated with BMI (r=0.922,P=0.001).
Patient status, graft function, and alterations in fat content after transplantation
After the baseline of echogenicity for each graft before transplantation was obtained and its correlation with fat content was confirmed, we examined the steatotic status of the graft after transplantation. First, to assess the function of the graft in the recipient, we compared the recipient's critical condition (ICU stay) and liver function parameters (including TB, ALT, and AST) one week after surgery (Table). ALT and AST levels were significantly higher in the steatotic group than those in the control group (P<0.05), suggesting that the steatotic grafts had impaired liver function.
Next, the recipients were divided into three groups according to the different fat contents: group a (n=10), fat content ≥10%; group b (n=23), fat content 5%-10%; and group c (n=34), fat content <5%. We further evaluated the fat content of the steatotic grafts in the recipients with the IBS value in the middle field of liver echogenicity at 1, 3, 6, 9, 12, 15, and 18 months after surgery. The IBS values of the echogenicity revealed that the fat content in all grafts with varying degrees of steatosis decreased over time (Fig. 5). The IBS value in fatty grafts with a variety degrees of steatosis decreased over 3 months after orthotopic liver transplantation (P=0.02). Twelve to eighteen months after transplantation, the IBS value decreased remarkably (P=0.001) and returned to normal levels in all patients (Fig. 5).
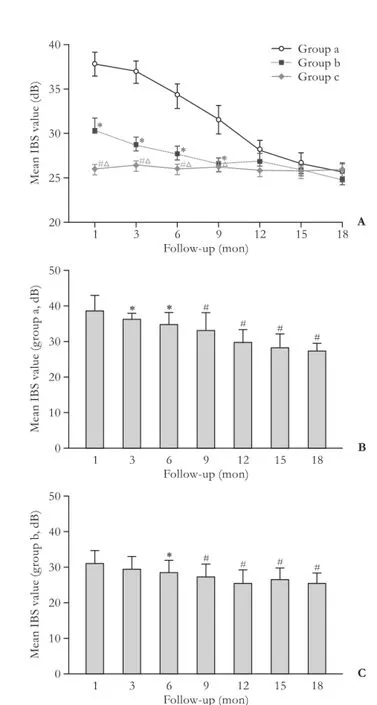
Fig. 5.A: Comparisons of groups and time points (*:P<0.05, groups a vs b; △:P<0.05, groups a vs c; #:P<0.05, groups b vs c).BandC: The IBS values in fatty grafts (fat content ≥5%) with varying degrees of steatosis decreased over 3 months after orthotopic liver transplantation (P<0.05). After 12 months, all patients showed normal IBS values (*:P<0.05; #:P<0.01).
Discussion
Currently, the gold standard for determining liver fat deposition is liver biopsy. Due to its invasive nature and the risk of infection and biliary leakage, its use is limited. Noninvasive imaging methods such as ultrasound, computed tomography (CT), magnetic resonance imaging (MRI), and proton magnetic resonance spectroscopy (MRS) are widely used in clinical practice.[15-20]Compared with CT, MRI, and MRS, which introduce ionizing radiation or incur a high cost, ultrasound is less expensive, easier to access, and allows an assessment of fatty liver with a sensitivity of 60%-94% and a specificity of 84%-95%.[21]Importantly, the technology of ultrasonic IBS is a new method that is noninvasive and provides quantitative assessment of the fatty liver. The method measuring ultrasound backscatter was used to test the degree of steatosis in the current study. The backscatter signals is created by the microstructures of the tissues. Increases in fat content in hepatocytes may cause changes in the shape, degeneration or necrosis, inflammatory cell infiltration, and proliferation of fibrous tissue, all of which lead to a change in intensity, size, or arrangement of the microstructures. A difference in the ultrasound resistance of the affected tissue and of the surroundingarea can be observed. This makes the IBS value increase in the area. Measurement of normal, steatotic, and cirrhotic livers has been performed by many researchers. Their experiments has shown that the scattering value per unit area is in direct proportion to fat content.[22,23]
One limitation of ultrasound-based steatosis detection is its subjectivity, in that it introduces variations among different operators. To avoid the variations from multiple operators, all ultrasound examinations in the present study were performed by the same sonographer who was blinded to other information about the patients and grafts. In addition, to minimize the variation of the same operator's judgment over time, we did not adopt the subjective reading for steatosis grade as previously reported.[24]Instead, we used the objective reading with IBS values in the middle field in all ultrasound examinations.