
Multidisciplinary team for the diagnosis and treatment of 2 cases of primary intestinal yolk sac tumor
2018-12-07 06:21:42QiujuanHuangChangxuLiuRuijunTangJieLiWeiLiLeiZhuYuhongGuoLinZhangTongyuanQuLingyiYangLingmeiLiYaleiWangBaocunSunBinMengJieYanWenguiXuHuilaiZhangDengfengCaoWenfengCao
Cancer Biology & Medicine 2018年4期
Qiujuan Huang, Changxu Liu, Ruijun Tang, Jie Li, Wei Li, Lei Zhu, Yuhong Guo, Lin Zhang,Tongyuan Qu, Lingyi Yang, Lingmei Li, Yalei Wang, Baocun Sun, Bin Meng, Jie Yan, Wengui Xu,Huilai Zhang, Dengfeng Cao, Wenfeng Cao
1Department of Pathology, Tianjin Medical University Cancer Institute and Hospital, National Clinical Research Center for Cancer, Key Laboratory of Cancer Prevention and Therapy, Tianjin; Tianjin's Clinical Research Center for Cancer, Tianjin Medical University, Ministry of Education, Tianjin 300060, China; 2Department of Pathology, Guilin TCM Hospital of China,Guilin 541002, China; 3Department of Pediatric Oncology; 4Department of Lymphoma; 5Department of Molecular Image and Nuclear Medicine, Tianjin Medical University Cancer Institute and Hospital, National Clinical Research Center for Cancer, Key Laboratory of Cancer Prevention and Therapy, Tianjin, Tianjin's Clinical Research Center for Cancer, Tianjin 300060, China;6Department of Pathology, Tianjin Central Hospital of Gynecology Obstetrics, Tianjin 300110, China; 7The Lauren V Ackerman Laboratory of Surgical Pathology, Division of Anatomic and Molecular Pathology, Department of Pathology and Immunology, Washington University School of Medicine, Saint Louis, MO 63110, USA
ABSTRACT Extragonadal primary yolk sac tumor of the intestinal tract origin is exceedingly rare. Through a multiple disciplinary team, the diagnosis and treatment of primary intestinal yolk sac tumor were further defined. We report 2 such cases with detailed histologic and immunohistochemical analysis. The two patients were a 7-year-old girl and a 29-year-old woman. Both of them preoperatively had an elevated serum alpha fetoprotein (AFP) level (≥ 1,210 ng/mL). The tumors are located in the intestine and imaging examination indicated the rectum as the primary site. Grossly the mass was grey-white and crisp texture. Microscopic examination featured reticular, microcystic, macrocystic, papillary, solid, and some glandular patterns. Immunohistochemically,tumor cells of both cases were positive for SALL4, AFP, pan-cytokeratin (AE1/AE3), and glypican-3. Simultaneously, a stain for EMA, OCT4, CD30, HCG, vimentin and CK20 were negative in all 2 neoplasms. The features of morphology,immunohistochemistry, laboratory examinations and imaging studies consist of the diagnosis of primary yolk sac tumor of the intestine.
KEYWORDS Yolk sac tumor; intestine; extragonadal; immunohistochemistry; multidisciplinary team (MDT)
Primary extragonadal yolk sac tumors (YSTs) originating in the intestinal tract are exceedingly rare. Through a multidisciplinary team (MDT), diagnosis and treatment of primary intestinal YST patients were further defined. We reported 2 such cases with detailed histological and immunohistochemical analysis. The patients were a 7-year-old girl and 29-year-old woman. Preoperatively, both of them had an elevated serum alpha fetoprotein (AFP) levels(≥ 1,210 ng/mL). In both patients, tumors were located in the intestine; imaging examination indicated the rectum as the primary site. Grossly, the masses were grey-white and had crisp textures. Microscopic examination revealed reticular,microcystic, macrocystic, papillary, solid, and some glandular patterns. Immunohistochemically, cells of both tumors were tested positive for SALL4, AFP, pan-cytokeratin (AE1/AE3),and glypican-3. Simultaneously, cells of both tumors were tested negative for epithelial membrane antigen (EMA),OCT4, CD30, human chorionic gonadotropin (HCG),vimentin, and cytokeratin 20 (CK20). According to morphological features and results of immunohistochemical,laboratory, and imaging examinations, both cases were diagnosed as primary YSTs of the intestine.
