
Disconnect between primary care and cancer follow-up care:An exploratory study from Odisha, India
2015-12-06 09:59:28SanghamitraPatiSukdevNayakDavidWeller
Sanghamitra Pati, Sukdev Nayak, David Weller
1. Indian Institute of Public Health Bhubaneswar, Public Health Foundation of India, 2nd and 3rd Floor, JSS Software Technology Park, E1/1, Infocity Road, Patia, Bhubaneswar 751024, Odisha, India
2. All India Institute of Medical Sciences, Sijua, Bhubaneswar 751019, Odisha, India
3. Ex-Director, Regional Cancer Center, Cuttack Odisha, India
4. Centre for Population Health Sciences, University of Edinburgh, Doorway 1, Medical Quad Teviot Place, Edinburgh EH8 9DX, UK
Disconnect between primary care and cancer follow-up care:An exploratory study from Odisha, India
Sanghamitra Pati1, Sukdev Nayak2,3, David Weller4
1. Indian Institute of Public Health Bhubaneswar, Public Health Foundation of India, 2nd and 3rd Floor, JSS Software Technology Park, E1/1, Infocity Road, Patia, Bhubaneswar 751024, Odisha, India
2. All India Institute of Medical Sciences, Sijua, Bhubaneswar 751019, Odisha, India
3. Ex-Director, Regional Cancer Center, Cuttack Odisha, India
4. Centre for Population Health Sciences, University of Edinburgh, Doorway 1, Medical Quad Teviot Place, Edinburgh EH8 9DX, UK
Objective:There has been a steady increase in the demand for cancer follow-up care in India.Compared with Western countries, there is little evidence on the capacity of the Indian primary care workforce to accommodate such tasks. We explored the perceptions of oncologists, general practitioners, and patients with regard to the involvement of primary care in cancer follow-up care.
Methods:We undertook semistructured focus-group discussions with eight oncologists, nine general practitioners, and 17 cancer patients to gain an understanding of their perceived roles and responsibilities with regard to primary care in delivering follow-up care and the potential concerns.Data from the focus groups were transcribed verbatim, translated, and analyzed with use of a thematic approach.
Results:Most general practitioners felt that their job is to see 'normal' patients, and cancer patients were exceptions to routine care. Oncologists were apprehensive with regard to the competence of general practitioners and patient trust. Patients consult oncologists for cancer follow-up care as they perceive it to be very specialized. Patients expressed difficulty in accessing follow-up care and want specialized oncological care by trained personnel in their vicinity.
Conclusion:Despite the growing number of cancer survivors, we found a disconnect between primary care and cancer follow-up care.
Primary care; cancer follow-up; general practitioner; qualitative perspectives;Odisha; India
Introduction
In the last few decades, commensurate with the steadily improving prognosis of many cancer patients, there has been a considerable increase in the number of cancer survivors globally [1].For example, the 5-year survival probabilities for those aged 15–39 years at diagnosis of breast or testicular cancers are 76% and 97%,respectively [2]. The rise in the number of cancer survivors has, at the same time, resulted in increased workload in the oncology setting for rendering follow-up care. In Western countries,efforts are under way to shift the cancer follow-up care from specialized oncology to primary care [3, 4] settings. India, home to 1.24 billion people, is grappling with the rising burden of noncommunicable diseases(NCD), including cancer [5, 6]. In response to the increasing burden of NCD, the Ministry of Health and Family Welfare has initiated an overarching strategy – namely, the National Programme for Prevention and Control of Cancer, Diabetes, Cardiovascular Disease and Stroke (NPCDCS). Considering the growing number of cancer patients, the NPCDCS's cancer care component has stipulated every district must provide specialized oncology services and envisaged greater involvement of primary care physicians (general practitioners, GPs) in delivering follow-up care [7, 8]. This is pivotal given the fact that primary care is the foundation of health care delivery systems and serves as the first contact point for access to health care services in India [9]. Oncological care remains sacrosanct, being coordinated through designated clinics [10]. Therefore, the first step in decentralizing follow-up care involves understanding the ways in which patients and oncologists think about the role of primary care in delivering cancer care. Furthermore, it is equally important to know the attitudes and interests of primary care physicians for them be involved in such care. Studies conducted in Western countries have identified both facilitators for and barriers to obtaining oncological care and updating GPs with regard to oncological care [11]. However, little is known on the role of primary care in follow-up care in India. Especially,a multiple perspective encompassing oncologists, GPs, and patients is lacking. The available research has been done primarily in high-income countries, and may have limited applicability for India [12–14]. Against this background, we sought to explore and examine the perceptions of health care providers and patients with regard to the involvement of primary care in cancer follow-up care. Patients and oncologists were interviewed to obtain an in-depth understanding of their perceptions regarding the appropriateness of primary care toward delivering follow-up care and the potential challenges. Further, we also attempted to explore how GPs visualize rendering cancer follow-up care within the ambit of their routine work.