[25,26]Finally, we measured the echogenicity of the grafts before surgery as the baseline and established its relationship with the fat content (r=0.898, P=0.001). Based on these multiple controls, we measured the fat content of the steatotic grafts with ultrasound over an 18-month follow-up study. Our results indicated that the fat content in the grafts with various degrees of steatosis started to decrease at 3 months. Twelve months or later after transplantation, the IBS value was at a normal level in all patients. These results suggested that a decrease in fat content in the steatotic grafts of recipients occurred in all of the studied single-graft living donor liver transplantations. Because the scanning of the graft requires extra care under sterile conditions within a very short-time after it is resected from the donor and our project is a long-term follow-up study requiring repeated scanning of patients, we chose ultrasound as the imaging tool to minimize the potential damage to grafts and reduce the risk of radiation and to further lower the examination cost. Importantly, we adopted multiple approaches, as detailed below, to ensure the validity of the ultrasound evaluation.
It is very encouraging that all of the grafts with various degrees of steatosis tended to lose fat content in the recipients, suggesting that the decrease of fat content was not limited to dual-graft liver transplantation, but it generally occurs in all transplanted liver grafts. However, owing to the small number of cases, especially in the severe steatosis group, we could not set up a complete standard to calculate the fat content based on the ultrasound readings; this will require further studies. Furthermore, this is still a controversial technology, even though IBS is sensitive to minor changes in the composites and structure of tissues. This is mainly because of the many causes affecting the magnitude of scattering, including the density, size, and arrangement of the material and its difference in sound resistance to the surrounding area. Results can also be affected by the elasticity of the material; the focus, size, or depth of a sample; or variations in the ultrasound equipment such as the energy emitted, TGC value, lateral gain compensation value, and probe frequency. Therefore, in order to ensure comparable data taken from the different donors or taken at different times, one must keep the same installment of the equipment, the same depth and area of the samples, and standardize the data using an appropriate reference. The TGC value is used as the reference when IBS is applied to liver transplantation.
The underlying mechanism for the decrease of fat content in steatotic grafts after transplantation remains to be determined. Moon et al[10]pointed out that because of the hypermetabolic state of the recipient after major graft regeneration, plus inadequate nourishment during the early postoperative period, fat in the graft may be mobilized and used for energy. Over the longterm, differences in the recipient's diet and physical activity may also affect the deposition of fat in the liver. In our center, preoperative examination is necessary to exclude severe fatty liver donors. Alternatively, exercise and diet therapy are initiated to reduce donor fat content before liver transplantation. For example, one donor in this study showed a liver echogenicity of 46.4 dB, which was categorized as a severe macro-vesicular steatosis by biopsy before surgery. Subsequently, the donor underwent a 3-month comprehensive therapy, including an adjustment of diet, increased physical activity, and blood lipid-lowering medication. The donor's liver echogenicity decreased to 42.2 dB prior to the surgery. Histological examination revealed that the type of steatosis changed to mixed macro- and micro-vesicles. This information suggested that the fat content in the liver is dynamic according to the condition of each individual. Oshita et al[27]used CT and/or ultrosound for diet-treated donors with steatotic liver at the initial consultation and got a reliable result, indicating that ultrasonic IBS could be used not only for the postoperative observation of recipients but also for the preoperative evaluation of diet-treated donors with steatotic livers at the initial consultation.
In conclusion, consistent with previous studies, a strong correlation between fat content and echogenic intensity in the middle field was detected in the present study. Fat content in steatotic grafts decreased in recipients undergoing single-graft living donor liver transplantation. Ultrasonic IBS is useful in determining the steatotic degree of grafts in donors and in monitoring the grafts after liver transplantation.