A YST or endodermal sinus tumor was first described by Teilum1-4and is one of the most common malignant germ cell tumors. YST mainly occurs in the gonads5; however, it may also occur in extragonadal sites6, typically in midline structures including the sacrococcygeal region, retroperitoneum,mediastinum, central nervous system, and vagina6-9. Other rare primary sites for YST include the nasal cavity, orbit,lung, stomach, bladder, endometrium, and thigh10-16. So far,primary YST in the intestine has not been reported. In this study, we retrospectively analyzed 2 patients with primary yolk sac tumor of the intestinal tract who were admitted to Tianjin Medical University Cancer Institute and Hospital between December 2015 and November 2017. With MDT discussions, the diagnostic and treatment processes were optimized and patients were provided with the best treatment options.
Case summary
Case 1
Case 1 involved a 7-year-old girl with no past medical history presenting with intermittent abdominal pain for approximately 1 month that was not relieved with antiinflammatory treatment. A subsequent abdominal computed tomography (CT) scan in a local hospital showed peritoneal effusion and retroperitoneal lymphadenopathy. Her AFP level was 1,210 ng/mL (normal range: < 25 ng/mL).Ultrasonography examination showed multiple enlarged abdominal and retroperitoneal hypoechoic lymph nodes.Positron emission tomography (PET)-CT showed a mass located in the right abdomen at the level of the fourth and fifth lumbar vertebrae; the adjacent intestinal wall boundary was unclear, indicating a primary intestinal malignant tumor(Figure 1). The bilateral ovaries and fallopian tubes as well as the uterus, cervix, and vagina were unremarkable. The patient underwent segmental jejunal resection.
The resected jejunal mass measured 4 cm in the largest dimension and involved the full thickness of the jejunum.The cut surface of the tumor was grey-white in color.Histologically, the tumor cells showed multiple patterns including microcystic, reticular, macrocystic, papillary, solid,and tubule-glandular structures (Figure 2). The tumor cells had large, irregular, pleomorphic nuclei with vesicular chromatin and variably prominent nucleoli. The tumor cells had moderate to abundant cytoplasm that was clear, mixed clear, or eosinophilic. Mitotic figures were abundant(highest, 18–20/10 high power fields). Pathologically, the lymph nodes were reactive hyperplasia, including two ileocecal lymph nodes and one small mesenteric lymph node.Immunohistochemically, the tumor cells tested positive for AE1/3 (90%), CK8/18 (90%), AFP (60%), glypican-3 (90%),CDX2 (70%), SATB2 (20%), and SALL4 (90%). The tumor cells tested negative for EMA, OCT4, CD30, and CK20(Table 1). Histological features and the immunohistochemical profile were consistent with YST.
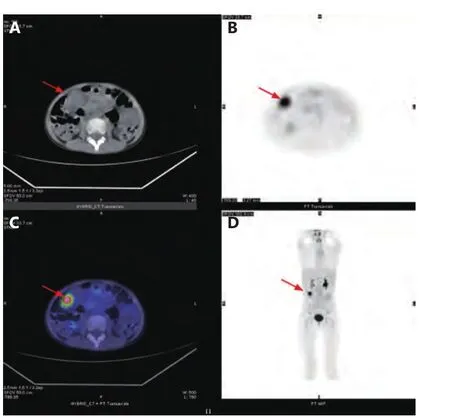
Figure 1 18F-FDG PET/CT imagings of jejunum YST patient(female, 7 years old). (A) CT plain scan shows the soft tissue shadow of jejunum in the lower right abdomen. The CT value is 40 Hu, the size is about 1.7 cm x 2.2 cm. (B) PET shows the abnormal concentration nodules of 18F-FDG uptake in the right lower abdominal. SUVmax is 7.8. (C) The PET/CT image is the fusion of CT (A) and PET (B), showing the lesions. (D) MIP of patient's whole body, showing abnormal accumulation of 18F-FDG uptake in the right lower abdomen (arrows).
After surgery, her serum AFP level dropped to the normal range. She received the bleomycin, etoposide, and cisplatin(BEP) chemotherapy regimen; CT did not show tumor recurrence at the 4-month follow-up examination.