Methods
Study design and setting
The research was conducted between May 2014 and February 2015 in Bhubaneswar, Odisha, India. A qualitative approach was deemed most appropriate since the objective was to explore the perceptions, views, and opinions of multiple stakeholders (primary care physicians, oncologists, and patients)with regard to delivering cancer follow-up care in primary care practice. As focus-group interviews are suitable for explorative studies in a new field, our study consisted of four semistructured focus-group interviews [15].
Selection of participants
Thirty-four interviewees comprising nine primary care professionals, eight oncologists, and 17 patients participated.We adopted a purposive and convenient sampling method to recruit the study participants. Oncologists working in three specialized cancer hospitals and four oncology departments of public and private medical college hospitals were approached.Using a stratified purposeful strategy, we recruited primary care physicians from urban, suburban, and rural practices. The sampling goal was to maximize the chances of identifying factors relevant to delivery of follow-up care. We decided to conduct focus-group discussions (FGDs) with GPs and oncologists separately as we expected the two groups would have divergent views owing to their belonging to different professions, leading to different competencies, positions, and tasks in the daily work. We believed that more nuances from the two professions would be presented when they were not together in a mixed group. Patients were drawn from our previous study sample, which comprised patients attending two tertiary oncology hospitals. In the selection of patients, care was taken to ensure maximum diversity in order to obtain a wide and varied picture [15].
Data collection
The study was approved by the Institutional Ethics Committee of the Indian Institute of Public Health, Bhubaneswar. All participants were informed about the research in advance. Before they were interviewed, they were informed in detail of the study purpose, and informed consent was obtained. The FGDs were semistructured; all participating professionals were presented with comparable questions. The FGD guide was developed on the basis of our previous research on patient-reported challenges and barriers in care seeking and similar studies conducted outside India [16–20].
The FGD with oncologists asked about practices surrounding the posttreatment follow-up care of their patients and the professional responsibilities involved in cancer follow-up care.They were asked to reflect on the potential of primary care to undertake follow-up care and to discuss with one another the responses regarding the possible advantages and challenges.
In the FGD with GPs, we first encouraged the GPs to describe their current daily practice. Through this we were able to sense the conventional actions of their profession, their implicit professional norms, their perceptions of their tasks and responsibilities as generalists, and their views on the role of GPs in providing cancer-related care for patients in the posttreatment phase. They were asked questions such as the following: "Are you routinely involved in follow-up care of your patients with cancer? How do you view your role and responsibilities in providing such care? What is your usual policy when cancer patients come to you for consultation?" We also probed the challenges and their needs to enable them to perform such a role.
Two semistructured FGDs were conducted with 17 patients on neutral ground in order to explore opinions and preferences about cancer follow-up care and who should do what and where.They were explicitly asked to reflect on how they visualized receiving care from GPs vis-à-vis oncologists, and were asked about the possible advantages and their potential apprehensions.All interviews were conducted by the same researcher (the first author), who has a medical degree and whose background is in public health. Each FGD lasted 60–90 min on average and was digitally recorded. Audio recordings were then transcribed verbatim and translated for analysis.
Data analysis
The transcripts were inductively analyzed and coded into themes after a process of reading and rereading the interview transcripts and verification with the literature [15, 19]. The first two authors independently identified the patterns and subthemes of the interviews. In conversations with the last author, the initial analysis was refined and further developed.Together, similarities and differences in the professionals'perspectives were looked for, within as well as between the professions involved [21].
