
Exclusive cigar smoking in the United States and smoking-related diseases: A systematic review
2020-12-16 09:00:46PeterLeeJanetteHamlingAlisonThornton
World Journal of Meta-Analysis 2020年3期
Peter N Lee,Janette S Hamling, Alison J Thornton
Peter N Lee, Department of Statistics, P.N.Lee Statistics and Computing Ltd., Sutton, Surrey SM2 5DA, United Kingdom
Janette S Hamling, Department of Statistics, RoeLee Statistics Ltd., Sutton SM2 5DA, United Kingdom
Alison J Thornton, Independent Consultant, Okehampton, Devon EX20 1SG, United Kingdom
Abstract
Key words: Tobacco products; Cigar smoking; Lung neoplasms; Pulmonary disease; Chronic obstructive; Heart diseases; Stroke; Circulatory disease; Systematic review; Metaanalysis
INTRODUCTION
There is extensive evidence on the relationship of cigarette smoking to health endpoints but far less evidence relating to cigar smoking.While some studies have reported results relating to dual use of cigars and pipes[1-4]or to cigar smoking in those who may also smoke other tobacco products[5], the health effects of exclusive cigar smoking have been less often reported.Comparing disease risk in cigar smokers who have never smoked other tobacco products with that in never smokers of any tobacco product avoids the problems of residual confounding by other smoking habits and of possible differences in cigar smoking habits (such as depth of inhalation[6]) in those who have ever smoked other tobacco products.
Exclusive cigar smoking is much less common than cigarette smoking so the population studied must be large enough to include enough exclusive cigar smokers for a useful risk assessment to be made.For this reason we have restricted attention to studies in the United States, a country not only with a large population, but one where cigar smoking is relatively common compared with other countries[7,8].We also restrict attention to the major smoking-related diseases.
MATERIALS AND METHODS
Study inclusion criteria
Published studies were included if they were carried out in the United States and reported the risk of lung cancer or chronic obstructive pulmonary disease (COPD) or heart disease, stroke and/or overall circulatory disease, comparing exclusive cigar smokers (current, former or ever cigar smokers who never smoked other tobacco products) with never smokers of any tobacco (or a closely-related comparison group).The results considered were for overall lung cancer rather than lung cancer subtypes, and related to overall risk measures rather than dose response indices, although dose response results by amount smoked were also identified.
Literature searches
Searching for results on cigar smoking was complicated by the MEDLINE search term “cigar smoking” being available only from the start of 2018.Before then the only search term to include cigar smoking was “tobacco products”.
For lung cancer, the first step was to examine publications from a previous review relating lung cancer to various indices of smoking based on studies published during the 1900s[9].Subsequently three different MEDLINE searches were conducted using terms such as (“cigar” or “cigars”), “United States” and “l(fā)ung neoplasms”.This was followed by a fourth search that attempted to retrieve relevant papers that had not yet been indexed with MeSH terms on MEDLINE, this search not being lung cancer specific.A fifth search used wholly non-MeSH search terms, with the final stage being to look for relevant results in papers identified as relevant in the searches for COPD and for heart disease, stroke and circulatory diseases.
For COPD, the process started with three different MEDLINE searches using the terms “COPD” or “pulmonary disease, chronic obstructive” to identify the disease.The fourth search used the term “Smoking” rather than “Cigar”, while the fifth search used the MeSH terms “Smoking/mortality” or “Smoking/adverse effects”.The next step was to review the results from the fourth lung cancer search, while the final step was to look at papers identified as relevant in the searches for lung cancer and for heart disease, stroke and circulatory diseases.
For heart disease, stroke and circulatory diseases, the process started with four different MEDLINE searches using the disease terms “Heart disease”, “Stroke” or “Heart”.The next step was again to review the results from the fourth lung cancer search, while the final step was to look at relevant papers from the lung cancer and COPD searches.
Searching ended when no new data was found and all the papers referenced by reviews had been examined.Full details of the searches are given in Supplementary material.
Sorting publications into studies and avoidance of overlap
The papers identified in the searches were reviewed for the studies they reported, and multiple publications reporting the same study were identified.
The source papers identified as providing relevant estimates were then considered for overlap of reporting.Where more than one of the source papers reported on the same study, the results may have been reported in different ways or for different lengths of follow-up, or have combined results from multiple studies.
Data recorded
For each paper identified as providing relevant results details were entered onto a study database and a linked relative risk (RR) database for the relevant disease.
The study database contained a record for each study describing the following aspects: A study name based on the published study name or on the name of the first author of the paper; study title; study design; sexes considered; age range and other details of the population studied; timing and length of follow-up; details of overlaps or links with other studies; number of cases; number of controls or subjects at risk; types of controls and matching factors used in case-control studies; and confounding variables considered.
The RR database holds the detailed results, typically containing multiple records for each study.Each record is linked to the relevant study via the study name, and holds details of a specific risk estimate.It records the type of estimate, its value and confidence interval, its source and other details such as the age range included in the estimate if this is different from the overall study age range.Some estimates were taken directly from the source paper.Others were derived using the details provided in the paper.
Where no RR estimate was given or a RR estimate was given without a confidence interval, information on the sample size and the number of deaths was used to estimate these.Estimates for separate independent subsets of the population such as age groups were combined using simple meta-analysis.Non-independent RRs using a common comparison group (e.g., never smokers) were combined using the Hamling method[10].This method was used to combine RRs by number of cigars smoked per day and to combine RRs for former and current smokers to give an estimate for ever smokers.It was also used to estimate risk for overall circulatory disease when the study provided separate estimates for cerebrovascular disease and a broad definition of coronary heart disease, and to estimate overall stroke from separate risk estimates for ischaemic and haemorrhagic stroke.The International Classification of Disease codes used to define IHD, stroke and circulatory disease can be found at https://coder.aapc.com/icd-10-codes-range/110.
Each extract was carried out by one of the authors, the entered data and any additional calculations then being reported and checked by another of the authors, with problems discussed and amendments made until both agreed that the data entered were a true representation of the study data.
Dose-response data on risk by number of cigars smoked per day were also identified and are discussed below.
Statistical analysis
For each disease considered, fixed-effect and random-effects meta-analyses were conducted using the Fleiss and Gross method[11], with heterogeneity quantified by H, the ratio of the heterogeneity to its degrees of freedom, which is directly related to theI2statistic[12]by the formulaI2= 100 (H-1)/H.
Whenever more than one paper provided equivalent results for a study, only one result was included in a meta-analysis.The selection of the result was based on four criteria: Prospective follow-up was given preference over cross-sectional analysis at baseline; the longest follow-up reported (for prospective studies); the widest age range reported; and finally the RR adjusted for the most confounding factors.
Some papers provided results for comparisons that did not exactly match our selection criteria.Where any were relevant to a meta-analysis, the analysis was performed excluding those results, and then including them in a sensitivity analysis.
The KAISER study[13]used a questionnaire that asked about the participant’s history of cigarette smoking and their current pipe and cigar smoking.Ever cigarette smokers were excluded from their analyses.It was, therefore, possible to identify participants who had never smoked cigarettes and who did not, at baseline, smoke cigars or a pipe.This is not completely equivalent to our requirement for the comparison group to be never smokers of any tobacco product.Also, the participants categorised as current cigar smokers may have included former pipe smokers.However, the study was large (1546 current cigar smokers and 16228 never cigarette smokers) and had a long followup (25-26 years) so justified inclusion in sensitivity analyses.