Case 2
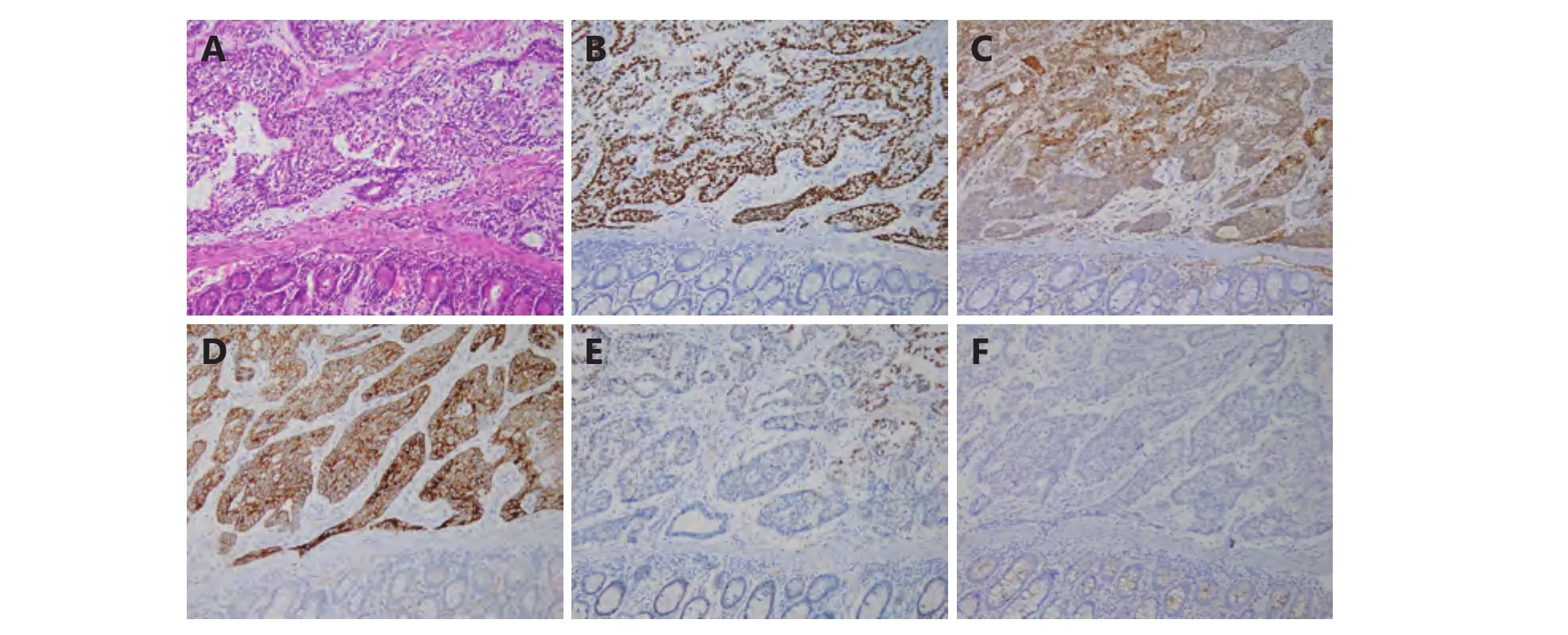
Figure 2 The YST in case 1 does not involve the mucosa and shows solid and glandular pattern with myxoid stroma (A, SP staining, 200 ×).Immunohistochemically the tumor cells are diffusely positive for AFP (B, SP staining, 200 ×), glypican-3 (C, SP staining, 200 ×) and SALL4 (D,SP staining, 200 ×). The tumor cells are focally positive for SATB2 (E, SP staining, 200 ×) and negative for EMA (F, SP staining, 200 ×) .

