
Assessment of atrial electromechanical interval using echocardiography after catheter ablation in patients with persistent atrial f i brillation
2016-04-18 11:17:08XiaodongChenMinglongChenYingyingWangBingYangWeizhuJuFengxiangZhangKejiangCao
Xiaodong Chen,Minglong Chen,Yingying Wang,Bing Yang,Weizhu Ju,Fengxiang Zhang, Kejiang Cao,?
1Department of Cardiology,the First Aff i liate Hospital of Nanjing Medical University,Nanjing,Jiangsu 210029,China;
2Department of Cardiology,Geriatrics,the First Aff i liate Hospital of Nanjing Medical University,Nanjing,Jiangsu 210029,China.
Assessment of atrial electromechanical interval using echocardiography after catheter ablation in patients with persistent atrial f i brillation
Xiaodong Chen1,Minglong Chen1,Yingying Wang2,Bing Yang1,Weizhu Ju1,Fengxiang Zhang1, Kejiang Cao1,?
1Department of Cardiology,the First Aff i liate Hospital of Nanjing Medical University,Nanjing,Jiangsu 210029,China;
2Department of Cardiology,Geriatrics,the First Aff i liate Hospital of Nanjing Medical University,Nanjing,Jiangsu 210029,China.
We sought to investigate variation of atrial electromechanical interval after catheter ablation procedure in patients with persistent atrial f i brillation using pulse Doppler(PW)and pulse tissue Doppler imaging(PW-TDI).A total of 25 consecutive in-patients with persistent atrial f i brillation,who restored sinus rhythm after ablation procedure,were recruited in our cardiac center.Echocardiography was performed on each patient at 2 hours,1 day,5 days,1 month and 3 months after the ablation therapy,and atrial electromechanical delay was measured simultaneously by PWand PW-TDI.There was no signif i cant difference between PW and TDI in measuring atrial electromechanical delay. However,at postoperative 2 hours,peak A detection rates were mathematically but nonsignif i cantly greater by PWTDI than by PW.Second,there was a signif i cant decreasing trend in atrial electromechanical interval from postoperative 2 hours to 3 months,but only postoperative 2-hour atrial electromechanical interval was signif i cantly greater than atrial electromechanical interval at other time.Lastly,patients without postoperative 2-hour atrial electromechanical interval had a signif i cantly longer duration of atrial f i brillation as compared to those with postoperative 2-hour atrial electromechanical interval,by the PW or by PW-TDI,respectively.In patients with persistent atrial f i brillation,atrial electromechanical interval may decrease signif i cantly within the f i rst 24 hours after ablation but remain consistent later,and was signif i cantly related to patients'duration of atrial f i brillation.Atrial electromechanical interval,as a potential predicted factor,is recommended to be measured by either PWor TDI after 24 hours,when patients had recovered sinus rhythm by radiofrequency ablation.
atrial f i brillation,echocardiography,tissue Doppler imaging,atrial electromechanical interval
Introduction
Atrial f i brillation(AF)is a common arrhythmia. Catheter ablation is a suitable therapeutic method for atrial f i brillation[1-4].It has been known that AF recurrence is closely related to left atrial structural and electrical remodeling.These changes are frequently seen in post catheter ablation cases[5-9].The electromechanical interval of atrium,which could be measured from onset of P wave in electrocardiogram signal to thetop of A wave in Doppler spectrum(PA Interval),is associated with total atrial conduction time.[10-11]and can effectively ref l ect left atrium remodeling[8-9].It is also an useful indicator to predict new-onset AF occurrence and AF recurrence after radiofrequency catheter ablation[9,12–15].
The PA interval can be obtained by mitral inf l ow pulse Doppler(PW)and Doppler tissue imaging(TDI). Theoretically,TDI is more sensitive and more accurate on measuring PA interval than PW as TDI measures myocardium motion directly.Recently,most studies have chosen TDI to estimate atrial electromechanical delay[14,16-17],while Chao et al.considered that the PA interval derived from PW ref l ected a global atrial electromechanical delay[9].Once a persistent AF(PAF) patient recovers to sinus rhythm after catheter ablation, reverse remodeling of the atrium initiates simultaneously.Data are scarce in the literature regarding whether PA intervals remain or not during the ablation process,as well as when and how the PA interval need to be measured.
