
Care and social support from family and community in patients with pulmonary tuberculosis in Pakistan
2020-01-09 02:26:52ShahabSaqibMokbulMorshedAhmadSanaullahPanezai
Shahab E Saqib , Mokbul Morshed Ahmad, Sanaullah Panezai
ABSTRACT Objectives This study aimed to validate the Medical Outcome Study-Social Support Survey (MOS- SSS)instrument in Pakistan and to quantify the nature of care and social support currently extended to patients with pulmonary tuberculosis (TB) in Pakistan.Design This is a cross- sectional study design conducted within a period of 3 months from 1 November 2016 to 31 January 2017.Participants A total of 269 patients, registered at 11 TB centres and private clinics, were interviewed through an interviewer- administered questionnaire.Main outcome measures Cronbach's alpha was used to measure the internal consistency and reliability of the MOS- SSS survey instrument. Univariate and multivariable logistic regressions have been used to explore the association between care and social support, and socioeconomic factors.Result This study validated the use of the MOS- SSS among patients with TB in Pakistan. Findings of the study revealed significant differences among the socioeconomic groups of patients in each subscale of social support.Additionally, results of logistic regressions showed that patients who were older (adjusted OR=6.17, 95% CI 1.55 to 24.59, p≤0.01), male (adjusted OR=2.73, 95% CI 1.49 to 4.98, p≤0.01), widow (adjusted OR=0.17, 95% CI 0.04 to 0.80, p≤0.05), and had a larger household size (adjusted OR=5.69, 95% CI 1.32 to 24.65, p≤0.05), higher monthly income (adjusted OR=2.00, 95% CI 1.11 to 3.60, p≤0.05)and house ownership (adjusted OR=1.99, 95% CI 1.10 to 3.60, p≤0.05) were significant factors associated with the extent of care and social support that the participants received.Conclusion To cure TB, this study suggests a coordinated approach that includes not only clinical services to address this issue but also a strong social support system based on family and community necessary throughout the treatment process.
Key points
INTRODUCTION
Tuberculosis (TB) is considered a major issue of public health with an estimated 10.4 million new TB cases worldwide.1Among these cases, 5.9 million cases are reported to be among men, 3.5 million among women, 1.0 million among chil—dren and 2.1 million in individuals living with HIV, accounting for all new TB cases.1Besides, along with HIV/AIDS, TB is a major cause of mortality worldwide and places the heaviest burden on the poorest and most vulnerable population of the society.2In South Asia, Pakistan has the highest inci—dence rate (276/100 000) between 2006 and 2014.3Pakistan ranks fifth among the high burden countries and accounts for about 61% of the TB burden in the East Mediter—ranean region. Each year, approximately 0.42 million new cases of TB emerge, among which half of the cases are sputum smear positive. Pakistan is also estimated to have the fourth highest prevalence of multidrug—resistant TB globally.4
This slow rate of decline in TB shows that a biomedical approach alone will not be sufficient for ending the TB epidemic and achieving its elimination targets. There is an increasing consensus that social deter—minants of TB play a vital role in fighting against this disease.5Despite well— established treatment regimens, TB remains a burden to public health; it affects both poor and marginalised populations who may not have access to social support, including migrants and the homeless.6If patients are carefully treated and observed by family and the surrounding community, this may result in increased rates of compliance to the treat—ment and enhanced psychological well—being of the patient.7Conversely, in cases where compliance to TB therapy does not occur as with many cases today, this can lead to drug resistance, prolonged infection and death.8For the empirical management of TB, a study revealed that the major drivers of drug— resistant TB are inappropriate drug regimens, insufficient attention to TB, and inade—quate care and social support for patients in facilitating full completion of the administered treatment.9
As a condition, TB has been linked to several negative social outcomes for patients. For instance, due to the contagious nature of TB, people avoid being in close proximity to individuals infected with TB and think of themselves to be infected. Additionally, during the initial stages of active TB, those under medical care are required to remain physically isolated for 2 weeks or longer, receiving treatment to ensure that they are no longer contagious.10However, whether individuals are contagious or not, the stigma originally caused by this ill effect still remains. Within the community,individuals do not forget when someone close carries a life— threatening disease. Patients with TB are often said to be silently isolated by the community, and contact is observed to be avoided with patients with TB. For instance, people are refusing to drink tea offered by patients in social gatherings and not greeting patients physically when they meet.11The factors of isolation and other social consequences are described as signifi—cant in delaying the diagnosis in TB, especially among patients who are female.11For instance, in Thailand,65% of patients are found to be highly stigmatised by TB.12Therefore, due to these different consequences,TB has multidimensional impacts in both the individual and domestic spheres.
