
Tumour response following preoperative chemotherapy is affected by body mass index in patients with colorectal liver metastases
2024-03-07 08:46:12HuaChuanSongHangChengZhouPingGuBingBaoQuanSunTianMingMeiWeiCuiKangYaoHuanZhangYaoShenYuZhangYongShuaiWangRuiPengSongJiZhouWang
Hua-Chuan Song,Hang-Cheng Zhou,Ping Gu,Bing Bao,Quan Sun,Tian-Ming Mei,Wei Cui,Kang Yao,Huan-Zhang Yao,Shen-Yu Zhang,Yong-Shuai Wang,Rui-Peng Song,Ji-Zhou Wang
Abstract BACKGROUND Colorectal cancer is the third most prevalent malignancy globally and ranks second in cancer-related mortality,with the liver being the primary organ of metastasis.Preoperative chemotherapy is widely recommended for initially or potentially resectable colorectal liver metastases (CRLMs).Tumour pathological response serves as the most important and intuitive indicator for assessing the efficacy of chemotherapy.However,the postoperative pathological results reveal that a considerable number of patients exhibit a poor response to preoperative chemotherapy.Body mass index (BMI) is one of the factors affecting the tumorigenesis and progression of colorectal cancer as well as prognosis after various antitumour therapies.Several studies have indicated that overweight and obese patients with metastatic colorectal cancer experience worse prognoses than those with normal weight,particularly when receiving first-line chemotherapy regimens in combination with bevacizumab.AIM To explore the predictive value of BMI regarding the pathologic response following preoperative chemotherapy for CRLMs.METHODS A retrospective analysis was performed in 126 consecutive patients with CRLM who underwent hepatectomy following preoperative chemotherapy at four different hospitals from October 2019 to July 2023.Univariate and multivariate logistic regression models were applied to analyse potential predictors of tumour pathological response.The Kaplan-Meier method with log rank test was used to compare progression-free survival (PFS) between patients with high and low BMI.BMI < 24.0 kg/m2 was defined as low BMI,and tumour regression grade 1-2 was defined as complete tumour response.RESULTS Low BMI was observed in 74 (58.7%) patients and complete tumour response was found in 27 (21.4%) patients.The rate of complete tumour response was significantly higher in patients with low BMI (29.7% vs 9.6%,P=0.007).Multivariate analysis revealed that low BMI [odds ratio (OR)=4.56,95% confidence interval (CI): 1.42-14.63,P=0.011],targeted therapy with bevacizumab (OR=3.02,95%CI: 1.10-8.33,P=0.033),preoperative carcinoembryonic antigen level < 10 ng/mL (OR=3.84,95%CI: 1.19-12.44,P=0.025) and severe sinusoidal dilatation (OR=0.17,95%CI: 0.03-0.90,P=0.037) were independent predictive factors for complete tumour response.The low BMI group exhibited a significantly longer median PFS than the high BMI group (10.7 mo vs 4.7 mo,P=0.011).CONCLUSION In CRLM patients receiving preoperative chemotherapy,a low BMI may be associated with better tumour response and longer PFS.
Key Words: Colorectal liver metastases;Body mass index;Tumour regression grade;Preoperative chemotherapy;Hepatectomy
lNTRODUCTlON
Colorectal cancer is the third most prevalent malignancy globally and ranks second in cancer-related mortality,with the liver being the primary organ of metastasis[1].Colorectal cancer liver metastasis (CRLM) is the primary cause of mortality in patients with colorectal cancer.At present,radical surgery is the most efficacious therapeutic approach for curing CRLMs,with a median overall survival of 5.2 years following hepatectomy[2].Preoperative chemotherapy,including chemotherapy regimens based on oxaliplatin and irinotecan with or without targeted therapy,is widely recommended for initially or potentially resectable CRLM patients due to its potential to reduce tumour load,increase resection rate,and consolidate surgical results[3].
Tumour pathological response serves as the most important and intuitive indicator for assessing the efficacy of chemotherapy,while also playing a crucial role as a long-term prognostic factor in patients with CRLM receiving chemotherapy[4,5].However,the postoperative pathological results reveal that a considerable number of patients exhibit a poor response to preoperative chemotherapy[6-8].For these patients,the potential benefits of receiving perioperative chemotherapy may outweigh the disadvantages.Therefore,it may be more prudent to proactively identify these patients prior to chemotherapy to implement timely and appropriate intervention measures or consider direct surgical treatment,thereby avoiding tumour progression and chemotherapy-related adverse events from unnecessary preoperative chemotherapy.
Obesity,an important risk factor threatening human health,is strongly associated with the occurrence and progression of numerous diseases[9].Epidemiological evidence suggests that overweight and obesity are associated with an increased risk of colorectal carcinogenesis and poorer tumour outcomes.Several studies have indicated that overweight and obese patients with metastatic colorectal cancer experience worse prognoses than those with normal weight,particularly when receiving first-line chemotherapy regimens in combination with bevacizumab[10-12].Furthermore,research has demonstrated that obesity and an increase in adipocytes are associated with therapeutic resistance in patients with colorectal cancer.In this study,we mainly investigated the correlation between body mass index (BMI) and pathological responses in CRLM patients receiving preoperative chemotherapy.