Results
Four FGDs were conducted altogether with GPs, oncologists,and patients. First, we identified codes by repeatedly going through the verbatim transcription of the FGD. Table 1 displays the codes extracted from each perspective relevant to primary care and cancer follow-up care. After the codes obtained from individual perspectives of GPs, patients, and oncologists had been synthesized, the overarching theme "challenging current professional identity within the present system of organization of care" emerged [21].
Study participants' views on the role of primary care in management of follow-up care for cancer Primary care physicians:Most GPs wished to continue with their present role as gatekeepers providing primary care.They reported being involved in the prediagnostic phases of cancer and felt they were best prepared to serve as educators to raise awareness of cancer risk and the potential benefits of health promotion. They opined that a GP's job is to see 'normal' patients, and cancer patients being different should not be seen in routine care. They felt neither sufficiently competent to offer nor interested in offering cancer follow-up care, and thought it not to be their responsibility. Some GPs observed that dealing with cancer patients requires a substantial investment of time and effort because of patient anxieties about cancer recurrence and felt challenged by the complex nature of cancer care. The GPs were overall unwilling to provide followup care. There was uncertainty about whether to be involved and their ability to undertake surveillance and manage potential side effects of treatment. A few said they would be willing to provide follow-up care if they were given specific training by oncologists and tailor-made instructions and if there was ongoing communication with the cancer specialist regarding the follow-up care plan. They were also not sure of the appropriateness of treatment of non–cancer-related health problems,which precluded any involvement with cancer patients.
Patients' perspectives:Patients described continual difficulty and financial strain while accessing regular follow-up care. They appreciated being seen by a familiar person who knew their case. Fear of recurrence was the main reason for patients wishing to remain continually in touch with oncologists. They were distressed by minor ailments and thought they could be the manifestation or early signs of recurrence. Patients did not consult primary care physicians for their cancerrelated problems as they perceived follow-up care to be a job for cancer specialists.
Patients wished to maintain contact with their primary care providers during the cancer care process even though they found it difficult to identify a GP role following thediagnosis of cancer. They valued the involvement of GPs in managing their chronic diseases and short-term health care needs. Regarding their views on GP involvement in follow-up care, many thought GPs were too busy in their routine practice, lacked knowledge, or were not interested in cancer care.Patients did not expect GPs to know a great deal about followup care. They emphasized that GPs should know enough to manage their non–cancer-related health concerns, relieve their apprehensions, and provide emotional support. GPs should be able to handle routine ailments, and not have to refer patients to the oncology facility. A number of advantages were identified,including the experience of GPs in managing chronic illness,familiarity of GPs with their patients, geographical proximity, and convenience. The most desired expectation was to have specialized oncology care by trained personnel in their vicinity.
