
Uptake of prostate cancer screening and associated factors among Chinese men aged 50 or more: a population-based survey
2014-09-26 06:01:00WinnieSoKaiChowChoiWinnieTangPaulLeeAnnShiuSimoneHoHelenChanWendyLamWilliamGogginsCarmenChan
Cancer Biology & Medicine 2014年1期
Winnie K.W.So, Kai Chow Choi, Winnie P.Y.Tang, Paul C.W.Lee, Ann T.Y.Shiu, Simone S.M.Ho, Helen Y.L.Chan,Wendy W.T.Lam, William B.Goggins, Carmen W.H.Chan
1The Nethersole School of Nursing, The Chinese University of Hong Kong, Hong Kong SAR, China; 2Department of Community Medicine, The University of Hong Kong, Hong Kong SAR, China; 3The Jockey Club School of Public Health and Primary Care, The Chinese University of Hong Kong, Hong Kong SAR, China
Introduction
Globally, prostate cancer has been reported to be the second most common cancer and the sixth leading cause of death among men1.Compared with worldwide figures, the incidence of prostate cancer in China is low, estimated in 2008 to be more than 33,000 with the age-standardized incidence and mortality rate of 4.3 and 1.8 per 100,000, respectively.However, the trend is increasing, and it is estimated that by 2020 new cases will number over 49,000 and account for more than 20,000 deaths2.Locally, the incidence of prostate cancer has also been increasing over the past two decades.In 2010, prostate cancer was the third most common cancer and the fifth leading cause of cancer death in males.The Hong Kong Cancer Registry3reported in 2010 that there were 1,492 new cases, the age-standardized incidence rate was 28.1, and the age-standardized death rate was 5.5 per 100,000 of the standard population.
Although the causes of prostate cancer are not yet fully understood, it is believed that advanced age (above 50), a positive family history of prostate cancer and an African-American ethnic background are risk factors4,5.Early detection is commonly effected by serum prostate specific antigen (PSA)screening, digital rectal examination (DRE) and transrectal ultrasound (TRUS).Among these three, PSA was found to be the most accurate single diagnostic tool, and more cost-effective than DRE or a combination of DRE and PSA6,7.The detection rate of DRE also depends on the level of PSA and the experience and technique of the physician.With low levels of PSA, the sensitivity of DRE was low, and its performance in detecting small-volume tumors was also poorer than PSA8.
However, the recommendation in early prostate cancer screening of serum PSA testing remains controversial.Arguments against such screening concern over-diagnosis, over-treatment and its consequent adverse effects9,10.One systematic review and meta-analysis found that the effect of screening on death and overall mortality from prostate cancer was insignificant11.In contrast, a large randomized controlled trial conducted by the European Randomized Study of Screening for Prostate Cancer(ERSPC) reported a 20% reduction in prostate cancer deaths12,and another observational study also found a significant decrease in such mortality13.PSA screening is also associated with an increased diagnosis of early stage prostate cancer and a decrease in advanced stage and distant metastases, and thus with higher survival rates8,11.Nevertheless, the American Cancer Society(ACS) recommends that men who are asymptomatic and have a life expectancy of at least ten years should discuss the matter with their physician and reach an informed decision about prostate cancer screening, with the pros and cons of such screening being fully explained.For men at risk, the optimal age for receiving such information depends on the level of risk—the higher the risk, the younger the age shared and informed decision-making should be initiated5.As the population is generally aging and the general public is more concerned about health, the need for screening is clearly increasing.
The uptake rates for prostate cancer screening among African Americans and Canadians were 36% and 47.5%, respectively14,15.In Chinese populations, the rate is low.In Taiwan, studies have reported the uptake rate to be between 12.4% and 29.4%16,17.Different studies have been conducted to investigate the factors associated with participation in prostate cancer screening.Qualitative studies have found fear of cancer, lack of knowledge, embarrassment and perceived low risk were barriers,while a family history of prostate cancer, urinary symptoms and physician’s recommendations were facilitators18,19.Age,educational attainment, household income, insurance coverage and marital status are common predictive factors14,20,21.Other contributing factors include chronic illness, obesity, medical visits and perceptions of health14,20,21.
Several studies have also investigated the facilitators and barriers in Chinese populations, with similar findings: physician’s recommendations, history of benign prostate hypertrophy,embarrassment, lack of knowledge, being asymptomatic, and financial status all being noted16,17.However, no study has been conducted in Hong Kong to investigate the rate of prostate cancer screening and the associated factors affecting uptake.In addition,even though Hong Kong and Taiwan share the same cultural origins, diverse sub-cultures have developed with the differences in historical backgrounds and geographical positions.Furthermore,there are differences in the social, political and economic systems between the two places22,23, which may cause variations in social norms and health-seeking behavior in their respective populations.It is therefore worth investigating the factors affecting prostate cancer screening in Hong Kong.Thus, the study aimed to investigate the uptake rate of PSA testing among Hong Kong Chinese males aged over 50, and identify the factors associated with the probability of that population undergoing PSA testing.