MATERlALS AND METHODS
Patient and treatment
We retrospectively collected and analysed the clinical and pathological data of 126 patients with CRLM who underwent radical hepatectomy after receiving preoperative chemotherapy at the First Affiliated Hospital of University of Science and Technology of China,Suzhou Hospital Affiliated to Anhui Medical University,Tongcheng People’s Hospital and Xuancheng People’s Hospital from October 2019 to July 2023.The inclusion criteria were as follows: (1) Patients received first-line chemotherapy preoperatively,including neoadjuvant and conversion therapies;and (2) The postoperative pathology findings are consistent with CRLM.The exclusion criteria were as follows: (1) Patients who had received radiotherapy,transarterial chemoembolization,or other local treatments for CRLM before hepatectomy;and (2) Combined with other malignant tumours.The data collection plan received approval from the Institutional Ethics Review Committee of the hospital.
The personalized treatment decisions of patients were deliberated by a multidisciplinary team (MDT) consisting of experts in hepatobiliary surgery,oncology,gastroenterology,imaging,pathology and ultrasound.All patients underwent preoperative chemotherapy with oxaliplatin and/or irinotecan,and this was followed by individualized decision-making regarding the addition of targeted therapy based on their specific tumour characteristics.The targeted therapies included cetuximab and bevacizumab.Subsequently,radical hepatectomy was performed for all patients after preoperative chemotherapy.
Definition and data collection
Considering variations in adipose tissue distribution across diverse ethnic populations,a BMI < 24.0 kg/m2was defined as low BMI within this study[13].A weight change exceeding 5% was recorded as either weight gain or weight loss during the period between the initiation of neoadjuvant chemotherapy and the time of surgery.Both weight and height data were measured on the day of patient admission before surgery.Postoperative complication grading was based on the Clavien-Dindo classification system[14].The occurrence of complications at Clavien-Dindo grade II and higher was recorded.More definitions of variables are summarized in Supplementary Table 1.
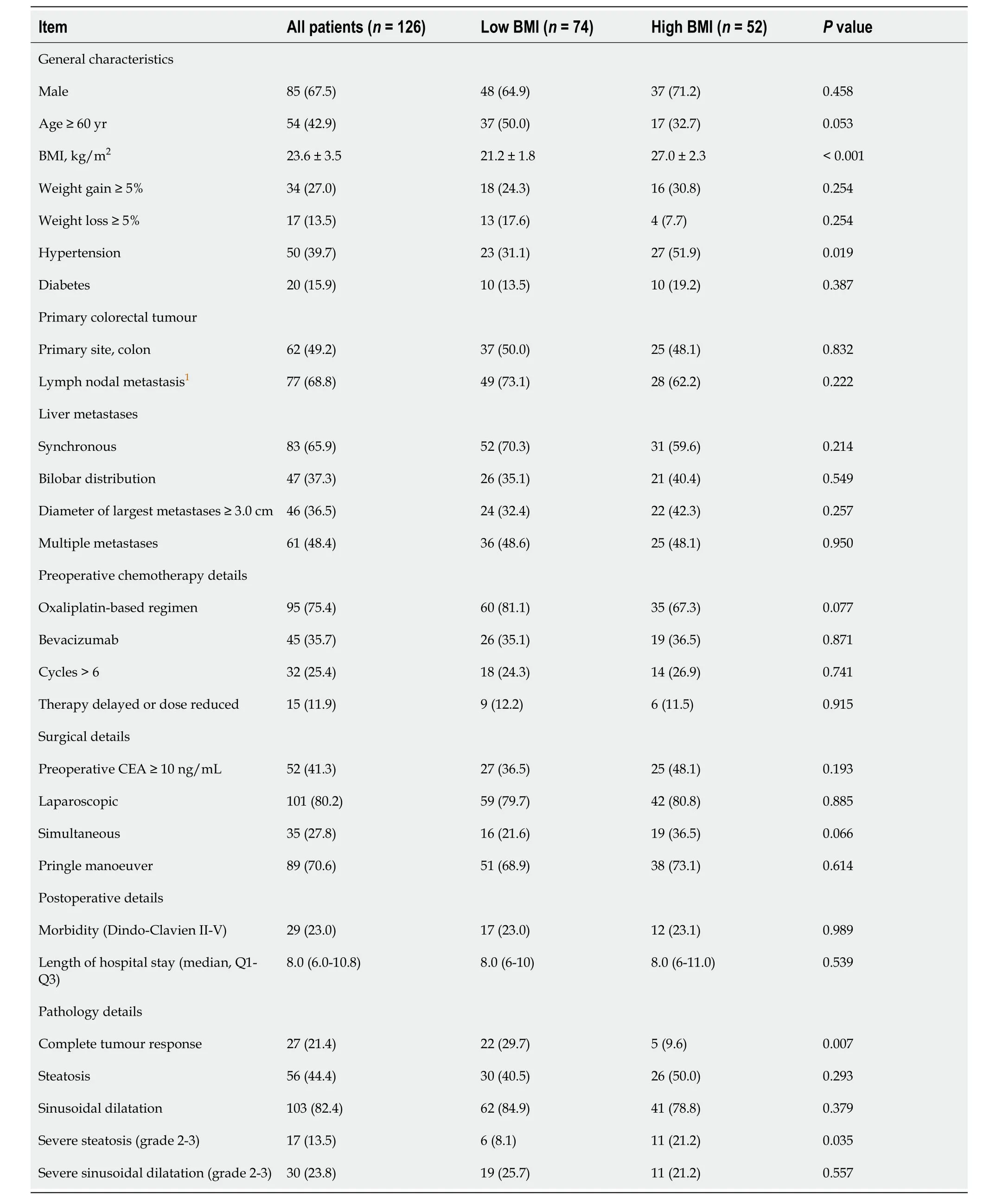
Table 1 Clinical and pathology characteristics
Pathological assessment
The metastatic specimens obtained after liver resection were evaluated by professional pathologists.The assessment of pathological responses to chemotherapy was based on the tumour regression grade (TRG) system proposed by Mandardet al[15] (Figure 1).Grade 1 indicates the absence of residual cancer and extensive fibrosis.Grade 2 signifies rare scattered residual cancer cells within fibrosis.Grade 3 demonstrates a higher presence of residual tumour cells,although fibrosis remains predominant.Grade 4 is characterized by a predominance of residual tumour cells.Grade 5 denotes the absence of signs indicating regression.TRG grade 1-2 was defined as a complete tumour response,while TRG grade 3-5 was defined as a poor tumour response[4,5].
