
Combined endoscopy/laparoscopy/percutaneous transhepatic biliary drainage, hybrid techniques in gastrointestinal and biliary diseases
2020-12-16 09:00:44YiLongFengJingLiLianSongYeXianHuiZengBingHu
World Journal of Meta-Analysis 2020年3期
Yi-Long Feng, Jing Li, Lian-Song Ye, Xian-Hui Zeng, Bing Hu
Yi-Long Feng, Jing Li, Lian-Song Ye, Xian-Hui Zeng, Bing Hu, Department of Gastroenterology, West China Hospital, Sichuan University, Chengdu 610041, Sichuan Province, China
Abstract
Key words: Hybrid technique; Laparoscopic and endoscopic cooperative surgery; Endoscopic retrograde cholangiopancreatography; Laparoscopic-assisted endoscopic retrograde cholangiopancreatography; Rendezvous technique; Magnetic compression anastomosis
INTRODUCTION
In recent years, a wide range of gastrointestinal endoscopy techniques have been developed, such as endoscopic submucosal dissection (ESD) and endoscopic retrograde cholangiopancreatography (ERCP).ESD is now widely carried out for early neoplastic lesions of the gastrointestinal tract and has advantages of minimal invasion, low cost, patient tolerance and better quality of life of patients[1].However, ESD is confined to incision of mucosal and submucosal layers.Laparoscopy is able to perform the full thickness resection, but sometimes laparoscopy cannot determine the precise incision line from the peritoneal cavity.ERCP has matured into an essential technique for managing biliary and pancreatic disorders, but it can be technically difficult in some situations (e.g., completely biliary obstruction and altered anatomy) where percutaneous transhepatic biliary drainage (PTBD) may get access to the biliary tree.
In brief, none of these techniques can overcome all the difficulties encountered in the clinical practice.Therefore, many hybrid techniques that combine two or more of endoscopy, laparoscopy and PTBD have been developed that have the advantages of different procedures and negate their limitations at the same time.This review aims to introduce these hybrid techniques and their applications for the treatment of gastrointestinal and biliary diseases.
COMBINATION OF ENDOSCOPY AND LAPAROSCOPY
Resecting the gastrointestinal tumors
Gastrointestinal submucosal tumors (SMTs) are frequently seen in patients undergoing upper gastrointestinal endoscopy[2], and gastrointestinal stromal tumor is the most common type of SMT[3].Usually, SMTs are treated by surgical approaches.Laparoscopic wedge resection has been confirmed a feasible option for SMT < 5 cm[4].However, localization of small and intraluminal growing SMTs is difficult from the peritoneal cavity.As a result, excessive resection is needed to ensure the negative surgical margins, which can cause the deformity of the remaining stomach and gastric malfunction.
In order to decrease the resection area as much as possible, Hikiet al[5]firstly reported the conventional laparoscopic and endoscopic cooperative surgery (LECS) where the resection is performed jointly by the endoscopy and laparoscopy.Endoscopic submucosal dissection is used in this surgery.Firstly, the periphery of the tumor is marked by coagulation.Then three-fourths of the marked areas are cut down to the submucosal layer after submucosal injection.Next, a perforation of the gastric wall is created artificially, and the tip of the ultrasonically activated device is inserted into the perforation hole.Then three-fourths of the seromusclar layer is dissected along the incision line.After the tumor is inverted into the abdominal cavity, the serosa of the unresected tumor is grasped and retracted, and finally the incision line is closed by a laparoscopic stapler (Figure 1).