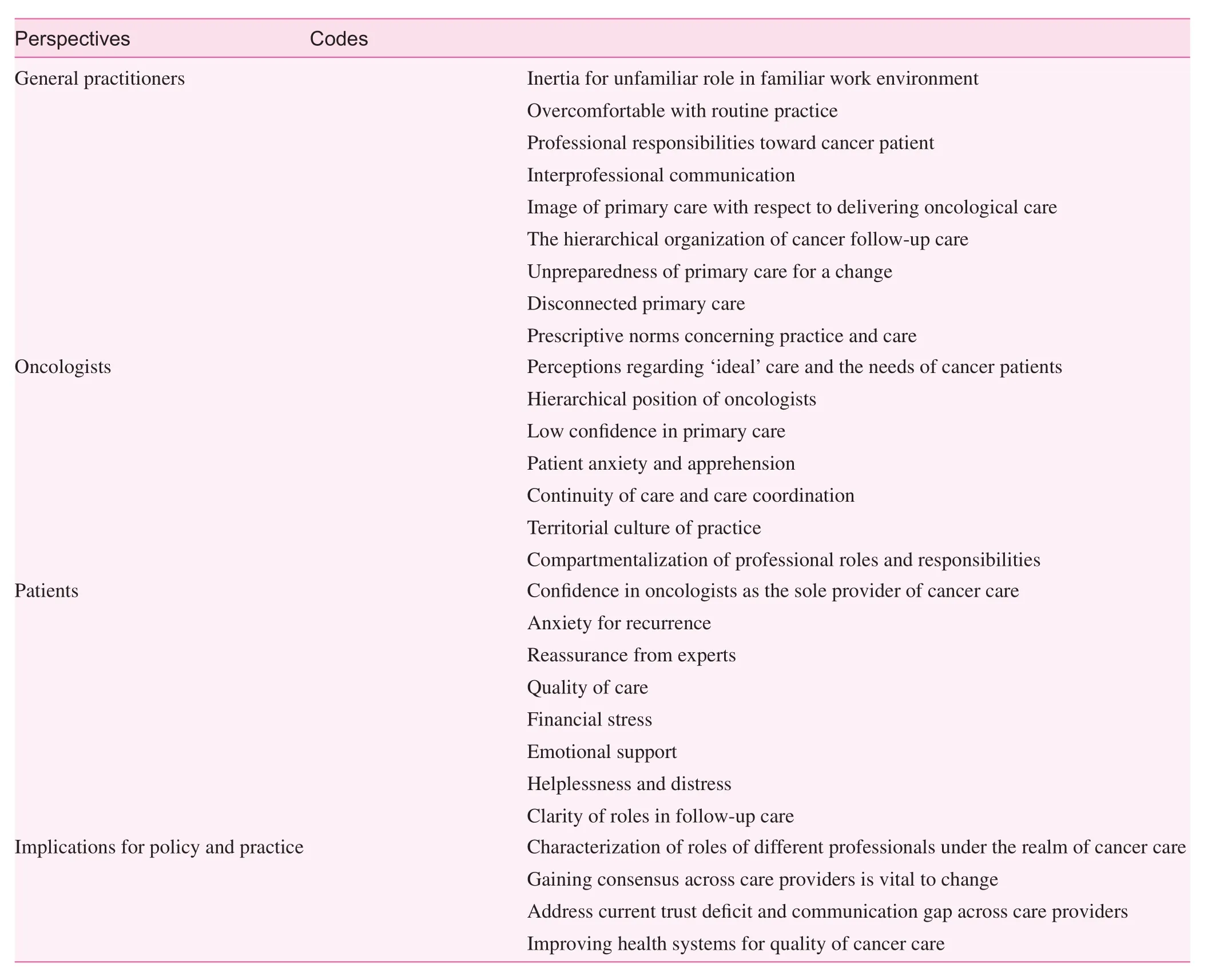
Table 1. Identified codes under each stakeholder perspective
Oncologists' perspectives:Oncologists wanted to stay involved throughout the cancer patients' care trajectory and indicated that they preferred to be the key health care decisionmaker and manager. They expressed a wide range of views(supportive, neutral, and critical) on the levels of engagement with cancer care by GPs. Oncologists recognized a role for GPs limited to the prediagnostic phase, preventive health care in the cancer care process. Regarding the specific role of GPs in relation to follow-up, oncologists felt GPs were not suitably trained to be able to fulfill the required role. The major reasons cited were low perceived ability of GPs and ability to achieve the trust of patients. For oncologists the most important purpose of follow-up was early detection of new malignancies.They argued that even if there is formal transfer of follow-up care to primary care, some patients might not be comfortable returning to their GP for follow-up, the availability of new treatments would necessitate another visit to the oncologist,and GPs need to remain up to date with regard to new knowledge. The patient may become confused and contact GPs for problems that should be referred to an oncologist, thus raising chances of missed care. Another aspect mentioned was the need for psychosocial support. The oncologists described that cancer patients were anxious about their risk of recurrence during follow-up. To alleviate such patients' anxiety and need for reassurance would be difficult for GPs, who need to be confident enough to assure their patients. When asked to comment on their perception of the benefits of discharge to primary care, oncologists highlighted a lesser workload as the major benefit. All oncologists agreed that taking care of non–cancer-related health problems in primary care would enable cancer specialists to focus more on follow-up care. Notably, all oncologists indicated that the most important prerequisite to provide follow-up care is appropriate training of GPs or having a specialist at the primary care level and an improved oncology infrastructure.
Discussion
The critical role of GPs in cancer screening and early detection is well established, and is now increasingly recognized in the follow-up care of cancer survivors in the Western world[3]. With the growing burden of cancer in India, the demand for oncology services is increasing, whereas a shortage of oncologists looms [10]. In this context, primary care could play a significant role in the coordination, comprehensiveness,and continuity of cancer care [22], at the same time decreasing unnecessary health care expenditures [23]. The NPCDCS is now envisioning redesigning the cancer care services by transferring a few care components from oncology services to primary care. However, to date, little information has been gathered on the optimal role of primary care during the followup phase. The present study was designed to elicit and analyze the perspectives of oncologists, primary care physicians, and patients with regard to primary care's possible role in managing cancer follow-up care.