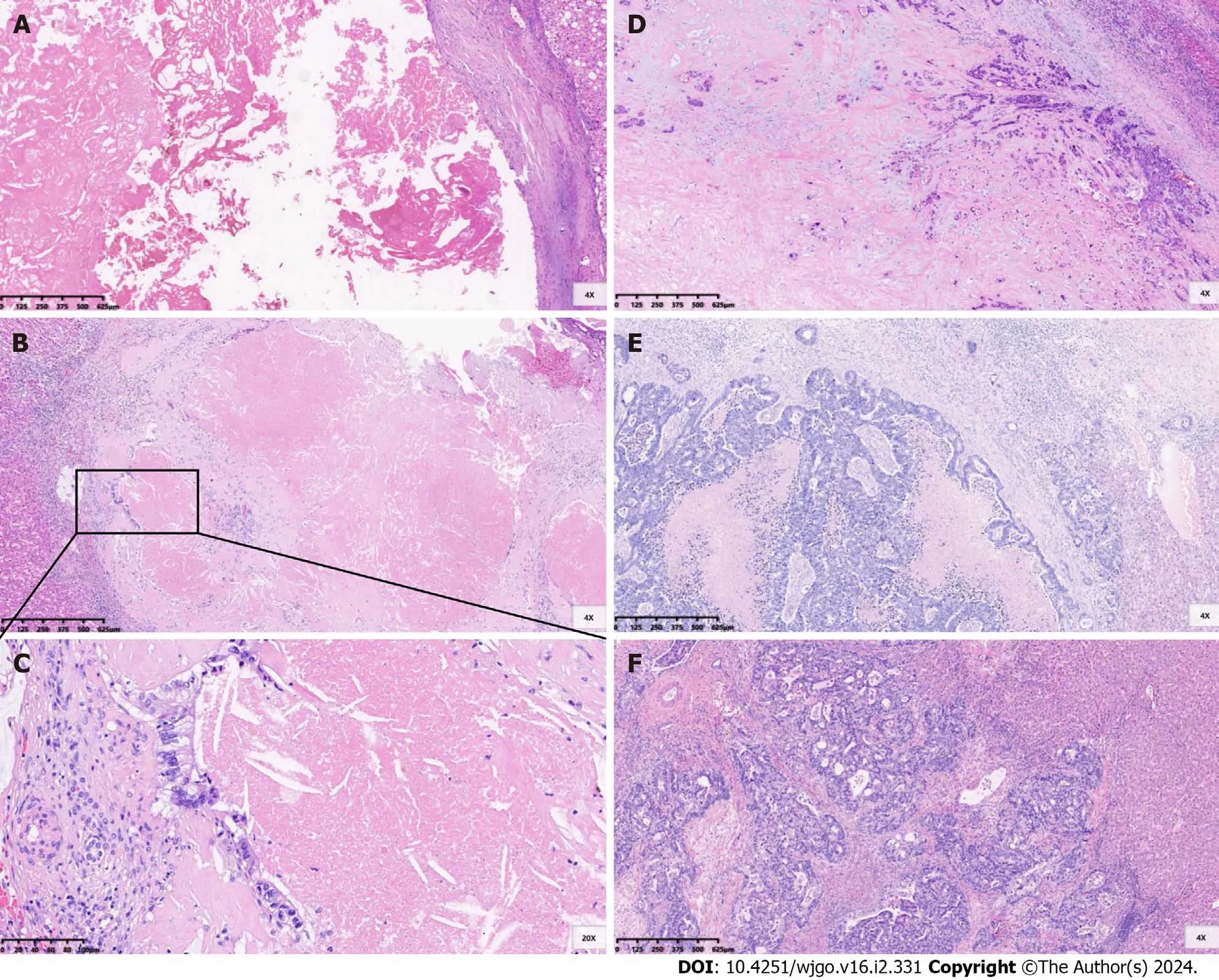
Figure 1 Tumour regression grade for colorectal liver metastases after preoperative chemotherapy. A: Tumour regression grade 1 (TRG1),no residual cancer cells;B and C: TRG2,rare scattered residual cancer cells within fibrosis;D: TRG3,more residual tumour cells but fibrosis remains predominant;E: TRG4,residual tumour cells predominant;F: TRG5,absence of regressive changes.
