
Assessment methods and services for older people with cancer in the United Kingdom
2020-06-19 06:36:00TaniaKalsiDanielleHarari
Tania Kalsi, Danielle Harari
Abstract
Key words: Geriatric assessment; Elderly; Older; Cancer; Support; Services
INTRODUCTION
With longer life expectancy, patients presenting to cancer services are often older and often have complex multi-morbidity[1]. Such patients have poorer outcomes[2-4]. Cancer services were not designed to manage these complex patients. Models of care focus on early cancer detection, diagnosis, investigation and treatment[5]. There has been less emphasis on coordination of cancer care in the context of comorbidities and wider psychosocial and functional needs.
The United Kingdom Independent Taskforce report “Achieving World-Class Cancer Outcomes:A strategy for England 2015-2020” acknowledged this gap in national care pathways, and called for improved assessment methods for older people in the United Kingdom and better collaborative working with geriatricians[6]. The existing literature supports better co-ordinated interdisciplinary support to deliver geriatric assessment, manage comorbidity burden with the goal of improving outcomes[7]. Yet, so far, little has changed to embed system-wide comprehensive assessments into routine clinical care for older people in most cancer services in the United Kingdom.
Some European countries such as France have made more progress with national level financial investment in a Geriatric Oncology programme[8]. In France, they developed a standardised approach to identify vulnerable older patients[9]. They use a brief assessment tool (called the G8) as an initial assessment process for all patients aged over 75+ years[10]. Those identified as vulnerable by this tool are referred to oncogeriatricians for a more in-depth assessment. This avoids the cost of unnecessary indepth assessment in “fit” older patients, whilst delivering a systematic approach to identifying those who are “l(fā)ess fit” and require more input[11]. They have demonstrated benefit of implementing such a national programme with better collaboration, better informed decision-making and provision of more comprehensive interventions to support older people undergoing cancer treatment.
The use of a brief assessment tools to case-find those requiring in-depth geriatric assessment (contrasting to clinical judgement/referral-based pathways) is the pathway of choice in most Geriatric Oncology services across the globe as well as in the literature. Although France uses the G8 as their tool of choice, there are a number of similar tools in the literature, largely showing similar feasibility as a method of identifying those who require further assessment and intervention[12-14]. The International Society of Geriatric Oncology reviewed these tools and came to the consensus that no tool was superior and services should use whatever tool is usable and feasible for them[15,16].
There is no current national Geriatric Oncology programme in the United Kingdom although pockets of good practice are emerging and some have been evaluated[17]. The extent of local change is not clearly understood and how much services have evolved is unknown. The cancer strategy calls for redesign of care pathways for frailer older people, but it is important to understand where the gaps lie in order to design solutions compatible with existing patient needs, workforce and resources. This nationwide survey aimed to identify current assessment methods used for older people in United Kingdom cancer services and to identify current access to relevant supporting services.
MATERIALS AND METHODS
A web-based survey (SurveyMonkey) was distributed between January to April 2016viaUnited Kingdom nationally recognised professional societies (Association of Cancer Physicians, Royal College of Radiologists, British Geriatrics Society, the Association for Cancer Surgery, United Kingdom Oncology Nursing Society,Association of Chartered Physiotherapists in Oncology and Palliative Care, British Oncology Pharmacist Association and British Gynaecological Cancer society). The survey targeted relevant health professionals working with older people with cancer in the United Kingdom. This included oncologists, cancer surgeons, geriatricians,nurses and allied health professionals. Participation in the survey was voluntary.
The survey (available in supplement 1) consisted of 3 sections:
(1) Work background of respondents (including specialty, profession,hospital/practice); (2) Current assessment methods used when reviewing older patients including: Which professionals were involved in assessment; assessment methods and tools applied; age cut-offs for assessment; communication of assessments; influence of assessment on cancer treatment decision-making; and (3)Current access to relevant supporting services for older people; Which assessment methods they would consider to use the future.
The tools were electronically linked to the British Geriatrics Society Oncology Specialist Interest Group website as an information resource of the assessment methods discussed. The purpose of this was to introduce cancer healthcare providers to the options they may wish to trial as part of their assessment pathways in the future.
