
Factors for self- assessment score of interprofessional team collaboration in community hospitals in Japan
2020-01-09 02:26:50JunjiHarutaSachikoOzoneRyoheiGoto
Junji Haruta, Sachiko Ozone, Ryohei Goto
ABSTRACT Objective Interprofessional collaboration is considered an important strategy in overcoming the complex issues associated with healthcare outcomes. A nationwide,community- based integrated care system developed for the care of older people in individual communities in Japan requires community hospitals to deliver integrated care to coordinate efforts for creating effective environments for health. This study aimed to explore the factors associated with the self- assessment score of interprofessional collaboration in community hospitals.Design Cross- sectional study using the Assessment of Interprofessional Team Collaboration Scale (AITCS).Setting This study was conducted in three small community hospitals in Japan.Participants All healthcare staff in the hospitals via research collaborators were asked to complete the anonymous self- administered questionnaire of the AITCS comprising questions related to individual factors (age, gender, profession), hospital to which they belonged, relationships with neighbouring facilities, job burden and job satisfaction from July to October 2018.The association between the questionnaire items as explanatory variables and AITCS score as an objective variable was determined using univariate followed by multiple regression analyses.Results The data from 325 of 630 participants were analysed, of whom 252 were female (77.5%) and 240 were nurses (73.8%). The mean of the total AITCS score was 117.6 (range 37-185), and the Visual Analogue Scale for relationships with neighbouring facilities, job satisfaction and job burden was 53.0 mm (0-100),46.1 mm (0-100) and 64.3 mm (0-100), respectively.In univariate analyses of the association with AITCS score, explanatory variables with a significance level of<0.05 were relationships with neighbouring facilities,job satisfaction and job burden. On multiple regression analysis, the total AITCS score was independently associated with age, profession (nurse/non- nurse),relationships with neighbouring facilities and job satisfaction.Conclusions Better self- assessment score of interprofessional collaboration is more strongly associated with younger age, a nursing profession, better relationships with neighbouring facilities and greater job satisfaction than with the hospital to which the participant belonged. These findings may help community hospitals enhance the integration of service delivery and benefit to the community through interprofessional collaboration.
Key points
INTRODUCTION
Interprofessional collaboration (IPC)is considered an essential strategy for improving the efficiency of healthcare systems and health outcomes. Policy makers,implementers and educators are aware of the need for cooperation among medical profes—sionals to improve health outcomes, health—care quality and medical safety.1In particular,given the increase in complex healthcare needs of individuals and populations in our rapidly changing society, policy makers in many countries have focused on advancing care delivery and enhancing collaboration in primary care.2—4Canada has implemented diverse policies, including primary care payment blended models that are mostly group— oriented. To restructure individual practices around interprofessional care, the integrated and interprofessional team model can provide resources in a blended capitation—based or salary— based model.5In the UK, the‘Integrated Care Pioneer' programme has provided multidisciplinary approaches to meeting the needs of the ageing population,delivering person— centred, coordinated and long— term support. The multidisciplinary care teams have provided better healthcare, and have in turn reduced the cost of local health—care provision.6Similarly, the USA formulated the Patient— Centered Medical Home model to transform the organisation and delivery of advanced primary care services.7The model coordinates care across the elements of the broader healthcare system and is expected to improve quality and decrease the cost of care.8
In Japan, the government has introduced a comprehensive and integrated nation—wide, community— based integrated care system to care for older people with chronic diseases or disabilities.9In particular, in cross— sectional/organisational collabora—tion, healthcare professionals in community hospitals should collaborate with specialists and staff in advanced treatment hospitals, and with staff in clinics and welfare facilities, to facilitate smooth hospital discharge by sharing patients' and families'background information.10As a community hub for health and social services, community hospitals should commit to both the process of IPC and patients' flow and outcome in delivering integrated care at the commu—nity level.11However, a number of challenges are associ—ated with developing and maintaining interprofessional networks within and across organisations.1213Mean—while, few studies have examined the factors related to IPC in community hospitals.
This study aimed to explore the factors associated with the self— assessment score of IPC in community hospitals with consideration for the effect of confounding factors.
METHODS
Design and setting
The study was conducted under a cross— sectional design using an anonymous self— administered questionnaire.
Surveys were conducted at three primary— level hospitals in Ibaraki Prefecture in Japan. Two hospitals (hospitals A and B) are private, while the third (hospital C) is a public healthcare institution, and all are located 1—2 hours by car from the city centre. The hospitals have 199, 179 and 183 beds, respectively.14The cities where the three hospitals are located have a population of 30 000, 90 000 and 40 000, respectively. The three hospitals provide community—based and primary care— led service— level care,11including a few specialties (mainly internal medicine, paediatrics and general surgery) and general practice, with limited laboratory services, available for general but not special—ised pathological analysis. All three hospitals have played a key role in a community— based integrated care system for communication among clinics, welfare facilities, and secondary or tertiary hospitals.