Materials and methods
This study was conducted in 2007 using a population-based telephone survey.The methodology of the survey was described elsewhere24.In brief, participants of the present study were Hong Kong Chinese residents aged 50 years or above.A structured questionnaire consisted of six sections: demographics, perceived health condition, use of complementary therapy, cancer screening behaviour, perceived susceptibility to cancer and family history of cancer.In the section on complementary therapy, respondents were given a four-point rating scale to indicate how frequently they used it, where 0, never; 1, once only; 2, occasionally; 3,on a regular basis; and the 2005 cancer module of the National Health Interview Survey25was used, in modi fied form, to collect data in the cancer screening behavior section.Ethical approval was obtained from the Survey and Behavioral Research Ethics Committee of the Chinese University of Hong Kong.Verbal consent was obtained from all participants.Telephone numbers were randomly selected from the updated residential directories,which include over 95% of households in Hong Kong, and anonymous interviews were carried out by the telephone survey team of the university’s Centre for Epidemiology and Biostatistics.Data collection went on from 6:30 pm to 10:30 pm only, to minimize over-representation of the non-working population.If there were two or more eligible household members, the member with birthday nearest to the interview date was recruited.To minimize any bias from non-responses, at least three calls were made at different times on the other days before assigning a nonresponse status to a number.