Research shows that social integration and social support are beneficial for good health.13Patients with TB have several medical and non— medical needs that should be fulfilled to cure this disease. If the patients are not carefully treated and observed by family and community, it may lead to non— compliance of treat—ment. Non— compliance to TB therapy can lead to drug resistance, prolonged infectiousness and death.8A meta— analysis study found that social support and social relationship influence risk of mortality.14Furthermore,it is also reported that stronger social relationships increase the likelihood of survival by 50% as compared with those who had no social relationships. Odds ratios were 1.9 for social integration, 1.5 for social networks,1.4 for perceived social support and 1.2 for received social support.14In Pakistan, a study is conducted on the socioeconomic consequences of TB.15Another study has been carried out on the need for a holistic approach to address all aspects of TB.16While acknowledging the importance of combining non— medical care with medical treatment, previous studies have assessed social support either by quantifying social relationships17—19or by other qualitative aspects.2021Limited studies have explicitly assessed the care and social support provided to patients with TB within the context of Pakistan, and no previous studies, in spite of their contributions, have explicitly assessed the social support received by patients with TB. Therefore, this study attempts primarily to validate the Medical Outcome Study—Social Support Survey (MOS— SSS) instrument in Pakistan. Second, this is our first attempt to quantify the nature of care and social support currently extended to patients with TB in Khyber Pakhtunkhwa, Pakistan.
METHODOLOGY
Study design
This is a cross— sectional quantitative study that is designed to test the reliability of MOS— SSS in Pakistan and explores the relationship with other socioeconomic and demo—graphic factors.
Study duration
The study was conducted within a period of 3 months from 1 November 2016 to 31 January 2017.
Study area
The study was conducted in District Mardan, Khyber Pakhtunkhwa Province of Pakistan. Mardan is the second largest city of the province and 19th in Pakistan.22This district is administratively divided into three subdistricts:Mardan, Takht Bhai and Katlang. The total population of the district is 1.46 million, of which 0.75 million are male and 0.71 million are female.23We purposively selected Khyber Pakhtunkhwa due to its high prevalence of TB cases, where approximately 58 449 of new cases of TB were reported in 2014.24In response to the high prev—alence, the provincial government has considered this a serious issue and passed an act in 2016 known as ‘the KP TB Notification Bill, 2016'. This act stipulated TB as a disease to be notified by all involved stakeholders,including medical practitioners, private and government clinics and community leaders.25
Study population and sampling
A multistage sampling was adopted to select the loca—tion of the study and the participants. A total of 5624 new patients with TB were registered at 11 TB centres and private clinics in the district in 2016.26We excluded the first quarter and second quarter registered patients,extrapulmonary cases, children and the significantly elderly within the target population due to their inability to participate in the interviews. Interviews were conducted in clinics. We have used the formula of a previous study and a sample size of 280 was calculated.27The total sample size was proportionally allocated among male and female participants, where male patients were 132 and female patients were 148. Lastly, those patients who were under treatment for at least 1 month in the last two quarters of year 2016 were randomly selected. However, in the third month of data collection, due to sociocultural constraints and incomplete questionnaire, the total sample size declined to 269 and consisted of 130 male and 139 female respondents.