Participants
We distributed the anonymous self— administered ques—tionnaire to all healthcare staff via research collabora—tors in the three community hospitals. Study participants included all staff in the three hospitals, excluding those who did not participate in providing healthcare services to patients, such as clerks, engineers and cleaners, and those who did not consent to participate in the study,because we aimed to focus on collaboration within interprofessional team practices with patient involve—ment. The questionnaires were collected from July to October 2018.
variables
The objective variable was the Assessment of Interprofes—sional Team Collaboration Scale (AITCS) score. AITCS is a validated measurement tool developed in Canada for evaluating collaboration within teams across various prac—tice settings and the integration of patient involvement as part of team practice.15In its original form, it consists of 37 items and 3 subscales representing discrete elements of interprofessional care, including (1) partnership/shared decision making, (2) cooperation and (3) coor—dination. The Japanese version of the AITCS was verified for reliability and cultural adaptability in 2018.16This veri—fication identified three corresponding subscales based on factor analysis: ‘Patient— centered collaborative care',‘Teamwork among healthcare professionals' and ‘Patient participation'.
The explanatory variables were selected by reviewing the literature and considering the effect of IPC in community hospitals. First, we defined age, gender and healthcare profession as individual factors. These factors are associated with implicit bias in healthcare settings.17Typically, since nurses tend to adopt a more collaborative culture than other professionals,1819we analysed healthcare profession data by dividing subjects into nurse and non— nurses (other) professions. Addi—tionally, hospital culture can have a marked effect on collaboration.20To meet the community's needs, there is also a growing requirement for IPC both within and across organisations.21Such interorganisational/intraorganisational collaboration can be organised according to individual multidisciplinary teams across the boundaries of different organisations and sectors.22Based on this concept, we selected the hospital to which staff belonged and relationships with neighbouring facilities as other variables. We estimated the neigh—bouring facilities included hospitals or welfare facilities which are located in the same medical administration area for participants' hospital. Moreover, the merits associated with IPC include job satisfaction,2324while disadvantages include emotional burden or collabo—ration burden regarding other professional relation—ships.2526Therefore, participants' characteristics (age,gender, healthcare profession and hospital to which they belonged), relationships with neighbouring facil—ities (determined using the Visual Analogue Scale(VAS)), job burden (VAS) and job satisfaction (VAS)were selected as explanatory variables. This explains why VAS has better responsiveness than the Likert scale and appears to be more closely associated with what participants experience.27For the VAS, partici—pants were asked to mark the point on a 100 mm hori—zontal line, with the end points clearly marked, that was representative of their feeling towards the variable in question. The distance from one end of the line to the participant's mark was measured and used as a quanti—tative variable for statistical analysis.
Statistical analyses
We examined the distribution of each explanatory vari—able. After determining the descriptive statistics, we inves—tigated the association between the explanatory variables and the objective variable, namely the total AITCS score.First, univariate analyses were performed using Pear—son's correlation coefficient. With consideration for age,gender, profession and hospital as potential confounders,variables found to be significant by univariate analysis were considered for multiple regression analysis. To elim—inate potential multicollinearity, significant explanatory variables were reviewed based on the correlation coeffi—cients of similar variables to determine which to include in the multiple regression analysis. All statistical analyses were performed using SPSS V.24 statistical software. All p values were two— sided and considered significant at p<0.05.
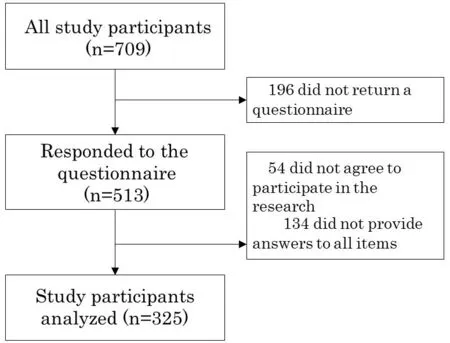
Figure 1 Study participant flow.
Sample size
For multiple regression analyses, the desired level is between 15 and 20 observations for each predictor vari—able.28Accordingly, more than 240 samples were targeted per hospital in anticipation of a 50% response rate.
