
Exploring the influencing factors for non- utilisation of healthcare facilities during childbirth: a special mixedmethod study of Bangladesh and 13 other low- and middle- income countries based on Demographic and Health Survey data
2020-01-09 02:26:48TanjimSiddiqueeHenryRatulHalderMdAkhtarulIslam
Tanjim Siddiquee, Henry Ratul Halder , Md Akhtarul Islam
ABSTRACT Objective To identify the associated factors affecting the decision regarding institutional delivery for pregnant women in 14 low- and middle- income countries (LMICs).Design A special mixed- method design was used to combine cross- sectional studies for harmonising data from Bangladesh and 13 other countries to obtain extended viewpoints on non- utilisation of institutional healthcare facilities during childbirth.Setting Demographic and Health Survey (DHS) data for 14 LMICs were used for the study.Participants There are several kinds of datasets in the DHS. Among them ‘Individual Women's Records' was used as this study is based on all ever- married women.Results In the binary logistic and meta- analysis models for Bangladesh, ORs for birth order were 0.57 and 0.51 and for respondents' age were 1.50 and 1.07, respectively.In all 14 LMICs, the most significant factors for not using institutional facilities during childbirth were respondents'age (OR 0.903, 95% CI 0.790 to 1.032) and birth order (OR 0.371, 95% CI 0.327 to 0.421).Conclusion Birth order and respondents' age were the two most significant factors for non- utilisation of healthcare facilities during childbirth in 14 LMICs.
Key points
INTRODUCTION
Globally, maternal mortality and morbidity are an alarming public health issue. In 2015,despite advances in the medical and public health sector, approximately 830 women died worldwide every day due to pregnancy and childbirth— related complications.1Lack of access and utilisation of healthcare facili—ties at the time of delivery is one of the main reasons for the high maternal and neonatal mortality in low— and middle— income coun—tries (LMICs).2—5At the primary level, ante—natal care (ANC) helps detect complications in the early period of pregnancy by providing a comprehensive range of health promotion and preventive healthcare services.67WHO recommend that throughout the pregnancy period at least four ANC visits are neces—sary for the safe and sound health of both the mother and the newborn.8Without any professional aid, there will be a high likeli—hood of mortality for both the mother and the child during pregnancy compared with those who have availed themselves of insti—tutional healthcare services.9—11However, in LMICs, a striking number of women still lack the opportunity for childbirth under trained medical personnel at healthcare facilities,and 99% of maternal deaths occur in devel—oping countries.12—15
A meta— analysis was conducted on the impact of place of delivery on maternal and perinatal mortality in sub— Saharan Africa, which was based on a limited number of studies, with some of them being population— based cohort studies.16Another meta—analysis on LMICs depicted that neonatal mortality is significantly affected by institutional deliveries, despite drawbacks due to study diversity and variation in context,limitation in data extraction, and incorporation of all risk factors.17In Bangladesh, diarrhoea and birth order were found to be the most significant risk factors for neonatal and child mortality, with a drawback being that the survey interviewed surviving women, which could lead to an underestimation of mortality rates and deficiency in the case of infant— specific variables.18Several studies have also aimed to explore the determinants of institutional delivery among women in Bangladesh; however, the studies were based on previously published Bangladesh Demographic and Health Survey (BDHS) datasets.1920The trends and regional patterns of disparities on util—isation of healthcare services in Bangladesh have been investigated.21—23Furthermore, small— scale studies have also been conducted in rural settings and provided strong programme recommendations to raise awareness in remote areas such as Matlab and Sunamganj.2425Never—theless, the small sample size of these studies conducted in a specific area might have influenced the results and may not be similar to other rural parts of Bangladesh.