Questions were asked using a mixture of yes/no/don’t know, five-point Likert scales and free text responses. Questionnaire validity was evaluated using a panel of experts (members of the United Kingdom Geriatric Oncology Expert Reference Group supported by Macmillan Cancer Support). This expert group included representatives from multiple relevant specialities (medical, clinical and acute oncology, geriatric medicine, surgery, general practitioners (GPs), health and social care researchers) and multiple professions (doctors, nurses, therapists, researchers) and older patient representatives. The panel reviewed the questionnaire for readibility, content and clarity of words. The content of the questionnaire was revised accordingly prior to dissemination. Ethical approval was obtained (IRAS no. 194929). Participant information was provided, including explanation that consent was implied through completion of the web-survey. Responses were analysed in frequencies and percentages. The denominator for percentages was the percentage of those who responded(i.e. excluding non-responders). Where different, the denominator has been described. Chi Square was used to compare the differences in responses between different groups. SPSS version 25 statistical software package (SPSS, Inc., Chicago, IL,United States) was used for data analysis.
RESULTS
640 health care professionals responded to the survey between January to April 2016.The backgrounds of respondents are summarised in Table 1, the largest represented group were oncologists.
Health professionals currently involved in assessment of older cancer patients
Table 2 summarises current multi-disciplinary involvement in patient care. Gaps in wider medical provision was demonstrated; only 14.1% often/always had geriatricians involved in the assessment of older people in cancer services, only 52.0%often/always involved GPs in the assessment. Most (89.4%) did routinely involve nurses but a significant minority rarely/never used social care or allied health professionals such as occupational therapy.
Current assessment methods used
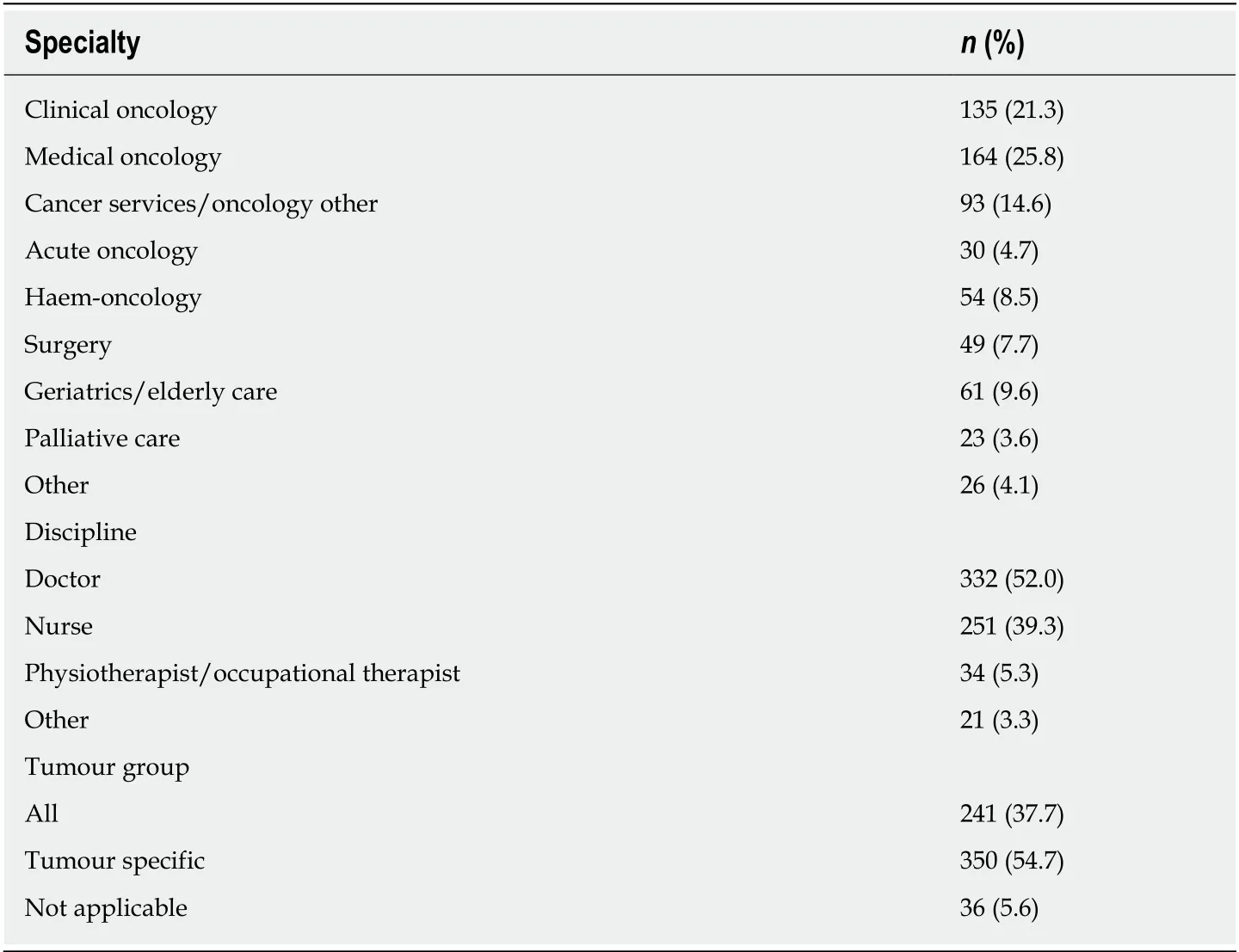
Table 1 Background of respondents
Clinical history-taking and performance status were favoured assessment methods regardless of profession (Table 3). Scoring tools were used far less and were favoured by nurses more than doctors,P< 0.0001.