We hypothesize the PA interval of PAF patients changes after radiofrequency catheter ablation when sinus rhythm is maintained.The purpose of this study was to explore variations in atrial electromechanical delay through assessment of the PA interval using PW and TDI.
Patients and methods
Patient population
Twenty-nine consecutive PAF patients who were refractory to antiarrhythmic drugs were included in the study at our hospital from August 2013 to March 2014. These cases had been conf i rmed as PAF by 24-h ambulatory ECG monitors,with duration ranging from 1 month to 48 months(mean duration 11.56±15.72 months).The history of selected cases included hypertension(8 cases),diabetes(3 cases),and coronary heart disease(2 cases,1 subject underwent coronary artery PCI operation,with one stent implanted in the anterior descending branch of the coronary artery). Excluded cases comprised reversible AF caused by dysfunction thyroid,alcohol poisoning,post operation, and etc.Analogously,cases manifesting contraindications to anticoagulation,left atrial appendage thrombus on transesophageal echocardiography(TEE)and presence of valvular heart disease or various cardiomyopathies were also taken into account.All cases underwent radiofrequency ablation operation.Four patients were excluded because AF or atrial tachycardia wasrecurrence within3 months after ablation.At last 25 patients completed 3 months of follow-up(containing 18 males and 7 females,mean age 55.44±11.73 years). All patients provided signed informed consent beforeparticipating in the study.The protocol was approved by the local institutional board at the authors'aff i liated institution.Patients'characteristics and echocardiographic measurements are presented in Table 1.

Table 1 Demographic characteristics and echocardiographic measurements of the study subjects(n=25)
Electrophysiological evaluation and ablation
TEE was performed to rule out any intracardiac thrombi.Then,the patients underwent an electrophysiological study in a mildly sedated and local anesthetized state.After transseptal punctures,intravenous heparin was administered to maintain an activated clotting time of 250 to 300 seconds.After catheter placement,a three dimensional(3D)anatomical shell of the LA and PVs was constructed using a circular mapping and/or ablation catheter with an electroanatomical mapping system(EnSite-NavX,St.Jude Medical, Inc.,St.Paul,Minnesota,USA).Catheter ablation was performed using an irrigation catheter(IBI,St.Jude Medical,Inc.,St.Paul,Minnesota,USA),following a sequential ablation strategy.If AF was organized into an atrial tachycardia(AT)or sinus rhythm was directly restored during ablation,complex fractionated electrogram(CFE)mapping and ablation were omitted.Any AT during the procedure was mapped and ablated accordingly.If AF was persisted after f i nishing the predesigned ablation strategy,electrical cardioversion was performed to restore sinus rhythm.Postoperative regimens included administration of amiodarone intravenously for 48 hours,then orally for 3 to 6 months,and simultaneous anticoagulation therapy comprising combined administration of low molecular weight heparin and warfarin for 3 or 5 days,afterwards heparin was withdrawn and oral warfarin anticoagulation was maintained by INR for 2-3.
Instruments and methods
All subjects received preoperative echocardiography with IE33 ultrasound system using a 1-5 MHz transducer(Philips Medical Systems,Bothell,WA, USA)through investigation of the parameters such as left atrial diameter(LAD),left ventricular end-diastolic diameter(LVEDD),and interventricular end-diastolic diameter(IVEDD)of the parasternal long axis plane. LAEF and LVEF were assessed in apical four chamber by Simpson's method.The measured time point was set at 2 hours,1 day(average 25.76±1.79 h),3 days,1 month,and 3 months after catheter ablation.The subjects,whose posture containing supine or left lateral position with calm breathing,were connected with synchronous ECG leads.During echocardiography,in the apical four chamber view,the sampling volume box was placed in the mitral inf l ow tract and Doppler spectrum speed was set to 100 mm/second for acquiring Doppler spectrum(MV-PW).Measurement of ECG P wave was evaluated from the starting point to peak A point with the MV-PW spectrum in lead II(PW-PA interval),as described in Fig.1.TDI was performed by adjusting the spectral pulsed Doppler signal f i lters until a Nyquist limit of 15to 20 cm/second wasreached using the minimal optimal gain.The sweep speed was set at 100 mm/second to optimize the spectral display of myocardial velocities.The pulsed Doppler sample volume(5 mm)was placed at the levels of the lateral mitral annulus.The late diastolic annular velocities(A' wave)of the lateral mitral annulus were measured.In the same view,TDI-PA interval was measured from the P wave starting point to the peak A'wave in PW-TDI spectrum(Fig.1).All indicators were measured repeatedly for three times.The average value was subsequently calculated.