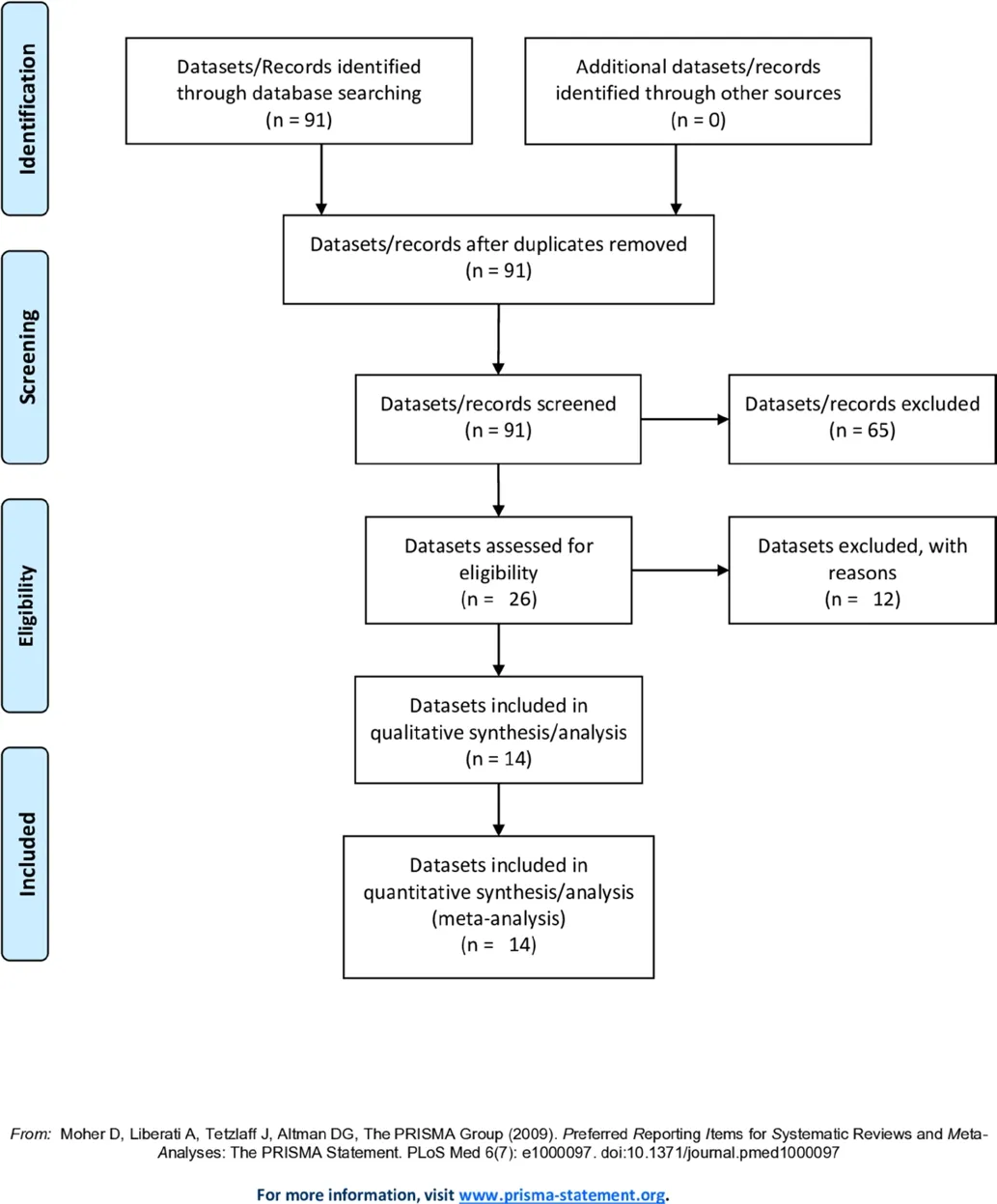
Figure 1 Flow diagram of the process of identifying and including datasets for the random- effects meta- analysis.
In this study, we attempted to determine the influ—encing factors for the non— utilisation of healthcare facil—ities during child delivery in Bangladesh and 13 other countries. We used a special mixed— method design to integrate data from Bangladesh and 13 other coun—tries to provide additional insight beyond what might be gained from a simple cross— sectional survey and meta— analysis.
METHODS
Design
This was a special convergent designed mixed— method study. We performed both binary logistic regression and meta— analysis for the cross— sectional study of Bangladesh.We then compared the results from Bangladesh with the meta— analysis of 13 other LMICs. Using this approach, we could extensively explore the factors affecting the deci—sion of pregnant women to not use healthcare facilities during childbirth. All data were based on the Demo—graphic and Health Survey (DHS).
Data source and data extraction
This cross— sectional study extracted relevant information for analysis from a nationwide representative secondary dataset, BDHS 2014. Information was collected from all seven administrative divisions of the country.26We also used the latest available datasets (accessed in January 2018) from MEASURE DHS (Monitoring and Evalua—tion to Assess and Use Result, Demographic and Health Survey) ( www. measuredhs. com) to conduct the meta—analysis. We obtained the latest available DHS data for Albania (2009), Azerbaijan (2006), Cameroon (2011),Egypt (2014), Haiti (2012), Jordan (2012), Kenya(2014), Lesotho (2014), Maldives (2009), Nepal (2011),Pakistan (2013), Peru (2012) and Tanzania (2016). One of the elementary goals of the DHS programme is to provide high— quality accessible data for analysis in the form of a questionnaire. For the analyst, this results in an information file containing incomplete or incon—sistent data, considerably complicating the analysis. In order to avoid these problems, the DHS programme has adopted a policy of editing and imputation in order to reflect population studies accurately. Additionally, the DHS data can be used immediately. The DHS database contains information from 91 countries (http:// dhspro—gram. com/ data/ available— datasets. cfm), but we only had authorised permission to access the data from 26 of them. We excluded 12 more countries due to excessive missing values and the insignificance of particular inde—pendent variables with the place of delivery in any of the selected countries. Finally, we selected Bangladesh and 13 other LMICs, which are homogeneous in nature as similar probability sampling for data collection was applied to them.
PRISMA flow diagram for eligibility criteria of datasets
In figure 1, which shows the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta— Analyses) flow diagram, we get a clear illustration of the eligibility criteria of the DHS datasets for the random— effects meta— analysis.