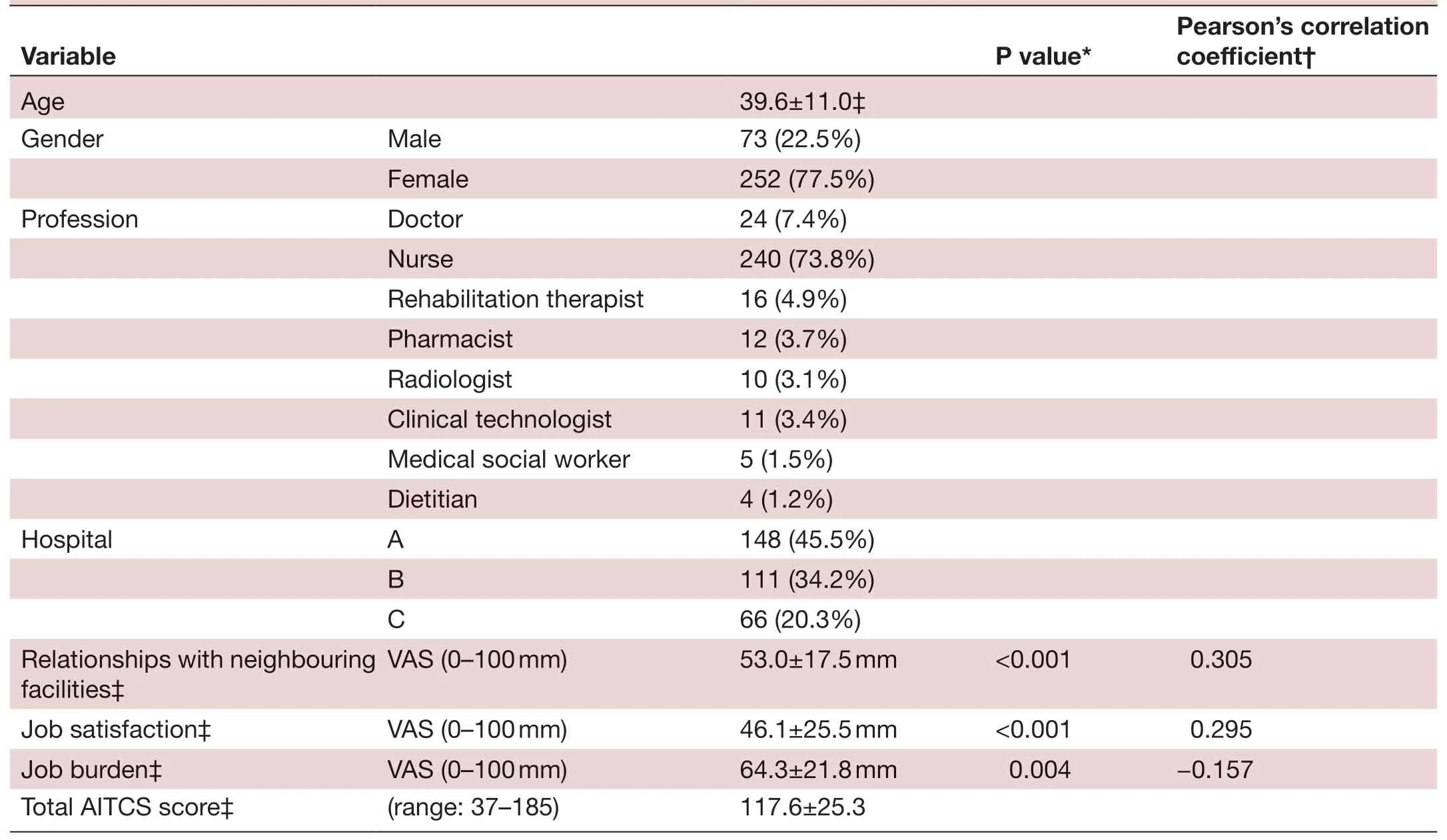
TabIe 1 Participant characteristics (N=325)
RESULTS
A total of 826 questionnaires were distributed, equivalent to the total number of staff in the three participating hospi—tals. Of the 709 participants surveyed, 196 did not return the questionnaire, while the remaining 513 responded.Of these, 54 did not agree to participate in the research and 134 did not provide answers to all items, leaving 325 participants for analysis (figure 1). Among these, 77.5%were female and the average age was 39.6 years. A total of 240 were nurses (73.8%), 24 were doctors (7.4%), 16 were rehabilitation therapists (4.9%) and 12 were phar—macists (3.7%) (table 1). There were 148 (45.5%) partic—ipants from hospital A, 111 (34.1%) from hospital B and 66 (20.3%) from hospital C. Among the 325 participants,the mean±SD of the total AITCS score was 117.6±25.3(range 37—185), and the VAS for relationships with neighbouring facilities, job satisfaction and job burden was 53.0±17.5 mm (0—100), 46.1±25.5 mm (0—100) and 64.3±21.8 mm (0—100), respectively (table 1). Age, rela—tionships with neighbouring facilities and job satisfaction were statistically significantly different among hospitals A,B and C (table 2).