Data were entered and analyzed with SPSS 17.0 (SPSS Inc,Chicago, USA).Descriptive statistics was used to summarize and present the data.Frequencies (percentages) were used to present the results of categorical variables.Stepwise multivariable logistic regression analysis was used to identify factors independently associated with prostate cancer screening behavior, and the factors to be explored are listed in Tables 1 and 2.A binary outcome variable was used to study screening behavior: ‘Have you ever had a prostate-specific antigen (PSA) test?’ (Yes/No).Univariate analyses were first performed on each of thestudied factors to select candidate independent variables for the multivariable analysis.Those factors with a P value <0.25 in the univariate analyses26were selected as candidate variables for stepwise multivariable logistic regression to delineate factorsindependently associated with the screening behavior outcome.The results of significant factors identified were presented with their odds ratio (OR) and 95% confidence intervals (CI).All statistical tests involved were two-tailed and statistical significant level was set at 0.05.
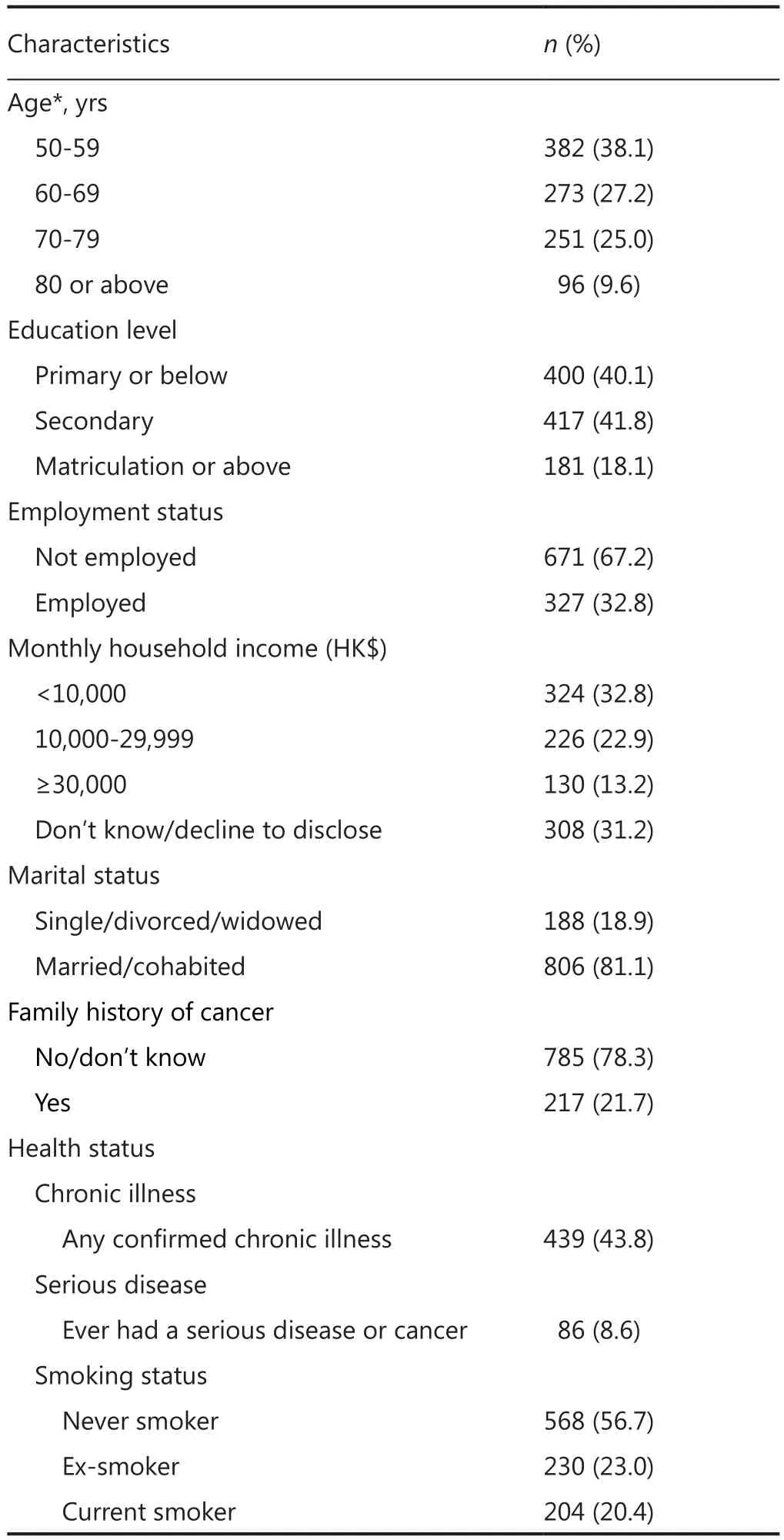
Table 1 Demographic characteristics and health status of the respondents (n=1,002)
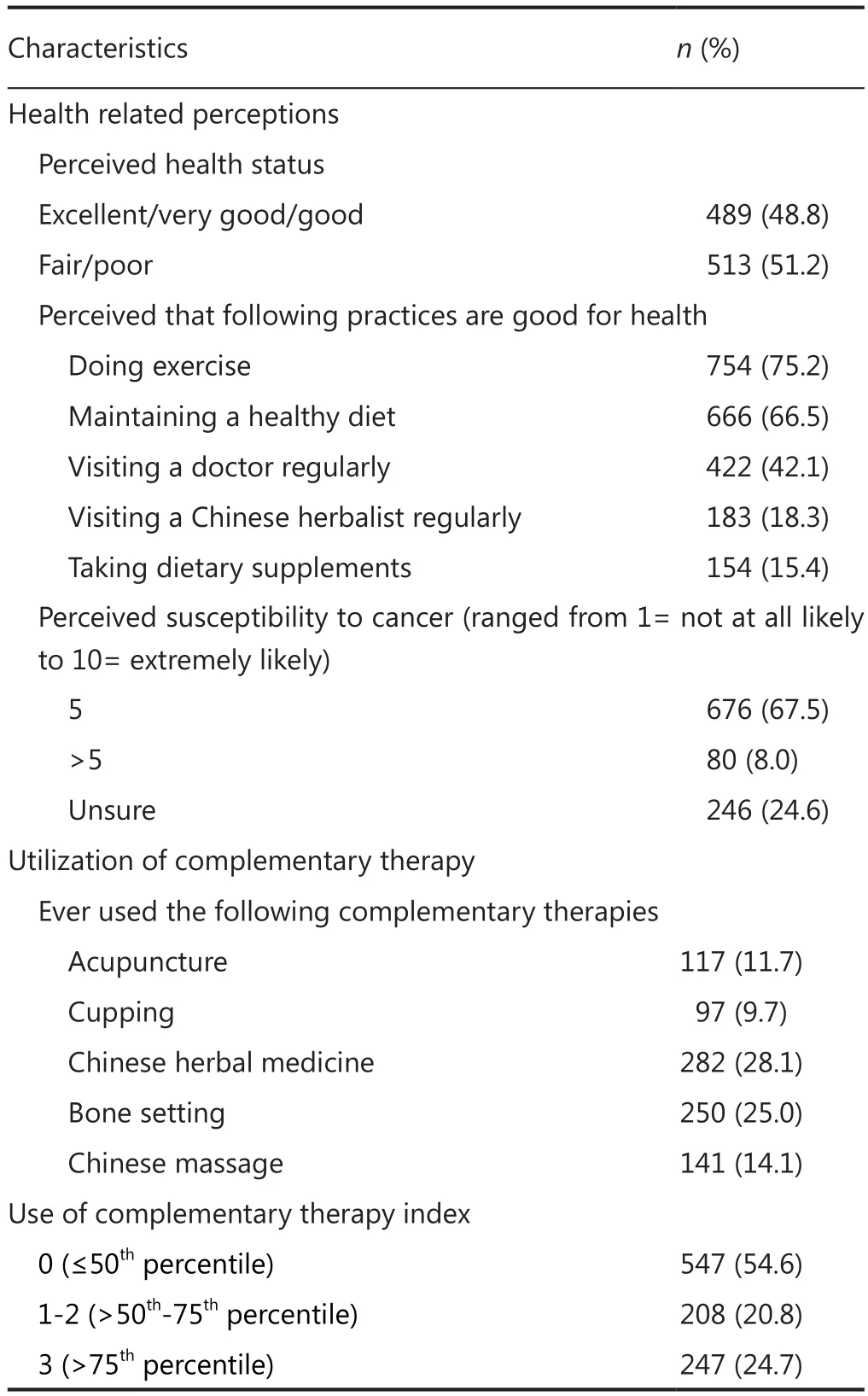
Table 2 Perceived health status and utilization of complementary therapies
Results
A total of 1,002 men aged 50 or above completed the anonymous survey and were included in the study (response rate =67%).The age distribution of the sample collected was reasonably comparable to that of the local population, although the 50-59 age group was somewhat under-represented (footnote to Table 1)27.