About 30.5%-44.3% of respondents did not use structured methods for assessment or assessment tools to evaluate patient factors such as comorbidities, function, falls or social background. Nurses were significantly more likely to use a structured assessment approach than doctors [P< 0.001 for all domains except medications review (0.046)].
Table 4 describes which specific tools are being used and explores potential interest in using existing tools in the future. The denominator for percentages was the total sample. Brief assessment tools from the Geriatric Oncology literature (G8, VES13)were rarely used with greater use of traditional tools such as Mini Mental State Examination, Abbreviated Mental Test, Malnutrition Universal Screening Tool and Body Mass Index. The Holistic Needs Assessment (HNA) was utilised by 44.8%.Clinical assessment was used to identify more complex patients by oncologists(54.2%), by CNSs (51.4%) orviamulti-disciplinary team (MDT) meetings (44.4%), few used tools to case-find (20.9%). There was no clear preference for a specific tool.
Operationalising assessments and effect on decision-making
Most respondents reported not using an age cut-off for older people specific assessments in their clinical services (n= 300). Of those who did perform these assessments, 238 reported these assessments were communicated into the MDT, 208 in to clinic and 69 information/advice givenviaphone/email. 148 produced a structured letter/report from the assessment.
When performed, the majority reported these assessments always/mostly influenced cancer treatment decision-making (40.5%) or at least sometimes (34.1%).
Multi-disciplinary access
Table 5 summarises urgent access to supporting services. Most had urgent access to palliative care (78.5%) but only a minority had urgent access available to other key professionals such as geriatricians, social workers, old age psychiatry or to specialist older people nurses.
Dedicated geriatric oncology services
14.8% of respondents reported having a dedicated Geriatric Oncology service. Where they existed and respondents were aware of funding streams, they were most commonly funded through medicine directorates (n= 20) or temporary charity funding (n= 20) rather than through cancer, surgery or CCGs (n= 3, 6 and 1respectively). 69.6% of respondents were interested in developing services with geriatricians, only 5.5% did not support this concept, the remaining respondents were unsure.