Statistical analysis
Measurement data were analyzed with software SPSS.17.0.Mean±SD was used for quantitative variables and numbers with percentages in parenthesis were used for qualitative variables.The difference of values between each corresponding time point detected by PW-TDI modes was compared with one-way analysis of variance(ANOVA),and Duncan method was applied to calculate the interclass differences. Students't test and Fisher'exact test were applied to compare differences in cardiovascular risk factors and echocardiographic measurements between patients with and without 2-hour-AEI for quantitative and qualitative variables,respectively.P<0.05 was considered to be statistically signif i cant.

Table 2 Atrial electromechanical delays by pulse Doppler and tissue Doppler at different time points after ablation therapy
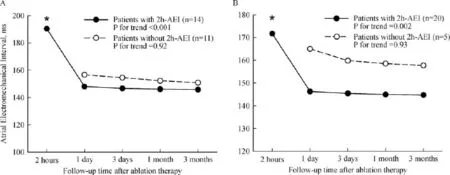
Fig.1 Atrial electromechanical interval measured by pulse-wave Doppler imaging(A)and tissue Doppler imaging(B)at different time points after ablation therapy.Atrial electromechanical interval are shown as in patients with(black circle with solid line)and without 2-h AEI (white circle with dashed line),separately.The P values for AEI trend at different time after ablation were tested by the ANOVA,and Duncan method was applied to calculate the interclass differences.*indicates the interclass differences reach statistical signif i cance.Tissue Doppler imaging has a higher possibility to detect patients'2-h-AEI than pulse-wave Doppler imaging(20/25 vs.14/25,P=0.06).
Results
The atrial electromechanical intervals at different time after ablation,such as 2 hours,1 day,3 days,1 month and 3 months,were compared between the Pulse Doppler group and the tissue Doppler group,but there was no signif i cant difference(P≥0.51,Table 2).
As shown in Fig.1,there were 14 out of 25 patients with available postoperative 2-hour AEI measurements by the pulse Doppler methods,whereas 20 out of 25 patients with available postoperative 2-hour AEI measurements by the tissue Doppler methods.Herein, at postoperative 2 hours,peak A detection rates were mathematically but nonsignif i cantly greater in the tissue Doppler group than in the pulse Doppler group(80%vs. 56%,P=0.07).Second,using the pulse Doppler methods,there was a signif i cant decreasing trend in AEI frompostoperative 2hoursto 6 months(P<0.001),and in the subgroup interclass analysis,only postoperative 2-hour AEI was signif i cantly greater than AEI at other time points(P<0.05).Similarly,using the tissue Doppler methods,a signif i cant decreasing trend was detected in AEI from postoperative 2 hours to 6 months (P=0.002),and in the subgroup interclass analysis, only postoperative 2-hour AEI was signif i cantly greater than AEI at other time points(P<0.05).Moreover,in subjects without available postoperative 2-hour AEI, there was no signif i cant change in AEI from postoperative 1 day to 3 months neither by the pulse Doppler(P=0.92)nor by the tissue Doppler(P=0.93).
In Table 3,cardiovascular risks and echocardiographic measurements were compared between patients with and without postoperative 2-hour-AEI,identif i ed either by the pulse Doppler or by the tissue Doppler. Notably,patients without postoperative 2-hour AEI had a signif i cantly longer duration of PAF as compared by those with postoperative 2-hour AEI,by the pulse Doppler(20.5±10.8 vs.8.1±10.6 months,P=0.0497) or by the tissue Doppler(29.6±16.6 vs.9.6±13.0 months,P=0.008),respectively.Patients without postoperative 2-hour AEI also had a signif i cantly greater LAD than those with 2-hour AEI(44.6±4.8 vs.39.2±4.3 mm,P=0.02).