For the MALHOT study a pooled analysis of data from five large prospective studies was reported[14].Of these studies, two (the Netherlands Cohort Study and the Melbourne Collaborative Cohort Study) were conducted outside the United States, while the other three (the VITamins And Lifestyle study, the NIH-AARP Diet and Health study and the Prostate, Lung, Colorectal and Ovarian Cancer Screening Trial) were conducted in the United States.However, the studies in the United States were larger and formed 85.7% of the total population reported, and the largest of the studies (NIH-AARP) followed up participants for a median of 15.5 years.The size of this pooled analysis, the large proportion of participants from the United States, the long follow-up in the largest study, and the lack of study-specific reports relating to cigar smoking for the studies pooled justified including the combined results in sensitivity analysis.
For the NHIS study, a cross-sectional analysis of baseline data[15]reports results for a definition of “Heart conditions” including angina, coronary heart disease, heart attack and other heart disease which is too broad for the results to be included in our main analysis of ischaemic heart disease (IHD).However, as the report considers data from four years’ surveys of this large, repeated, nationally representative study, and as no other source was found that reported IHD for this study, it was decided to include its results in sensitivity analysis.
Also for the NHIS study, an analysis of prospective findings from six years’ survey data with follow up for at least five years, the source publication[16]reports results for a broad definition of coronary heart disease which includes rheumatic fever, some hypertensive heart disease, IHD and some other heart disease.Though this definition is too broad to be included in our analyses of IHD, the paper also reports results for cerebrovascular disease (stroke), and taken together, the definitions of coronary heart disease and cerebrovascular disease were very close to our ideal definition of circulatory disease.We therefore combined the results for coronary heart disease and for cerebrovascular disease, and included the resulting estimates in the sensitivity analyses for overall circulatory disease.
The NLMS study[17]reported too broad a definition of cardiovascular disease, an ideal definition of stroke and a definition of circulatory disease that included all the relevant disease categories except diseases of the veins and other diseases of the circulatory system.The reported results for stroke were included in the main metaanalyses and the results for circulatory disease were included in sensitivity analysis only.
RESULTS
Literature search
For lung cancer, 17 publications were identified that were relevant to the metaanalyses (including the sensitivity analyses), 13 from the previous review[9], three from additional searches, and one from reviews identified in the searches, as shown in Figure 1.Two of these[18,19]are by the same authors reporting the same study, the first giving overall study information and the second giving results by disease, so only the latter is cited in the analysis results.For COPD, four publications were identified (Figure 2), while for heart disease, stroke and circulatory disease 12 were found (Figure 3).
Studies
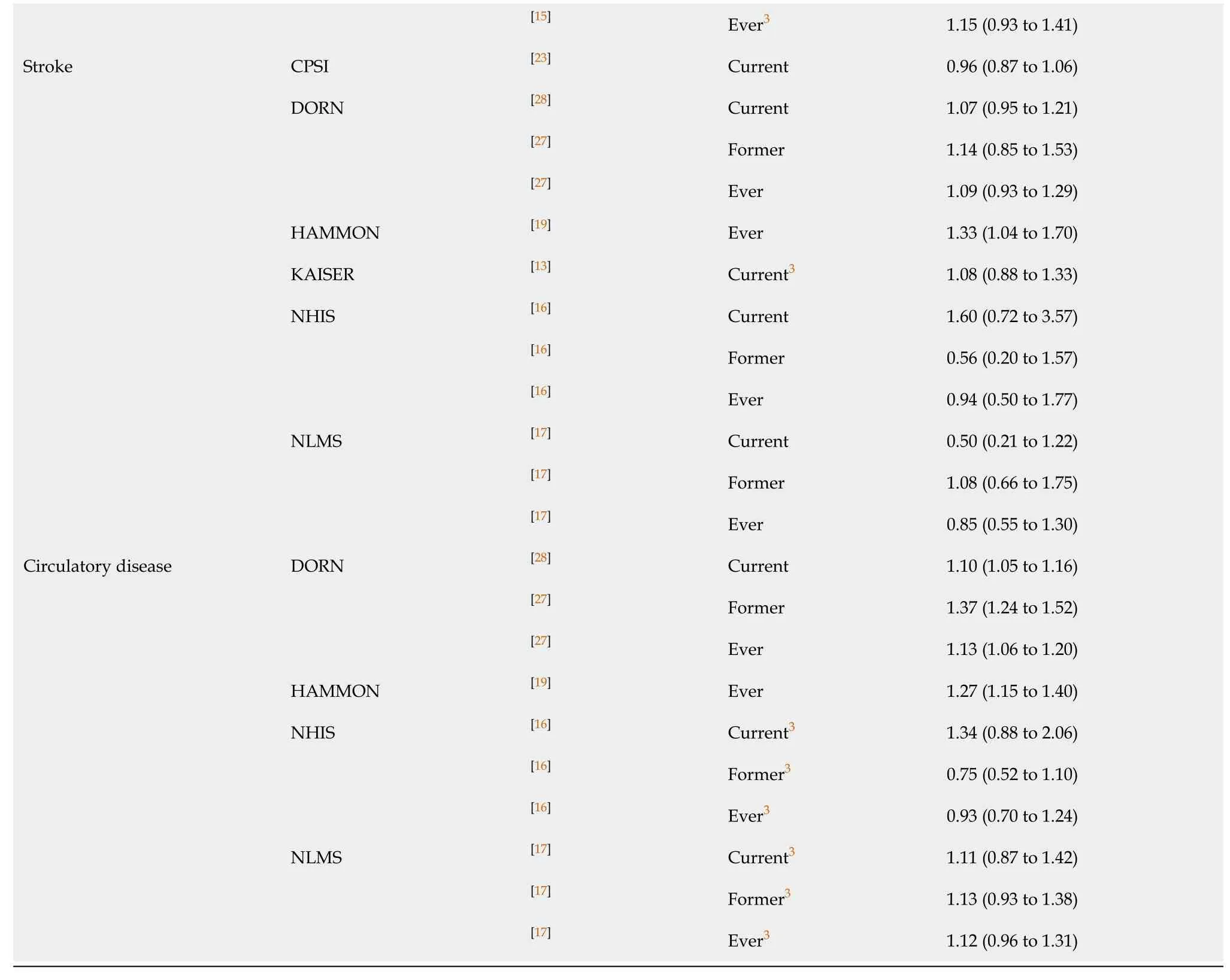
Table 1[13,14,17-31](lung cancer), Table 2[13,17,23,27](COPD), and Table 3[13,15-17,19,21,23,26-28,32,33](heart disease, stroke and circulatory disease) present details on each study, including its name, the source publications, the study type, the years of follow-up, the study size, and the sexes and age groups considered.Results used in sensitivity analyses only are marked with an asterisk.Table 3 also includes details of the definition of heart disease, stroke and circulatory diseases.
For lung cancer, the 17 publications relate to 11 studies, though two (KAISER, MALHOT) are only used in sensitivity analyses.Eight of the studies are of prospective design and three case-controls.Except for NLMS, which considers both sexes, all provide results only for males.The studies vary widely in size, with three involving over 400000 people, and four less than 10000.