Inclusion and exclusion criteria
This study employed both TB smear— positive and smear—negative patients under treatment for at least the previous 4 weeks, and at the time of the interview, they had at least two visits to the TB centre. We excluded the extrapulmonary patients from the study popula—tion. The patients below age 15 and above 60 were also excluded from the sample population because the chil—dren and the very old age patients could not answer the questions.
Study instrument
The MOS— SSS is a 19— item scale survey that contains subscales that include the domains of emotional/infor—mational, tangible, affectionate, positive social interac—tion, additional support and one additional item.1928The MOS— SSS is one of the most widely used instru—ments and is validated in different cultures, languages and contexts.29—32Data were collected on a Likert scale and were transformed from 0 to 100 for each subscale,where the higher values imply higher levels of care and social support. We obtained a score for each subscale and calculated the mean scores for each item in the subscale. The questionnaire was translated into Pushto language by following the WHO guidelines.33Cron—bach's alpha was used to measure the internal consis—tency and reliability. The questionnaire also contained demographic and socioeconomic information of the patients, such as age, sex, marital status, location of the house, income and main occupation.
Statistical analysis
Statistical tests such as t— test and analysis of variance were used to see the differences in subscale items along with socioeconomic groups. This study is further extended to explore the relationship between social support and other socioeconomic characteristics of the patients. Therefore, we used univariate logistic and multivariable logistic regressions. Furthermore, the social support index was converted into a dichotomous variable, taking the mean value as a cut point following other relevant studies.34—37
RESULTS
Demographic information of the participants
Patients were mostly young (56.13% were of ages ranging from 15 to 30 years). Among the total partic—ipants, 51.67% were female. Married patients were 60.2%, and 54.65% had 5—10 household members.Majority of them were illiterate (51.28%). In addi—tion, most of the patients (62.45%) were living in rural areas (table 1). Most of the patients were from the low—income class: 54.65% made <US$250 per month as household income. Besides, 34.20% and 28.63% were wage labourers and had agriculture as the main source of the family's income, respectively.
Summary of social support items
In all the eight items of subscales, most of the respondents had an emotional/information support score of 3.5. The mean score of all items was 3.42 (table 2). ‘To give you advice' and ‘to prepare your meals' had the highest score(3.55). In contrast, ‘get together for relaxation' and ‘help you get your mind off things' showed the lowest score(3.14).