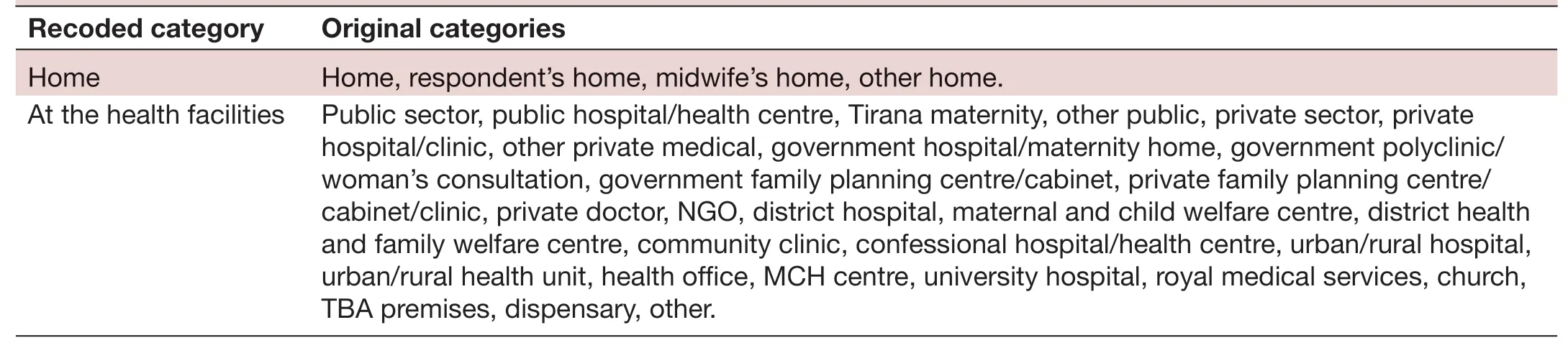
TabIe 1 Categorisation of the dependent variable from original categories to recoded categories
variables
The dependent variable for this study is theplace of delivery,and we categorised this variable into two main categories:‘Home’and‘Atthe Health Facilities’(table 1).
A set of socioeconomic and demographic factors for the determination of place of delivery were purposely selected as independent variables based on previous literature. A test of association was conducted to check whether or not they were significantly associated with the depen—dent variable. Subsequently, only significantly associated variables were selected for binary logistic regression and meta— analysis. Beginning with thetype of place of residence,the category remained the same as in the original data—sets. For the purpose of the analysis, we subcategorised the rest of the independent variables. Respondents' age was converted into nominal scale. The categories for this variable wereup to 20andabove 20. In the meta— analysis,those who had at least oneANC visitwere considered in the categoryyes, otherwiseno, whereas for binary logistic regression we subcategorised this asno visit,1-3 visitsandmore than 3 visits. In terms ofrespondents’ education level,we mergedno education,primaryandsecondaryintoup to secondary, andhigher educationconsisted ofabove secondary,in the meta— analysis. Forwealth index,poorest,poorerandmiddlefell underpoor, whereasricherandrichestformed therichcategory in the meta— analysis. On the other hand,for binary logistic regression,poorestandpoorerconstitutedpoor,middleconstitutedmiddle,and the rest of the other categories constitutedrich. Categories forbirth orderwerefirst orderwith one birth only,and the rest of birth orders formedother order. Finally, forbody mass index(BMI),worldwide commonly accepted BMI ranges were used:underweight (<18.5 kg/m2), normal weight (18.5—25 kg/m2), overweight (25—30 kg/m2) and obese (>30 kg/m2).27For convenience in our study, we keptnormal weightunder the categorynormal, and all other categories (underweight,overweight,obese) were classified asnot normal.
Statistical analysis
Data analysis was carried out using SPSS V.23 (SPSS Inc,Chicago, USA) and R V.3.5.2 statistical software (Bell Laboratories, New Jersey, USA). For BDHS data, binary logistic regression was applied to mark off the relationship between place of delivery for women in Bangladesh and other associated factors.28Meta— analysis was performed on the DHS data from Bangladesh and 13 other countries.Heterogeneity among datasets was assessed by computing values from I2and p values.29As the test statistics showed there was significant heterogeneity among datasets, the random— effects model in the meta— analysis was used to estimate the DerSimonian and Laird's pooled effect.303195% CI were shown in the forest plots for the most signif—icant factors of all 14 LMICs. In the forest plots, the size of each box indicates the weight of the study, while each crossed line refers to 95% CI. OR was used as a summary measure, and all results were weighted to eliminate undersampling and oversampling bias.