For COPD, the four publications concern separate studies, though again KAISER is only used in sensitivity analyses.All the studies are prospective, with all except NLMS considering only males.All four of these studies also provide results for lung cancer.The study size in KAISER is much lower than in the other three studies.
For heart disease, stroke and circulatory disease, the 12 publications concern eight studies: Six prospective, one case-control and one reported both as a cross-sectional analysis of baseline data and using prospective follow-up.KAISER (all results), NHIS (prospective results for circulatory disease and cross-sectional results for ischaemic heart disease) and NMLS (results for circulatory disease) were only used in the sensitivity analyses.Most results were for men only, the exceptions being those from NHIS and NLMS that were for the sexes combined.As for lung cancer, the studies varied widely in size.
Overall, as many studies provided data for more than one disease, there were 13 studies, of which two only provided results for the sensitivity analyses and two others had some results restricted to sensitivity analyses.
Meta-analyses
The individual study RR estimates used are given in Table 4[13-17,19,20,22,23,25,27-33], with the results of the meta-analyses conducted summarised in Table 5.Unless otherwise stated references to combined estimates are to random-effects estimates, with 95%CI given in parentheses.
Lung cancer
For current smokers there was highly significant heterogeneity (P< 0.001) between the five estimates, which ranged from 1.66 (1.18 to 2.34) for DORN to 5.10 (4.00 to 6.60) for CPS II.The overall estimate was 3.12 (2.11 to 4.62).Including the result from study KAISER little affected the combined estimate, which became 2.98 (2.08 to 4.26).
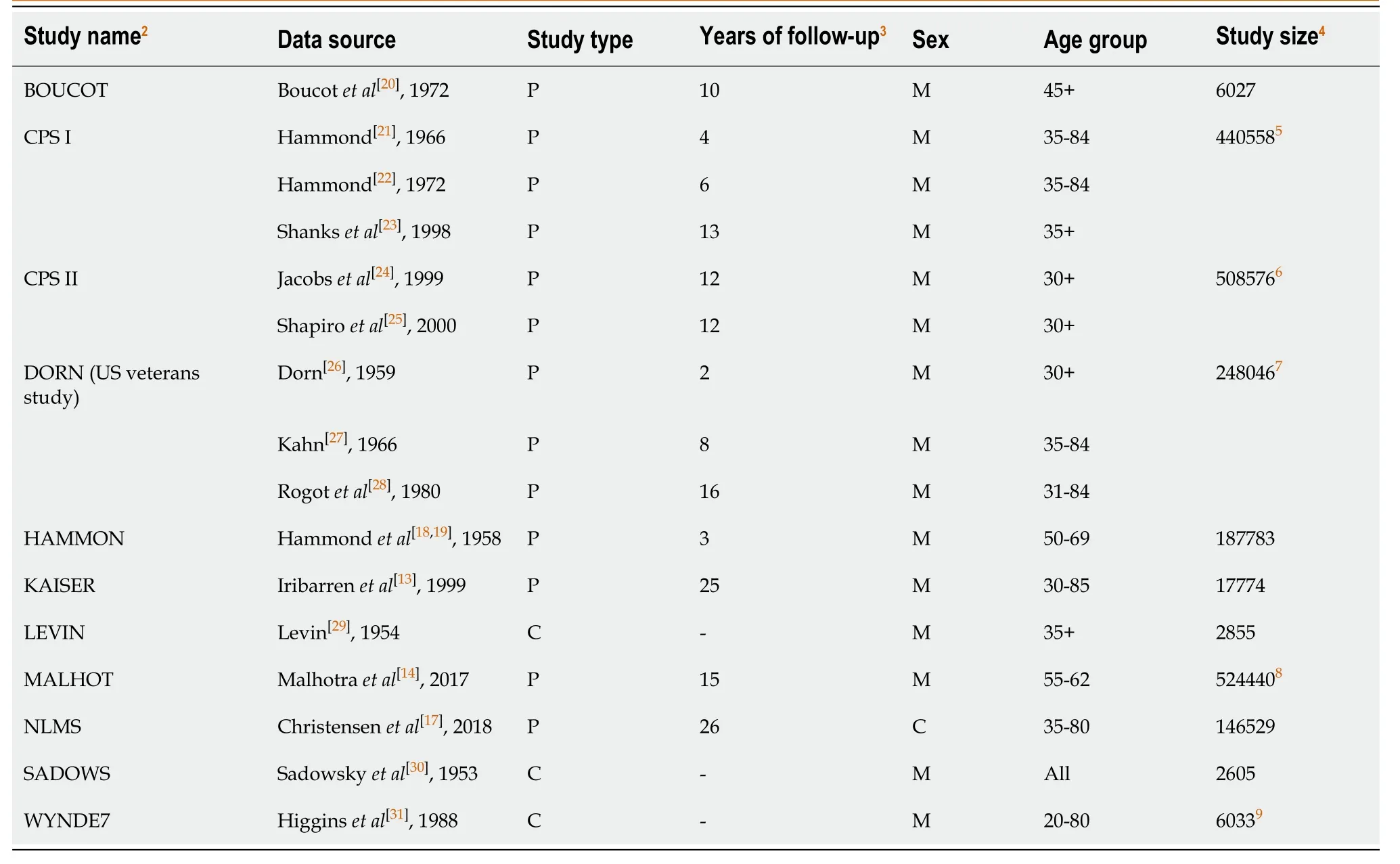
Table 1 Studies in meta-analysis of lung cancer and exclusive cigar smoking1
The four results for former smokers showed no significant heterogeneity (atP< 0.1), and gave a somewhat lower estimate of 1.61 (1.23 to 2.09).
The nine results for ever smokers showed significant (P< 0.05) heterogeneity due to the high estimate from BOUCOT of 8.81.The rest of the estimates ranged from 1.02 to 3.01.The overall estimate was 2.11 (1.64 to 2.72).When the result from MALHOT was included, this became 2.22 (1.79 to 2.74).
COPD
None of the analyses showed significant heterogeneity, and there was very limited evidence of an association.Results were available from only four studies and for only two of these were results available for each of the exposures current, former and ever smokers (Table 4).This resulted in all the combined estimates being based on between two and four results.For current smokers the overall estimate was slightly raised at 1.42 (0.89 to 2.26) excluding KAISER and 1.44 (1.16 to 1.77) including KAISER, but no increase was seen for ever smokers 0.86 (0.48 to 1.54).For former smokers, the overall estimate of 0.47 had an extremely wide CI of 0.02 to 9.88, based on individual estimates of 0.05 (0.00 to 3.19) and 1.38 (0.42 to 4.51).
IHD, stroke and circulatory disease
As is evident from Table 5, overall estimates generally only slightly exceeded 1.00, though some of those for IHD and circulatory disease, but not stroke, were significantly raised (atP< 0.05).There was also evidence of heterogeneity in some of the meta-analyses presented.Generally, the results from the sensitivity analyses were similar to those from the main analyses, so only the former set of results, which involve more studies, are considered below.