Contributors:LB and QY proposed the study and revised the manuscript. YHT, CKF and LQ performed research and wrote the first draft. WYG and HWQ collected and analyzed the data. All authors contributed to the design and interpretation of the study and to further drafts. LB is the guarantor.
Funding:None.
Ethical approval:This study was in accordance with theDeclaration of Helsinki(2000) and was further approved by the medical ethics committee of the West China Hospital.
Competing interest:No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
1 Wieckowska A, Feldstein AE. Diagnosis of nonalcoholic fatty liver disease: invasive versus noninvasive. Semin Liver Dis 2008;28:386-395.
2 Mehta SR, Thomas EL, Bell JD, Johnston DG, Taylor-Robinson SD. Non-invasive means of measuring hepatic fat content. World J Gastroenterol 2008;14:3476-3483.
3 Phillips ML, Boase S, Wahlroos S, Dugar M, Kow L, Stahl J, et al. Associates of change in liver fat content in the morbidly obese after laparoscopic gastric banding surgery. Diabetes Obes Metab 2008;10:661-667.
4 Merion RM, Goodrich NP, Feng S. How can we define expanded criteria for liver donors? J Hepatol 2006;45:484-488.
5 Sheng Y, Jiahong D, Benli H. Feasibility of reduced-size orthotopic liver transplantation with fatty grafts and its potential regeneration in rats. Arch Med Res 2009;40:146-155.
6 Lan X, Li B, Wang XF, Peng CJ, Wei YG, Yan LN. Analysis of risk factors for marginal donors in living donor liver transplantation. Zhonghua Gan Zang Bing Za Zhi 2009;17: 124-127.
7 Verran D, Kusyk T, Painter D, Fisher J, Koorey D, Strasser S, et al. Clinical experience gained from the use of 120 steatotic donor livers for orthotopic liver transplantation. Liver Transpl 2003;9:500-505.
8 McCormack L, Petrowsky H, Jochum W, Mullhaupt B, Weber M, Clavien PA. Use of severely steatotic grafts in liver transplantation: a matched case-control study. Ann Surg 2007;246:940-948.
9 Gao F, Xu X, Ling Q, Wu J, Zhou L, Xie HY, et al. Efficacy and safety of moderately steatotic donor liver in transplantation. Hepatobiliary Pancreat Dis Int 2009;8:29-33.
10 Moon D, Lee S, Hwang S, Kim K, Ahn C, Park K, et al. Resolution of severe graft steatosis following dual-graft living donor liver transplantation. Liver Transpl 2006;12:1156-1160.
11 Bertini M, Delgado V, den Uijl DW, Nucifora G, Ng AC, van Bommel RJ, et al. Prediction of cardiac resynchronization therapy response: value of calibrated integrated backscatter imaging. Circ Cardiovasc Imaging 2010;3:86-93.
12 Rossi M, Cupisti A, Santoro G, Morelli E, Meola M, Barsotti G. Ultrasonic tissue characterization of the carotid artery in chronic renal failure patients. Nephron 2002;91:270-275.
13 Meziri M, Pereira WC, Abdelwahab A, Degott C, Laugier P. In vitro chronic hepatic disease characterization with a multiparametric ultrasonic approach. Ultrasonics 2005;43: 305-313.
14 Perseghin G, Lattuada G, De Cobelli F, Ntali G, Esposito A, Burska A, et al. Serum resistin and hepatic fat content in nondiabetic individuals. J Clin Endocrinol Metab 2006;91: 5122-5125.
15 Cheng YF, Chen CL, Lai CY, Chen TY, Huang TL, Lee TY, et al. Assessment of donor fatty livers for liver transplantation. Transplantation 2001;71:1221-1225.
16 Hess CF, Wolf A, K?lbel G, Kurtz B. Subjective evaluation and quantitative gray-scale analysis in the sonographic diagnosis of diffuse changes in the liver parenchyma. Rofo 1986;145:140-144.
17 Schwenzer NF, Springer F, Schraml C, Stefan N, Machann J, Schick F. Non-invasive assessment and quantification of liver steatosis by ultrasound, computed tomography and magnetic resonance. J Hepatol 2009;51:433-445.