RESULTS
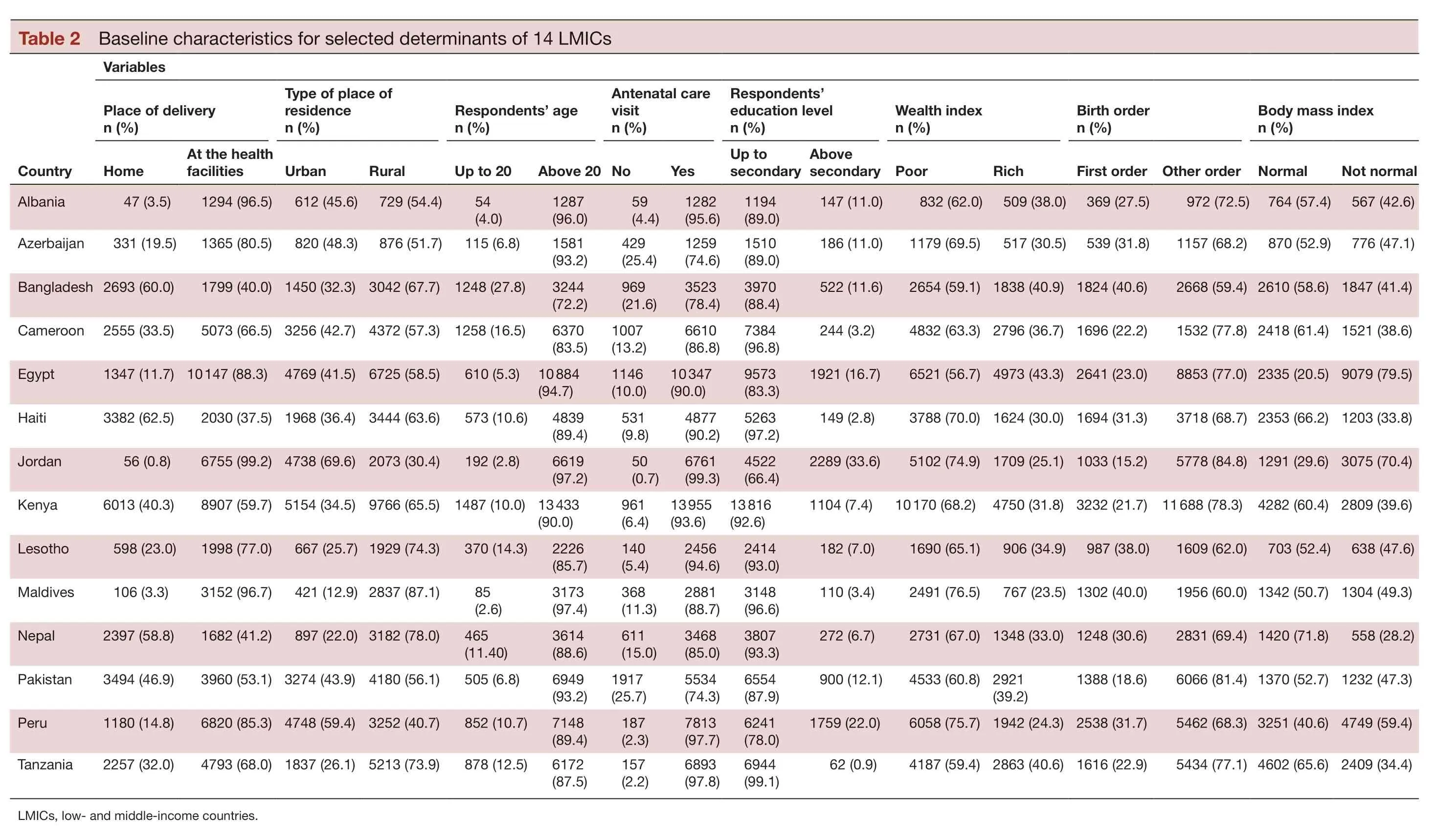
The baseline characteristics of the selected variables for 14 LMICs are shown in table 2. For place of delivery,respondents who have child delivery at home ranged from 0.8% (Jordan) to 62.5% (Haiti). Maldives has the highest percentage (87.1%) of rural residents. With regard to respondents' age, Bangladesh has the highest(27.8%) percentage for age up to 20 years. In terms of ANC visit, Jordan has the lowest (0.7%) and Pakistan has the highest (25.7%) percentage of ‘no' category. Further—more, Jordan exhibits the lowest (66.4%) and Tanzania exhibits the highest (99.1%) percentage of mothers with up to secondary education. It is also seen that Egypt has the lowest (56.7%) and Maldives has the highest (76.5%)percentage with regard to poor wealth index. Jordan and Bangladesh demonstrate the lowest (15.2%) and the highest (40.6%) percentage with regard to first— order child. Egypt has the lowest (20.5%) and Nepal has the highest (71.8%) percentage of normal BMI.
Table 3 illustrates the various socioeconomic and demo—graphic factors influencing the decision to choose the place of delivery for women in Bangladesh. The binary logistic regression model is statistically insignificant by the Hosmer and Lemeshow test (p=0.803), meaning that the model is a good fit. Also, the test of multicollinearity was conducted using the variance inflation factor (VIF).VIF concluded that most of the independent variables were moderately correlated (1<VIF<5) with each other,which can be neglected during regression analysis.