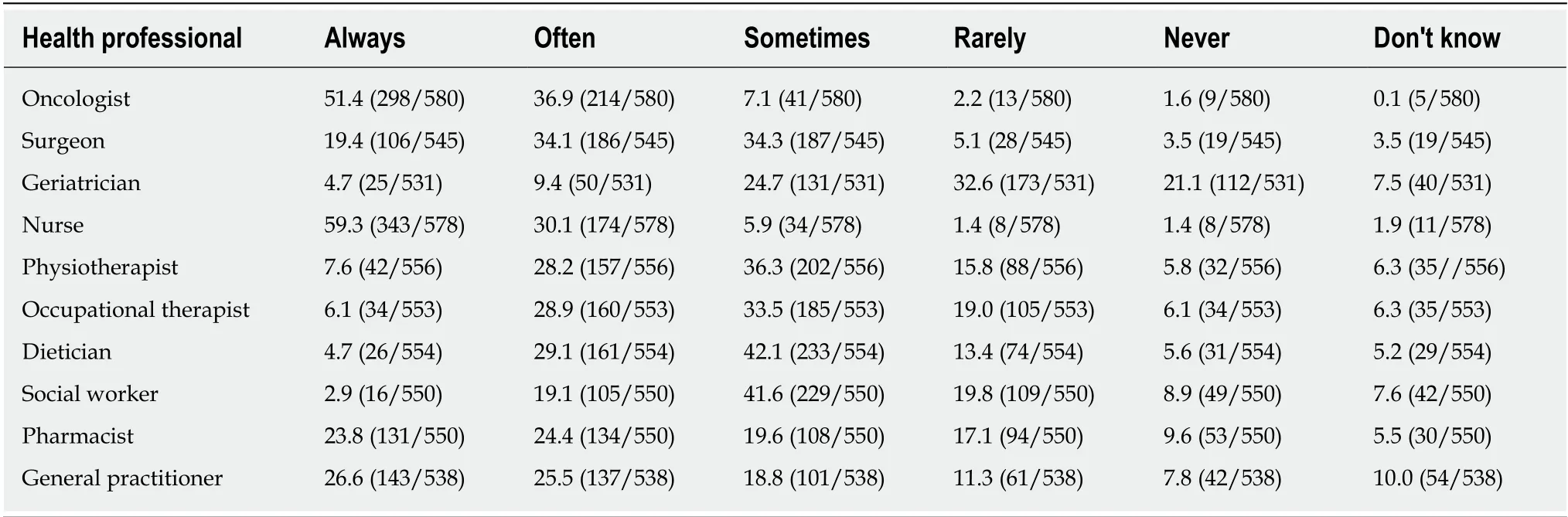
Table 2 Health professionals involved in the assessment of older people presenting to cancer service (%)
DISCUSSION
This United Kingdom wide survey demonstrates variability in assessment methods and access to supporting services for older people with cancer across the United Kingdom. Overall, health professionals tended to prefer performance status and traditional history-taking. Encouragingly, more than half of professionals reported they already use structured assessment for assessing issues such as comorbidity,cognition and nutrition giving a good base to standardise practice across cancer services. Nurses were more likely to use a structured approach to assessment than doctors. Studies exploring the reasons behind these differences would be helpful.Efforts seem best suited to developing a collaborative model with doctors, nurses and others in providing these assessments within a team-based structure[18]. Geriatric Oncology services should be evaluated for clinical effectiveness and feasibility to ensure the desired collaborative care is achieved[19].
Validated scoring tools (including the G8 and frailty scores) were not often used and there was little appetite to use them in the future. There has been significant interest in the research community to discover the holy grail of clinical score or frailty tool to aid cancer treatment decision-making[15]. This survey demonstrates that frontline clinicians do not support this concept and favour clinical information. Front-line clinicians already use performance status, and it is likely they acknowledge that the wider issues are too complex to be reduced down to an additional numerical indicator of fitness. The findings of this survey would suggest that any tool applied in the United Kingdom should be brief and focus around clinical history to have clinician buy-in.
Work is required to better link cancer services with other generalist doctors. Few had geriatricians involved in the assessment of older people in cancer services, and only half involved GPs. Evidence suggests that there is currently variation in delivery of follow up cancer care by GPs[20]. Standardised assessment pathways should ensure clarity of the responsibilities of primary, secondary and tertiery care before, during and after cancer treatment.
Most respondents had nurses involved in assessment supporting the positive impact of previous investment in specialist cancer nurses who to an extent provide wider questioning through the HNA[21]. However, most acknowledge that although the HNA provides significant value, it does not provide the means for delivering comprehensive geriatric assessment. Reassuringly, almost all respondents reported access to palliative care services, the majority having urgent access demonstrating feasibility of early collaborative working with other services.