Discussion
PA interval is a parameter which is derived from the method integrating ECG signal and echocardiography. P wave of ECG represents atrial electrical activity,while A wave of mitral inf l ow based in pulse Doppler and A' wave of the left lateral wall of the mitral annulus based in TDI represent left atrium mechanical movement.PA interval is associated with LAD,LAvolume,total atrial conduction time(TACT)and left atrial voltage[9]. Fuenmayor et al.[10]have demonstrated that the duration from high right atrial activation to the coronary sinus is closely related to PA interval,by means of running standard electrophysiological examination and pulse Doppler.Another study performed by Klaartje et al.[11]demonstrated that PA interval based TDI has high correlation with the duration of P wave based signalaverage ECG(SA-ECG,R=0.91,P<0.001).Therefore,PA intervals assessed by pulse echocardiography or TDI were both reliable indicators to ref l ect inter-atrialconduction of electricity.Notably,the changes of PA interval can ref l ect the process of left atrial electrical remodeling and reverse remodeling[9].TEE and TTE have been frequently used to explore atrial stunning[18–23],especially after TDI technology emerged.As TEE is not easy to be accepted by patients, pulse Doppler spectrum and TDI are prevalent methods to measure PA interval.It is not clear which one of the two is better for evaluating A wave induced by atrial mechanical motion when patients maintain sinus rhythm at the early phase after PAF cardioversion. Atrial stunning can be observed in patients with chronic atrial arrhythmia when their rhythm recovered to sinus rhythm by drugs,electrical cardioversion or ablation[24–27].This chronic atrial arrhythmia is linked to atrial remodeling.Its etiologies are currently considered including atrial cardiomyopathy caused by long-term rapid atrial arrhythmia[28],atrial muscle cell calcium overload[29-30],and atrial myocardial hibernation[31-32]. Atrial reverse remodeling process begins as soon as an atrial arrhythmia recovers to a sinus rhythm.The recovery of atrial mechanical movement is also relevant to how long atrial f i brillation persists.Nevertheless,we have found few reports on atrial electrical activity recovery.Our data demonstrated that the postoperative atrial electromechanical delay(PA interval)was shortened apparently within 1-day post PAF,and with tendency to a steady-state within 3 months follow up. This phenomenon is referred to as the leap phenomenon of PA interval.Therefore,we call this“atrial electromechanical stunning.”Although the underlying mechanism remains unclear,we speculated that atrial electrical activity stayed in a turbulence state that was driven by multiple wavelets in the atrium;upon recovery to a sinus rhythm,atrial stunning attenuated intra left-atrial and reciprocal atrial electrical conductions.Thereafter,with alleviation of calcium overload and recovery of dysfunctional myocardial electrical conduction,atrial electric conduction recovers faster than the recovery of mechanical function.Accordingly, the leap phenomenon of PA interval could be detected as soon as electric conduction is recovered.Different from the restoration of electrical conduction,myocardial mechanical movement recovers much slower and is more unstable in the acute phase.To sum up,we regarded atrial slow conductance within postoperative 24 hours as atrial electromechanical stunning.
In our study,two different echocardiographic methods,PW and TDI,were addressed in measuring PA interval.Our study showed that peak A disappearing in a portion of PAF patients under both modes after conversion,probably due to the presence of atrial stunning.But our data also revealed that peak A disappearing was not recorded in all 25 subjects with PW,and peak A was detectable in 14 cases while 20 cases showed peak A with TDI.MV-PW ref l ects f l ow through the mitral valve,which is affected by several factors,such as contraction of the atrial myocardium, electric conduction of the left atrium,and pressure difference between the left atrial and left ventricle,while TDI is used to quantify the myocardium motion. Therefore,the patients after ablation procedure mayhave left atrium motion detectable by TDI,but may not produce inf l ow through the mitral valve due to disorder in electric conduction of the left atrium,atrium-ventricle dyssynchrony,or low pressure difference between the left atrial and left ventricle.Our study showed that A wave measurement by PW-TDI was signif i cantly higher than that by PW in the 2-hour group after ablation.On one hand,this result demonstrated the existence of atrial stunning;on the other hand,TDI showed high exhibition with atrial myocardium motion.In conclusion,TDI was more sensitive than PW in detecting postoperative peak A in 2 hours.The supposed interpretation underlies PW-PA interval ref l ecting atrial mechanical movement indirectly,while TDI-PA interval ref l ects the atrial myocardial motions directly.The complicated atrial-restarting process,involving chronic atrial reverse remodeling and recovery of currency dynamics,will not accomplish in 24 hours.Our data coincided with the principle of two ultrasonic modes.