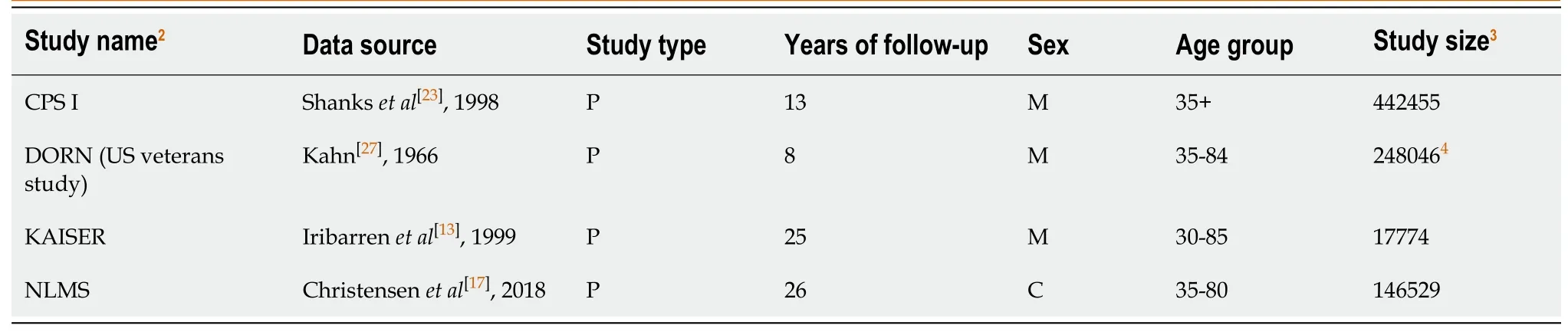
Table 2 Studies in meta-analysis of chronic obstructive pulmonary disease and exclusive cigar smoking1
For ischaemic heart disease, the estimates were somewhat higher for former than current smokers, being 1.11 (1.04 to 1.19) for current smokers, 1.26 (1.03 to 1.53) for former smokers, and 1.15 (1.08 to 1.23) for ever smokers.
For stroke, the estimates were all closer to 1.00, but again somewhat higher for former than current smokers, being 1.02 (0.92 to 1.13) for current smokers, 1.08 (0.85 to 1.38) for former smokers, and 1.11 (0.95 to 1.31) for ever smokers.
For overall circulatory disease, the three estimates were quite similar, being 1.10 (1.05 to 1.16) for current smokers, 1.11 (0.84 to 1.46) for former smokers and 1.15 (1.06 to 1.26) for ever smokers.
Dose-response data
Many studies did not provide data on risk by number of cigars smoked per day.Table 6[13,17,23,27,30,32,33]summarizes the limited data available from six studies, five of which provided data for ischaemic heart disease, four for lung cancer, and two for COPD.With the possible exception of the result for the SADOWS study, the data for lung cancer seemed consistent with an increasing risk with increasing amount smoked.The data for COPD and for ischaemic heart disease, however, did not consistently show any clear increase in risk with amount smoked.
DISCUSSION
The meta-analysis results show some increase in risk among exclusive cigar smokers for each disease studied, except for stroke where all the risk estimates were close to 1.For current smoking the overall estimates in the sensitivity analyses were 2.98 for lung cancer, 1.44 for COPD and 1.11 for ischaemic heart disease.These are much lower than those associated with cigarette smoking: For the United States, estimates for current cigarette smokers[34]are 11.68 for lung cancer and 4.56 for COPD; for ischaemic heart disease[34]the current cigarette smoker estimate for age 65 to 74 is 1.70, with estimates for younger ages being higher.Even for heavy cigar smokers, the RRs shown in Table 6 are still generally lower than the estimates for overall cigarette smoking.For former smoking the estimates of 1.61 for lung cancer, 0.47 for COPD (though based on only two widely differing estimates) and 1.26 for ischaemic heart disease are again much lower than those for cigarette smoking.Similar results were observed for ever smoking.
There are some limitations with the data available for our analyses.Several of the studies were conducted some time ago.The numbers of exclusive cigar smokers participating in the studies were often quite low.Very few studies have reported results for exclusive cigar smokers.For many of these studies, cigar smoking is not the primary focus of the study.This suggests that there may be reporting bias, in that other studies may have had relevant data but did not report a non-significant finding for the study’s small number of cigar smokers.
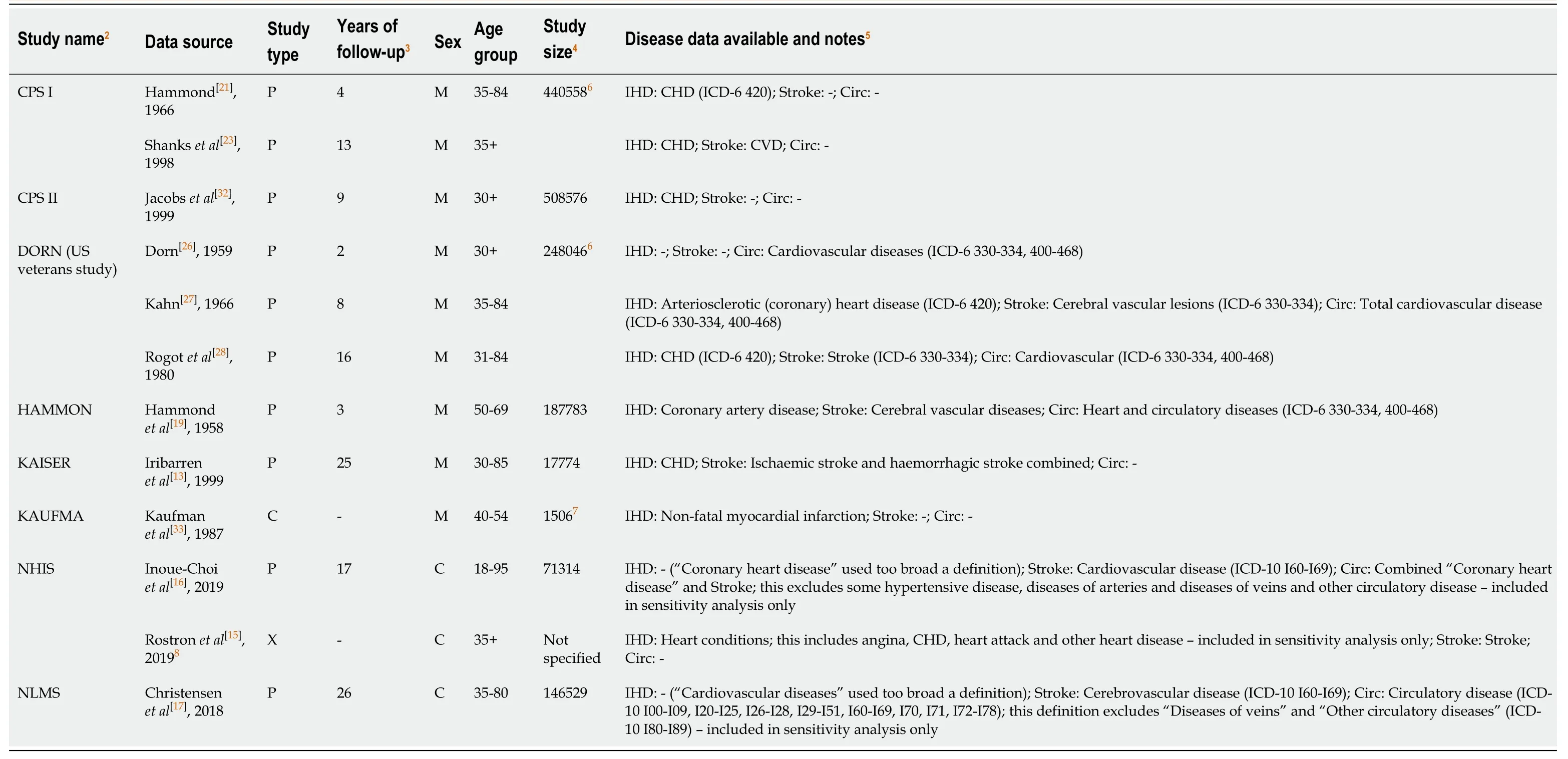
Table 3 Studies on ischaemic heart disease, stroke and circulatory disease and exclusive cigar smoking1
There was a limited amount of dose-response data, and a lack of data on how risk varied by type of cigar smoked.No meta-analyses could be carried out by subgroups such as race and age and gender, as there was insufficient data.No study reported results for sex separately, so no analysis by sex could be done.