Sharing of assessments was variable. Only a minority used these assessments to inform the MDT meeting yet reported that assessments often influenced cancer treatment decision-making. This may be due to MDT meeting culture where decisionmaking is often diagnostics focussed often excluding patient-centre factors from MDT decision-making[22]. Lack of comorbidity and clinical information in MDT meetings hinder their effectiveness[23]. Evidence suggests that when comorbidity is identified post-MDT, patients are more likely to receive conservative treatment[22]. Futurepathways delivering geriatric assessments need to consider how this information should feed into MDT decision-making or whether MDT meetings need radical change to allow for meaningful patient-centred discussion.
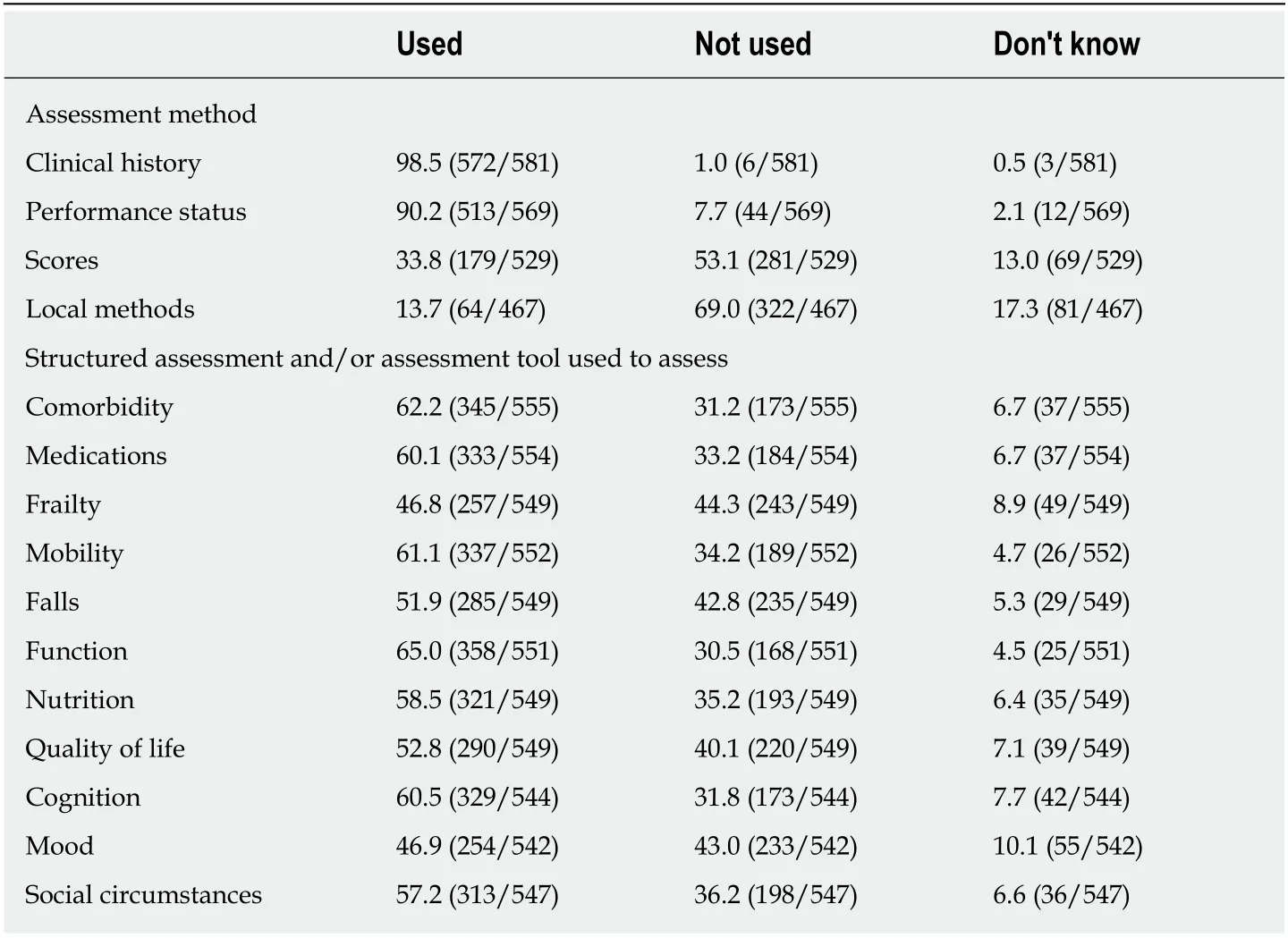
Table 3 Assessment methods currently used (%)
Access to key multidisciplinary team members was variable highlighting the lottery of use of supporting services across the United Kingdom. The survey was designed to scope clinical practice of individuals, including their access of these services rather than describe supporting service existence from a public health perspective. It is possible that more services exist than respondents were aware of and therefore did not access. Future work should focus on local service mapping to better link up existing services to avoid duplication given the workforce implications for developing new services[24]. This survey demonstrated that urgent geriatrician resource was sparse. Therefore, care models to deliver improved assessments must involve upskilling cancer services. Developing intervention algorithms for cancer services to manage co-existing needs identified by geriatric assessment should be tested.Feasibility of such algorithms using technology has been evaluated elsewhere[25]. This would reduce the need for geriatrician input for only the most complex.