Table 1 Immunohistochemical profile of primary YST of the intestine
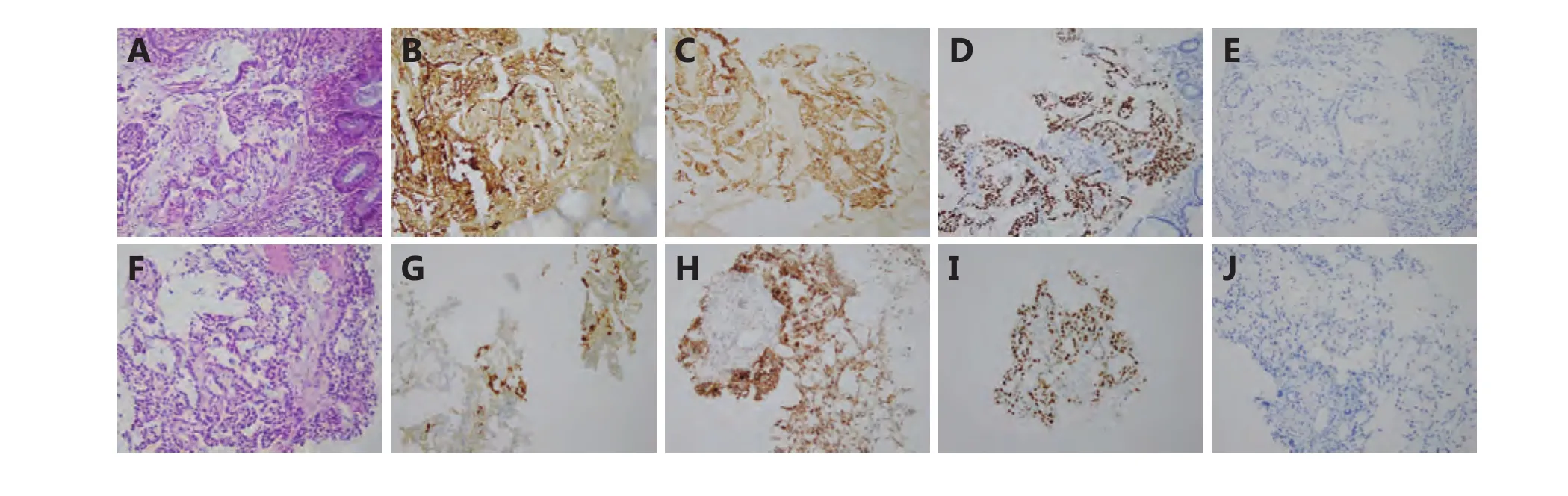
Figure 3 The YST in case 2 shows microcystic and glandular patterns with myxoid stroma (A, SP staining, 200 ×). The tumor cells are diffusely positive for AFP (B, SP staining, 200 ×), glypican-3 (C, SP staining, 200 ×), SALL4 (D, SP staining, 200 ×) and negative for SATB2 (E,SP staining, 200 ×). The metastatic YST in the liver shows similar morphology (F, SP staining, 200 ×) and immunohistochemically it is focally positive for AFP (G, SP staining, 200 ×) but diffusely positive for glypican-3 (H, SP staining, 200 ×), SALL4 (I, SP staining, 200 ×) and negative for SATB2 (J, 200 ×).
A 29-year-old woman presented with anorexia, abdominal distension, and large bowel habit change. An abdominal ultrasound examination at a local hospital showed multiple solid space-occupying lesions in the liver. Her serum AFP level exceeded 1,210 ng/mL (normal range, < 25 ng/mL).PET-CT showed a rectal mass measuring 5.5 × 4.9 × 4.7 cm.Colonoscopy examination revealed that the tumor was located 15 cm above the anal edge and that the rectal lumen was narrowed. She was referred to our hospital and underwent liver needle biopsy. Histologically, the neoplasm cells had abundant, pale eosinophilic cytoplasm and vesicular nuclei; the cells were arranged into reticular, microcystic, and some papillary structures (Figure 3). Immunohistochemically, the tumor cells tested positive for AE1/3 (95%),SALL4 (90%), AFP (70%), placental alkaline phosphatase(30%), and glypican-3 (90%). The tumor cells tested negative for CK20, EMA, OCT4, CD30, SATB2, and beta-HCG(Table 1). Morphological and immunohistochemical patterns supported the diagnosis of metastatic YST in the liver. One week later, the rectal mass was biopsied; it showed morphological features that were similar to that of the liver tumor. Based on the solitary rectal mass, multiple liver lesions, and absence of tumors at other sites including the ovaries, we believe that the rectal tumor was the primary tumor that had metastasized to the liver. The patient received BEP chemotherapy. After six cycles of chemotherapy, her serum AFP levels gradually dropped to the normal range.Through repeated CT examination, we found that the rectal tumor with a diameter of 5.5 cm had completely disappeared,and the multiple metastases in the liver had also reduced significantly. At the last follow-up at 27 months, she was alive with disease in her rectum and liver, with no progression or additional metastasis.
