
Primary care clinicians' strategies to overcome f nancial barriers to specialty health care for uninsured patients
2015-12-06 09:59:28JamesWernerKittyCorbett
James J. Werner, Kitty K. Corbett
1. Department of Family Medicine and Community Health,Mandel School of Applied Social Sciences, Case Western Reserve University, 11000 Cedar Avenue,Suite 402, Cleveland, OH 44106,USA
2. School of Public Health and Health Systems, University of Waterloo, 200 University Avenue West, Waterloo, Ontario, N2L 3G1, Canada
Primary care clinicians' strategies to overcome f nancial barriers to specialty health care for uninsured patients
James J. Werner1, Kitty K. Corbett2
1. Department of Family Medicine and Community Health,Mandel School of Applied Social Sciences, Case Western Reserve University, 11000 Cedar Avenue,Suite 402, Cleveland, OH 44106,USA
2. School of Public Health and Health Systems, University of Waterloo, 200 University Avenue West, Waterloo, Ontario, N2L 3G1, Canada
Objective:This study describes strategies used by federally qualified health centers (FQHCs)to assist medically uninsured patients in obtaining specialty health care services.
Methods:Qualitative methods were used to study strategies for obtaining specialty health care for uninsured patients. Data were gathered from 10 primary care clinicians at three FQHC clinics by means of 10 semistructured interviews, 23 brief interviews, and 45 h of direct observations. We captured additional data by studying cases of referred uninsured patients.
Results:The following six strategies were identified: (1) quid pro quo – a specialist accepting the clinic's medically uninsured patients was rewarded with referrals of the clinic's insured patients; (2) over referral – clinicians referred insured patients whose needs could have been met at the FQHC; (3) brief hospitalization – when a specialist could not be obtained, high-risk patients were briefly hospitalized; (4) case building – diagnostic tests were conducted at the FQHC to justify a referral; (5) direct communication – communication between clinicians and specialists was necessary when requesting a referral; (6) specialty clinics – in return for conducting a specialty clinic at the FQHC, the specialist received all referrals of insured patients.
Conclusion:Uninsured FQHC patients encountered difficulties accessing specialty health care, and in response, clinicians developed a range of innovative strategies.
Health services accessibility; barriers to health care; medically uninsured; health care inequities; access to specialty care, qualitative methods
Introduction
The Patient Protection and Affordable Care Act of 2010 improved access to health care in the United States, yet more than 38 million Americans remained medically uninsured in 2015 [1]. The lowest rates of health insurance coverage are among Hispanics, African Americans, and the poor, who often face disparities in health outcomes. Although primary care services are available to uninsured residents on a sliding scale at more than 1200 federally qualified health centers (FQHCs) in the United States [2], low-cost specialty services are often difficult to obtain. Although 25% of visits to primary care clinicians at community health centers result in the need for a specialty referral [3], many struggle to obtain specialty access for their patients [4, 5]. Community health centers and free clinics are often not affiliated with hospitals and have limited access to specialist physicians, resulting in a gaping hole in the health care safety net [6–9].
Uninsured patients have greater difficulty obtaining access to off-site specialty services and diagnostic testing than patients with Medicaid, Medicare, or private insurance [3]. FQHCs that are integrated into larger health care systems or that have developed programs for specialty access can more effectively obtain specialty care for their patients, but FQHCs in low population density areas often do not have access to these resources [4, 10].Inequitable access to specialty health care is a pressing problem for the millions of Americans who are medically uninsured.
The tenets of primary care emphasize the importance of coordinating specialty services for patients [11], but without ready access to such services, providers of medically uninsured patients may be called on to advocate for access on behalf of patients. For uninsured patients in need of specialty care, access may be precariously dependent on the effectiveness of their primary care clinician to influence local specialists through advocacy, negotiation, and persuasion. In the absence of training in advocacy skills, which are seldom taught in medical schools or residency programs, many primary care clinicians devise their own strategies [12–14].
The present study was undertaken to identify and describe strategies and techniques used by FQHC primary care clinicians to assist low-income, medically uninsured patients in gaining access to specialty health care services.
Methods
Qualitative research methods were used to study primary care clinicians' methods for meeting the specialty health care needs of uninsured patients at an FQHC in Colorado from 2000 to 2002. The FQHC had eight community, migrant,and teen health clinics that served 27,170 patients in a fivecounty area. Three FQHC community clinics located in different communities served as data collection sites. Profiles of the communities in which the participating FQHC clinics were located are provided in Table 1.