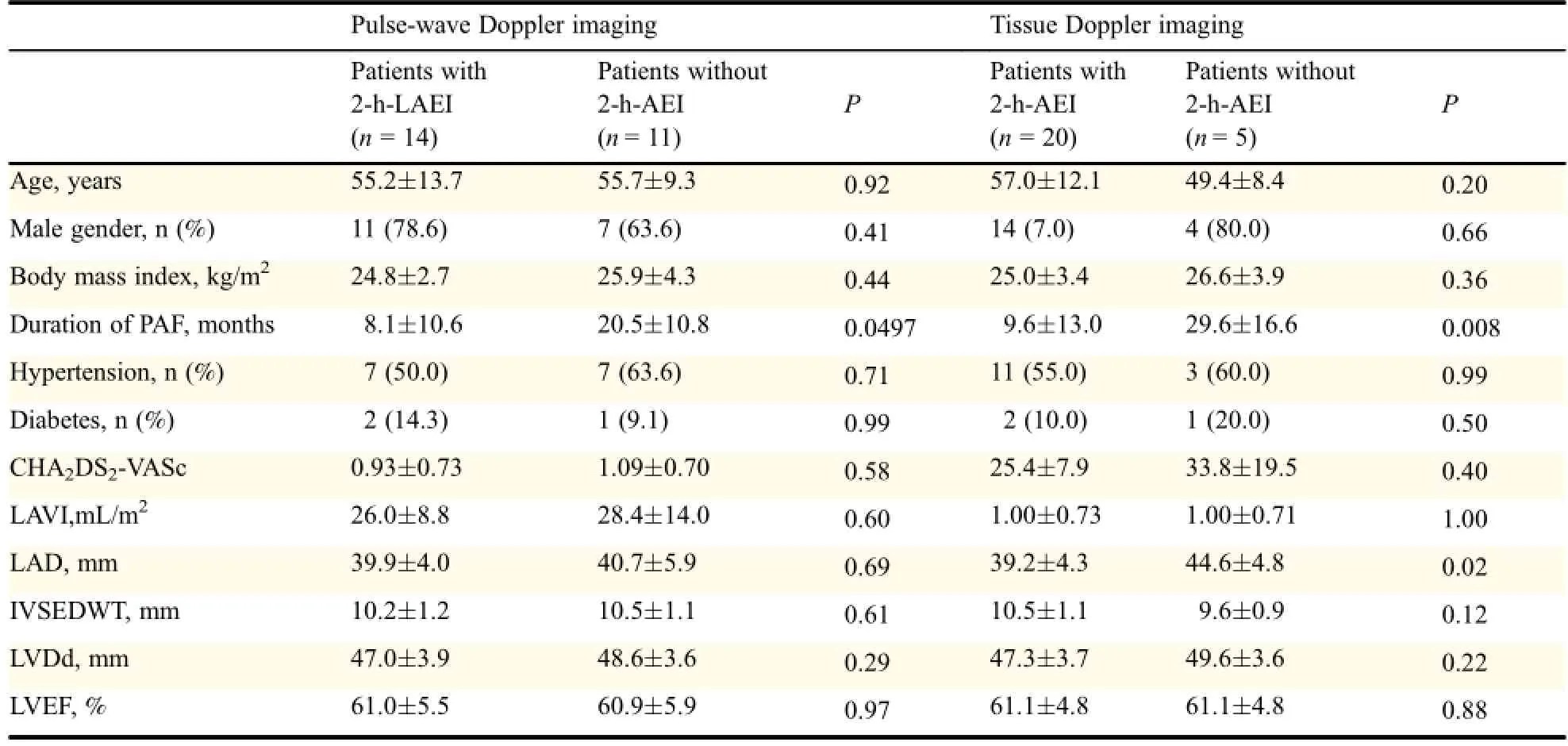
Table 3 Comparison of cardiovascular risks and echocardiographic measurements between patients with and without 2-hour-AEI
Chao et al.[9]disclosed that trans-mitral inf l ow Doppler pattern measurement PW-PA ref l ected the atrial electromechanical delay more accurately than tissue Doppler measurement(TDI-PA),because TDI measurement ref l ected regional myocardial motions; consequently,TDI-PA presented different values of myocardial tissue in different sites.Since there is heterogeneity in myocardial matrix or asynchronous disorder of the left atrium,TDI-PA,an indicator obtained from regional myocardial motions,cannot genuinely evaluate the mechanical motion of the left atrium as a whole.Park et al.[17]argued that only the TDI-PA interval located in the mitral annulus of the left atrial side wall is the independent predictor of AF recurrence.Our data have also shown that there was no statistically signif i cant difference at each corresponding time point on PA interval measured by PWand TDI.We hypothesized that the probable mechanism underlying the left lateral wall is the latest excited part of the left atrium during electrical impulse convey,and thus we referred to the left lateral wall as an alternative site in measuring PA interval,which was capable of ref l ecting atrial electromechanical interval precisely.Therefore, our conclusion is not contradictory to Park's inference[17].Theoretically,PA interval detected by PW-TDI is not as long as that by MV-PW,but our results challenged the viewpoint.We speculated that the possible causes include bias resulting from the insuff icient samples,or difference beyond the detection sensitivity by means of the two methods.
Atrial electromechanical interval measured by echocardiography is usually used as an indicator to predict new-onset atrial f i brillation and atrial f i brillation after catheter ablation,cardioversion or cardiac surgery[9,12–15,33].In these studies,the measuring time of atrial electromechanical interval was not standardized.The earliest measuring time was about 6 hours after cardioversion.Most studies reported the measuring time approximately from several days to several months by either MV-Doppler or TDI[9,12–15].From this study's result,atrial electromechanical interval should be measured 24 hours after recovering sinus rhythm in PAF patients.There may be more sensitivity and specif i city about the interval which was much valuable.