Determination of place of delivery is associated with the type of place of residence, with an adjusted OR of 2.617 (95% CI 0.528 to 0.721; p≤0.001) for the rural cate—gory. Similarly, respondents' age has a significant impact on place of delivery, with an adjusted OR of 1.479 (95%CI 1.217 to 1.799; p≤0.001) for category ‘a(chǎn)bove 20'. The categories ‘1—3 visits' and ‘more than 3 visits' with ORs of 3.448 (95% CI 2.729 to 4.355; p≤0.001) and 6.011 (95%CI 4.695 to 7.694; p≤0.001), respectively, show the asso—ciation between place of delivery and ANC visit during pregnancy. Secondary and higher education of respon—dents have a relationship with place of delivery, where the adjusted OR is 1.799 (95% CI 1.397 to 2.315; p≤0.001)and 3.946 (95% CI 2.838 to 5.488), respectively. Respon—dents from middle— class families exhibit a notable influ—ence on place of delivery, where the ORs is 1.613 (95%CI 1.326 to 1.963; p≤0.001) and 2.583 (95% CI 2.160 to 3.090; p≤0.001) for respondents from rich families. Birth order is likewise associated with place of delivery; when the birth order isother orderthe OR is 0.567 (95% CI 0.473 to 0.679; p≤0.001).
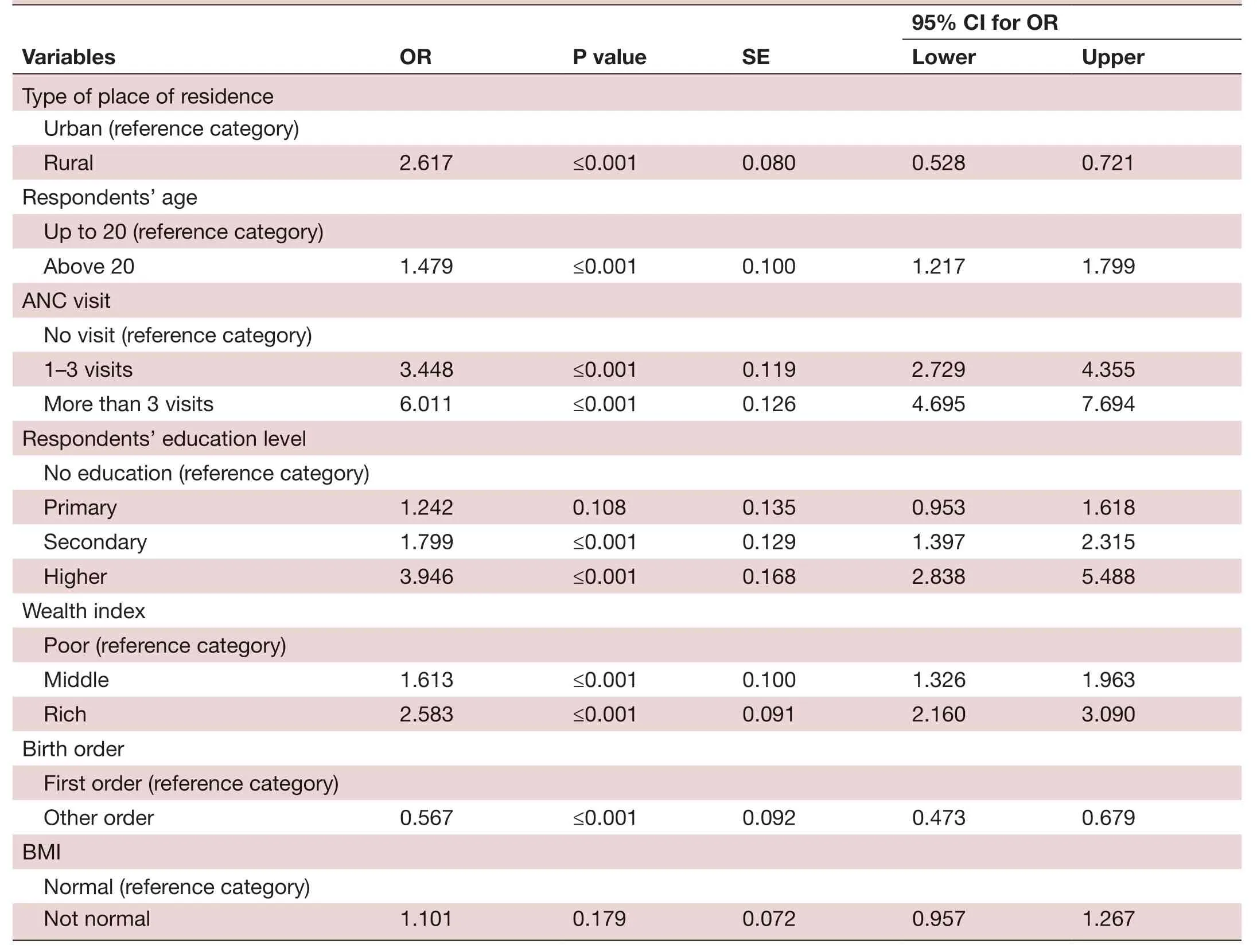
TabIe 3 Results of the BLR model affecting socioeconomic and demographic factors for non- utilisation of healthcare facilities during childbirth for women in Bangladesh
From tables 4 and 5, an estimate of the average treatment effect, which varies from study to study, can be obtained by the true treatment effect from the random— effects model.In this study, we have observed high heterogeneity and this is why the random— effects model was used. About 96.3% of the variation ( I2=96.3%) has been found for the type of place of residence. The overall OR is 4.020 (95% CI 3.217 to 5.024), meaning that urban residents have 4.020 times higher chance of using healthcare facilities as a place of delivery than rural residents. About 80.5% of the variation( I2=80.5%) has been found for respondents' age, and the overall OR is 0.903 (95% CI 0.790 to 1.032), which suggests that as age increases the chance of using a healthcare facility as the place of delivery decreases. For ANC visit, I2has been found to be 96% for the overall model. The overall OR is 6.177 (95% CI 4.489 to 8.501), which means respondents have 6.177 times higher chance of using healthcare facil—ities as the place of delivery for those who have received ANC compared with those who have not. About 84.2% of variation ( I2=84.2%) has been found for respondents'education level, and the overall OR is 11.161 (95% CI 7.910 to 15.748), which means that with an increment in education level, respondents have 11.161 times higher chance of using healthcare facilities during childbirth.For wealth index, I2has been found to be 93.3%, and the overall OR is 6.278 (95% CI 5.207 to 7.569), which reveals rich respondents have 6.278 times higher chance of using health facilities as a place of delivery compared with respon—dents who are poor. For birth order, I2has been found to be 86.8%, and the overall OR is 0.371 (95% CI 0.327 to 0.421).