Demographic characteristics and health status
The demographic characteristics and health status of the respondents are shown in Table 1.The mean age of the respondents was 64.2±10.2 years and ranged from 50 to 94 years.More than half had received a secondary education or above(60%).The majority were married or cohabiting (81%) and unemployed (67%), with 36% reporting a middle (HK$10,000-29,999, 1US$≈7.8HK$) or high (HK$30,000+) monthly household income, although a considerable proportion (31%)did not know or declined to disclose their income.Less than half had at least one type of chronic illness (44%), and only 9% had ever had cancer or other serious disease.One fifth of the men were current smokers, and 22% had a family history of cancer.
Perceived health status and use of complementary therapies
The respondents’ perceived health status and utilization of complementary therapies are shown in Table 2.Slightly over half reported their health status as fair or poor (51%), and the majority believed that doing exercise (75%) and maintaining a healthy diet (67%) were good for their health.Fewer than half perceived that visiting a doctor regularly was good for the health (42%), and only a small proportion believed that visiting a Chinese herbalist regularly (18%) or taking dietary supplements (15%) were good for the health either.More than two-third (68%) perceived that they were unlikely susceptible to cancer.
Among the five most commonly used complementary therapies in Chinese societies28, it was interesting to note that the usage rates (‘had ever used’) reported by this sample were not high: acupuncture (12%), cupping (10%), herbal medicine(28%), bone setting (25%) and Chinese massage or ‘tuina’(14%).
Prostate cancer screening behavior
Among all respondents, only 10% con firmed that they had ever had a PSA test.The three main reasons for having the most recent PSA test were: (1) regular physical check-ups (39%); (2)prompted by local signs and symptoms (34%) and (3) physician’s recommendation (21%).The three most common reasons cited by respondents for never having had a PSA test were: (1) they did not think it was necessary (44%); (2) they did not know it was available (33%) and (3) they regarded themselves as healthy all along (8%) (Table 3).Only 4% reported that they had been recommended by health professionals for a PSA test.
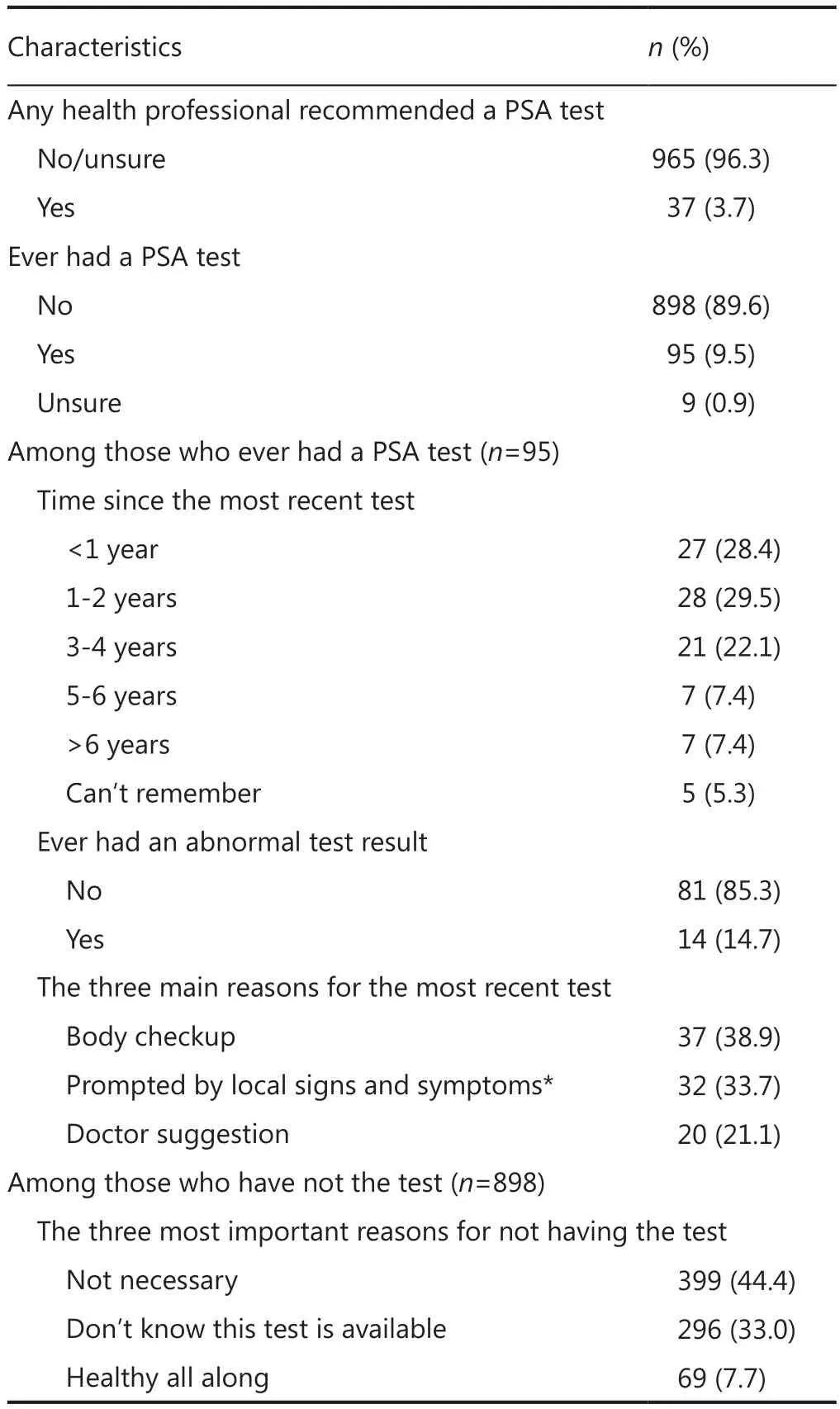
Table 3 Prostate cancer screening behaviour–prostate-specific antigen (PSA) test
Factors associated with having had a PSA test
Table 4 shows the results of factors that were associated with having had a PSA test.Stepwise multivariable logistic regression, with removal and entry criteria set at P>0.1 and P<0.05 respectively, using those factors with P values <0.25 in univariate analysis as candidate independent variables revealed that employment status, use of complementary therapy, visiting a doctor regularly seen as good for health and recommendation from health professional were all significantly associated with ever having had a PSA test (Table 4).Respondents who