This largely inductive study was designed to discover and describe the types of strategies used by the FQHC clinicians to improve specialty access for medically uninsured patients.Cross-sectional data were gathered from 10 primary care clinicians working in the clinics by means of the following methods: 10 semistructured interviews about accessing specialty services for uninsured patients, 23 brief interviews with clinicians following patient visits in which specialty access was discussed, and 45 h of observations of clinicians' interactions with uninsured patients in need of specialty care and clinicians' activities to obtain access to specialists.
The semistructured interviews were designed to enable interviewees to share their perspectives and to elicit their experiences. The interviews featured open questions that were developed a priori and shaped by prior data analysis and interpretation activities, which were reflexively conducted concurrently with data collection. In each interview, additional open questions,prompts, probes, and clarifications were requested by the interviewer to explore the information shared.
Additionally, we captured prospective data by following, at each clinic, a case for which a primary care clinician arranged for a specialist to provide health care for an uninsured patient.Cases were followed from the time at which specialty carewas first recognized as necessary until 3 months after the patient's initial visit with the specialist. For each case, the primary care clinician was interviewed three times (initial interview, follow-up interview at 4 weeks, and final interview after determination), and each specialist was interviewed once in a semistructured interview. Interviews were audio-recorded and transcribed. The research study was approved by the Colorado Multiple Institutional Review Board. Fig. 1 illustrates the relationships between the data collection and analytic activities.

Table 1. Demographic profiles of participating federally qualified health center clinic locations.
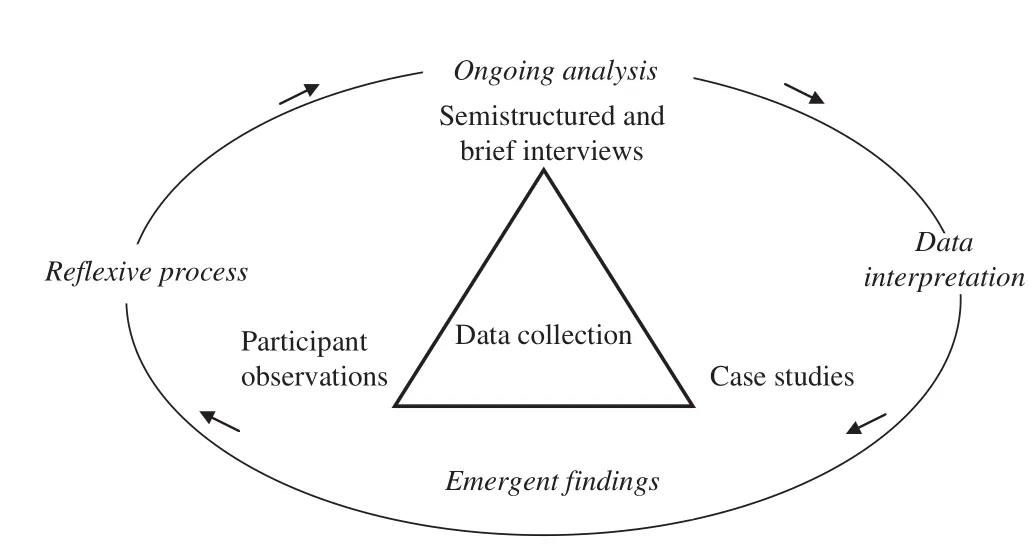
Fig. 1. Relationships between data collection, analysis, and interpretation.
Data consisted of interview transcripts and observational field notes. The analysis was conceptually based in research questions about access to specialty health care but was open to new interpretations. The data were first aggregated into common categories to identify and categorize the information.This coding procedure did not include a priori codes; rather the codes, patterns, and themes emerged from the data [18] in order to minimize assumptions and to prevent force-fitting the data into preconceived categories. Each transcript was coded three to five times over an 18-month period to prevent premature closure and incomplete analysis. Transcripts were coded by the first author and reviewed by the second author to check for consistency of application, and coding disagreements were resolved through discussion. With use of the analytic software application ATLAS.ti, commonly coded quotations were grouped together and examined for consistency and fidelity to code the definitions, and misplaced quotations were recoded.At a higher level of inference, patterns among the coded data were identified in order to reduce the data into smaller numbers of analytic units [19]. Finally, patterns were further condensed into themes that represented the core of the study's findings.