Some geriatric oncology services were operational but surprisingly were funded more often through medicine directorate investments or charities. This contrasts to countries such as France where strong national investment has been applied[8]. Most were supportive of developing Geriatric Oncology services demonstrating a willingness for change. Similar previous surveys of Chiefs of Medical Oncology divisions in Italy were equally supportive of more time, attention and resource to older cancer patients[26].
This is the first survey to describe assessment methods used by front-line clinicians working in United Kingdom cancer services. This data is important in beginning to understand what clinicians in the United Kingdom will or won’t buy into. It was completed by professionals working in cancer services with sufficient representation from different groups (medical and clinical oncology, surgery, nursing and therapies)to gain a sense of views and clinical practice.
However, the survey has limitations. Participation in the survey was voluntary and it was distributed widely through professional societies, therefore we cannot evaluate response rates. It is likely that those more motivated to improving older people care were more likely to respond thus may not be representative of all front-line staff. The survey was designed to allow respondents to skip any question they wished to. This resulted in some questions having more missing data than others. We cannot make any conclusions as to why questions were skipped by some respondents. We would propose that some may relate to lack of awareness of local service availability. The questionnaire was only internally validated. It would benefit from external validation to exclude problems with the survey design. We only collected basic data on thebackground of respondents. Future work should consider collecting more baseline characteristics of the respondents to allow for multivariate analysis of factors associated with different assessment preferences.
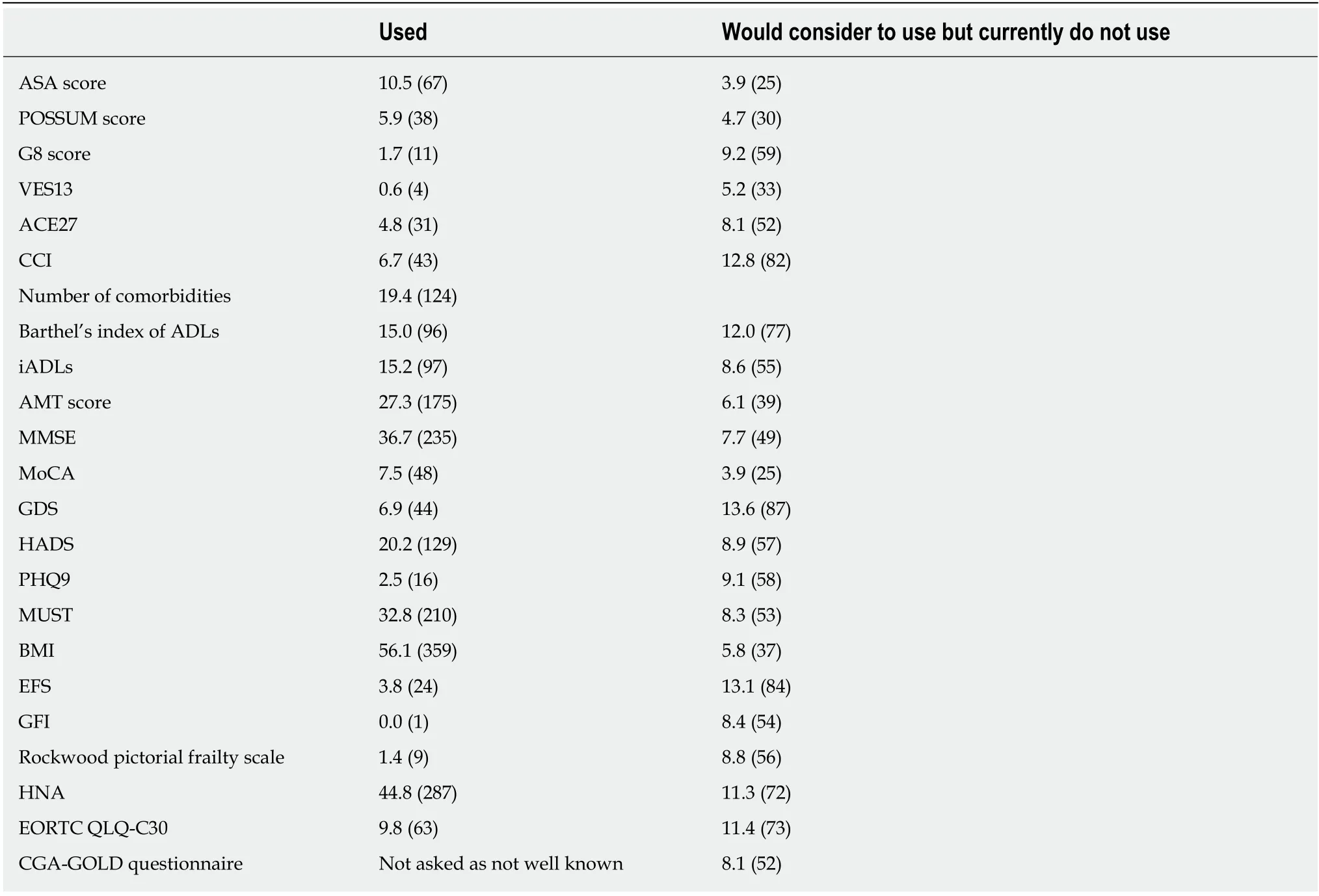