Discussion points
1) Pathological features and diagnosis of primary YST of the intestine; 2) the possible tissue origin of extragonadal YSTs;3) treatment options for patients with primary intestinal YSTs; 4) imaging features of primary intestinal YSTs; 5) the importance of knowledge about YSTs originating from the intestinal tract to clinicians and pathologists.
Clinical discussion
An MDT involves a multifaceted team of professionals who work concertedly to strategize a treatment plan for a patient.Especially for patients with tumors and rare diseases, the MDT model can achieve individualized and optimized diagnostic and treatment strategies, resulting in better outcomes and ultimately, greater patient satisfaction. In this study, we reported 2 primary YSTs of the intestinal tract (case 1, in jejunum; case 2 in rectum). To our knowledge, our study is the first to report primary YST in the intestinal tract.Through MDT discussions, our patients were accurately diagnosed and precisely treated.
Pathology Department: The diagnosis of YST relies on typical morphology with confirmatory immunohistochemical markers. The difficulty in correctly diagnosing YST in the intestinal tract lies partly in the fact that pathologists may not think of this entity in an unusual location. The pathognomonic feature of YST is the Schiller-Duval body but it is only present in one-thirds of YSTs in the ovary. In our study, there was no Schiller-Duval body in the first case. In case 2, the limited biopsy material from the rectum and liver did not show a Schiller-Duval body. Another characteristic feature of YST is the presence of multiple histological patterns within the same tumor, as demonstrated by both our cases. Common immunohistochemical markers for YST include AFP, glypican-3, and SALL4. Among them, SALL4 is the most sensitive. The major differential diagnoses for primary YST in the intestinal tract are metastatic YST from the gonads and other midline sites and primary intestinal adenocarcinoma. It is difficult to distinguish between intestinal adenocarcinoma and intestinal YST because YSTs often show positive expression of CDX217. A panel of immunohistochemical markers should be used to distinguish between them rather than relying on one marker such as CDX2. Meanwhile, SATB2, a sensitive and specific marker for intestinal adenocarcinoma, plays a vital role in distinguishing between the two neoplasms18. YSTs typically show negative expression of EMA but intestinal adenocarcinomas show positive expression. In addition, AFP,glypican-3, and SALL4 are not expressed in intestinal adenocarcinomas. Regarding liver metastasis, metastatic YST should also be distinguished from primary liver tumors including rare YST, hepatocellular carcinoma, and hepatoblastoma. Metastatic YSTs are distinguished from primary liver YSTs based on clinicopathological correlation,as histological features and immunohistochemical markers are not useful for this purpose. Hepatocellular carcinomas and hepatoblastomas also show positive expression of AFP and glypican-3. In hepatoblastomas, SALL4 is positively expressed in all embryonal components in all cases and in the fetal component in some cases; however, it is negatively expressed in the small cell undifferentiated and mesenchymal components19. Typically, YST shows diffusely positive expression of SALL420-22.
YST mainly occurs in the gonads5but it may also occur at extragonadal sites; 24% of YSTs occur at extragonadal sites.The origin of primary extragonadal YSTs is still controversial.Some theories have been proposed. The first theory is that these tumors originate from abnormally differentiated somatic cells; this can explain rare YSTs in non-midline extragonadal sites, such as the orbit, ear, lung, omentum, and intestinal tract11,12,23,24. The second theory is that extragonadal YSTs arise from germ cells which have been misplaced during embryogenesis when germ cells migrate from the primitive urogenital ridge to the gonads23,24. The early germ cell precursor is immediately reprogrammed to pluripotency. This theory explains the reason why extragonadal YSTs mainly occur in the midline25. The third theory is that germ cells exist in all tissues10, and this is the least convincing theory. The fourth theory involves evolution of the yolk sac during embryonic development. As we all know, the yolk sac is separated from the original intestine and gradually degenerates in the 5–6thgestational week.Subsequently, it becomes a small sac that is less than 5 mm in diameter and remains on the surface of the placenta in the 7–8thgestational week. The secondary human yolk sac consists of the primitive endoderm, correlating with various types of extraembryonal and somatic cell differentiation, as a source of organs and tissues derived from the foregut (liver,stomach, lung etc.), midgut, and hindgut (small and large intestine, bladder epithelium, etc.)17,20. This can also explain the etiologies of intestinal YST. The last theory is about the genetic origin of tumors, which states that tumors arise through mitosis of somatic or germ cells10.