Considering that steatosis and sinusoidal dilatation are the two most common liver injuries associated with oxaliplatin,irinotecan,and 5-fluorouracil chemotherapy for CRLM,we conducted a comprehensive assessment of the extent of these chemotherapy-associated liver injuries in the liver area surrounding metastases.The percentage of steatosis in involved hepatocytes was assessed and graded into the following categories: Absent (0%),grade 1 (1%-30%),grade 2 (31%-60%) and grade 3 (> 60%)[4].Sinusoidal dilatation was scored according to the pathological grade system published by Rubbia-Brandtet al[16]: Absent,grade 1,grade 2 and grade 3.Grade 2-3 steatosis and sinusoidal dilatation were defined as severe liver injuries[5].
Follow-up
Lung,abdominal and pelvic contrast-enhanced computed tomography scans (liver contrast-enhanced magnetic resonance imaging examinations if deemed necessary) were performed at 3-mo intervals during the initial 2-year period postsurgery,followed by biannual assessments thereafter.
Statistical analysis
The data were analysed using the statistical software packages R version 4.2.0 (The R Foundation;http://www.R-project.org) and EmpowerStats (www.empowerstats.com;X&Y Solutions,Boston,MA,United States).Ttests and the Kruskal-Wallis rank sum test were employed to test normally and nonnormally distributed continuous variables,respectively.χ2tests were used to compare categorical variables.The relevant factors associated with tumour histopathological response were examined using univariate and multivariate logistic regression models.Predictors with a significance level ofP< 0.10 in the univariate analysis were included in the multivariate models.The Kaplan-Meier method with log rank test was used to compare progression-free survival (PFS) between patients with high and low BMI.Statistical significance was considered atP< 0.05.
RESULTS
Patient characteristics
A total of 126 patients were enrolled in this study,including 85 males and 41 females.The median age at the time of hepatectomy was 58 years [interquartile range (IQR) 51.0-67.0].The median BMI was 23.3 (IQR 20.8-25.9) kg/m2,with low BMI observed in 74 (58.7%) patients.Hypertension was present in 50 (39.7%) patients,and diabetes was diagnosed in 20 (15.9%) patients.Among the patients in the cohort,the rectum was the primary tumour site in 64 (50.8%) patients.Synchronous liver metastases were identified in 83 (65.9%) patients,with multiple liver metastases observed in 61 (48.4%) patients.The median diameter of the largest metastatic lesion was 2.7 cm (IQR 1.7-4.2).A preoperative carcinoembryonic antigen (CEA) level ≥ 10 ng/mL was observed in 52 (41.3%) patients.
Ninety-five (75.4%) patients received an oxaliplatin-based preoperative chemotherapy regimen.Targeted therapy was administered to 77 (61.1%) patients,including bevacizumab in 45 (35.7%) patients and cetuximab in 32 (25.4%) patients.The median number of chemotherapy cycles was 5 (IQR 3.0-7.0),with more than 6 cycles being administered in 32 (25.4%) patients preoperatively.Laparoscopic procedures were performed in 101 (80.2%) patients,while simultaneous surgery was conducted in 35 (27.8%) patients.The Pringle maneuver was utilized in the surgical approach for a total of 89 (70.6%) patients.Complications of grade II or higher were observed in 29 (23%) patients.The median duration of postoperative hospital stay was recorded as approximately 8 (IQR 6.0-10.8) d.Different degrees of steatosis and sinusoidal dilatation were observed in 56 (44.4%) and 103 (82.4%) patients,respectively.A complete tumour response was found in 27 (21.4%) patients (Table 1).
Relationship between BMI and tumour histological response
The baseline clinicopathologic and treatment characteristics based on BMI grouping are summarized in Table 1.The characteristics of the two groups were basically similar,with the high BMI group demonstrating a higher incidence of hypertension (51.9%vs31.1%,P=0.019) and severe steatosis (21.2%vs8.1%,P=0.035) than the low BMI group.The rate of complete tumour response was significantly higher in patients with low BMI (29.7%vs9.6%,P=0.007).Univariate analysis identified that low BMI [odds ratio (OR)=3.98,95% confidence interval (CI): 1.39-11.34,P=0.010],targeted therapy with bevacizumab (OR=2.88,95%CI: 1.20-6.87,P=0.018),preoperative CEA level < 10 ng/mL (OR=3.98,95%CI: 1.39-11.34,P=0.010) and severe sinusoidal dilatation (OR=0.20,95%CI: 0.05-0.91,P=0.038) were significant factors associated with complete tumour response (Table 2).Multivariate analysis revealed that low BMI (OR=4.56,95%CI: 1.42-14.63,P=0.011),targeted therapy with bevacizumab (OR=3.02,95%CI: 1.10-8.33,P=0.033),preoperative CEA level < 10 ng/mL (OR=3.84,95%CI: 1.19-12.44,P=0.025) and severe sinusoidal dilatation (OR=0.17,95%CI: 0.03-0.90,P=0.037) were independent predictive factors for complete tumour response (Figure 2 and Supplementary Table 2).The effect of BMI on tumour histological response was consistent across subgroups (Supplementary Table 3).