wereemployed were less likely to have a PSA test [employed vs.unemployed, OR=0.4 (95% CI: 0.2-0.8), P=0.004].Those respondents with most frequent use of complementary therapies were more likely to have a PSA test than those who had never used them [OR=2.1 (1.2-3.6), P=0.006].Perceptions of visiting a doctor as good for health were associated with increased odds of ever having had a PSA test [OR=2.7(1.7-4.4), P<0.001].Finally, and remarkably, recommendations from health professionals had a very strong influence on the screening test [OR=25.9 (11.8-56.7), P<0.001].
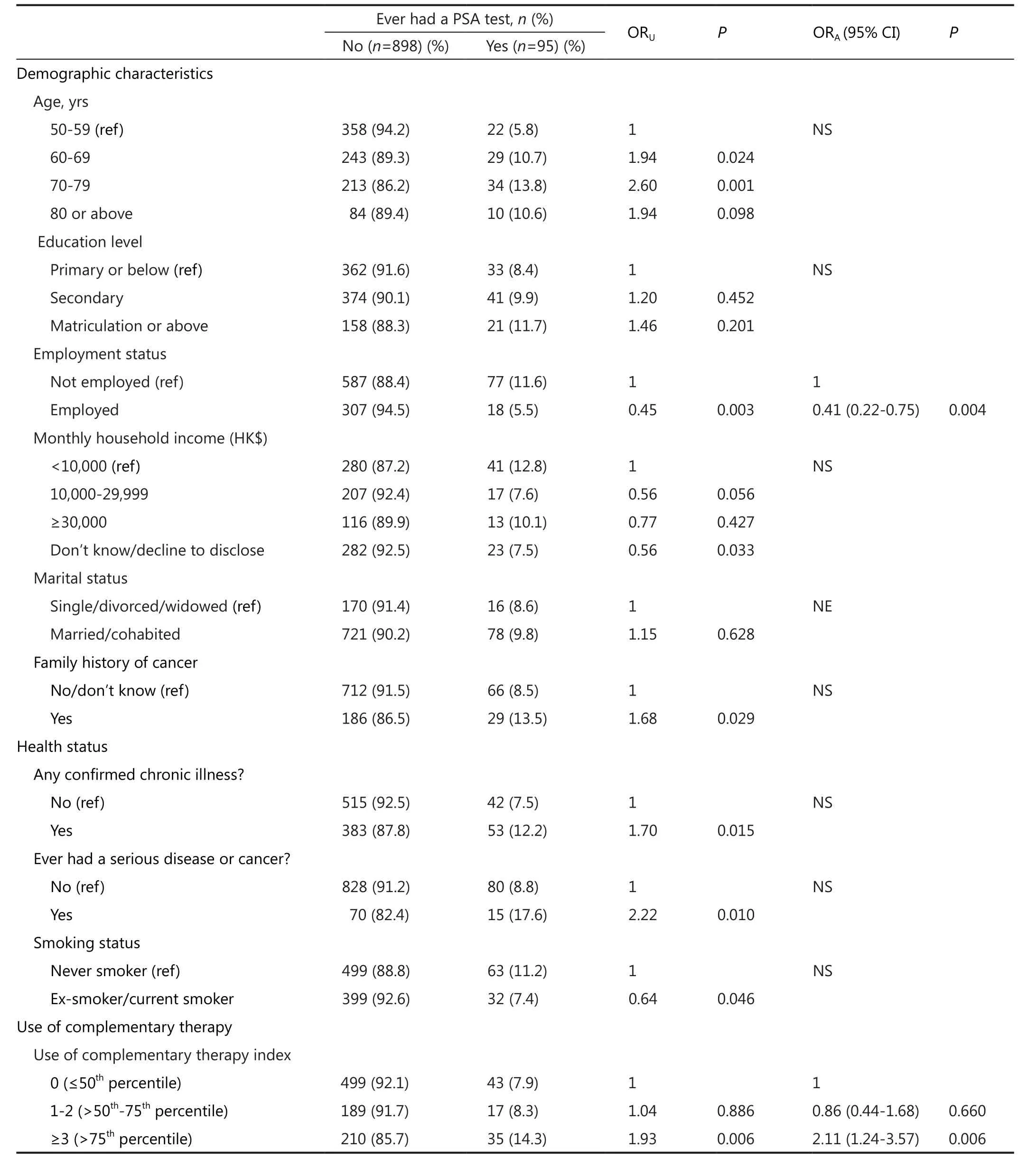
Table 4 Factors associated with ever having had a PSA test
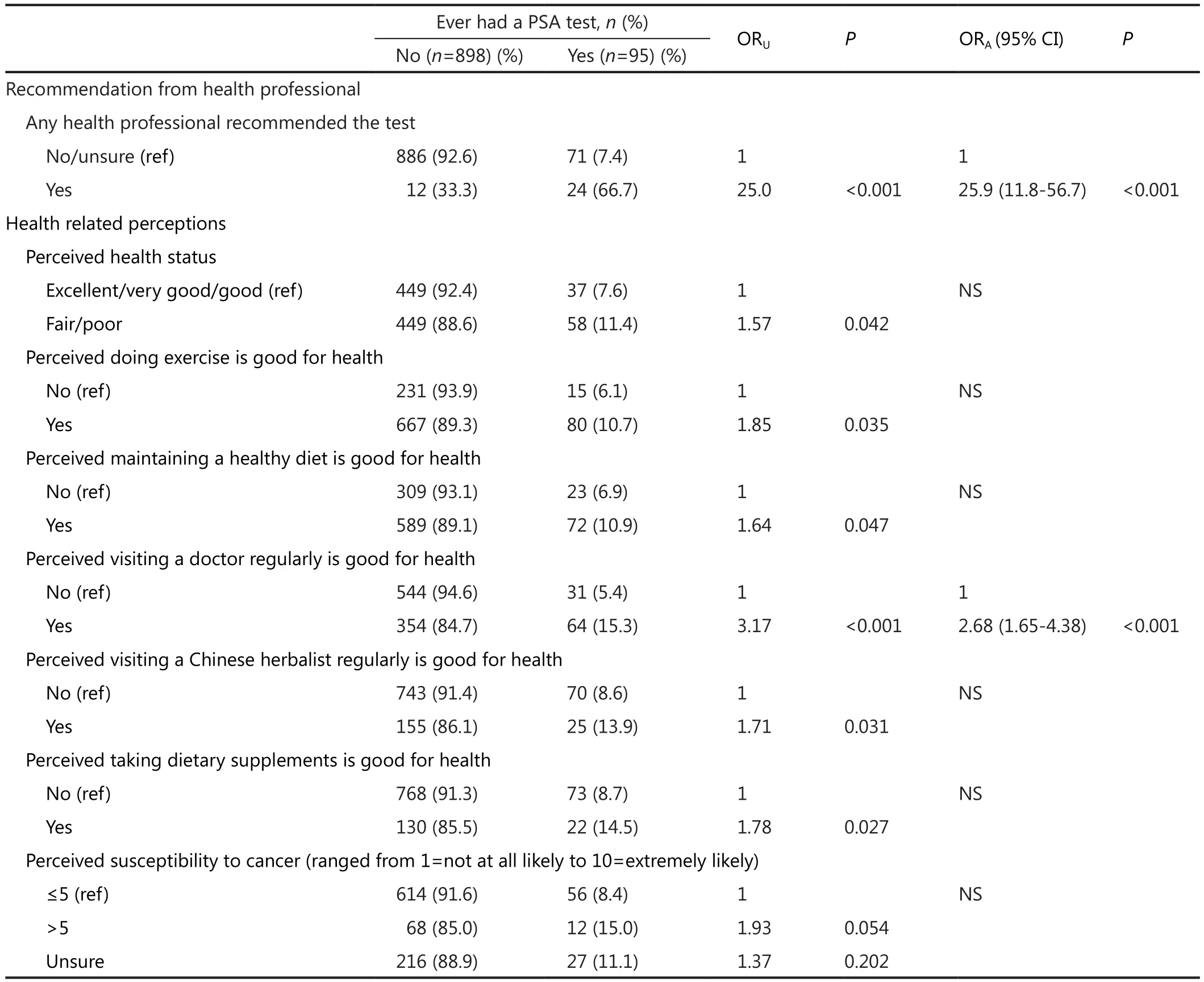
Table 4 (continued)
Discussion
Uptake of PSA testing
The uptake rate of PSA testing was 10%, lower than in other studies conducted in comparable groups17,18.The three main reasons for having the test were ‘regular physical checkups’, ‘presence of unusual signs and symptoms’, and ‘doctor’s recommendation’.On the other hand, respondents had not undergone the test because they perceived the test was ‘not necessary’, they ‘did not know the test was available’ or they considered they were ‘healthy all along’.The findings re flect the respondents lacked knowledge and had misconceptions about prostate cancer and the benefits of screening.Similar results have also been reported by other studies, indicating that a lack of knowledge and faulty perceptions of prostate cancer risk influence males in adopting certain health behavior17,18,29.