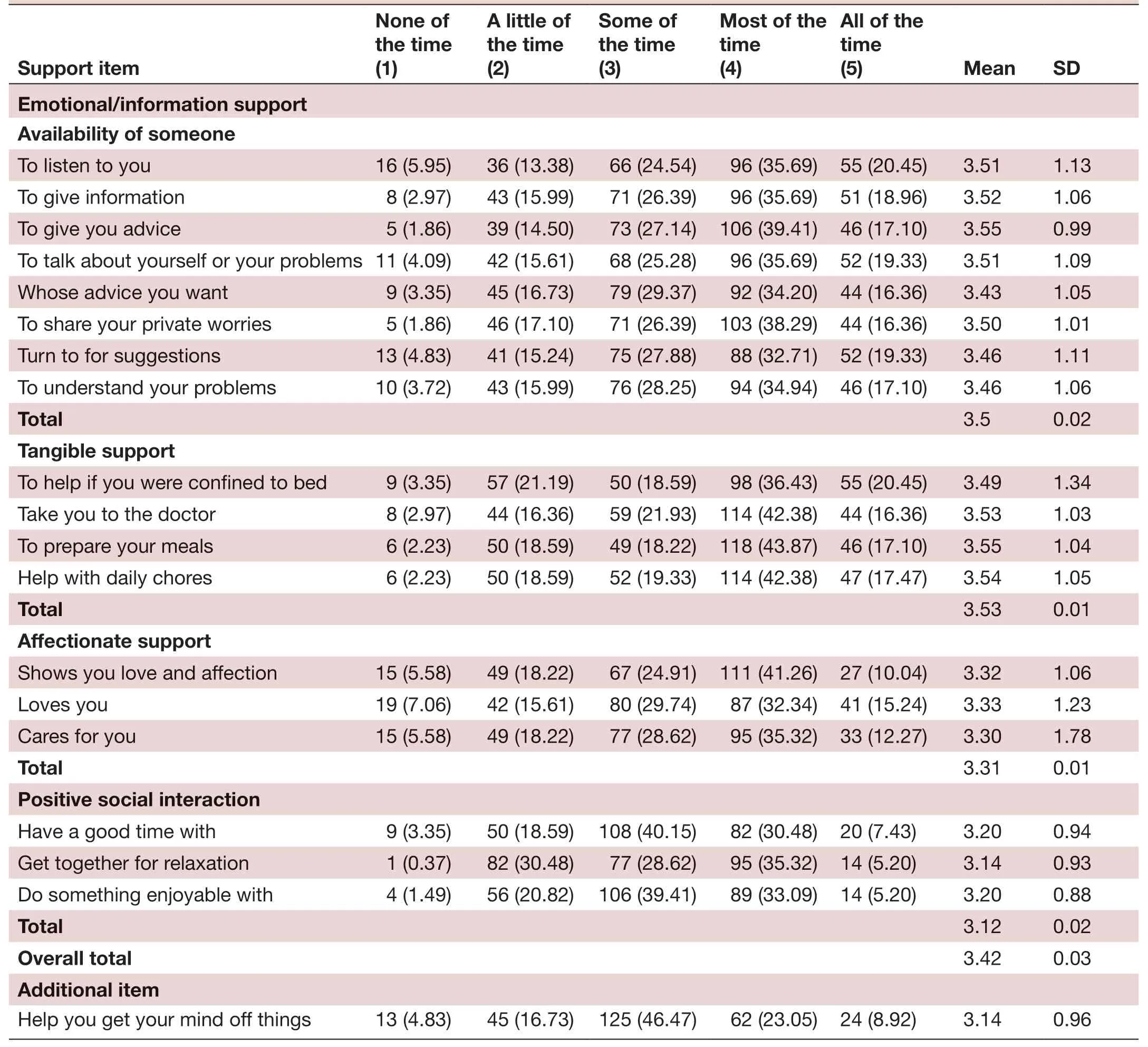
TabIe 2 Frequency distribution of social support measuring items
Descriptive statistics of subscale measuring items
The mean scores of the subscales are from 53.62(minimum) to 63.22 (maximum). Cronbach's alpha values ranged from 0.79 to 0.95. The overall average value of social support was 60.14 and was taken as a cut point to make a dichotomous dependent variable(table 3).
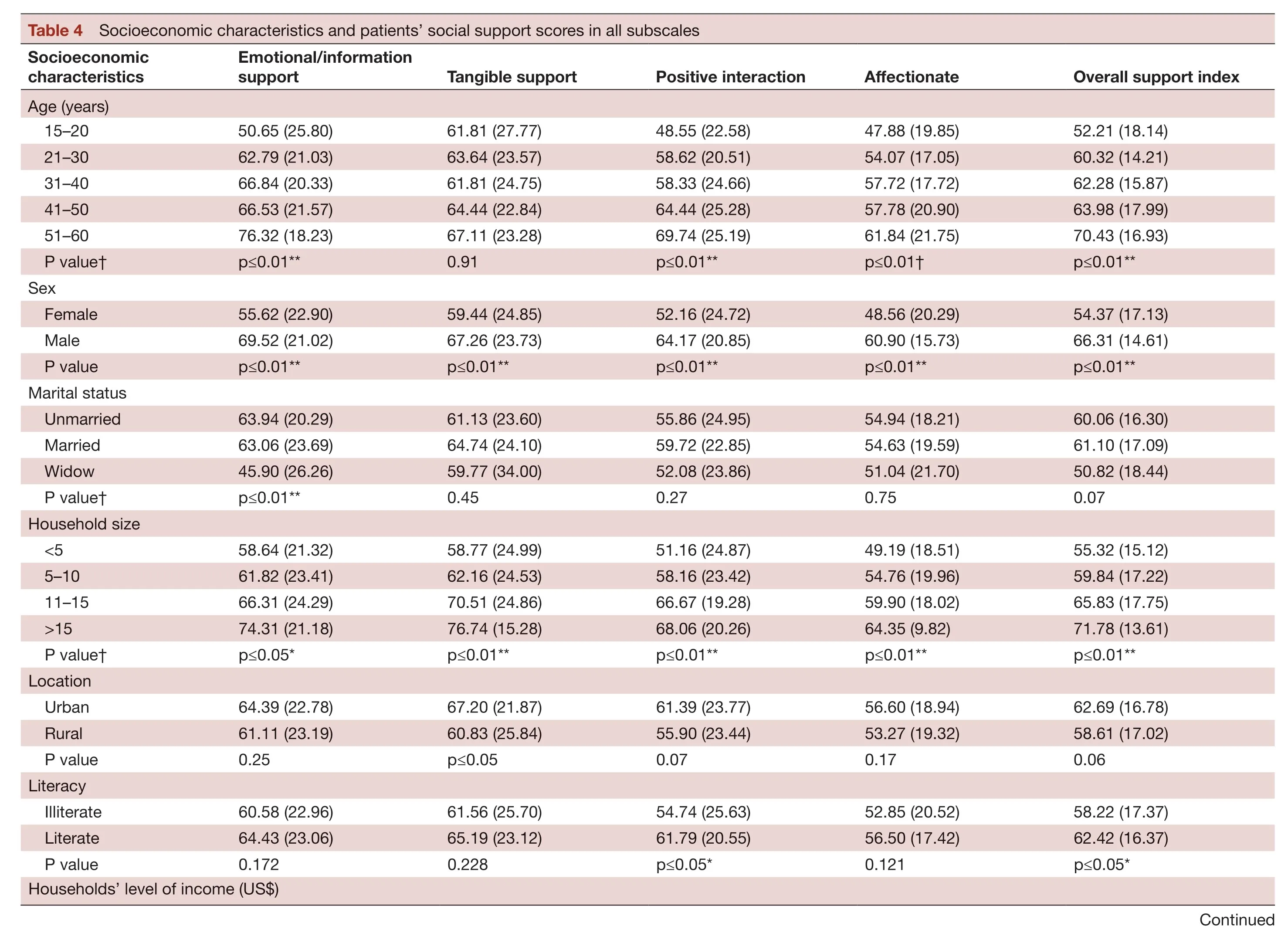
Comparison among patients’ social support scores in different subscales
As shown in table 4, there is a significant difference(p≤0.01) in almost all subscales of social support with all age groups except for tangible support. The results for overall support index was higher (66.31) in men than in the women (54.37), and there is a significant differ—ence (p≤0.01) between men and women in all subscales of social support. Unmarried patients received better emotional/information support than other patients who were married and widows (p≤0.01). Patients with a larger household's size or owned the house receive better social support in all aspects (all p values were ≤0.05). Patients who were living in urban areas received better tangible support (p≤0.05), and literate patients had better posi—tive interaction (p≤0.05). There was no significant differ—ence in all social support scales among the patients' main households' occupation groups.