In conclusion,DI detection was more sensitive than PW detection in measuring AEI,which exhibits obvious postoperative leap phenomenon within the f i rst 24 h after ablation and maintains its stability later.AEI was also signi fi cantly related to the duration of atrial fi brillation.
The fi nding in this paper need to be interpreted within the context of limitations.First,this study is limited by the absence of the control group with paroxysmal atrial fi brillation after undergoing radiofrequency ablation.As conclusion in theory,if patients did not have continuous atrial arrhythmia,there was no atrial stunning.Therefore,this study just showed such phenomenon which was f i rst reported in such patients,and it is limited by the relatively small sample size.Second,the 2-hour LAEI may be inf l uenced by medication(such as amidarone,etc.)or cardioversion.However,it is of note that every participant with PAF had both the medication and cardioversion therapy;therefore,in this case,these confounders would be balanced in those patients.
[1] Jones DG,Haldar SK,Hussain W,et al.A randomized trial to assess catheter ablation versus rate control in the management of persistent atrial f i brillation in heart failure[J].J Am Coll Cardiol,2013,61(18):1894–1903.
[2] Pappone C,Vicedomini G,Augello G,et al.Radiofrequency catheter ablation and antiarrhythmic drug therapy:a prospective,randomized,4-year follow-up trial:the APAF study[J]. Circ Arrhythm Electrophysiol,2011,4(6):808–814.
[3] Miyazaki S,Kuwahara T,Takahashi A,et al.Effect of left atrial ablation on the quality of life in patients with atrial f i brillation [J].Circ J,2008,72(4):582–587.
[4] Hunter RJ,Berriman TJ,Diab I,et al.A randomized controlled trial of catheter ablation versus medical treatment of atrial fi brillation in heart failure(the CAMTAF trial)[J].Circ Arrhythm Electrophysiol,2014,7(1):31–38.