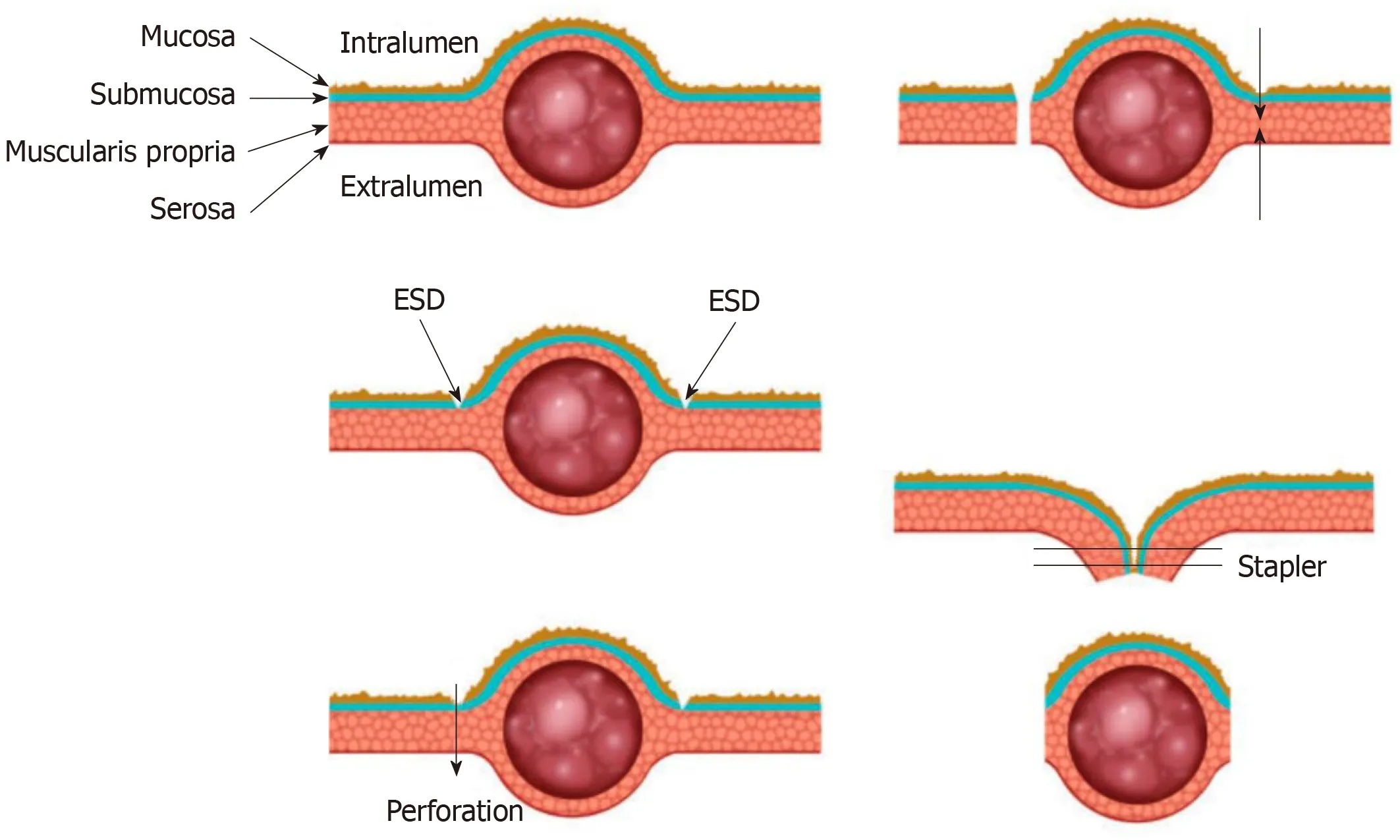
Figure 1 Conceptual diagram of the classical laparoscopic endoscopic cooperative surgery procedure[14].ESD: Endoscopic submucosal dissection.Used with permission from John Wiley and Sons.
After the emergence of LECS, several modified LECS were developed excessively, including inverted LECS[6], laparoscopic assisted endoscopic full thickness resection[7,8], combination of laparoscopic and endoscopic approaches for neoplasia with non-exposure technique[9], non-exposed wall invasion surgery (NEWS)[10]and closed-NEWS[11].Based on whether the gastric wall is open during the surgery, these techniques can be divided into exposed technique and non-exposed technique.Table 1 compares characteristics of these two techniques.Though there are differences among these techniques, in general they all consist of two main parts that are the ESD technique and the laparoscopic surgery.The endoscopist determines the precise margin of the tumor, and then the resection is performed jointly by the endoscopy and laparoscopy.
As a less invasive approach, LECS has advantages of minimum resecting area and reserving function of organs at the greatest extent.In addition, LECS can be applied to tumors located in the esophagogastric junction or pyloric ring that cannot be removed by laparoscopic wedge resection[12,13].The exposed LECS has a risk of tumor seeding and contamination of gastric juice in the peritoneal cavity due to the artificial perforation of the gastric wall[14].The non-exposed LECS avoids the gastric open during the surgery and thus expands the indication of LECS for gastric epithelial neoplasms[15].A series of studies on LECS and modified LECS have been conducted, showing that these techniques are feasible and safe for gastric SMTs[2,16-19].