Table 2 Univariate regression analysis of factors for complete tumour response
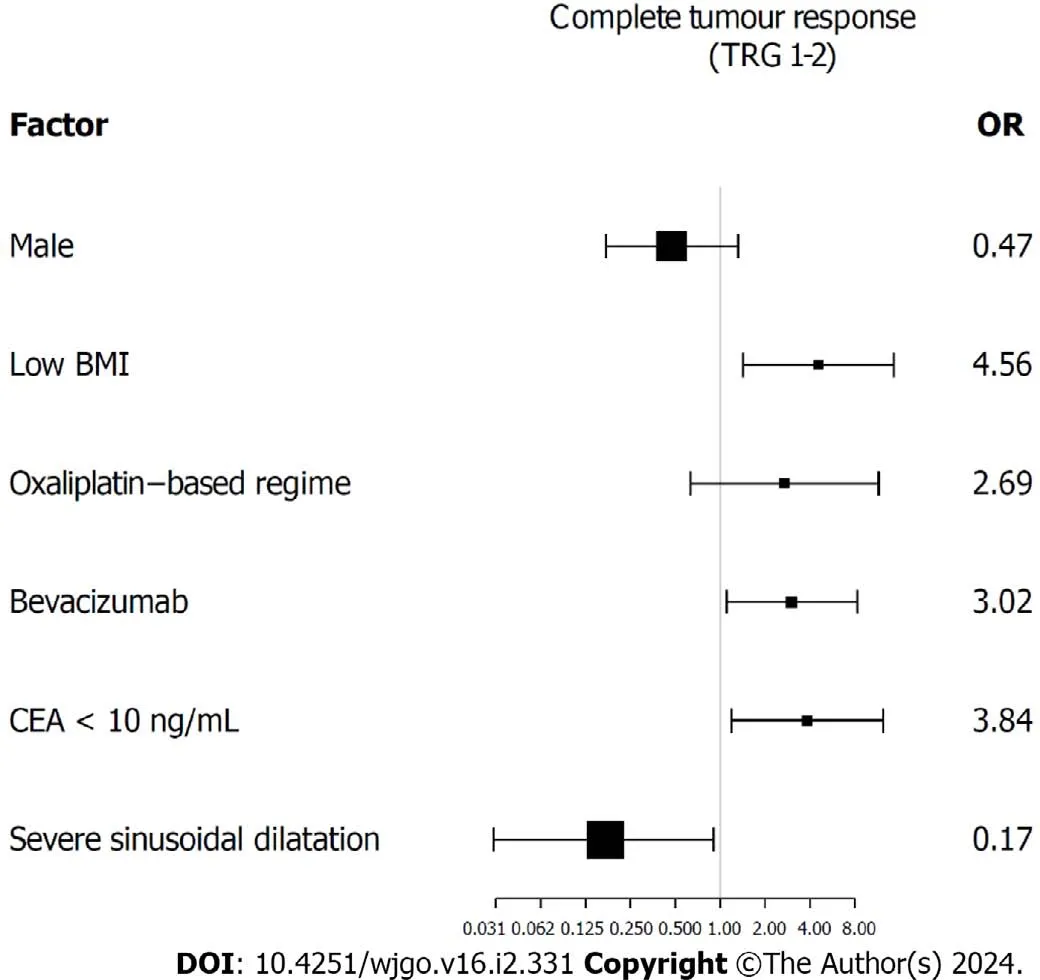
Figure 2 Factors related to complete tumour response (multivariate regression analysis).BMI: Body mass index;CEA: Carcinoembryonic antigen;TRG: Tumour regression grade.
The relationship between BMI and chemotherapy-related liver injuries and postoperative details
The incidence of severe steatosis in patients with high BMI (21.2%vs8.1%P=0.035) was significantly higher than that in patients with low BMI,with no statistically significant difference in sinusoidal dilatation.No statistically significant difference was observed in the incidence of postoperative complications or the length of hospital stay postoperatively (Table 1).
Impact of BMI and histological responses on PFS
The median follow-up for PFS was 5.7 (IQR 2.4-12.8) mo.At the time of analysis,disease progression was observed in 87 (69.0%) patients.The low BMI group exhibited a significantly longer median PFS than the high BMI group,with median PFS of 10.7 (95%CI: 6.3-17.9) mo and 4.7 (95%CI: 3.0-8.4) mo,respectively (P=0.011) (Figure 3A).The median PFS was preferable in patients with complete tumour response compared with poor response,although this difference did not reach statistical significance (10.7 movs6.0 mo,P=0.057) (Figure 3B).