Results
Securing specialty care on behalf of low-income uninsured patients was universally recognized to be a challenge by the participating providers. Six strategies for accessing specialty care were identified, as described below. Summaries of the strategies and examples of quotations are provided in Table 2.
Quid pro quo
The FQHC clinicians initiated quid pro quo reciprocal exchange arrangements to obtain access for uninsured patients. The essence of the exchange was that if a specialist agreed to accept the FQHC clinic's medically uninsured patients, he or she would be rewarded with referrals of the clinic's insured patients. Some pacts were negotiated in detail,whereas others were tacitly acknowledged. Participating specialists believed these deals to be in their best interest because they could receive significant numbers of referrals of insured patients. This strategy was attractive for specialists who were new in a community and who sought to build their referral base of insured patients.
Over referral
The services of local specialists were so highly valued that FQHC clinicians occasionally referred insured patients whose needs could have been met at the FQHC. The intent was to build goodwill by enabling specialists to benefit financially from referred cases of insured patients. The hope was that such action would cause specialists to become more receptive to accepting uninsured patients.
Brief hospitalization
Hospitalization was generally regarded as the surest route to specialty care. In cases where access to a specialist had not been obtained for an uninsured patient with a high-risk health condition, FQHC clinicians sometimes admitted patients to local hospitals for a few hours. Once the patient had been admitted to the hospital, an appropriate specialist was legally required to provide services. Emergency departments were also used in this way, but if emergency department staff believed that the condition was not emergent, the patient would often be sent home.
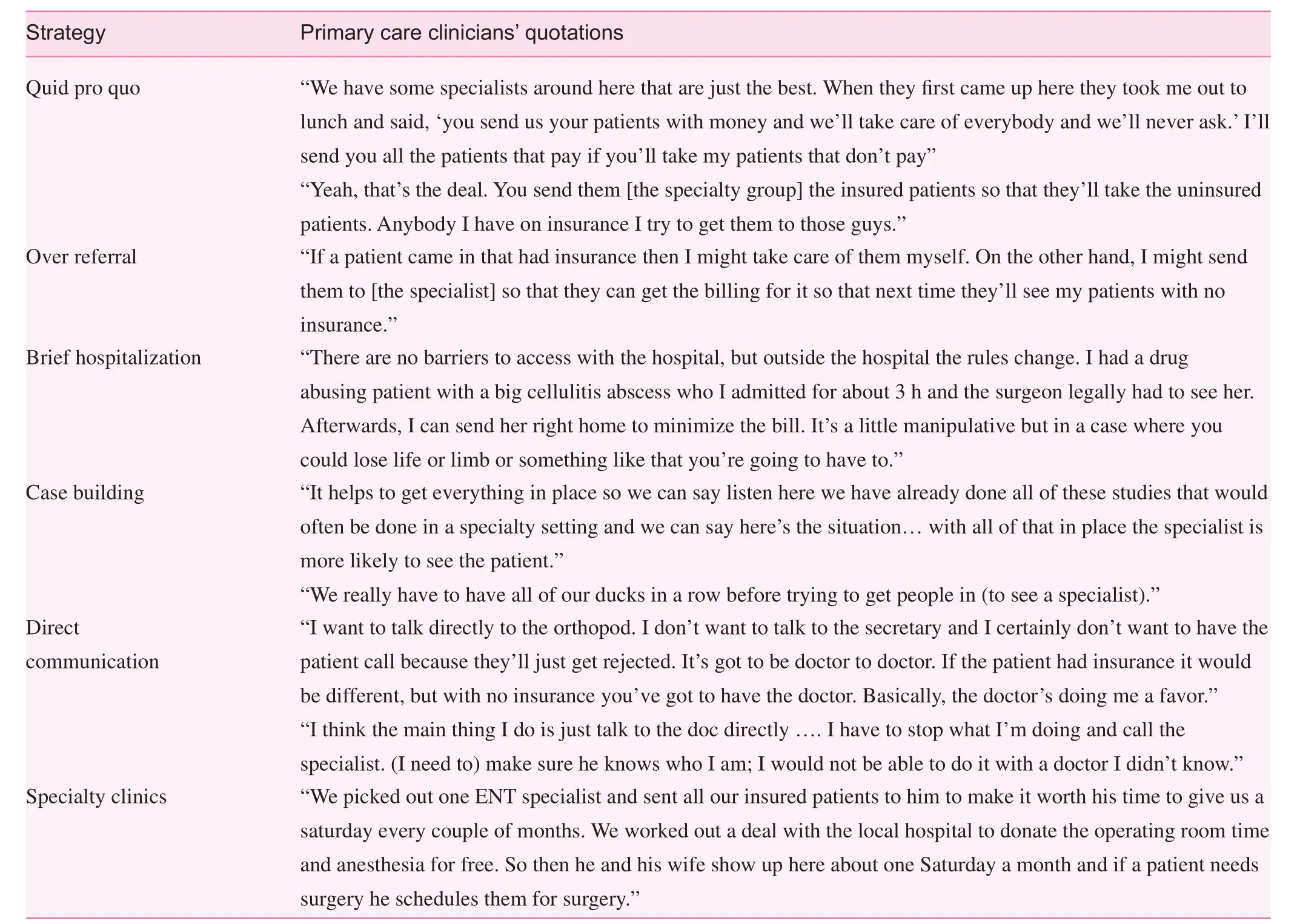
Table 2. Federally qualified health center strategies to obtain specialty access and exemplary quotations.