Besides gastric tumors, LECS has been used to resect tumors in other parts of the gastrointestinal tract.There are a few reports of LECS for early superficial duodenal tumors (SDT), showing that this technique may be safe and feasible and could be an option for surgical SDT resection[37-25].Standard treatment for SDT has not been established.Though ESD has been considered safe and effective for early gastric tumors, ESD for early duodenal cancer is associated with a high risk of perforation during and after surgery as a result of the narrow lumen and thin walls of the duodenum[26,27].In LECS, the laparoscopic suture and monitoring may help to prevent the occurrence of perforation.Therefore, compared to ESD, LECS might be a safer approach for the treatment of SDT.For colon polyps and colorectal tumors that cannot be removed by conventional endoscopic techniques, LECS may also be an alternative choice[28].
Localization of gastrointestinal tumors
Endoscopic localization is essential in both endoscopic procedures and surgeries.In laparoscopy, endoscopic tattooing that uses suspensions of carbon particles is a commonly used approach to localize the tumor during laparoscopy.However, intraoperative endoscopic localization may be difficult to arrange between endoscopic and surgical teams.Huet al[29]reported performing tumor resection using an ultrasonic scalpel through a gastric fistula formed by percutaneous endoscopic gastrostomy.Some novel methods may provide other choices for preoperative localization of tumors.Ohdairaet al[30]applied a magnet-string-clip system to gastric mucosa in 15 patients with early gastric cancer, and the tumor site was detected in all cases during laparoscopic gastrectomy.Hyunet al[31]introduced an endoscopic fluorescent band ligation method.The fluorescent rubber bands were endoscopically placed on the mucosa of porcine stomachs and colons, and the bands were clearly identified using the near-infrared fluorescence laparoscopy system during subsequent surgery.
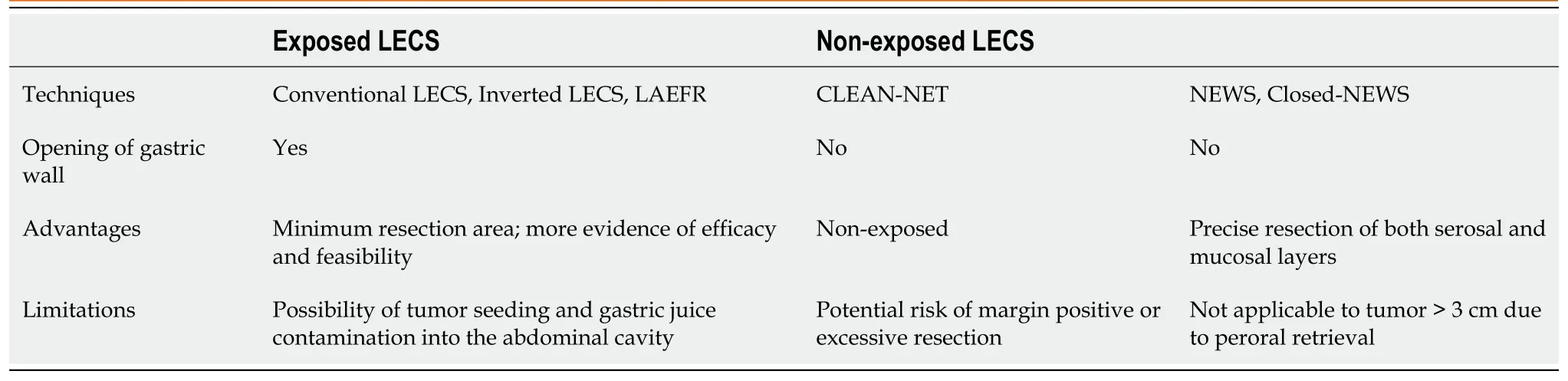
Table 1 Comparison between the characteristic of exposed laparoscopic endoscopic cooperative surgery and non-exposed laparoscopic endoscopic cooperative surgery
Air leak test by intraoperative endoscopy
Anastomotic leak (AL) is one of the most frequent and devastating complications after many gastrointestinal surgeries[32,33].Among measures that have been used to prevent AL, intraoperative air leak test (ALT) is the most widely used to identify a mechanically insufficient anastomosis[32].The bowel proximal to the anastomosis is clamped, and then air is insufflated into the bowel lumen using a syringe or endoscope with the anastomosis under irrigation of saline.Leakage is detected by the bubbles arising from the anastomosis.
Compared to syringe, the intraoperative endoscopy can simultaneously provide air insufflation with adequate and steady pressure for ALT[33].More importantly, it enables real-time assessment of anastomotic integrity, bleeding, vascular insufficiency and allows for repeatability if a leak is repaired[34].The intraoperative ALT is easy, quick and associated with little or no risk[35].One prospective randomized controlled trial showed that intraoperative endoscopy had significant lower rate of AL and lower need for reoperation than simple visual inspection in laparoscopic Roux-en-Y gastric bypass (RYGB)[36].For colorectal surgeries, intraoperative endoscope has also been confirmed safe and effective[37-39].