Another possible reason may be insufficient health promotion and education of the public—only 3.7% (n=37)of the respondents received recommendations from health professionals for a PSA test.In fact, the Cancer Expert Working Group on Cancer Prevention and Screening30concluded that insufficient scientific evidence was available to recommend whether or not prostate cancer screening in asymptomatic men should be carried out.Men are therefore encouraged to discuss with their doctors the benefits and risks of such screening.However, lack of knowledge about prostate cancer in men and insufficient health promotion of prostate cancer screening may hinder men’s awareness and compliance of the recommendation.
Factors associated with PSA testing
Respondents more likely to have had a PSA test were those who were unemployed, used complementary therapies for health promotion and restoration, perceived visiting a doctor regularly as good for health or had received a recommendation from health professionals.It was interesting to find that unemployed respondents were more likely to take a PSA test.Perhaps employment status may be directly or indirectly related to age.The results of univariate analysis showed that respondents aged 50-59 were less likely to take a PSA test than those aged 60-79, though the result was not significant in multivariate analysis.Further studies are needed to get a clearer picture of the perceptions and attitudes towards having a PSA test among older adults who are or are not employed.
The use of complementary therapy was another associated factor identified in multivariate analysis.In Chinese societies,various complementary therapies are commonly used to promote and restore health, which may be why those who have resorted to such complementary measures are more receptive to undergoing a PSA test.
Regarding regular visits to a doctor as good for health and recommendations from health professionals were two important factors associated with the uptake of PSA testing.In particular, the odds of test uptake were 25.9 times better among participants who had received recommendations from health professionals than among those who had not.Similar results have been produced by other studies conducted with comparable age groups17,24.Health professionals should therefore take up a significant role in health promotion and education to increase awareness of cancer prevention and detection among the male population in Hong Kong.They would also be expected to explain and discuss the potential benefits and risks of PSA testing to help their patients come to a decision.
Limitations
There are several limitations to this study.First, it uses a crosssectional survey design, which makes it difficult to establish the causality and identify the predictors of PSA testing uptake.Second, other factors that may be associated with the uptake,such as a history of benign prostate hypertrophy or a family history of prostate cancer, were not included.Third, recall bias exists in self-report data.Last, but not the least important, data collected from a self-report survey, such as questions about having ever had a PSA test or being recommended by a health professional, were not validated.
Conclusion
This study reported the uptake rate of PSA testing, which was very low, and identified associated factors among older Chinese men.After adjusting for confounding variables, those respondents who were not employed, used complementary therapy, perceived visiting a doctor regularly as good for health and had been recommended by a health professional were found to be more likely to have a PSA test.Among all the factors identified, recommendations from health professionals showed the strongest association with PSA test uptake in this population.Health professionals should take an active role in educating this particular population in cancer prevention and detection.
Acknowledgements
This study was supported by the Chinese University of Hong Kong.Its content is solely the responsibility of the authors and does not necessarily represent the official views of the institution.
Conflict of interest
No conflicts of interest are disclosed.
1.Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D.Global cancer statistics.CA Cancer J Clin 2011;61:69-90.
2.Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM.Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008.Int J Cancer 2010;127:2893-2917.
3.Hong Kong Cancer Registry.Fast stats for prostate cancer 2010.2010.Available online: http://www3.ha.org.hk/cancereg/e_stat.asp, accessed May 312013.
4.Thompson IM, Ankerst DP.Prostate-specific antigen in the early detection of prostate cancer.CMAJ 2007;176:1853-1858.
5.Wolf AM, Wender RC, Etzioni RB, Thompson IM, D’Amico AV, Volk RJ, et al.American Cancer Society guideline for the early detection of prostate cancer: update 2010.CA Cancer J Clin 2010;60:70-98.
6.Hamashima C, Yoshida K.Cost-effectiveness analysis of prostate cancer screening.Environ Health Prev Med 2000;5:111-117.
7.Romero FR, Romero KR, Brenny FT, Pilati R, Kulysz D, de Oliveira Júnior FC.Reasons why patients reject digital rectal examination when screening for prostate cancer.Arch Esp Urol 2008;61:759-765.
8.Pienta KJ.Critical appraisal of prostate-specific antigen in prostate cancer screening: 20 years later.Urology 2009;73:S11-S20.
9.Duffy MJ.Prostate-specific antigen: does the current evidence support its use in prostate cancer screening? Ann Clin Biochem 2011;48:310-316.