Table 4 Specific tools used or would consider to use, % (n)
There is variability in assessment methods for older people with cancer across the United Kingdom and variation in perceived access to supporting services. Clinical history taking was preferred to scoring systems. Fostering closer links with geriatricians appears supported.
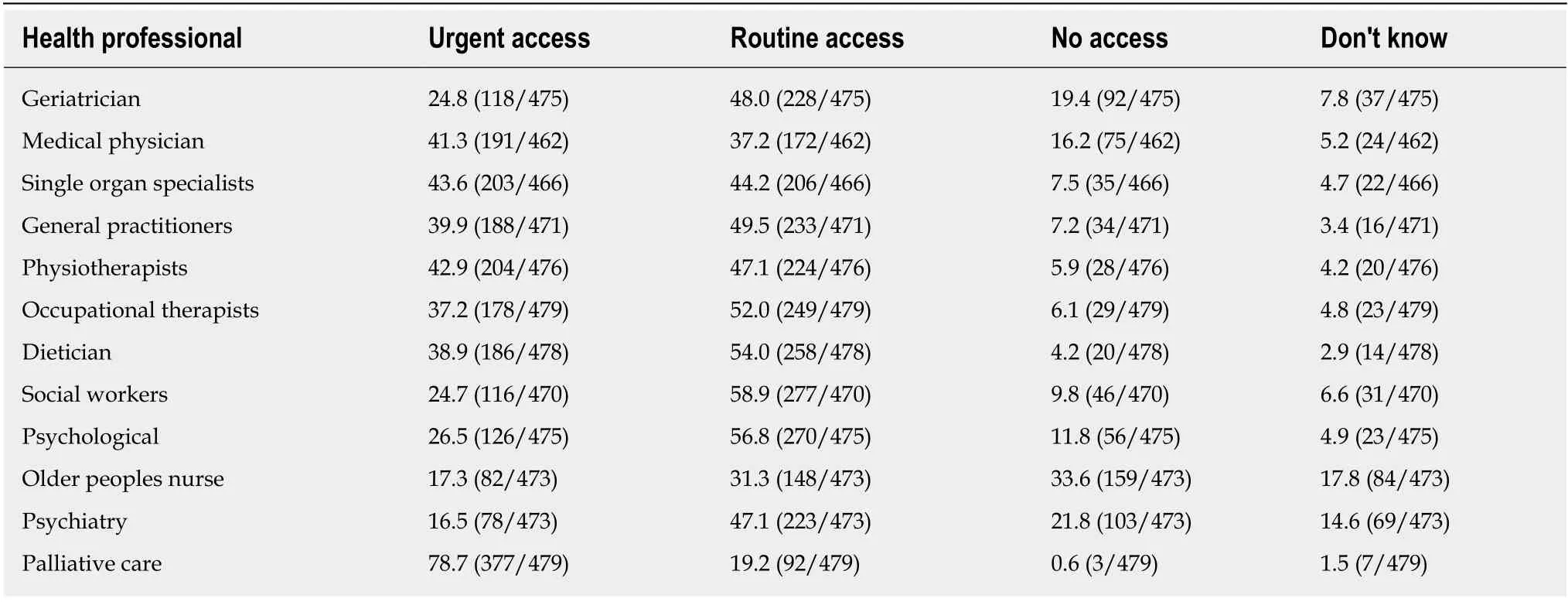
Table 5 Multi-disciplinary access (%)
ARTICLE HIGHLIGHTS
Research background
The United Kingdom Independent Taskforce report “Achieving World-Class Cancer Outcomes”calls for improved assessment methods for older people. Existing evidence and international bodies such as the American Society of Clinical Oncology and the International Society of Geriatric Oncology support this concept and recommend routine comprehensive geriatric assessment. However, assessment methods across a nation have yet to be described.
Research motivation
Older patients with cancer often have complex multi-morbidity and wider needs. These patients have poorer outcomes and are less likely to receive curative treatment. By better understanding current clinical assessment methods, future clinical care pathways can be designed around gaps in practice and be evaluated for effectiveness.
Research objectives
This nationwide survey aimed to identify current assessment methods and access to relevant supporting services for older people with cancer. By understanding current clinical practice and views, future research can focus towards interventions likely to be most acceptable and useful.
Research methods
A web-based survey was distributed between January to April 2016viaUnited Kingdom nationally recognised professional societies. The survey targeted relevant health professionals working with older people with cancer in the United Kingdom.
Research results