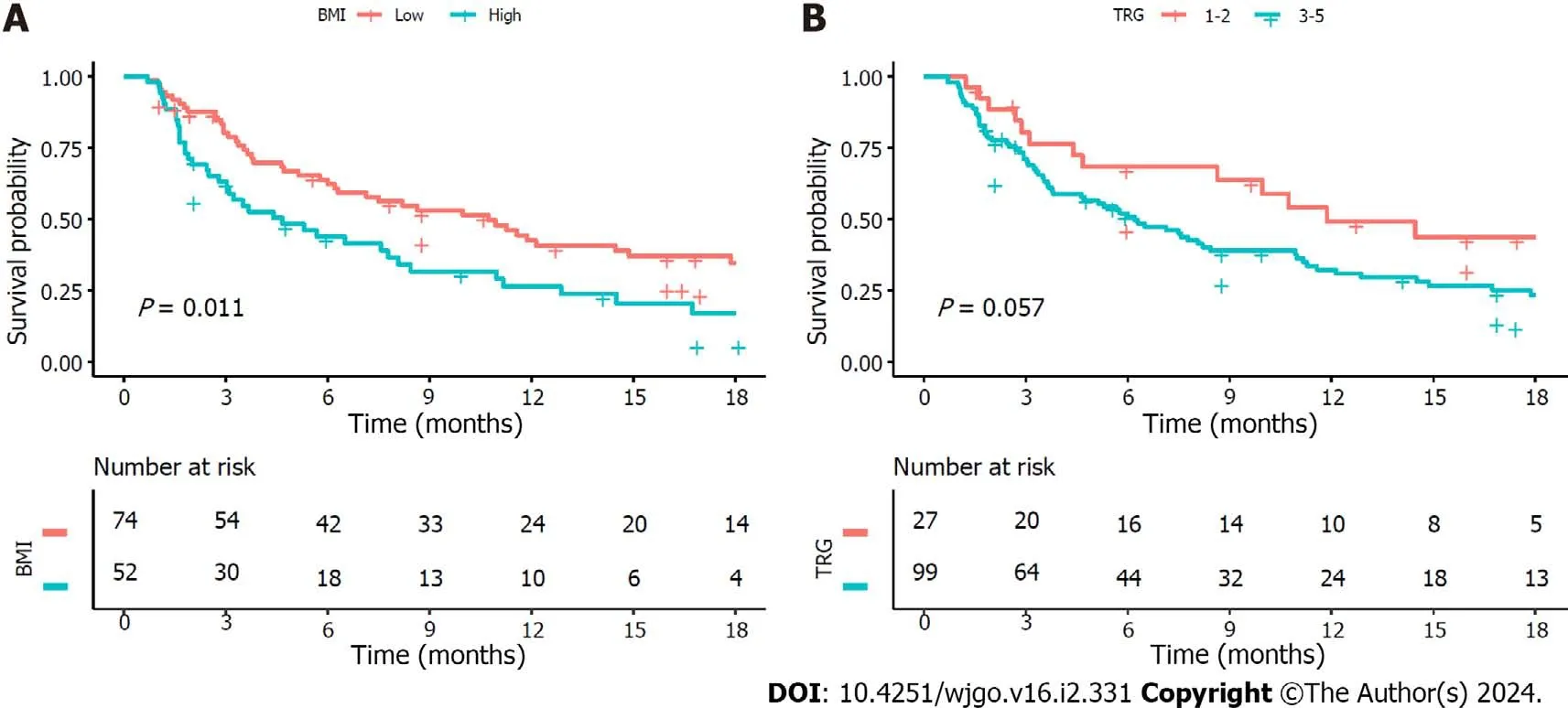
Figure 3 Kaplan-Meier survival curve: lmpact of body mass index and tumour regression grade on progression-free survival. A: A better progression-free survival (PFS) was observed in patients with low body mass index;B: Impact of tumour regression grade on PFS.BMI: Body mass index;TRG: Tumour regression grade.
DlSCUSSlON
Obesity (or high BMI) is associated with an increased risk of colorectal carcinogenesis and unfavourable prognosis[9].However,the impact of BMI on the pathological response of CRLMs to preoperative chemotherapy has been reported in a limited number of studies.In this study,we observed that overweight and obese patients with CRLM exhibited a poorer response to chemotherapy and appeared to have shorter PFS than patients with low BMI.The World Health Organization standard defines adult overweight as having a BMI ≥ 25.0 kg/m2,while obesity is defined as having a BMI ≥ 30.0 kg/m2.Nevertheless,considering variations in average BMI among different ethnic groups,the Chinese standards employed a threshold of BMI ≥ 24.0 kg/m2to define overweight and ≥ 28.0 kg/m2for obesity[13].Therefore,a BMI < 24.0 kg/m2was defined as low BMI within the study.
Similar findings have been reported in some studies of primary and metastatic colorectal cancer.Previous studies have shown that obesity is associated with a lower rate of pathological complete response and a higher risk for local recurrence after neoadjuvant chemoradiation therapy in patients with locally advanced rectal cancer[17,18].A retrospective study showed that high BMI,visceral fat area and subcutaneous fat area were significantly associated with nonresponse (stable disease or progressive disease) in metastatic colorectal cancer patients treated with a bevacizumab-based chemotherapeutic regimen.Patients with high BMI had a significantly shorter mean time to progression than patients with normal BMI (9vs12 mo,P=0.01).In the multivariate analysis,a high visceral fat area independently predicted nonresponse [hazard ratio (HR)=7.18,95%CI: 1.69-30.6],a shorter time to progression (HR=2.80,95%CI: 1.35-5.79) and shorter survival (HR=2.88,95%CI: 1.13-7.32)[12].An analysis of 563 patients with metastatic colorectal cancer who had received first-line chemotherapy in combination with bevacizumab showed that the nonobese group exhibited a longer median PFS (10.8vs9 mo,P=0.030) and a higher 2-year survival rate (34%vs23%,P=0.036) than the obese group[11].A similar result of low BMI being associated with longer median PFS (24vs17.9 mo,P=0.04) in CRLM patients was also found in the work by Hopirteanet al[19].