TabIe 4 Random- effects model estimation of OR for Bangladesh and 13 other LMICs

TabIe 5 Random- effects model estimation (summary effect) for different variables in Bangladesh and 13 other LMICs
This suggests that respondents with more than one child have 0.371 times lower chance of using healthcare facili—ties. About 80.2% of the variationhas been found for BMI, and the overall OR is 1.512 (95% CI 1.364 to 1.676). This suggests that respondents with a BMI that is not normal have 1.512 times higher chance of using health—care facilities as a place of delivery.
Meta— analysis in the context of Bangladesh shown in table 5 portrayed that urban residents have 2.95 higher odds of using health facilities as the place of delivery than their rural counterparts. Likewise, respondents'age, ANC visit, respondents' education level, wealth index and BMI are positively associated with availing healthcare facilities during childbirth, with ORs of 1.07,5.26, 6.24, 4.62 and 1.14, respectively. Here, the refer—ence category for respondents' age is up to 20, yes for ANC visit, illiterate for respondents' education level,poor for wealth index, and normal for BMI. However,only birth order has a notable negative influence on the utilisation of healthcare facilities, with an OR of 0.51. All in all, birth order and respondents' age are the two most effective factors in the decision by respondents to avail themselves of healthcare facilities during childbirth for both the overall random— effects meta— analysis model and Bangladesh.
Figure 2 shows that in the Maldives respondents aged up to 20 are less likely to choose healthcare facilities as the place of delivery. In contrast, in Jordan the respondents show much more interest in choosing healthcare facilities.The summary estimate of this variable shows an OR of 0.90 and 95% CI of 0.79 to 1.03. Also, the overall estimate is statistically significant (p<0.01) at a 5% level of significance.
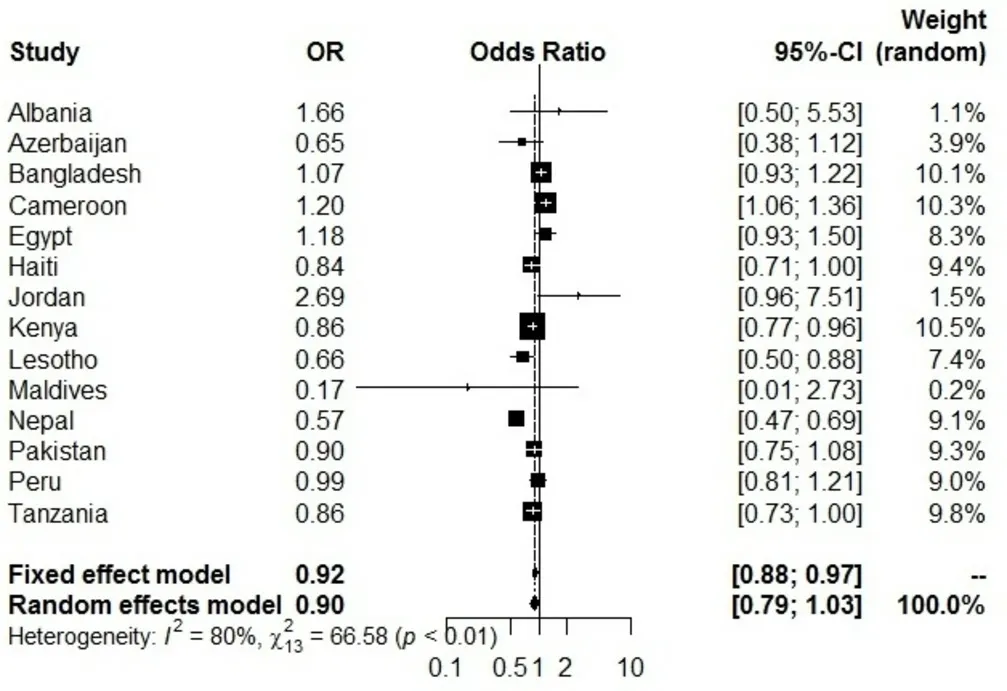
Figure 2 Forest plot for respondents’ age. The size of each box indicates the weight of the study, while each crossed line refers to 95% CI.