Nevertheless, the data provide fairly clear evidence that exclusive cigar smoking is associated with an increased risk of lung cancer, though less markedly than is the case for exclusive cigarette smoking.For COPD and ischaemic heart disease, the association is weaker, and is also less than that for cigarette smoking.
How do these results compare with previous estimates? It should be noted that no other review has provided meta-analysis estimates for exclusive cigar smokers in the United States, and that many of the previous reviews considered below were conducted many years ago.
The review of smoking and lung cancer[9]referred to under literature searches provided random effects meta-analysis estimates for lung cancer in current, former and ever exclusive cigar smokers of 4.67 (n = 15), 2.85 (n = 5) and 2.95 (n = 15) respectively, but these analyses were not restricted to studies in the United States.The risk estimates included in those analyses showed significant heterogeneity.A review by Wynder et al[35]considering the risk of lung cancer in pipe and cigar smokers noted that, in prospective studies in North America the mortality ratios were in the range 2 to 6.For retrospective studies, mostly conducted in Germany and Switzerland, “it appears that the risk of lung cancer is higher than that for such smokers in the United States”.This review suggested that these differences stemmed from different patterns of inhalation in the two regions.A similar review by Higgins et al[31], also considering pipe and cigar smokers, again suggested that risk estimates from prospective studies in North America are lower than those from case control studies in Europe.Smoking and Tobacco Control Monograph No.9[23], reviewing data from CPS-I, stated that “Lung cancer mortality ratios increase with increasing number of cigars smoked per day and with increasing depth of inhalation.When depth of inhalation and number of cigars per day are examined together, depth of inhalation is more powerful in predicting lung cancer risk than number of cigars smoked per day.” The 1979 report by the Surgeon General[36]summarised the available evidence as “Several prospective epidemiological studies have demonstrated higher lung cancer mortality ratios for pipe and cigar smokers than for nonsmokers, but the risk of developing lung cancer for pipe and cigar smokers is less than for cigarette smokers”.
Smoking and Tobacco Control Monograph No.9[23]also reported estimates for COPD risk.It concluded that “The data taken as a whole support the conclusion that cigar smoking can cause COPD in smokers who inhale deeply”.
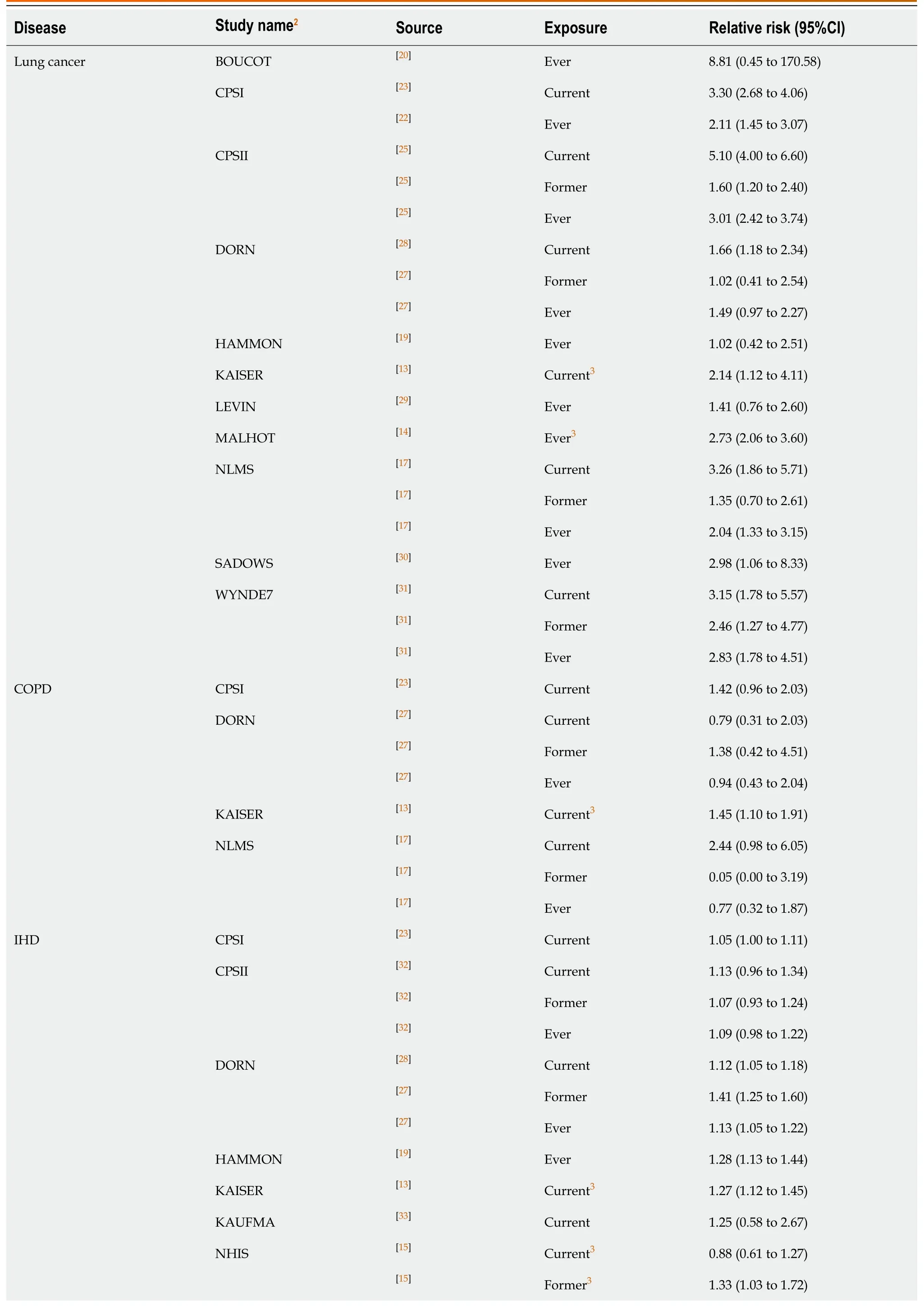
Table 4 Individual estimates used in the meta-analyses1
1Compared with never smoking any tobacco product.2Study name is an identifier assigned by the authors based on the published study name or the name of the first author of the source paper.This identifier is used in the meta-analysis output.3These results were only included in the sensitivity analyses.COPD: Chronic obstructive pulmonary disease; IHD: Ischaemic heart disease.