18 Mazhar SM, Shiehmorteza M, Sirlin CB. Noninvasive assessment of hepatic steatosis. Clin Gastroenterol Hepatol 2009;7:135-140.
19 Cucchetti A, Vivarelli M, Ravaioli M, Cescon M, Ercolani G, Piscaglia F, et al. Assessment of donor steatosis in liver transplantation: is it possible without liver biopsy? Clin Transplant 2009;23:519-524.
20 Tsang LL, Chen CL, Huang TL, Chen TY, Wang CC, Ou HY, et al. Preoperative imaging evaluation of potential living liver donors: reasons for exclusion from donation in adult living donor liver transplantation. Transplant Proc 2008;40: 2460-2462.
21 Palmentieri B, de Sio I, La Mura V, Masarone M, Vecchione R, Bruno S, et al. The role of bright liver echo pattern on ultrasound B-mode examination in the diagnosis of liver steatosis. Dig Liver Dis 2006;38:485-489.
22 Hill CR, Rivens I, Vaughan MG, ter Haar GR. Lesion development in focused ultrasound surgery: a general model. Ultrasound Med Biol 1994;20:259-269.
23 Lu ZF, Zagzebski JA, Lee FT. Ultrasound backscatter and attenuation in human liver with diffuse disease. Ultrasound Med Biol 1999;25:1047-1054.
24 Saadeh S, Younossi ZM, Remer EM, Gramlich T, Ong JP, Hurley M, et al. The utility of radiological imaging in nonalcoholic fatty liver disease. Gastroenterology 2002;123: 745-750.
25 Graif M, Yanuka M, Baraz M, Blank A, Moshkovitz M, Kessler A, et al. Quantitative estimation of attenuation in ultrasound video images: correlation with histology in diffuse liver disease. Invest Radiol 2000;35:319-324.
26 Roldan-Valadez E, Favila R, Martínez-López M, Uribe M, Méndez-Sánchez N. Imaging techniques for assessing hepatic fat content in nonalcoholic fatty liver disease. Ann Hepatol 2008;7:212-220.
27 Oshita A, Tashiro H, Amano H, Kobayashi T, Onoe T, Ide K, et al. Safety and feasibility of diet-treated donors with steatotic livers at the initial consultation for living-donor liver transplantation. Transplantation 2012;93:1024-1030.
Received April 14, 2013
Accepted after revision September 5, 2013
AuthorAffiliations:Department of Liver Surgery and Liver Transplantation Center (Yang HT, Chen KF, Wei YG and Li B), Department of Ultrasound (Lu Q), West China Hospital, Sichuan University, Chengdu 610041, China; Institute of Biochemistry and Molecular Biology, West China School of Preclinical and Forensic Medicine, Sichuan University, Chengdu 610041, China (Qin Y and Huang WQ)
Bo Li, MD, PhD, Department of Liver Surgery and Liver Transplantation Center, West China Hospital, Sichuan University, Chengdu 610041, China (Tel: +86-28-85422476; Fax: +86-28-85423724; Email: cdlibo@medmail.com.cn)
? 2014, Hepatobiliary Pancreat Dis Int. All rights reserved.
10.1016/S1499-3872(14)60039-4
Published online March 27, 2014.
 Hepatobiliary & Pancreatic Diseases International2014年4期
Hepatobiliary & Pancreatic Diseases International2014年4期
- Hepatobiliary & Pancreatic Diseases International的其它文章
- Effects of melatonin on the oxidative damage and pancreatic antioxidant defenses in ceruleininduced acute pancreatitis in rats
- A matched-pair analysis of laparoscopic versus open pancreaticoduodenectomy: oncological outcomes using Leeds Pathology Protocol
- Pancreaticoduodenectomy and pancreaticoduodenectomy combined with superior mesentericportal vein resection for elderly cancer patients
- Effect of external beam radiotherapy on patency of uncovered metallic stents in patients with inoperable bile duct cancer
- Prostacyclin decreases splanchnic vascular contractility in cirrhotic rats
- Liver transplantation using organs from deceased organ donors: a single organ transplant center experience