In Odisha, the posttreatment cancer follow-up care is currently highly specialized and oncologist driven. It usually entails repeated visits by the patient to the oncologist to examine the progress and early recognition of recurrences [16]. In our study, oncologists indicated relatively low confidence in GPs' competence in managing cancer-related problems. These uncertainties were reflected in their practice of non-counterreferral of patients to primary care and relatively low comfort in delegating the follow-up care responsibility to GPs. Further,they expressed concerns with the proposed policy of the NPCDCS to entrust some components of cancer care to GPs,and identified individual-level and system-level constraints.All oncologists agreed that taking care of non–cancer-related health problems in primary care would enable cancer specialists to focus more on follow-up care. The general suggestion was the GP's roles with regard to cancer care should be limited to problems not related to cancer and should not include follow-up. The oncologists' reticence to refer patients to primary health care professionals suggests that they view themselves as the custodian of cancer care, thus reflecting the prevailing territorial nature of oncology [24–27].
The common practice among patients was to consult oncologists throughout their cancer care trajectory, not recognizing what role their GP could play. Patients feared recurrence, especially during the early phase after completing treatment, and sought frequent oncologist consultations.Research suggests that continuity of care (seeing the same person) is of utmost importance for cancer patients [28, 29].This partly explains the inclinations of our patients to consult oncologists for follow-up. Patients expressed the desire to maintain contact with their primary care providers for noncancer conditions and short-term health care needs. Some wished their primary care providers to be involved in providing supportive care [30, 31]. At the same time, they want oncologists to provide care for treatment-related side effects,surveillance for recurrence, and coordination of care. These findings indicate the need to clarify the relative roles of GPs and oncologists in cancer care and to better understand each actor's expectations [32, 33].
GPs were more comfortable with continuing their routine health care provider role, and assumed no responsibility toward dealing with cancer patients. These findings are in contrast with reports from Western countries [34]. The findings imply that GPs have grown overly comfortable with their ways of general practice and are not interested in embarking on a newer domain. Such reluctance to treat even noncancer ailments of cancer patients and reservations to be a part of the follow-up care also indicate their lesser familiarity with cancer therapy [35, 36]. It is not surprising that GPs assumed no responsibility for cancer care as they may not be cognizant of various specific options in which they could be involved to improve the lives of their cancer patients [37, 38]. In their everyday work, GPs are used to providing care in a reactive way and they classify their patients into 'normal' and 'exotic'ones. Since GPs label cancer patients as 'exotic,' they expect these patients to consult oncologists for all their health problems. This also reflects the prevailing powerful and intractable image of cancer among GPs [39].
We found that clinicians and patients value clinical reasons for follow-up more highly than supportive reasons, with 'early detection of recurrence' as the top priority. This is expected as in the period immediately after the end of treatment, there may be a high risk of recurrence; hence, follow-up programs in India are primarily focused on detecting recurrence.Furthermore, cancer experts were particularly concerned that transfer of care to the GP would result in the loss of patient care continuity. Understandably, the delivery of follow-up care remains a priority for them [40].
Research has demonstrated that management of health screening and chronic illness care after cancer is improved when patients are seen by both cancer specialists and primary care providers, suggesting that an ongoing primary care relationship is important throughout cancer care [41–43]. Some work suggests that patients seeing both their oncology team and their primary care physicians obtain the greatest benefit in delivery of preventive services [44]. Further research is needed to define the components of care provided by different specialties to cancer patients and to seek ways to support the collaboration of multiple professionals involved toward designing appropriate and acceptable models of care shared between GPs and oncologists.