TabIe 2 Comparison of variables among hospitals A, B and C (N=325)
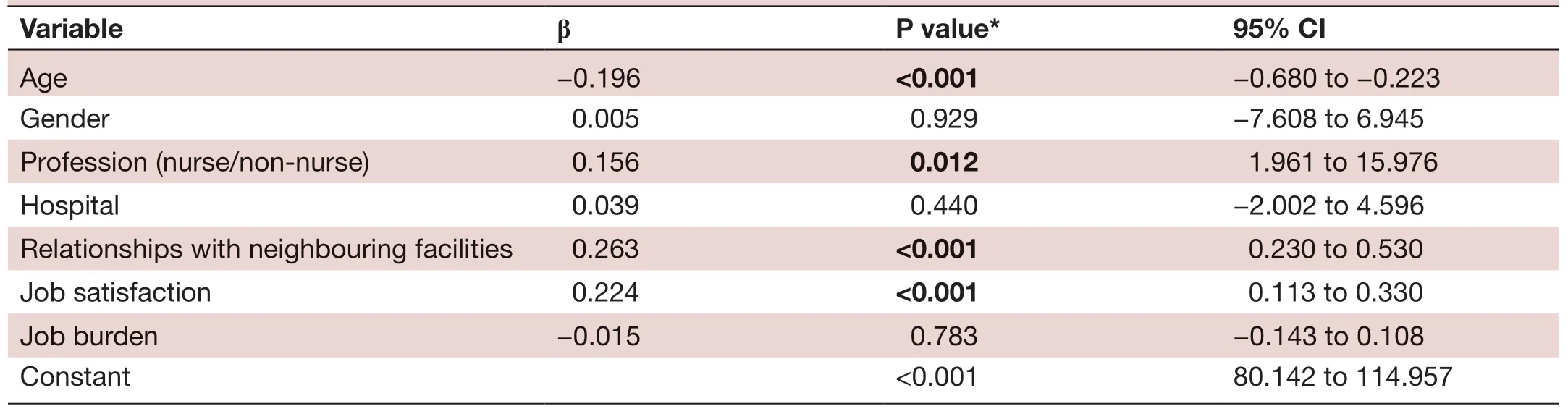
TabIe 3 Independent factors for AITCS
Univariate analyses
The results of univariate analyses of the association between AITCS score and explanatory variables are presented in table 1. Explanatory variables with a significance level of <0.05 were relationships with neighbouring facilities(r=0.305, p<0.001), job satisfaction (r=0.295, p<0.001) and job burden (r=-0.157, p=0.004). No significant correla—tion was observed between any two of these variables. After univariate analyses, we checked the frequency distribution of each variable and confirmed that there was no ceiling or floor effect. All three variables were therefore further exam—ined using multiple regression analysis.
Multiple regression analysis
Multiple regression analysis was performed using an analytical model that included the following explanatory variables: age, gender, profession (nurse or non— nurse),hospital to which the staff belonged (A, B and C), rela—tionships with neighbouring facilities, job satisfaction and job burden. The results are presented in table 3. The beta coefficients (β) of age, profession (reference, nurse), rela—tionships with neighbouring facilities and job satisfaction in the AITCS total score were -0.196 (95% CI -0.68 to -0.22,p<0.001), 0.156 (95% CI 1.96 to 16.0, p=0.012), 0.263 (95%CI 0.230 to 0.530, p<0.001) and 0.224 (95% CI 0.11 to 0.33,p<0.001), respectively.
DISCUSSION
The AITCS score, a self— assessment score of IPC, was associated with age, profession (nurse/non— nurse), rela—tionships with neighbouring facilities and job satisfac—tion. Our findings suggest that younger professionals or nurses may be ideal members to lead community hospi—tals in increasing opportunities for IPC among clinics,welfare facilities, and secondary or tertiary hospitals,and to enhance self— efficacy— associated job satisfaction.Given that evidence on the effectiveness of community hospitals is relatively scarce, these findings may be useful for systematic changes in community hospitals, which can play the role of community hub to provide health and social services based on a more locally integrated health and care system.