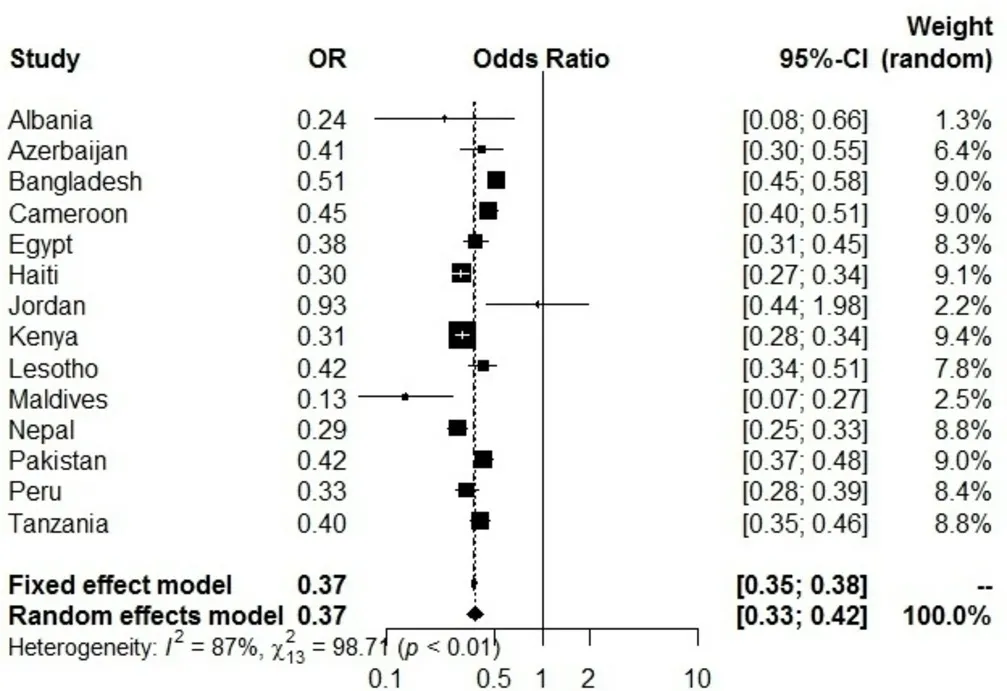
Figure 3 Forest plot for birth order. The size of each box indicates the weight of the study, while each crossed line refers to 95% CI.
Figure 3 show a forest plot for birth order and depicts a summary estimate OR of 0.37 with 95% CI of 0.33 to 0.42,meaning that the overall estimate is statistically significant(p<0.01) at a 5% level of significance. Birth order there—fore has a significant effect on non— utilisation of health—care facilities during childbirth.
DISCUSSION
Motherhood is a memorable moment in the life of women and is positively related to the supreme goals of happiness, completeness and family integration.32There—fore, the decision of women to avail themselves of health—care facilities during childbirth is very crucial and this is a definitive example.33
The key findings of the binary logistic regression model for Bangladesh depict that birth order and respondents'age are two significant factors for non— utilisation of health—care facilities during childbirth. As respondents get older and birth order increases, their preference to choose healthcare facilities as the place of delivery decreases.The ORs of Bangladesh in both binary logistic regres—sion and meta— analysis model for birth order are 0.57 and 0.51, respectively. The variation between these two values is negligible as they are close to each other. However, the overall OR of meta— analysis is 0.371 with an I2of 86.8%,which is much lower than both binary logistic regression and meta— analysis in Bangladesh. This means that multip—arous women from Bangladesh tend to avail themselves of healthcare facilities more when compared with the overall meta— analysis model. Altogether the improve—ment of this factor is a dying need, especially in Maldives,Nepal and Albania. Primiparous women usually have a higher risk of pregnancy complications than multiparous women.34These primiparous women have a higher prob—ability of accessing institutional delivery than multiparous women who have a preference for traditional birth atten—dants (TBAs).3536Homogeneous results have been seen in previous literature.37—41On the flip side, when multip—arous women had their first childbirth safely at home,they became less fearful about this and preferred to avoid facility delivery compared with primiparous women.1942
Furthermore, the OR of respondents' age in Bangla—desh for both models has a visible difference. The risk of mortality for both the mother and the child does not get any less as they grow older; the truth is the risk remains the same. The overall OR from meta— analysis for this factor is 0.903 with an I2of 80.5%, which suggests that respondents from Bangladesh aged above 20 are more likely to use healthcare facilities in comparison with the overall meta— analysis. Country— wise, respondents from Maldives aged above 20 have the lowest and Jordan the highest chance of choosing healthcare facilities for child—birth. Due to advancements in medicine and women's education in recent years, younger women are able to expand and update their knowledge regarding health—care facilities and put their faith in contemporary medi—cation rather than healthcare facilities.43—45
Also, respondents from rich families tend to have their chil—dren delivered at healthcare facilities because they have more social resources and can pick any facilities that offer health—care services. It has also been observed that 70% of childbirths occur at home for the lowest two wealth indexes.46The most common reason for not delivering in a facility is quoted by the head of the household as ‘not necessary', and this is influ—enced by the social and cultural beliefs at the household and community levels.47Research consistently showed that poor families could not bear the cost, and this is also an important constraint on service utilisation.34424348—50In the meta— analysis,Bangladesh has the second lowest OR to choose a health facility as the place of delivery than other selected countries.Due to the affordable cost and the benefit of payment negotia—tion, low— income families tend to undergo childbirth at home with the assistance of untrained TBAs.51By reducing out—of— pocket expenses for institutional delivery, this behaviour can be minimised especially for the poor.52Also, it requires time to change this practice, and maximum efforts should be made towards enhanced training of these birth attendants so that they can help during childbirth at home and make referrals to the nearest healthcare facility when needed.53Yet there are some reasons why a larger number of women still have birth at home rather than at a healthcare facility. Among them, sudden labour pain, distance from home to healthcare facility and poor availability of transport are the noteworthy ones mentioned by women who had childbirth at home.54—56