Our study unveils a few major issues underlying primary care's involvement in follow-up care. The practical logic of the GP's work is at odds with catering to the needs of cancer patients, who are perceived as 'exotic' patients. Since cancer patients are not perceived as a part of a GP's domain of work,it can be questioned whether GPs are ready to fulfill a pivotal role in cancer follow-up care as envisaged by the national program. Further, patients and oncologists were inclined to support GP-led routine care for noncancer ailments, but were less positive about GP-led follow-up. Cancer patients enter an intense world of specialized care, including surgery, chemotherapy, and/or radiation therapy, to treat and manage their disease [41]. Although other chronic illness care and preventive health recommendations persist throughout and after cancer treatment, our study reveals both patients and primary care providers perceive that they should not be in contact with one another after a cancer diagnosis [39]. The territorial issue looms large and may act as a deterrent in the mainstreaming of follow-up care into the routine primary medical care initiative of the national and state governments. An established and continuous specialist-generalist relationship serves an important therapeutic function in follow-up care [42]. However, our study reveals that generalists and oncologists are dissociated.Before any intervention, eliciting acceptance of the GPs by the oncologist fraternity and establishing a system of clinical communication between treating oncologists and GPs appear critical.
Cancer experts and GPs both agree that primary care expertise in cancer care is currently insufficient and thus a distinct disadvantage of follow-up in this setting. Notably, all indicated that the most important resource to provide a quality follow-up service is appropriate training or having a specialist at the primary care level. At the same time, the role of GPs in providing psychosocial support and emotional care could be explored as our results show patients to be more receptive to this idea.The long-standing GP-patient relationship puts GPs in a strategic position to provide emotional support [45]. Thus, providing GPs with appropriate training, customized guidelines for referral to oncologists, and rapid access to follow-up by hospital specialists could be considered. Nevertheless, maintaining a balance can be difficult in view of the prevailing climate of cancer care delivery.
Strengths and limitations
This is the first study to explore the multiple perspectives on primary care involvement in follow-up care. Despite the limited sample size, these perspectives drawn from a diverse group of GPs and oncologists through semistructured interviews provide considerable latitude for expression of individual perspectives. The purposive sample of patients and the small sample size make it difficult to generalize the findings.However, we contend that the results are hypothesis generating. Drawing on our qualitative data, future research should explore the barriers to and potential facilitators for follow-up care in a large sample.
Conclusion
Our study reveals a prominent disconnect between primary care and cancer follow-up care in Odisha. GP competence in delivering appropriate care, lack of communication between oncologists and GPs, and the limited resources of primary care facilities were viewed as the most significant challenges.Further, the conventional role of the GP as the gatekeeper and the demand-driven service delivery approach pose additional barriers. Future research should attempt to examine if and how this can be solved within the current organization of primary care practice.
Acknowledgments
The authors thank the primary care physicians, oncologists,and patients who participated in the research study and provided valuable insights.
Conflict of interest
The authors declare no conflict of interest. The authors alone are responsible for the content and writing of the paper.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
1. Ferlay J, Steliarova-Foucher E, Lortet-Tieulent J, Rosso S, Coebergh JW, Comber H, et al. Cancer incidence and mortality patterns in Europe: estimates for 40 countries in 2012. Eur J Cancer 2013;49:1374–403.
2. Verdecchia A, Guzzinati S, Francisci S, De Angelis R, Bray F,Allemani C, et al. Survival trends in European cancer patients diagnosed from 1988 to 1999. Eur J Cancer 2009;45:1042–66.
3. Burstein HJ, Winer EP. Primary care: primary care for survivors of breast cancer. N Engl J Med 2000;343:1086–94.
4. Grunfeld E, Fitzpatrick R, Mant D, Yudkin P, Adewuyi-Dalton R,Stewart J. Comparison of breast cancer patient satisfaction with follow-up in primary care versus specialist care: results from a randomized controlled trial. Br J Gen Pract 1999;49:705–10.
5. Patel V, Chatterji S, Chisholm D, Ebrahim S, Gopalakrishna G,Mathers C, et al. Chronic diseases and injuries in India. Lancet 2011;377:413–28.
6. Ramnath T, Nandakumar A. Estimating the burden of cancer.Natl Med J India 2011;24:69–71.
7. National Programme for Prevention and Control of Cancer, Diabetes, Cardiovascular Diseases and Stroke (NPCDCS) approved.Press Information Bureau, Government of India. http://www.pib.nic.in/newsite/erelease.aspx?relid=63087 (accessed July 4, 2015).