Case building
Making a strong case for a patient's need for a referral appointment helped to break through barriers that might have otherwise prevented access. To build a case, FQHC clinicians found it beneficial to conduct appropriate diagnostic tests at the FQHC. By prequalifying the patient for a referral and by minimizing the amount of work-up required by the specialist, the FQHC minimized the specialist's financial risk and increased the likelihood that access could be obtained.
Direct communication
The FQHC clinicians stressed the importance of direct communication between themselves and a specialist when requesting access for an uninsured patient. Uninsured patients who contacted specialists' offices to make appointments were often rejected by receptionists who screened them out because of the risk of not receiving payment for services. Direct communication between physicians was reported to be an effective method for obtaining access; however, mid-level providers and medical assistants experienced less success when interfacing with specialist physicians.
Specialty clinics
One FQHC clinic worked with a local specialist to develop a specialty clinic on one Saturday morning each month. On the day of the clinic, a prequalified group of uninsured patients came to the FQHC for evaluation and treatment by the specialist. Treatment was provided at no cost to the patient or the FQHC. The specialty clinic approach was combined with the quid pro quo strategy. In return for conducting the specialty clinics, the specialist received all of the clinic's referrals of insured patients.
Clinicians displayed differing levels of skill in developing and implementing strategies to improve specialty access. The medical director of the FQHC used the negotiation strategies(quid pro quo, direct communication, specialty clinics) and brief hospitalization more frequently than providers with less experience, and indicated that his stature as a leader in the regional medical community made this possible. Less experienced and less assertive physicians, nurse practitioners, and physician assistants were observed to rely more heavily on case building and over referral strategies.
Discussion
In attempts to meet the needs of medically uninsured patients,FQHC primary care clinicians were observed to use six strategies to obtain access to specialty care. The strategies ranged from rewarding cooperative specialists by referring insured patients to them, to briefly hospitalizing patients to force specialists to see them, to persuading specialists through direct interactions.
Organizational models that enable FQHCs to more consistently access specialty services for uninsured patients have been observed and new models have been proposed, although they require resources to support their development and maintenance[4, 6, 20]. Without a clear system through which specialty care can be obtained for uninsured patients, FQHCs in some parts of the United States have developed volunteer specialist referral programs in an attempt to obtain specialty services [21]. These programs recruit specialists to provide services to a specific number of uninsured patients at no cost to the patient, or for a small co-payment [6]. Such programs are limited by the number of volunteer specialists available and their capacity for charity care, even as reduced numbers of specialists engage in the care of vulnerable populations [22]. Despite these obstacles, such programs may be the best option for communities where other solutions do not exist, such as the locations in which the present study was conducted. In these circumstances, knowledge of the strategies reported here may increase the effectiveness of obtaining specialty services for uninsured patients.
It may be useful for FQHCs to maintain an archive of institutional knowledge about specialty access strategies that have proven effective within each community. This information may be especially useful to FQHCs that hire clinicians through loan repayment programs, where clinician turnover is often high. In the clinics that were the focus of this study, two of the three key informant physicians left the FQHC after 3-year loan repayment periods. It will be advantageous for more experienced and assertive clinicians to assist new clinicians with specialty access issues. Experienced clinicians can provide guidance in analyzing the access situation in their community,in identifying leaders in the medical community, in making full use of available resources for uninsured patients, and in developing effective strategies to improve access.