The same Monograph reviews coronary heart disease risk, concluding that “The studies of cigar smoking and coronary events present a pattern of slightly elevated rates among cigar smokers who smoke heavily or inhale deeply”.The Surgeon General’s 1983 report[37]states that “In general, the risk for coronary heart disease mortality of smoking pipes and cigars is substantially lower than the risk of smoking cigarettes.This is generally felt to be due to the tendency of pipe and cigar smokers not to inhale smoke into the lung”.
For risk of stroke, the Surgeon General’s 1983 report[37]cited results from the United States Veterans study[28](which are included in this review), stating that “Mortality ratios for stroke were near unity for smokers of only cigars or pipes – l.07 and 0.99, respectively.” As noted for lung cancer, there may be differences in stroke risk estimates between studies in the United States and in Europe.Smoking and Tobacco Control Monograph No.9[23]states “It is difficult to reconcile the results from the European studies and the CPS-I results.The CPS-I primary cigar data are primarily individuals who report that they do not inhale (78 percent), while inhalation information is not provided by the other studies.If inhalation rates are much higher in the European studies, this could explain some of the differences found in the RR of stroke between the two groups of studies.”
Generally, these results reach conclusions quite similar to ours, and suggest that the conclusions we have drawn from our review of the evidence from the United States may not necessarily apply to cigar smoking in Europe.
In conclusion, we find that exclusive cigar smoking is associated with a moderate increase in risk of lung cancer, and a smaller increased risk of COPD and IHD, and that these increases in risk are less than for cigarette smoking.
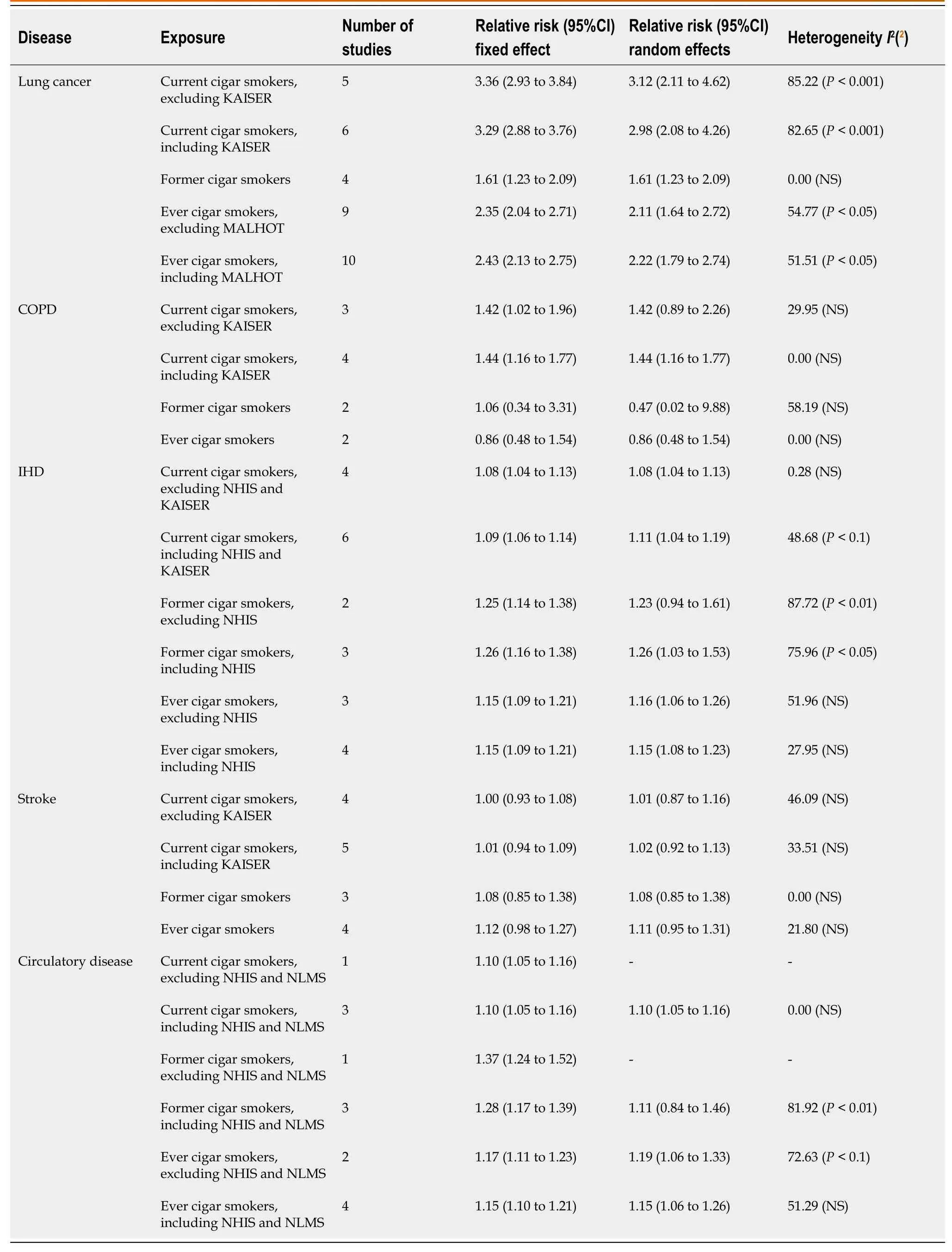
Table 5 Meta-analysis results for lung cancer, chronic obstructive pulmonary disease, ischaemic heart disease, stroke and circulatory disease for cigar smoking1
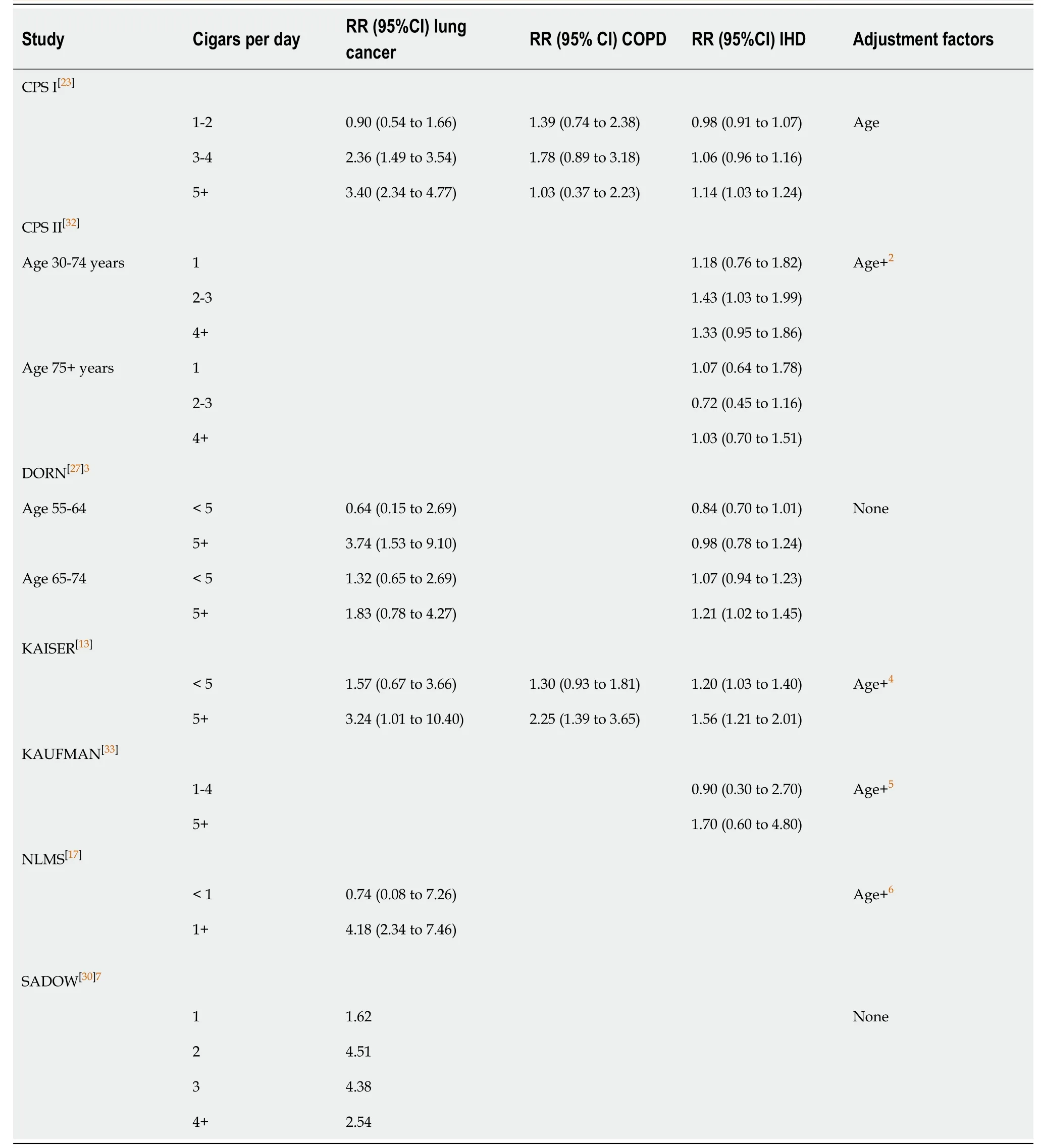
Table 6 Relative risks and 95%CIs by current amount smoked1
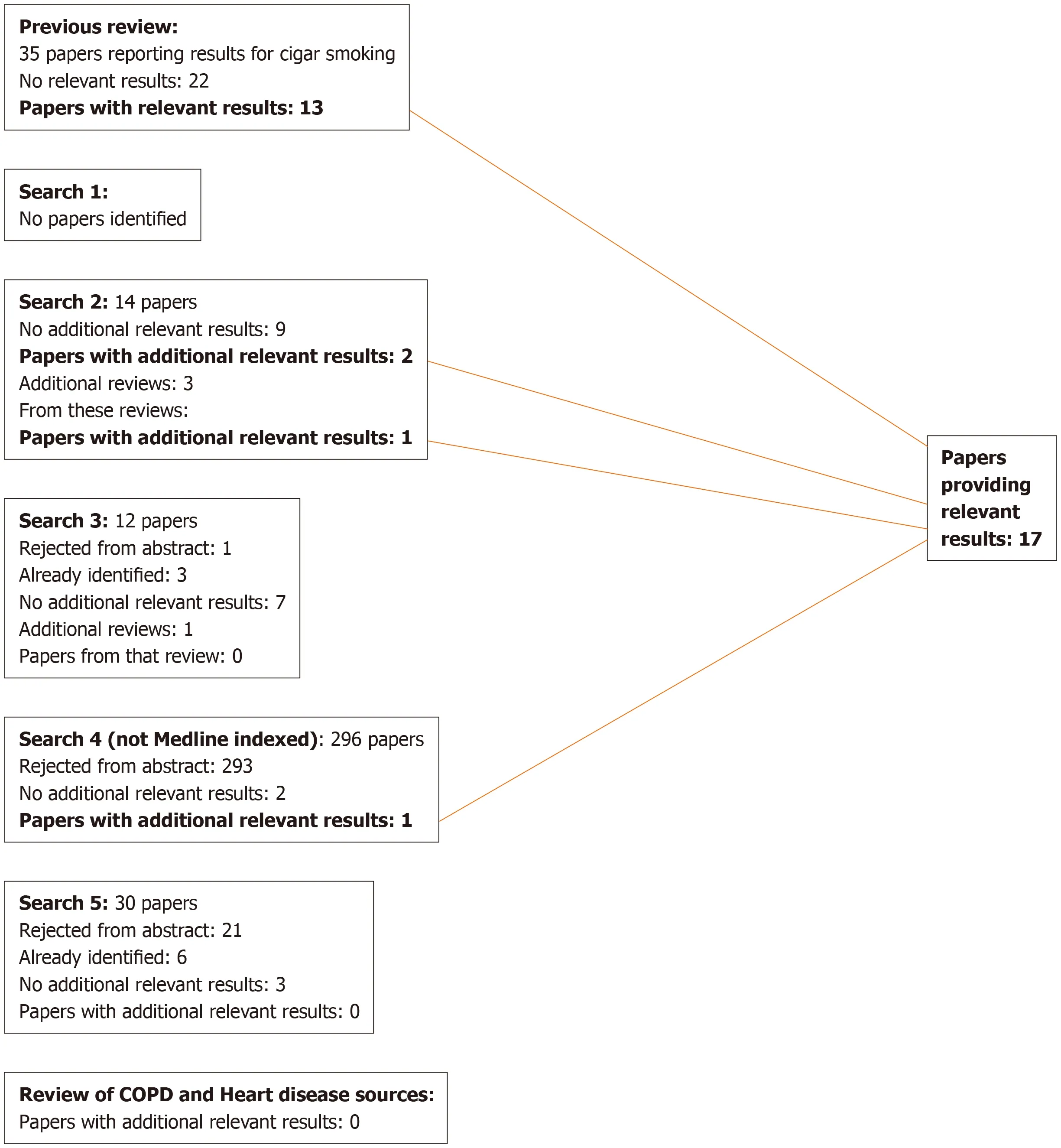
Figure 1 Lung cancer searches.COPD: Chronic obstructive pulmonary disease.

Figure 2 Chronic obstructive pulmonary disease searches.