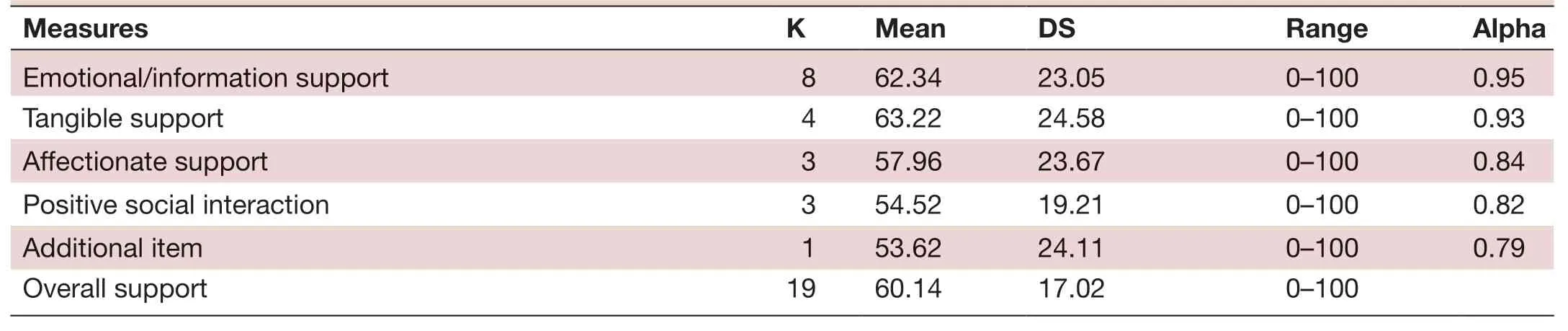
TabIe 3 Mean scores of the subscales
Results of the regression model
In regression analysis, the p value of the Hosmer and Leme—show test was 0.487, revealing good model fit (table 5).Factors such as the age of the patients, sex, marital status,household size, monthly income and house ownership were identified as significant factors associated with the social support received by the patients. There was no significant difference in main households' occupation.Therefore, we have excluded this variable in the regres—sion model. Patients in the age group 51—60 years were more likely to receive social support than the adolescent group between 15 and 20 years old (adjusted OR=6.17,95% CI 1.55 to 24.59). Men were more likely to receive social support than women (adjusted OR=2.73, 95% CI 1.49 to 4.98). Social support received by widows was lower than unmarried participants (adjusted OR=0.17, 95%CI 0.04 to 0.80). Patients who had >15 family members received a higher level of social support than the lowest category of the household size (adjusted OR=5.69, 95%CI 1.32 to 24.65). Patients with >US$750 monthly income were more likely to acquire social support than the lowest income group (adjusted OR=2.0, 95% CI 1.11 to 3.60).Patients who owned their houses were also more likely to get support than non— owners (adjusted OR=1.99, 95% CI 1.10 to 3.60).
DISCUSSION
TB targets most often the utmost vulnerable in any popu—lation such as the poor, malnourished and homeless who have no access to social support.6Therefore, the impor—tance of the care and social support to patients with TB from family and community can never be neglected during treatment. The findings of this study revealed that MOS— SSS is a valid instrument used for measuring the levels of social support provided to patients with TB in Pakistan by substantiating high reliability in all the subscale measuring items.19Patients with pulmonary TB in our study received limited social support. However, it was still higher than another study conducted in China(60.14 vs 34.56).38
The score of tangible support indicate that respon—dents received a good level of support from their families,friends and the surrounding community. However, the results on affectionate support and positive social interac—tion showed that in these subscales, the patients received limited social support.
The findings of the current study revealed that older patients received a higher care and social support score than young patients. These findings are different from the study in China, which demonstrated that young patients received lower social support (27.75) than elderly patients(31.60), and the population between 40 and 59 years old showed the highest score (33.60).38Young patients usually have more energy and financial power. There—fore, they reported less social support from families and community. The elderly were perceived to require more attention from family, friends and the community. There—fore, they reported higher social