The professional qualities exhibited by FQHC clinicians had a significant bearing on the level of cooperation that could be obtained from specialists. It may be useful for FQHCs to take clinicians' leadership skills into consideration when hiring staff. Further, matching clinicians' skills with the needs of communities may optimize access. In communities with longstanding specialty access problems for uninsured patients, it may be necessary to hire or transfer experienced clinicians in order to improve the access situation as quickly as possible.
Three of the observed strategies (quid pro quo, direct communication, and specialty clinics) required physicians to leverage their individual social capital within their medical communities on behalf of patients. Individual social capital has been defined as the networks of connections between individuals involving trust, social ties, and social position [23, 24].It involves connections with others, and differs from personal leadership skills and experience which may exist in isolation,although they may contribute to individual social capital.Building and leveraging individual social capital on patients'behalf are skill sets that are unlikely to be taught in medical schools and residency programs [25]. Primary care clinicians in training may benefit from better understanding social capital within medical communities and learning the ways that it can be used to increase access and improve health outcomes for medically uninsured patients.
The physicians who participated in this study indicated that their residency programs did not prepare them to deal effectively with the access difficulties they encountered. Many residency programs operate within vertically integrated health care systems in which there is ready access to specialty care.Residents bound for FQHC work may benefit from preparation for the types of access difficulties that are likely to be encountered. Such training may include understanding the necessity of building social capital by becoming a respected and active member of the medical community, appreciating practice financial pressures associated with the care of uninsured patients from the perspective of private specialists, and instruction in strategies for building mutually beneficial relationships with local specialists.
Limitations
The present study had several limitations. The project was conducted at a time when expansion of health insurance coverage through the Patient Protection and Affordable Care Act was not in effect. It is difficult to estimate the impact the legislation would have had on specialty access within the FQHC system that was the venue for this study. In addition, this qualitative descriptive study did not quantify the frequency of use for each of the strategies, and the magnitude of their respective contributions to specialty access is unknown. Finally, although we were reflexive throughout the ethnographic investigation, it is possible that subtle biases could have influenced the study findings.
Conclusion
Medically uninsured patients receiving services at three FQHC clinics encountered difficulties accessing specialty health care,and in response, clinicians developed a range of innovative strategies to secure specialty access within their local communities. These strategies included attempts to directly persuade specialists, setting up quid pro quo referral arrangements, minimizing specialists' financial risk by doing extensive testing at the FQHC, and using hospital regulations to compel specialists to see patients during brief hospital stays. Clinicians' individual social capital was central to three of the strategies, and efforts to train providers to build and use their individual social capital may benefit health care access.
The findings from this investigation reflect the uncertainties faced by medically uninsured patients who fall into the safety net of a health care system that was not designed to provide equal access. Physicians went to great lengths in advocating for access on behalf of their patients, often leveraging their individual social capital to do so. The strategies identified highlight the extraordinary resourcefulness of primary care clinicians in finding ways to overcome system limitations and underscore their commitment to meet patients' needs for specialty health care services.
Conflict of interest
The authors declare no conflict of interest.
Funding
This publication was made possible by the Clinical and Translational Science Collaborative of Cleveland,UL1TR000439 from the National Center for Advancing Translational Sciences component of the National Institutes of Health (NIH) and the NIH Roadmap for Medical Research,by Case Comprehensive Cancer Center Support Grant P30CA43703-23 from the National Cancer Institute of the NIH, and by the Centers for Primary Care Practice-Based Research and Learning from the Agency for Healthcare Research and Quality through grant P30HS021648-03. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the Agency for Healthcare Research and Quality or the NIH.
1. Levy, J. In U.S., uninsured rate drops to 11.9% in first quarter.Available from: www.gallup.com/poll/182348/uninsured-ratedips-first-quarter.aspx. Accessed July 10, 2015.
2. National Association of Community Health Centers. Key health center data by state, 2013: federally-funded health centers only. Available from: www.nachc.com/client/2013%20Key%20 facts%20by%20state%20data.pdf. Accessed January 9, 2015.
3. Cook NL, Hicks LS, O'Malley AJ, Keegan T, Guadagnoli E,Landon BE. Access to specialty care and medical services in community health centers. Health Aff (Millwood) 2007;26(5):1459–68.