[5] Wijffels MC.The natural history of atrial fi brillation:what is the role of atrial remodeling and what can we learn from the atrial de fi brillator[J]?J Cardiovasc Electrophysiol,1999,10(9):1210–1213.
[6] Berruezo A,Tamborero D,Mont L,et al.Pre-procedural predictors of atrial fi brillation recurrence after circumferential pulmonary vein ablation[J].Eur Heart J,2007,28(7):836–841.
[7] Lo LW,Tai CT,Lin YJ,et al.Predicting factors for atrial fi brillation acute termination during catheter ablation procedures:implications for catheter ablation strategy and long-term outcome[J].Heart Rhythm,2009,6(3):311–318.
[8] Chang SL,Tai CT,Lin YJ,et al.Biatrial substrate properties in patients with atrial f i brillation[J].J Cardiovasc Electrophysiol, 2007,18(11):1134–1139.
[9] Chao TF,Sung SH,Wang KL,et al.Associations between the atrial electromechanical interval,atrial remodelling and outcome of catheter ablation in paroxysmal atrial f i brillation[J]. Heart,2011,97(3):225–230.
[10]Fuenmayor AJ,Ramírez L,Fuenmayor AM.Validation of interatrial conduction time measurement by means of echo-Doppler [J].Arch Cardiol Mex,2002,72(2):125–128.
[11]Merckx KL,De Vos CB,Palmans A,et al.Atrial activation time determined by transthoracic Doppler tissue imaging can be used as an estimate of the total duration of atrial electrical activation [J].J Am Soc Echocardiogr,2005,18(9):940–944.
[12]den Uijl DW,Gawrysiak M,Tops LF,et al.Prognostic value of total atrial conduction time estimated with tissue Doppler imaging to predict the recurrence of atrial f i brillation after radiofrequency catheter ablation[J].Europace,2011,13(11): 1533–1540.
[13]Antoni ML,Bertini M,Atary JZ,et al.Predictive value of total atrial conduction time estimated with tissue Doppler imaging for the development of new-onset atrial f i brillation after acute myocardial infarction[J].Am J Cardiol,2010,106(2):198–203.
[14]De Vos CB,Weijs B,Crijns HJ,et al.Atrial tissue Doppler imaging for prediction of new-onset atrial f i brillation[J].Heart, 2009,95(10):835–840.
[15]Omi W,Nagai H,Takamura M,et al.Doppler tissue analysis of atrial electromechanical coupling in paroxysmal atrial f i brillation[J].J Am Soc Echocardiogr,2005,18(1):39–44.
[16]Hoshi Y,Nozawa Y,Ogasawara M,et al.Atrial electromechanical interval may predict cardioembolic stroke in apparently low risk elderly patients with paroxysmal atrial fi brillation[J].Echocardiography,2014,31(2):140–148.
[17]Park SM,Kim YH,Choi JI,et al.Left atrial electromechanical conduction time can predict six-month maintenance of sinus rhythm after electrical cardioversion in persistent atrial fi brillation by Doppler tissue echocardiography[J].J Am Soc Echocardiogr,2010,23(3):309–314.
[18]Jones DG,Haldar SK,Hussain W,et al.A randomized trial to assess catheter ablation versus rate control in the management of persistent atrial fi brillation in heart failure[J].J Am Coll Cardiol,2013,61(18):1894–1903.
[19]Dogan A,Gedikli O,Ozaydin M,et al.Mitral annular velocity by Doppler tissue imaging for the evaluation of atrial stunning after cardioversion of atrial fi brillation[J].Int J Cardiovasc Imaging,2009,25(2):113–120.
[20]Zapolski T,Wysokiński A.Stunning of the left atrium after pharmacological cardioversion of atrial f i brillation[J].Kardiol Pol,2005,63(3):254–262.,discussion 263–264.
[21]Grimm RA,Stewart WJ,Maloney JD,et al.Impact of electrical cardioversion for atrial f i brillation on left atrial appendage function and spontaneous echo contrast:characterization by simultaneous transesophageal echocardiography[J].J Am Coll Cardiol,1993,22(5):1359–1366.