support. Besides, in the cultural and religious contexts of Pakistan, supporting the sick and the elderly is believed to be rewarded later by God: ‘Helping the one who is sick and serving him is an act of charity'. The Prophet (blessings and peace of Allah be on him) said, ‘Helping a man onto his mount or lifting up his luggage onto, it is a charity' (narrated by a Muslim, 1009). The findings of the study are consistent with a study conducted among Indians in America. They revealed that the respect for elders is an important tradi—tional value that may translate into higher social support in American Indians.39
Additionally, the present study revealed that male patients received higher levels of social support than female patients. As Pakistani society is patriarchal, men are perceived as the primary authority figures in the home, and men hold a superior position in relation to women in both the financial and social spheres.40Male and female patients with TB in Pakistan face many social and economic problems, but female patients suffered more than men.15A study reported that female patients with TB had less social support from their families.16This result is in contrast with the findings of a study from China, which revealed no difference between men and women receiving the social support.38

In all subscales, marital status is an important determi—nant of social support. Widows showed a negative associa—tion with social support, which implies that widows receive less social support than their unmarried and married counterparts. This phenomenon also substantiated that the marriage is an important source of social support.Married patients had higher social support.3941Addition—ally, the factor of household size among the patients was a significant determinant of social support. Our finding implied that in a large— sized household, the patient would receive more social support from the family. The previ—ously mentioned characteristics are both demonstrated in the research conducted in China.38
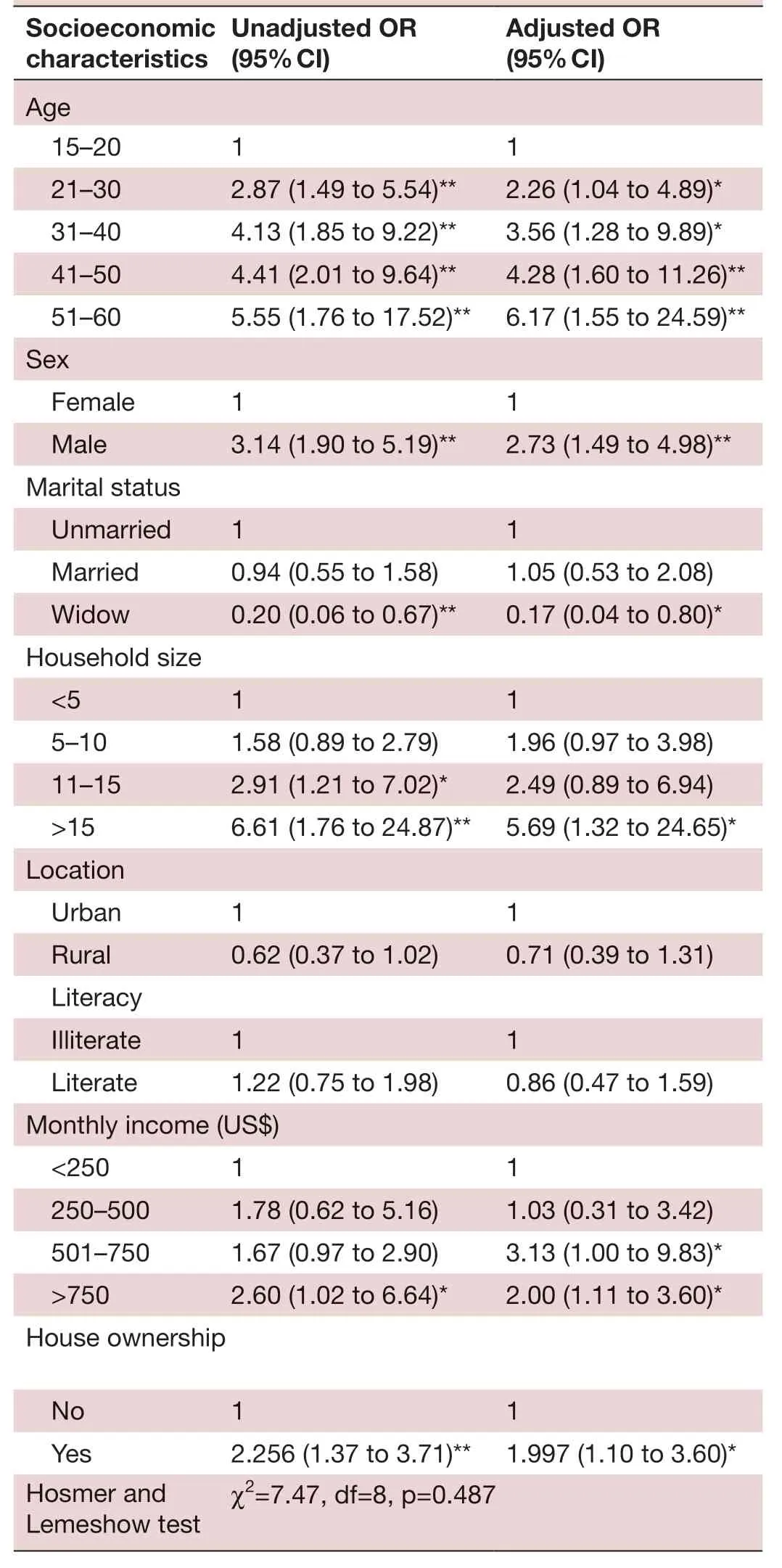
TabIe 5 Results of logistic regression
TB is more prevalent among the individuals with a lower socioeconomic status.6This implies that economic status is also one of the factors that plays a role in perceived social support of patients with TB. The find—ings of the current study showed that patients from groups with higher income levels received more social support. Mardan is a central district and people from the northern part of the province usually migrate and live in kacha (local term used for houses that are made from mud) houses or in slums that result in very poor living conditions. Patients from these households usually have low social support. Furthermore, in line with the view that the factor of homelessness is significant, we have included a proxy determinant that is the factor of home owner—ship. Therefore, the findings of the study showed that the factor of home ownership may be positively associated with care and social support from family and community.