At the initiation of chemotherapy,the dosage of first-line chemotherapy agents commonly used for CRLM,such as oxaliplatin,irinotecan,5-fluorouracil and capecitabine,is determined based on body surface area,while bevacizumab is dosed according to weight.However,in our study,there was no statistically significant difference in the chemotherapy cycle delays or dose reductions (11.5% in the low BMI group and 7% in the high BMI group) due to factors between the two patient cohorts (Table 1).Therefore,we propose that these findings are not attributable to relatively inadequate medication dosages or substantially lower systemic drug concentrations among patients with higher BMI compared to those with lower BMI.The inferior pathological response and prognosis observed in patients with high BMI may arise from more aggressive tumour biology or increased susceptibility to chemotherapy resistance of CRLMs in obese patients involving insulin resistance and adipose tissue-derived factors[12].
Previous studies have demonstrated that adipose tissue secretes various growth factors and cytokines,including leptin,adiponectin,vascular endothelial growth factor (VEGF),insulin-like growth factor-1 (IGF-1),and angiopoietins (Angs)[20].The systemic or local internal environment is then altered to facilitate tumour growth,metastasis and angiogenesisas well as confer resistance to chemotherapy and targeted therapies[20-22].Angiogenic factors such as leptin,VEGF,IGF-1 and Angs exert a direct effect on promoting cancer angiogenesis,which may be the main reason for the resistance of obese patients to anti-VEGF therapy such as bevacizumab and tumour progression[12,20].Chenet al[23] discovered that obesity-associated leptin promotes chemoresistance towards the chemotherapy drug 5-fluorouracil in colorectal cancer.Elevated IGF-1 levels elicit various biological responses,including enhanced tumour proliferation and aggressiveness,resistance to apoptosis,promotion of an inflammatory tumour microenvironment,and obesity-related resistance to chemotherapy[22].Dallaset al[24] found that the levels of activated IGF-1 receptors were elevated in chemoresistant (5-fluorouracil and oxaliplatin) colorectal cancer cell lines compared with parent cell lines.Additionally,a cross-resistance phenomenon was observed between 5-fluorouracil and oxaliplatin[24].Moreover,heightened blood insulin levels in obese patients induce resistance to oxaliplatin colon cancer cells by activating the PI3K/Akt pathway.Simultaneously,there is an augmented proliferative response of chemoresistant cancer cells to insulin that is accompanied by decreased insulin metabolism[25].
The poor outcomes associated with obesity may be attributed to insufficient engagement in appropriate physical activities and an unhealthy dietary regimen among patients with CRLM.Increased levels of physical activity and a lower BMI have been found to correlate with extended disease-free survival in individuals diagnosed with colorectal cancer,apparently enhancing their long-term survival outcomes[26,27].In metastatic colorectal cancer,high levels of physical activity were associated with longer PFS and lower treatment-related adverse events[28].Physical activity may ameliorate insulin resistance and mitigate the effects of obesity-related growth factors,including insulin,IGF-1,and adiponectin,thereby enhancing tumour outcomes[29-36].Western dietary patterns,high glycaemic load,and total carbohydrate intake exhibit a positive correlation with an elevated risk of colorectal cancer recurrence and mortality[37-39].Therefore,physical activity and a controlled diet are recommended for patients diagnosed with colorectal cancer to improve prognosis[40].Furthermore,research findings have demonstrated that bariatric surgery in obese adults can significantly reduce both obesity-related cancers and cancer-related mortality[41].The incidence of colorectal cancer in obese individuals exhibits a significant reduction after bariatric surgery[42-44].Similar results have been found in other tumours,and diverse modalities of weight loss can enhance outcomes in breast cancer patients[45-47].Additionally,bariatric surgery has the potential to improve the response to immune checkpoint blockade in breast cancer patients[48].
First-line chemotherapy combined with the anti-VEGF agent bevacizumab in the treatment of CRLM can improve the resection rates,objective response rates and overall survival rates[5,49,50].Consistent with these findings,our study revealed a superior pathological response when preoperative chemotherapy was combined with bevacizumab for CRLMs.Given the comparable pathological response between patients treated with cetuximab and those without targeted therapy (complete response rates of 15.6% and 14.3%,respectively),both groups exhibited inferior outcomes compared to the bevacizumab-treated group (complete response rate of 33.3%).Consequently,we categorized patients receiving cetuximab or no targeted therapy as the nonbevacizumab group.Although previous studies have shown that the effectiveness of first-line bevacizumab-based treatment for CRLMs is more likely to be affected by BMI in metastatic colorectal cancer[10-12],our findings indicated that,whether receiving bevacizumab or not,patients with high BMI exhibited poorer pathological responses.