Younger age was associated with higher total AITCS score. This is inconsistent with previous reports which suggest that it is typically difficult for novice profes—sionals to play the role that other professionals envision of them within their own profession and to understand the contextual roles of other professions.2930IPC requires that mutual professionals learn expected roles with, from and about each other through prolonged interprofes—sional communication across many years. Based on their prerequisite education, it is likely that young healthcare professionals may regard superficial sharing of infor—mation as IPC,3132suggesting that younger healthcare professionals may tend to think that they conduct better IPC than older healthcare professionals. Younger profes—sionals who are motivated to collaborate more within and across organisations may play a critical role in IPC.
Nurses also play a critical role in IPC33and should there—fore be more autonomous in IPC.34Additionally, nurses can lead other professionals in effective IPC and create a culture that encourages the values and role models of collaborative practice within a team context.35These characteristics of nurses may affect the self— assessment score of IPC.
Relationships with neighbouring facilities reflect interorganisational relationships. To enhance the effec—tiveness of interorganisational relationships, communi—cation should be formal and informal within and across organisations.34Additionally, because the degree of organisational relationships is linked to levels of collab—oration, effective relationships across organisations should be active, regular, reciprocal, open and comfort—able for communication among members.36Such open and flexible communication styles within or across organisations may promote effective horizontal and vertical IPC. Horizontal integration refers to peer— based and cross— sectoral collaboration to improve overall health, while vertical integration refers to that which transcends organisational boundaries and connects community— based generalists with largely hospital— site specialists.10Both types of collaboration can interact with each other and break down the walls of multipro—fessionals and multiorganisations.
Other studies have shown that job satisfaction is associ—ated with interprofessional perspective,37team climate,38and organisational culture and teamwork.3940While a number of previous studies have demonstrated that organisational culture is important for IPC,4142we found that relationships with neighbouring facilities were more strongly associated with IPC than the hospital to which participants belonged in multiple regression analysis.Moreover, job satisfaction was independently associated with IPC even after accounting for confounding factors.That healthcare professionals in community hospitals may regard IPC as their role may explain the association of the self— assessment score of IPC with job satisfaction.41
This study has several limitations. First, confounding factors of AITCS were defined as participants' charac—teristics, namely age, gender, healthcare profession and hospital to which they belonged, and potential associ—ated factors were relationships with neighbouring facili—ties, job burden and job satisfaction. It is likely that there were other confounding factors given that IPC is used as a dimension of organisational culture,43leadership is a dimension of teamwork, and climate is highly associated with culture.39However, this study showed that factors associated with the organisational culture of different hospitals were not independently associated with IPC in multiple regression analysis. Second, this study focused on only separating nurse and non— nurses (other) as profession categories. A larger sample is more representa—tive of the population and needed to analyse detail factors(more professional categories, and the size of clinics and hospitals, and so on). Third, the findings may not be generalisable to all community— based hospitals. However,comparison of the low response rate with that in other studies in healthcare27suggests that these findings may be useful for developing an interprofessional education system in community hospitals. Given that evidence on the effectiveness of community hospitals is relatively scarce, a strength of our study is that our findings may be useful for systematic changes in community hospitals to enhance the integration of service delivery and benefit to the community. In particular, Japan has a unique work culture comprising a hierarchical and relationship—dependent climate within organisations, and workers are expected to be hard working. Given that this cultural background may differ among countries, it is important to compare factors associated with IPC in other cultures.
CONCLUSION
Better self— assessment score of IPC was associated with younger age, a nursing profession, better relationships with neighbouring facilities and greater job satisfaction in community hospitals in Japan. These findings may be useful for helping community hospitals to play the role of community hub to provide health and social services based on a more locally integrated health and care system.
Contributors JH, SO and GR were involved in the conception and design of this study, carried out all qualitative enquiries, analysed the data and wrote the paper.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not- for- profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This study was approved by the Ethics Committee of the University of Tsukuba (approval number: 1202-3).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement The datasets during and/or analysed during the current study available from the corresponding author on reasonable request.
Open access This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY- NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non- commercially,and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non- commercial. See: http:// creativecommons. org/ licenses/ by- nc/ 4. 0/.
 Family Medicine and Community Health2019年4期
Family Medicine and Community Health2019年4期
- Family Medicine and Community Health的其它文章
- From potential to practice: how accelerating access to HPV tests and screen and treat programmes can help eliminate cervical cancer
- Care and social support from family and community in patients with pulmonary tuberculosis in Pakistan
- How French general practitioners adapt their care to patients with social difficulties?
- Improving sexual and reproductive health knowledge and practice in Mozambican families with media campaign and volunteer family health champions
- Improving patient satisfaction through improved telephone triage in a primary care practice
- Exploring the influencing factors for non- utilisation of healthcare facilities during childbirth: a special mixedmethod study of Bangladesh and 13 other low- and middle- income countries based on Demographic and Health Survey data