8. Government to expand NPCDCS to cover all districts in India.eHospice. http://www.ehospice.com/india/ArticlesList/GovernmentofIndiacallsformajorscalingupoftheresponsetononcommunicablediseases040713075119/tabid/5917/Article Id/4015/language/en-GB/View.aspx (accessed April 4, 2015).
9. Reddy KS. Health assurance: giving shape to a slogan. Curr Med Res Pract 2015;5(1):1–9.
10. Goss PE, Strasser-Weippl K, Lee-Bychkovsky BL, Fan L, Li J,Chavarri-Guerra Y, et al. Challenges to effective cancer control in China, India, and Russia. Lancet Oncol 2014;15(5):489–538.
11. Grunfeld E, Mant D, Yudkin P, Adewuyi-Dalton R, Cole D,Stewart J, et al. Routine follow-up of breast cancer in primary care: randomized trial. Br Med J 1996;313:665–9.
12. Lydon A, Beaver K, Newbery C, Wray J. Routine follow-up after treatment for ovarian cancer in the United Kingdom (UK): patient and health professional views. Eur J Oncol Nurs 2009;13:336–43.
13. Del Giudice ME, Grunfeld E, Harvey BJ, Piliotis E, Verma S.Primary care physicians' views of routine follow-up care of cancer survivors. J Clin Oncol 2009;27:3338–45.
14. Greimel E, Lahousen M, Dorfer M, Lambauer M, Lang U.Patients' view of routine follow-up after gynecological cancer treatment. Eur J Obstet Gynecol Reprod Biol 2011;159:180–3.
15. Kelly S. Qualitative interviewing techniques and styles. In:Bourgeault I, Dingwall R, de Vries R, editors. The SAGE handbook of qualitative methods in health research. Los Angeles:SAGE; 2010. p. 307.
16. Pati S, Chauhan AS, Nayak S, Hussain MA, Nayak S. Treatment pathways, experiences and expectations of women with gynecological cancer in Odisha: a qualitative inquiry. Int J Behav Med 2014:21(Suppl 1):S149.
17. Pati S, Hussain MA, Chauhan AS, Mallick D, Nayak S.Patient navigation pathway and barriers to care seeking in cancer in India: a qualitative inquiry. Cancer Epidemiol 2013;37(6):973–8.
18. Khan NF, Evans J, Rose PW. A qualitative study of unmet needs and interactions with primary care among cancer survivors. Br J Cancer 2011;105:S46–51.
19. Hewitt M, Bamundo A, Day R, Harvey C. Perspectives on posttreatment cancer care: qualitative research with survivors, nurses,and physicians. J Clin Oncol 2007;25:2270–3.
20. Bradley E, Pitts M, Redman C, Calvert E, Howells R, Wafai C.What are the factors associated with the follow-up preferences of women in long-term remission from gynecological cancer?J Obstet Gynaecol 2000;20:408–11.
21. Holstein JA, Gubrium JF. The constructionist analytics of interpretive practice. In: Denzin NK, Lincoln YS, editors. The SAGE handbook of qualitative research. 4th ed. Thousand Oaks, California: SAGE; 2011. pp. 341–59.
22. Stille CJ, Jerant A, Bell D, Meltzer D, Elmore J. Coordinating care across diseases, settings, and clinicians: a key role for the generalist in practice. Ann Intern Med 2005;142:700–8.
23. Grunfeld E, Gray A, Mant D, Yudkin P, Adewuyi-Dalton R,Coyle D, et al. Follow-up of breast cancer in primary care versus specialist care: results of an economic evaluation. Br J Cancer 1999;79:1227–33.
24. Mol A. The logic of care: health and the problem of patient choice. London: Routledge; 2008.
25. Earle CC, Grunfeld E, Coyle D, Cripps MC, Stern HS. Cancer physicians 'attitudes toward colorectal cancer follow-up. Ann Oncol 2003;14:400–5.
26. Watson E, Sugden E, Rose P. Views of primary care physicians and oncologists on cancer follow-up initiatives in primary care:an online survey. J Cancer Surviv 2010;4:159–66.
27. Lewis R, Neal R, Hendry M, France B, Williams N, Russell D, et al. Patients' and healthcare professionals' views of cancer followup: systematic review. Br J Gen Pract 2009;59:e248–59.
28. Cox K, Wilson E, Heath L, Collier J, Jones L, Johnston I. Preferences for follow-up after treatment for lung cancer. Cancer Nurs 2006;29:176–87.