There was variability in assessment methods and access to supporting services for older people with cancer in the United Kingdom. Health professionals preferred performance status and traditional history-taking to scoring tools. Few had geriatricians involved in the assessment of older people and only half involved general practitioners. Access to key multidisciplinary team members was variable. This is the first study to describe assessment methods used by front-line clinicians in the United Kingdom. This data is important to informing design of future services to improve clinical assessment and support for older people with cancer.
Research conclusions
There was variability in assessment methods and access to supporting services. Clinical history taking was preferred to scoring systems. Future research evaluating delivery of comprehensive geriatric assessment should bear these results in mind. Future studies should consider moving away from scoring tools if the intention is for use in clinical practice. Developing care pathways to better link up existing supporting services would be a helpful initial step to improve access to key other professionals.
Research perspectives
A number of questions remain. How can comprehensive geriatric assessment be feasibly embedded within cancer care pathways across a nation? Is the workforce adequately trained to managed co-existing needs alongside cancer treatment? If not, would changes in education provide cancer services with the skills to better manage complex older patients? Or is collaborative working more effective? How can we test new assessment methods for feasibility and clinical effectiveness in cancer services?
 World Journal of Clinical Oncology2020年3期
World Journal of Clinical Oncology2020年3期
- World Journal of Clinical Oncology的其它文章
- Glycoconjugation: An approach to cancer therapeutics
- Efficacy, patterns of use and cost of Pertuzumab in the treatment of HER2+ metastatic breast cancer in Singapore: The National Cancer Centre Singapore experience
- What factors influence patient experience in orthopedic oncology office visits?
- Thrombocytopenia with multiple splenic lesions - histiocytic sarcoma of the spleen without splenomegaly: A case report
- Roles of cell fusion, hybridization and polyploid cell formation in cancer metastasis