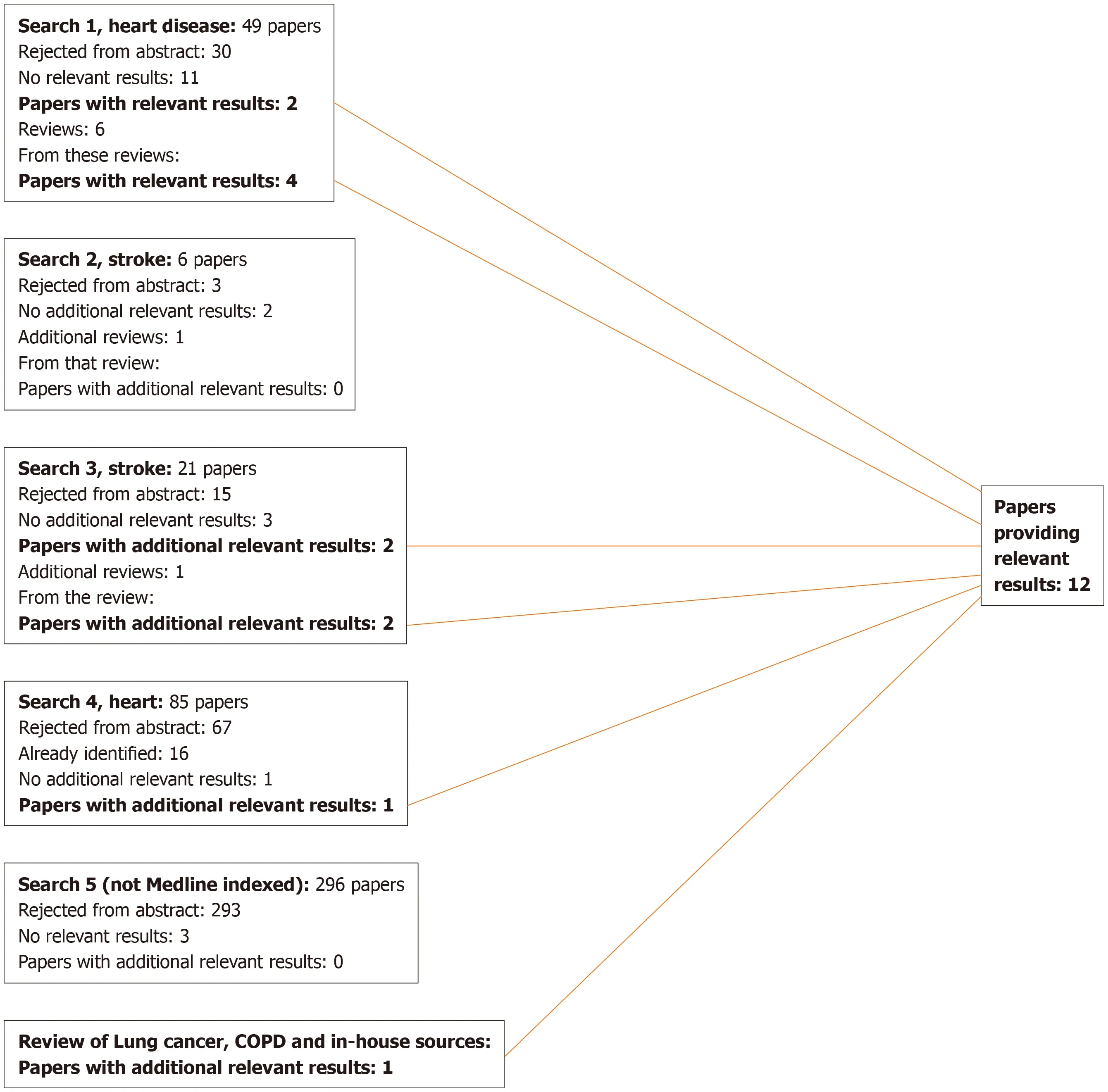
Figure 3 Heart disease, stroke and circulatory disease searches.COPD: Chronic obstructive pulmonary disease.
ARTICLE HIGHLIGHTS
Research background
Many reviews have studied the relationship of smoking to lung cancer, chronic obstructive pulmonary disease (COPD), heart disease and stroke, but the effects on these diseases of cigar smoking, particularly exclusive cigar smoking, have rarely been considered.
Research motivation
As the United States is a country with a large population and a relatively high percentage of cigar smokers, we felt that insight into the effects of exclusive cigar smoking could usefully be gained from studies conducted there.
Research objectives
To carry out a systematic review of the relationship of exclusive cigar smoking to the four main smoking-related diseases in studies conducted in the United States.
Research methods
Literature searches were conducted to identify studies in the United States that reported risk of lung cancer, COPD, heart-disease, stroke and/or overall circulatory disease comparing cigar smokers who had never smoked other tobacco products with those who had never smoked any tobacco.For each study identified as providing relevant results, data were recorded on study characteristics and on the appropriate relative risks (RRs) and 95%CIs relating to overall current, former and ever exclusive cigar use, and, for current smokers, by daily cigar consumption.RRs for a given smoking group and disease were combined using fixed-effect and random-effects meta-analyses.
Research results
Data were available on lung cancer from 11 studies, on COPD from four studies and on heart disease, stroke and circulatory disease from 10 studies.As RRs tended to be heterogeneous, random-effects estimates are given below.For current smoking overall RR estimates were 2.98 (95%CI: 2.08 to 4.26, based onn= 6 estimates) for lung cancer, 1.44 (1.16 to 1.77,n= 4) for COPD, 1.11 (1.04 to 1.19,n= 6) for ischaemic heart disease, 1.02 (0.92 to 1.13,n= 5) for stroke and 1.10 (1.05 to 1.16,n= 3) for overall circulatory disease.These RRs are much lower than those reported for the United States for exclusive cigarette smokers; 11.68 for lung cancer, 4.56 for COPD and at least 1.70, depending on age, for ischaemic heart disease.Even for heavy cigar smoking, RRs are generally lower than for overall cigarette smoking.RRs for former and for ever smoking were also much lower than for cigarette smoking.
Research conclusions
Although our analyses were based on relatively few studies, some conducted some time ago, the results clearly show that exclusive cigar smoking is associated with an increased risk of lung cancer, though much less than is the case for exclusive cigarette smoking.For COPD and ischaemic heart disease the association is weaker, and also less than for cigarette smoking.No previous study has clarified the effects of exclusive cigarette smoking so clearly.Future research could extend results on exclusive cigar smoking to countries other than the United States, and compare risks of cigar smoking with those of using other nicotine products.
Research perspectives
While our results show that exclusive cigar smoking is associated with risks of smoking-related diseases that are much lower than those associated with cigarettes smoking, little of the evidence comes from studies conducted in this millenium.Further large prospective studies are needed to collect more up-to-date results, and to clarify how risk varies by type of cigar smoked.
ACKNOWLEDGEMENTS
We thank Barbara Forey for assistance with the literature searching and study selection, and comments on drafts of the paper, and also John Fry and John Hamling for assistance with conduct of the meta-analyses.We also thank Yvonne Cooper and Diana Morris for typing the various drafts of the paper.
 World Journal of Meta-Analysis2020年3期
World Journal of Meta-Analysis2020年3期
- World Journal of Meta-Analysis的其它文章
- Prevalence of anxiety among gestational diabetes mellitus patients: A systematic review and meta-analysis
- Hydatidosis and the duodenum: A systematic review of the literature
- Role of non-coding RNAs in pathogenesis of gastrointestinal stromal tumors
- Thrombopoietin-receptor agonists in perioperative treatment of patients with chronic liver disease
- Combined endoscopy/laparoscopy/percutaneous transhepatic biliary drainage, hybrid techniques in gastrointestinal and biliary diseases
- Immunotherapy in hepatocellular carcinoma: Combination strategies