COMBINATION OF ERCP AND PTBD
Rendezvous technique
ERCP has become the first choice of treatment for many biliary diseases, including bile duct injuries, obstruction and stenosis.Endoscopic treatment of the biliary stricture relies on initial passage of a guidewire across the stricture, followed by subsequent stricture dilation and stent placement[40].However, this maneuver is not possible when the biliary duct is completely obstructed or transected.The rendezvous technique could be a choice for the recanalization of bile duct in this situation.
The rendezvous technique that combines endoscopic and percutaneous transhepatic approach was initially described for duodenoscopic sphincterotomy in the 1980s[41,42].A guide wire is placedviathe PTBD route, advanced into the duodenum, then grasped by grasping forceps or snares of the duodenoscope and pulled out of the duodenoscope.Then a catheter is advanced into the bile duct over the guidewire for drainage.Stents or balloons can also be placed to dilate the stricture of the bile duct.The procedure can also be completed in a reverse way where a guide wire placed endoscopically is grasped and pulled out through the PTBD route[43,44].
Because the guide wire may be damaged during withdraw and the procedure is cumbersome, a few modified techniques have been developed to avoid these problems, such as parallel cannulation technique[45-47].With the advance in endoscopic ultrasonography (EUS) technology, the EUS guided rendezvous technique has been developed, where the bile duct is punctured under the EUS guidance, and a guide wire is advanced antegrade through the papilla to perform a transpapillary procedure[48].
The rendezvous technique increases the success rate of biliary duct cannulation and facilitates the treatment of biliary tract diseases.It is reported with a high technical success rate of 80%-100%[49-53]and a significantly lower complication rate when compared to percutaneous transhepatic cholangiography[53].The rendezvous technique can also be used to establish the continuity of the bile duct when surgical bile duct injury occurs, with a high primary success rate and a long term success rate of 55%[44].
Besides recanalization of bile ducts, the rendezvous technique is also reported to remove stones in the bile ducts[43,54,55].Lithotomy by percutaneous transhepatic approach was performed firstly, but there were stones remaining in the intrahepatic duct or common bile duct (CBD).After the guide wire was grasped, the endoscopy was inserted further with the guide wire into the hepaticojejunostomy anastomotic region or CBD and lithotomy was performed for the remaining stones.
Magnetic compression anastomosis
Besides the rendezvous technique, biliobiliary and bilioenteric anastomosis using magnetic compression anastomosis (MCA) is another choice for the treatment of severe biliary strictures or complete obstructions.The working principle of MCA is that the magnetic compression force leads to gradual tissue necrosis within magnets while with tissue healing at the edge of the magnet simultaneously[56].
Two magnets are needed for the procedure, parent and daughter magnet.These two magnets can be delivered by a variety of methods, but the most common route is by the percutaneous-peroral approach[57].One magnet is delivered through the PTBD route into the anastomosis site, and the other magnet is delivered endoscopically.When inserting a magnet into the CBD, full sphincterotomy or balloon dilation is usually required, and a metal stent may be inserted to facilitate further magnet delivery[58,59].After recanalization and magnets removal, biliary stents can also be placed to prevent restenosis[59].
Bilioenteric anastomosis is a common operation to bypass extrahepatic biliary obstructions[60].The conventional hand-sewn is time-consuming and associated with a high risk of complications[60].In contrast, the MCA is considered to be associated with little complication because fistula formation after MCA requires a relatively long time.Also, there is no dilation of fibrotic tissue in the progress of fistula formation, so the risk of restenosis upon recoiling of fibrotic tissue is low[57].
COMBINATION OF ERCP AND LAPAROSCOPY
Laparoscopic-assisted ERCP
RYGB surgery is one of the most common bariatric procedures to treat obesity[61].However, the patients have a high risk of biliary disease with up to 40% developing symptomatic cholelithiasis[61,62].In addition, ERCP is challenging due to the surgically altered anatomy.Laparoscopic-assisted ERCP (LA-ERCP) is an option for these patients.
A gastrostomy is performed by the laparoscopy, and a port is placed into the remnant stomach.Then ERCP is performed by a conventional side-view duodenoscopeviathis port (Figure 2).After completion of the procedure, the port is removed, and the defect is closed by a suture or stapler.The transgastric route is commonly used to perform the LA-ERCP, and transjejunal route has also been reported[63].Because the jejunal loop can easily reach the abdominal wall, the transjejunal LA-ERCP can be performed in all Roux-en-Y cases, even when the gastric remnant is not attainable.However, the transjejunal route needs a colonoscope to reduce the risk of intestinal injuries as a result of limited visual field of side-viewing of the duodenoscope.