Department of Pediatric Oncology and Oncological Surgery: Given the rarity of primary extragonadal YSTs, these tumors are often treated with strategies that are similar to those used for gonadal germ cell tumors. Radical surgical resection combined with adjuvant chemotherapy (BEP regimen) and/or radiation are often used for primary ovarian YSTs26,27. Some specialists have also proposed surgery and chemotherapy for extragonadal YSTs10,14,26. The patients can be followed by measuring their serum AFP levels. Our patient 1 had no evidence of disease and her AFP level dropped to the normal range after surgery even though the follow-up period was short. AFP secretion has been observed as early as the 5thgestational week and it is secreted throughout the evolution of the secondary human yolk sac17.
With the exception of preoperative elevated serum levels of AFP, extragonadal YSTs lack a characteristic clinical manifestation, which is mainly dependent on the size and location of the tumor and its relationship with adjacent organs, tissues, nerves, and so on. In case 1, the patient mainly presented with abdominal pain, incomplete intestinal obstruction, and progressive elevation of AFP levels.Currently, there is no unified treatment or standardized administration regimen for extragonadal YST owing to its low incidence and high degree of malignancy. Local excision of the lesion was the best treatment option for this patient. It could both relieve symptoms and further confirm the diagnosis. The surgical plan is mainly based on tumor site and clinical stage. The tumor was located in the jejunum during operation and there was no obvious adhesion with the surrounding tissues. She underwent segmental jejunal resection and anastomosis. Margins of resection were deemed free of the tumor, which is the key to improvement of cure rates of intestinal YST and provides a reliable guarantee for control of local recurrence. According to the criteria for staging and risk stratification of childhood germ cell tumors, the patient was classified as stage I and intermediate risk.
Medical Oncology: YSTs belong to an inferior class of germ cell tumors with a peak incidence in young women and adolescent girls. Approximately 80%–90% of YSTs arise in the reproductive organs but they may also occur in extragonadal regions. Two-thirds of patients have stage I tumors at the time of diagnosis. The optimal treatment is surgical resection of the tumor, followed by adjuvant chemotherapy (BEP)28. The 5-year survival rate for tumor stages I, II, III, and IV have been reported to be 96%, 75%,30%, and 25%, respectively29. In the last 20 years, survival rates have improved dramatically because of various combination chemotherapy regimens. Almost all patients with early-stage tumors and most patients with advancedstage tumors show long time survival30-32.
Surgery is the initial step in diagnosing and treating patients30. As most patients present with the disease at reproductive ages, there must be an emphasis on fertility preservation. Fertility-sparing surgery appears to be safe with excellent survival rates after long-term follow-ups; patients undergoing hysterectomy with bilateral salpingooophorectomy show similar outcomes. Patients presenting with advanced-stage and bulky abdominal and pelvic masses have traditionally been managed with upfront debulking surgery. Sometimes, rapid growth of the postoperative tumor may limit the utility of the initial surgery. Therefore,neoadjuvant chemotherapy has been increasingly used in histologically confirmed patients to increase the chances of successful fertility-preserving surgery and to minimize the extent of surgery required to achieve maximal cytoreduction.This is not the current standard of care but it deserves future study.
Cisplatin-based combination chemotherapy with BEP leads to cure in most patients. Because of its efficacy and tolerability, BEP has become the standard chemotherapy.Many oncologists recommend the use of 3 cycles of BEP for patients with completely resected disease; 4 cycles of BEP are recommended for patients with macroscopic residual disease,sometimes with the omission of bleomycin30. Patients with persistent and recurrent disease can be treated with either of the following regimens: vinblastine, ifosfamide, and cisplatin;paclitaxel, ifosfamide, and cisplatin; and nanoparticle albumin-bound-paclitaxel. High-dose chemotherapy can also be considered in some patients. In case 2, the patient received BEP chemotherapy without surgery owing to the presence of multiple liver metastasis.