[22]Susam I,Sacar M,Dereli M,et al.Mitral annular velocity in patients with postoperative atrial f i brillation[J].J Surg Res, 2012,178(1):92–95.
[23]Eren M,Oz D.The mitral late diastolic f l ow acceleration slope after the restoration of sinus rhythm in acute atrial f i brillation: relationship to atrial function and change over time[J].Anadolu Kardiyol Derg,2010,10(6):488–494.
[24]Logan WF,Rowlands DJ,Howitt G,et al.Left atrial activity following cardioversion[J].Lancet,1965,2(7410):471–473.
[25]Dell’Era G,Rondano E,Franchi E,et al.,and the Novara Atrial Fibrillation(NAIF)Study Group.Atrial asynchrony and function before and after electrical cardioversion for persistent atrial fi brillation[J].Eur J Echocardiogr,2010,11(7):577–583.
[26]Akyürek O,Diker E,Din?er I,et al.The relation between transmitral early fi lling wave deceleration time and the recovery of atrial contractility after electrical cardioversion of atrial fi brillation[J].Int J Cardiol,2001,79(2-3):151–157.
[27]Manning WJ,Leeman DE,Gotch PJ,et al.Pulsed Doppler evaluation of atrial mechanical function after electrical cardioversion of atrial f i brillation[J].J Am Coll Cardiol, 1989,13(3):617–623.
[28]Manning WJ,Silverman DI,Katz SE,et al.Impaired left atrial mechanical function after cardioversion:relation to the duration of atrial f i brillation[J].J Am Coll Cardiol,1994,23(7):1535–1540.
[29]Daoud EG,Marcovitz P,Knight BP,et al.Short-term effect of atrial f i brillation on atrial contractile function in humans[J]. Circulation,1999,99(23):3024–3027.
[30]Leistad E,Aksnes G,Verburg E,et al.Atrial contractile dysfunction after short-term atrial f i brillation is reduced by verapamil but increased by BAY K8644[J].Circulation,1996, 93(9):1747–1754.
[31]Dispersyn GD,Ausma J,Thoné F,et al.Cardiomyocyte remodelling during myocardial hibernation and atrial f i brillation:prelude to apoptosis[J].Cardiovasc Res,1999,43(4): 947–957.
[32]Ausma J,Wijffels M,van Eys G,et al.Dedifferentiation of atrial cardiomyocytes as a result of chronic atrial f i brillation[J]. Am J Pathol,1997,151(4):985–997.
[33]Müller P,Schiedat F,Bialek A,et al.Total atrial conduction time assessed by tissue doppler imaging(PA-TDI Interval)to predict early recurrence of persistent atrial f i brillation after successful electrical cardioversion[J].J Cardiovasc Electrophysiol,2014,25(2):161–167.
?Corresponding author:Kejiang Cao,M.D.,Ph.D.,Department of Cardiology,the First Aff i liate Hospital of Nanjing Medical University,Guangzhou Road 300,Nanjing,Jiangsu 210029,China, Tel/Fax:13901599830/86-25-85637817;Email:kjcao@njmu.edu.cn.
?2016 by the Journal of Biomedical Research.All rights reserved
Received 05 December 2015,Revised 17 February 2016,Accepted 04 August 2016,Epub 20 September 2016
R445.1,Document code:A
The authors reported no conf l ict of interests.
10.7555/JBR.30.20150164
 THE JOURNAL OF BIOMEDICAL RESEARCH2016年6期
THE JOURNAL OF BIOMEDICAL RESEARCH2016年6期
- THE JOURNAL OF BIOMEDICAL RESEARCH的其它文章
- Pathology and molecular characterization of recent Leucocytozoon caulleryi cases in layer f l ocks
- Modified methods for isolation of pancreatic stellate cells from human and rodent pancreas
- Retrograde traff i cking of VMAT2 and its role in protein stability in non-neuronal cells
- Protein inhibitor of activated STAT 4(PIAS4)regulates liver fi brosis through modulating SMAD3 activity
- Chronic intermittent hypoxia induces cardiac inf l ammation and dysfunction in a rat obstructive sleep apnea model
- Elevated thyroid stimulating hormone levels are associated with metabolic syndrome in a Chinese community-based population of euthyroid people aged 40 years and older