LA-ERCP is a safe and highly effective therapy for patients who develop biliary diseases after RYGB surgery[64].One advantage of LA-ERCP is the high successful rate, which was reported to be approximately 90%-100%[65].Another one is that the successful rate remains high in long-limb reconstruction cases because a limb length of > 150 cm is associated with a high failure rate in other ERCP techniques[66].In addition, LA-ERCPs would be favored if the patient also requires cholecystectomy.Therefore, LA-ERCP is preferred in patients with long limbs who require concomitant cholecystectomy[65].
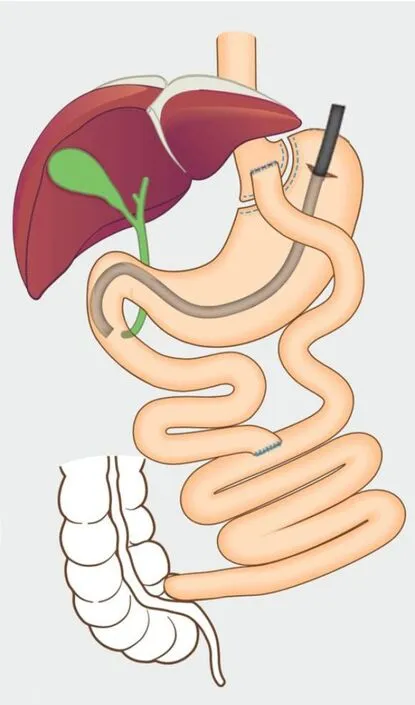
Figure 2 Laparoscopic-assisted endoscopic retrograde cholangiopancreatography in patients with Roux-en-Y anatomy[73].
Laparo-endoscopic rendezvous technique
The simultaneous presence of stones in the gallbladder and the CBD is a common clinical circumstance[67].ERCP and laparoscopic cholecystectomy (LC) are considered as standard approaches to treat CBD stones and gallstones, respectively[68,69].To perform ERCP and LC at the same time, the rendezvous intraoperative ERCP with transcystic guide-wire-assisted cannulation technique was developed as a one-stage intervention[70,71].An antegrade guidewire is inserted and advanced through Vater’s papilla into the duodenum by a surgeon.Subsequently, the guidewire is grasped by a snare and pulled out through the working channel of the duodenoscope and then cannulation of the CBD is performed.
The major advantage of the rendezvous procedure is a lower risk of pancreatic injury caused by the ERCP.The transcystic guide wire facilitates the endoscopic procedure and thus ensures elective CBD cannulation and avoids the inadvertent cannulation of the pancreatic duct.In addition, the antegrade approach avoids the problem of discordant patient positioning encountered when ERCP and LC are performed at the same time but separately.A recent meta-analysis compared different combinations of laparoscopic and intraoperative techniques (LC plus preoperative, intraoperative and postoperative ERCP and LC plus laparoscopic CBD exploration) and showed that the rendezvous approach was associated with the highest rates of safety and success[67].The major limitation is that an experienced endoscopist may not be available for the procedure, and it may be difficult to arrange and carry out the rendezvous procedures in the operating room[68,72].Moreover, using intraoperative cholangiography to detect CBD stones is essential before performing the rendezvous procedure[68].Therefore, in centers where preoperative ERCP is routinely used to detect CBD stones, this technique is not applicable.
CONCLUSION
A wide range of hybrid techniques have been developed for the treatment of gastrointestinal and biliary diseases.These techniques expand the indications of therapeutic endoscopy, make it easier and safer to perform difficult procedures and decrease the agony of patients.Some of the techniques are only reported in few cases and further detailed evaluation of feasibility and efficacy is needed.For those that have been confirmed safe and effective, how to choose between hybrid techniques and conventional methods could be difficult.Further prospective investigations should be conducted to determine the best treatment options.
 World Journal of Meta-Analysis2020年3期
World Journal of Meta-Analysis2020年3期
- World Journal of Meta-Analysis的其它文章
- Prevalence of anxiety among gestational diabetes mellitus patients: A systematic review and meta-analysis
- Hydatidosis and the duodenum: A systematic review of the literature
- Exclusive cigar smoking in the United States and smoking-related diseases: A systematic review
- Role of non-coding RNAs in pathogenesis of gastrointestinal stromal tumors
- Thrombopoietin-receptor agonists in perioperative treatment of patients with chronic liver disease
- Immunotherapy in hepatocellular carcinoma: Combination strategies