To reduce the high maternal mortality rate in LMICs,the master plan can include easily reachable and accurate care for pregnancy complications and beneficial postnatal care within the first 24 hours of delivery.5758Furthermore,the global health community has introduced two interven—tions to reduce maternal mortality. An emergency obstetric care service is the first intervention and is highly effective at reducing mortality from postpartum haemorrhage, infec—tion, pre— eclampsia, obstructed labour and a range of other causes.59The second is community— based interventions for TBAs, which will provide them with intensive training and a chance to build better and stronger relationships with referral networks.60The key strategy for Bangladesh is to promote the rate and benefits of institutional delivery to reduce the burden of maternal and child mortality, with the aim of attaining maternal and child health— related goals, as suggested by previous studies.2661—63
This study has some limitations and strengths. The first limitation is that we could only collect data from 14 of the 91 countries from the DHS database due to the require—ment for authorised permission. The second limitation is that the DHS data used in this study covered a wider location and time points, which added selection bias. The third limitation is that each variable was categorised into two categories, and then a 2×2 cross— tabulation table was performed to calculate the OR. Also, we were not able to include all the potential risk factors due to missing values or the insignificance of particular independent variables in any of these countries. This can also cause bias.
However, despite these limitations, the strength of our study is that we innovatively used a special mixed— method design: we combined cross— sectional data based on national surveys with the meta— analysis data of 14 LMICs.New knowledge and insights were generated through their integration. This is a breakthrough in mixed—method methodology. By using this innovation, we effec—tively expanded the external validity of cross— sectional surveys and created a new research approach.
CONCLUSION
Institutional delivery is doubtlessly a vital factor for the reduction of maternal mortality and morbidity. This study rigorously recognised the dominance in the increment of respondents' age and birth order. The attitude and beliefs of multiparous women and the misconceptions surrounding increased age need change. Also, free— of—cost health schemes for poor families need to be intro—duced to reduce both maternal and child mortality. If incentives regarding institutional delivery can be imple—mented, then the targeted maternal mortality ratio of the Sustainable Development Goals can be fulfilled by 2030.
Acknowledgements We would like to thank the MEASURE DHS for allowing us to use DHS datasets for analysis. We would also like to thank the reviewers and the editor for their valuable comments, guidance and suggestions, which helped us to improve the previous version of this paper.
Contributors MAI came up with the idea and concept and supervised the study.TS and HRRH were responsible for the methodology, formal analysis, interpretation,validation, investigation, data curation, draft preparation, review and editing.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not- for- profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Ethics approval The DHS survey was approved by the ICF International Institutional Review Board. The corresponding author has permission to use DHS data, which were accessible in the public domain in an unidentifiable form.Therefore, no additional approval was necessary.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.
Open access This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY- NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non- commercially,and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non- commercial. See: http:// creativecommons. org/ licenses/ by- nc/ 4. 0/.
ORCID iD Henry Ratul Halder http:// orcid. org/ 0000- 0002- 1362- 3077
 Family Medicine and Community Health2019年4期
Family Medicine and Community Health2019年4期
- Family Medicine and Community Health的其它文章
- From potential to practice: how accelerating access to HPV tests and screen and treat programmes can help eliminate cervical cancer
- Care and social support from family and community in patients with pulmonary tuberculosis in Pakistan
- How French general practitioners adapt their care to patients with social difficulties?
- Factors for self- assessment score of interprofessional team collaboration in community hospitals in Japan
- Improving sexual and reproductive health knowledge and practice in Mozambican families with media campaign and volunteer family health champions
- Improving patient satisfaction through improved telephone triage in a primary care practice