Medical Imaging Department: PET-CT imaging is a molecular imaging technology that combines anatomical and morphological imaging with functional and metabolic imaging. Currently,18F-fluorodeoxyglucose (FDG) PET-CT imaging has been widely recognized in clinical practice for diagnosis, differential diagnosis of benign and malignant tumors, clinical staging, and detection of primary tumor lesions. Most tumor tissues show abnormally high levels of18F-FDG uptake in varying degrees, which provides the basis for identification of benign and malignant tumors. In case 1,the CT images showed a mass located in the right abdomen at the level of the fourth and fifth lumbar vertebrae with an unclear boundary with the adjacent intestinal wall. During PET-CT, there was a pathologically intense accumulation of18F-FDG in the right abdomen (maximum standardized uptake value was 7.8). Eventually, case 1 was diagnosed as a soft tissue mass in the jejunum with locally active metabolism based on the above imaging characteristics; however, specific diagnosis needs further identification and analysis.
Because of the special anatomical location, small intestine tumors often lack typical clinical symptoms to distinguish them from diseases of nearby organs. The incidence of small bowel tumor is very low and accounts for less than 5% of digestive tract tumors, which mainly include adenocarcinomas, stromal tumors, neuroendocrine tumors,lymphomas, etc33. Small bowel adenocarcinomas mainly occur in the duodenum (50.4%), followed by the jejunum(20.4%). Furthermore, small bowel adenocarcinomas are common in adults, with the average age of onset being 65 years. Our patient was a 6-year-old female child. The age of onset and CT features were inconsistent with typical small bowel adenocarcinoma. Stromal tumors are also rare in children. In children, lymphoma is an important small intestinal tumor; it mostly occurs in the ileum and presents with diffuse thickening of the intestinal wall that causes narrowing of the intestine but with few intestinal obstructions. It is usually associated with the abdominal cavity and/or retroperitoneal lymphadenopathy and splenomegaly. Case 1 involved a solitary bowel wall lesion.Thus, a diagnosis of lymphoma was relatively insufficient but it could not be completely ruled out. Some benign diseases could also be considered, such as adenomas, polyps, and lymphoid hyperplasia. Most of these masses invade the lumen of the intestine and rarely grow out of the wall. For example, visible polymorphic polyps in children can be observed as isolated and sporadic manifestations. They are mainly observed in the intestine and are often found owing to repeated intussusception or hemorrhage. Most lymphadenias are located on the intestinal mesenterium and their borders with the intestinal wall are unclear at some places; however, they rarely invade the intestinal lumen,which is also inconsistent with the imaging characteristics of this case. In summary, PET-CT indicated a possible primary intestinal malignant tumor. Postoperative pathology confirmed that it was a YST in the jejunum, which was consistent with preoperative PET-CT imaging features.Because the high malignancy of tumors showed18F-FDG abnormally concentrated lesions on PET/CT, the degree of uptake was related to the degree of malignancy.
In summary, we reported 2 primary intestinal YSTs with morphological and immunohistochemical analysis. A diagnosis of primary YST of the intestinal tract should be made only after excluding the possibilities of metastasis from another site (particularly the gonads) and primary intestinal adenocarcinoma. These patients can be managed with strategies similar to those used for gonadal YSTs. To our knowledge, our study is the first to report primary intestinal YST. Through MDT discussions, we can have a more comprehensive understanding of YSTs. According to patientspecific conditions, standardized and individualized treatment can be provided to maximize patient benefits.
Acknowledgements
This work was supported by Tianjin Municipal Health Bureau Science and Technology Foundation (Grant No.16KG125) and National Clinical Research Center for Cancer.
Conflict of interest statement
No potential conflicts of interest are disclosed.
 Cancer Biology & Medicine2018年4期
Cancer Biology & Medicine2018年4期
- Cancer Biology & Medicine的其它文章
- 2017 Chinese expert consensus on the clinical application of serum marker for thyroid cancer
- Comparison of sentinel lymph node detection performances using blue dye in conjunction with indocyanine green or radioisotope in breast cancer patients: a prospective singlecenter randomized study
- Prognostic factors of refractory NSCLC patients receiving anlotinib hydrochloride as the third- or further-line treatment
- PD-L1 expression and its effect on clinical outcomes of EGFR-mutant NSCLC patients treated with EGFR-TKIs
- Five-CpG-based prognostic signature for predicting survival in hepatocellular carcinoma patients
- A new tumor-associated antigen prognostic scoring system for spontaneous ruptured hepatocellular carcinoma after partial hepatectomy