Strengths and limitations of the study
MOS— SSS 19— item scale is an instrument to measure social support and provides its usefulness for future studies in this region of Pakistan. This is a first attempt to measure the social support extended to patients with TB in Paki—stan. The findings of the study capture the perceived social support among the population of patients with TB;however, these are not the representatives of the national—level population. Moreover, the selected participants of the study were under treatment for the last 4 weeks, and there might be a difference in the social support at the start and at the end of the treatment. Therefore, future research will explore that how the social support level may impact the adherence of patients to TB treatment.
CONCLUSION
The previous findings show that it is paramount to address the treatment of TB within the context of the care and social support provided to patients, in addition to standard medical procedure. This study indicated that patients with pulmonary TB experienced an overall low level of care and social support from their families, friends and communities. Considering this issue, patients of TB should be considered as an integral part of the popula—tion who need to receive both clinical and social care. In addition, the findings of this study imply the need for a coordinated and integrated approach including not only clinical services but also encouragement of strong family and community support throughout the treatment. Indi—viduals such as the poor, widows, women and marginal—ised patients should be extended more social support.Additionally, effective counselling and knowledge dissem—ination about TB ought to be present in families affected by TB at micro level, as well as society at the macro level.
Acknowledgements We extend our sincere thanks to the two anonymous reviewers and editor of this journal for their invaluable comments and suggestions on the earlier drafts of the manuscript. We also thank the study participants for their participation in the study and Mr Howard Goldman for proofreading the manuscript.
Contributors SES designed and performed the data collection and the analysis of the results. MMA supervised all the work from the start to the end. SP wrote the manuscript with inputs from other two authors.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not- for- profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Ethics approval The study was approved by the research ethical review committee of the Asian Institute of Technology, Thailand, under reference number RERC-2017/001. In addition, the data were collected only after receiving written consent from the respondents. Authors followed all standard protocols needed to conduct this study.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.
Open access This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY- NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non- commercially,and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non- commercial. See: http:// creativecommons. org/ licenses/ by- nc/ 4. 0/.
ORCID iD Shahab E Saqib http:// orcid. org/ 0000- 0003- 0326- 5197
 Family Medicine and Community Health2019年4期
Family Medicine and Community Health2019年4期
- Family Medicine and Community Health的其它文章
- From potential to practice: how accelerating access to HPV tests and screen and treat programmes can help eliminate cervical cancer
- How French general practitioners adapt their care to patients with social difficulties?
- Factors for self- assessment score of interprofessional team collaboration in community hospitals in Japan
- Improving sexual and reproductive health knowledge and practice in Mozambican families with media campaign and volunteer family health champions
- Improving patient satisfaction through improved telephone triage in a primary care practice
- Exploring the influencing factors for non- utilisation of healthcare facilities during childbirth: a special mixedmethod study of Bangladesh and 13 other low- and middle- income countries based on Demographic and Health Survey data