4. Neuhausen K, Grumbach K, Bazemore A, Phillips RL. Integrating community health centers into organized delivery systems can improve access to subspecialty care. Health Aff (Millwood)2012;31(8):1708–16.
5. Forrest CB, Shadmi E, Nutting PA, Starfield B. Specialty referral completion among primary care patients: results from the ASPN Referral Study. Ann Fam Med 2007;5(4):361–7.
6. Hall MA. Organizing uninsured safety-net access to specialist physician services. J Health Care Poor Underserved 2013;24(2):741–52.
7. Gusmano MK, Fairbrother G, Park H. Exploring the limits of the safety net: community health centers and care for the uninsured.Health Aff (Millwood) 2002;21(6):188–94.
8. Stanley A, Cantor JC, Guarnaccia P. Holes in the safety net: a case study of access to prescription drugs and specialty care.J Urban Health 2008;85(4):555–71.
9. Felt-Lisk S, McHugh M, Howell E. Monitoring local safetynet providers: do they have adequate capacity? Health Aff(Millwood) 2002;21(5):277–83.
10. Spatz ES, Phipps MS, Wang OJ, Lagarde S, Lucas GI, Curry LA,et al. Expanding the safety net of specialty care for the uninsured:a case study. Health Serv Res 2012;47(1 Pt 2):344–62.
11. Donaldson MS, Yordy KD, Lohr KN, Vanselow NA, editors.Primary care: America's Health in a new era. Washington, DC:National Academy Press; 1994.
12. Earnest MA, Wong SL, Federico SG. Perspective: physician advocacy: what is it and how do we do it? Acad Med 2010;85(1):63–7.
13. Cha SS, Ross JS, Lurie P, Sacajiu G. Description of a researchbased health activism curriculum for medical students. J Gen Intern Med 2006;21(12):1325–8.
14. Gill PJ, Gill HS. Health advocacy training: why are physicians withholding life-saving care? Med Teach 2011;33(8):677–9.
15. Health Resources and Services Administration (HRSA), Community Health Status Indicators Project. Available from: www.communityhealth.hrsa.gov.
16. US Census Bureau, State and county QuickFacts. Available from: http://quickfacts.census.gov.
17. Abel P, editor. Colorado health resource book: insurance, access,and expenditures. Denver: Colorado Coalition for the Medically Underserved; 1988.
18. Crabtree BF, Miller WL. Doing qualitative research. 2nd ed.Thousand Oaks, CA: Sage; 1999.
19. Miles MB, Huberman AM. Qualitative data analysis: an expanded sourcebook. 2nd ed. Thousand Oaks, CA: Sage;1994.
20. Olayiwola JN, Bodenheimer T, Dube K, Willard-Grace R,Grumbach K. Facilitating care integration in community health centers: a conceptual framework and literature review on best practices for integration into the medical neighborhood. San Francisco, CA: UCSF Center for Excellence in Primary Care;2014.
21. Scott HD, Bell J, Geller S, Thomas M. Physicians helping the underserved: the Reach Out program. J Am Med Assoc 2000;283(1):99–104.
22. Cunningham P, May J. Medicaid patients increasingly concentrated among physicians. Track Rep 2006;16:1–5.
23. Yang K. Individual social capital and its measurement in social surveys. Surv Res Methods 2007;1(1):19–27.
24. Putnam R. Bowling alone: the collapse and revival of American community. New York: Simon & Schuster; 2000.
25. Wagner P, Hendrich J, Moseley G, Hudson V. Defining medical professionalism: a qualitative study. Med Educ 2007;41(3):288–94.
James J. Werner Department of Family Medicine and Community Health, Mandel School of Applied Social Sciences, Case Western Reserve University, Cleveland, OH, USA
E-mail: james.werner@case.edu
22 July 2015;
Accepted 15 September 2015
 Family Medicine and Community Health2015年3期
Family Medicine and Community Health2015年3期
- Family Medicine and Community Health的其它文章
- The innovations in China's primary health care reform: Development and characteristics of the community health services in Hangzhou
- Primary health care, a concept to be fully understood and implemented in current China's health care reform
- Survival in men older than 75 years with low- and intermediate-grade prostate cancer managed with watchful waiting with active surveillance
- Disconnect between primary care and cancer follow-up care:An exploratory study from Odisha, India
- Stool DNA-based versus colonoscopy-based colorectal cancer screening: Patient perceptions and preferences
- Overview