29. Brennan M, Butow P, Spillane A, Marven M, Boyle F. Follow up after breast cancer. Views of Australian women. Aust Fam Physician 2011;40:311–6.
30. Miedema B, MacDonald I, Tatemichi S. Cancer follow-up care.Patients' perspectives. Can Fam Physician 2003;49:890–5.
31. Kendall M, Boyd K, Campbell C, Cormie P, Fife S, Thomas K,et al. How do people with cancer wish to be cared for in primary care? Serial discussion groups of patients and carers. Fam Pract 2006;23:644–50.
32. Bulsara C, Ward AM, Joske D. Patient perceptions of the GP role in cancer management. Aust Fam Physician 2005;34:299–300,302.
33. Pennery E, Mallet J. A preliminary study of patients' perceptions of routine follow-up after treatment for breast cancer. Eur J Oncol Nurs 2000;4:138–45.
34. Sisler JJ, Brown JB, Stewart M. Family physicians' roles in cancer care. Survey of patients on a provincial cancer registry. Can Fam Physician 2004;50:889–96.
35. Del Giudice ME, Grunfeld E, Harvey BJ, Piliotis E, Verma S.Primary care physicians' views of routine follow-up care of cancer survivors. J ClinOncol 2009;27:3338–45.
36. Nissen M, Beran M, Lee M, Mehta S, Pine D, Swenson K. Views of primary care providers on follow-up care of cancer patients.Fam Med 2007;39:477–82.
37. Johnson CE, Lizama N, Garg N, Ghosh M, Emery J, Saunders C. Australian general practitioners' preferences for managing the care of people diagnosed with cancer. Asia Pac J Clin Oncol.2014;10(2):e90–8.
38. Worster A, Bass MJ, Wood ML. Willingness to follow breast cancer. Survey of family physicians. Can Fam Physician 1996;42:263–8.
39. Anvik T, Holtedahl K, Mikalsen H. "When patients have cancer,they stop seeing me" – the role of the general practitioner in early follow-up of patients with cancer – a qualitative study. BMC Fam Pract 2006;7:19.
40. Grunfeld E, Mant D, Vessey MP, Fitzpatrick R. Specialist and general practice views on routine follow-up of breast cancer patients in general practice. Fam Pract 1995;12:60–5.
41. Hewitt M, Greenfield S, Stovall E, editors. From cancer patient to cancer survivor: lost in transition.Washington, DC: National Academies Press, 2006.
42. Hall S, Samuel L, Murchie P. Toward shared care for people with cancer: developing the model with patients and GPs. Fam Pract 2011;28:554–64.
43. Earle CC, Neville BA. Under use of necessary care among cancer survivors. Cancer 2004;101:1712–9.
44. Holtedahl K, Norum J, Anvik T, Richardsen E. Do cancer patients benefit from short-term contact with a general practitioner following cancer treatment? A randomised, controlled study. Support Care Cancer 2005;13:949–56.
45. Pascoe SW, Neal RD, Allgar VL, Selbyd PJ, Wright EP. Psychosocial care for cancer patients in primary care – recognition of opportunities for cancer care. Fam Pract 2004;21(4):437–42.
Sanghamitra Pati Additional Professor, Indian Institute of Public Health Bhubaneswar, Public Health Foundation of India, 2nd and 3rd Floor, JSS Software Technology Park, E1/1, Infocity Road, Patia,Bhubaneswar 751024, Odisha,India
E-mail: sanghamitra.pati@iiphb.org, drsanghamitra12@gmail.com
13 August 2015;
Accepted 11 September 2015
 Family Medicine and Community Health2015年3期
Family Medicine and Community Health2015年3期
- Family Medicine and Community Health的其它文章
- The innovations in China's primary health care reform: Development and characteristics of the community health services in Hangzhou
- Primary health care, a concept to be fully understood and implemented in current China's health care reform
- Survival in men older than 75 years with low- and intermediate-grade prostate cancer managed with watchful waiting with active surveillance
- Primary care clinicians' strategies to overcome f nancial barriers to specialty health care for uninsured patients
- Stool DNA-based versus colonoscopy-based colorectal cancer screening: Patient perceptions and preferences
- Overview