The present study found that a preoperative CEA level < 10 ng/mL was associated with favourable tumour response rates as mentioned in a previous study[50].However,further research is needed to explore the underlying mechanism responsible for this association.Consistent with previous studies,this study revealed that severe sinusoidal dilatation (grade 2-3) was also significantly associated with poor pathological response rates[4,5].This involves various alterations,including the loss of fenestrae in sinusoidal endothelial cells,weakened hepatic microcirculation,limited transportation of drugs,and hypoxia associated with sinusoidal dilatation.Collectively,these factors contribute to inferior tumour response rates.
There were several limitations in this study.First,genetic factors such as RAS and mismatch repair/microsatellite instability status that have been shown to be important prognostic factors in colorectal cancer were not included in the analysis because the recorded data were partially missing.Second,the study needed a review of tumour pathological sections after hepatectomy to assess the TRG of liver metastases,resulting in a study population that included only resectable CRLM patients,inevitably resulting in selection bias.Third,due to the small sample size,we did not conduct a subgroup analysis of underweight patients.Nevertheless,we believe that this study provides useful information for clinical practice.
This study provides evidence that tumour response following preoperative chemotherapy is affected by BMI in patients with CRLM,and this finding may serve as a reference for developing personalized treatment strategies.For example,neoadjuvant chemotherapy is not recommended for initially resectable CRLM patients with high BMI.Next,it is worth further exploring whether deliberately increasing physical activity and weight loss can improve the response to chemotherapy in obese CRLM patients.
CONCLUSlON
From this study of CRLM patients receiving preoperative chemotherapy,low BMI appears to be associated with better tumour response and longer PFS.The MDT should consider this factor when designing personalized treatment strategies for the optimal management of CRLM patients.
ARTlCLE HlGHLlGHTS
Research background
Radical surgery is the most efficacious therapeutic approach for curing colorectal liver metastases (CRLMs).Preoperative chemotherapy is widely recommended for patients with CRLM.However,a considerable number of patients exhibit poor response to preoperative chemotherapy.
Research motivation
Epidemiological evidence suggests that body mass index (BMI) is associated with colorectal carcinogenesis and outcomes.Exploring the relationship between BMI and pathological response to preoperative chemotherapy may help us better manage CRLM patients.
Research objectives
This study was designed to explore the predictive value of BMI regarding the pathologic response following preoperative chemotherapy for CRLMs.
Research methods
A retrospective analysis was conducted on the clinical and pathological data of 126 CRLM patients who underwent hepatectomy after preoperative chemotherapy.We analysed the potential predictive factors affecting tumour regression grade (TRG).TRG 1-2 was defined as a complete pathological response.
Research results
The rate of complete tumour response was significantly higher in patients with low BMI.Multivariate analysis revealed that low BMI independently predicted complete tumour response to preoperative chemotherapy.The low BMI group exhibited a longer median progression-free survival (PFS) than the high BMI group.
Research conclusions
In CRLM patients receiving preoperative chemotherapy,a low BMI may be associated with better tumour response and longer PFS.
Research perspectives
Whether deliberately increasing physical activity and weight loss may improve the response to chemotherapy in obese CRLM patients is an interesting topic worthy of further exploration.
ACKNOWLEDGEMENTS
Thanks to all authors for their efforts in this work.
FOOTNOTES
Co-first authors:Hua-Chuan Song and Hang-Cheng Zhou.
Author contributions:Song HC and Zhou HC contributed equally to this work;Song HC,Zhou HC,Song RP,and Wang JZ designed the research study;Song HC,Bao B,Sun Q,Mei TM,Yao K,Cui W,and Yao HZ performed the research and collected the data;Zhou HC and Gu P assessed the pathological section;Song HC,Zhang SY,and Wang YS analysed and interpreted data;Song HC and Zhou HC wrote the manuscript;Song RP and Wang JZ revised and proofed the manuscript;and all authors have read and approve the final manuscript.
Supported byNational Natural Science Foundation of China,No.82170618.
lnstitutional review board statement:The study was reviewed and approved by the First Affiliated Hospital of University of Science and Technology of China Institutional Review Board (Approval No.2023KY-323).
Clinical trial registration statement:This study is registered at Medical Research Registration and Filing Information System of China (www.medicalresearch.org.cn),Filing number is MR 34 23 043810.
lnformed consent statement:All study participants,or their legal guardian,provided informed written consent prior to study enrollment.
Conflict-of-interest statement:All the authors report no relevant conflicts of interest for this article.
Data sharing statement:All data and materials are available from the corresponding author.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is non-commercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORClD number:Ji-Zhou Wang 0000-0002-6934-072X.
S-Editor:Wang JJ
L-Editor:A
P-Editor:Zhang YL
 World Journal of Gastrointestinal Oncology2024年2期
World Journal of Gastrointestinal Oncology2024年2期
- World Journal of Gastrointestinal Oncology的其它文章
- Does enhanced recovery after surgery programs improve clinical outcomes in liver cancer surgery?
- Cardiotoxicity induced by fluoropyrimidine drugs in the treatment of gastrointestinal tumors
- Effect of screening colonoscopy frequency on colorectal cancer mortality in patients with a family history of colorectal cancer
- Preoperative controlling nutritional status as an optimal prognostic nutritional index to predict the outcome for colorectal cancer
- Expression of cyclin-dependent kinase 9 is positively correlated with the autophagy level in colon cancer
- Progress in the treatment of advanced hepatocellular carcinoma with immune combination therapy