10.Rogers CS.Perspective on prostate cancer screening.Int J Clin Pract 2011;65:31-34.
11.Djulbegovic M, Beyth RJ, Neuberger MM, Stoffs TL, Vieweg J,Djulbegovic B, et al.Screening for prostate cancer: systematic review and meta-analysis of randomised controlled trials.BMJ 2010;341:c4543.
12.Schr?der FH, Hugosson J, Roobol MJ, Tammela TL, Ciatto S, Nelen V, et al.Screening and prostate-cancer mortality in a randomized European study.N Engl J Med 2009;360:1320-1328.
13.Bartsch G, Horninger W, Klocker H, Pelzer A, Bektic J, Oberaigner W, et al.Tyrol Prostate Cancer Demonstration Project: early detection, treatment, outcome, incidence and mortality.BJU Int 2008;101:809-816.
14.Patel K, Kenerson D, Wang H, Brown B, Pinkerton H, Burress M,et al.Factors influencing prostate cancer screening in low-income African Americans in Tennessee.J Health Care Poor Underserved 2010;21:114-126.
15.Beaulac JA, Fry RN, Onysko J.Lifetime and recent prostate specific antigen (PSA) screening of men for prostate cancer in Canada.Can J Public Health 2006;97:171-176.
16.Chung LC, Hsieh ML, Liu HE.Determining factors of prostatic cancer screening behaviors among high risk men using health belief model.Tsu Chi Nurs 2003;2:38-48 (in Chinese).
17.Lin YH, Li HC, Cheng HF, Wu YH, Kao CC.Factors influencing southern Taiwanese men’s acceptance of prostate-specific antigen screening.Int J Urol Nurs 2011;5:83-89.
18.Conde FA, Landier W, Ishida D, Bell R, Cuaresma CF, Misola J.Barriers and facilitators of prostate cancer screening among Filipino men in Hawaii.Oncol Nurs Forum 2011;38:227-233.
19.Ferrante JM, Shaw EK, Scott JG.Factors influencing men’s decisions regarding prostate cancer screening: a qualitative study.J Community Health 2011;36:839-844.
20.G?bl CS, Ortag F, Bozkurt L, Smeikal A, Dadak C, Kautzky-Willer A.Health behaviour and attitude towards screening examinations in an Austrian urban and rural population: gender aspects -screening and sex.Wien Med Wochenschr 2011;161:143-148.
21.Richardson H, Aronson KJ, James A, McGregor ES, Bryant H.Factors related to use of prostate cancer screening: the Alberta Tomorrow Project.Open Med 2007;1:e3-e12.
22.Liao PS, Fu YC, Yi CC.Perceived quality of life in Taiwan and Hong Kong: An intra-culture comparison.J Happiness Stud 2005;6:43-67.
23.Yao G, Wu CH.Similarities and differences among the Taiwan,China, and Hong-Kong versions of the WHOQOL questionnaire.Social Indicators Res 2009;91:79-98.
24.So WK, Choi KC, Chan DN, Shiu AT, Ho SS, Chan HY, et al.Colorectal cancer screening behaviour and associated factors among Chinese aged 50 and above in Hong Kong - a populationbased survey.Eur J Oncol Nurs 2012;16:413-418.
25.Centers for Disease Control and Prevention.NHIS 2005.NHIS survey description.2006.Available online: ftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/NHIS/2005/srvydesc.pdf, accessed May 312013.
26.Hosmer DW, Lemeshow S.Applied logistic regression.2nd ed.New York: John Wiley and Sons, 2000.
27.Census and Statistic Department.Women and men in Hong Kong key statistics.2012.Available online: http://www.statistics.gov.hk/pub/B11303032012AN12B0100.pdf, accessed May 302013.
28.Ahn AC, Ngo-Metzger Q, Legedza AT, Massagli MP, Clarridge BR,Phillips RS.Complementary and alternative medical therapy use among Chinese and Vietnamese Americans: prevalence, associated factors, and effects of patient-clinician communication.Am J Public Health 2006;96:647-653.
29.Avery KN, Blazeby JM, Lane JA, Neal DE, Hamdy FC, Donovan JL.Decision-making about PSA testing and prostate biopsies: a qualitative study embedded in a primary care randomised trial.Eur Urol 2008;53:1186-1193.
30.Centre for Health Protection.Hong Kong Department of Health.Screening for prostate cancer information for men and their families.2010.Available at http://www.chp.gov.hk/ files/pdf/screening_for_prostate_cancer_information_for_men_and_their_families_2010.pdf, accessed May 312013.
 Cancer Biology & Medicine2014年1期
Cancer Biology & Medicine2014年1期
- Cancer Biology & Medicine的其它文章
- Inhalation treatment of lung cancer: the influence of composition, size and shape of nanocarriers on their lung accumulation and retention
- Interferon-alpha-2b induces autophagy in hepatocellular carcinoma cells through Beclin1 pathway
- pH-responsive mesoporous silica nanoparticles employed in controlled drug delivery systems for cancer treatment
- Mechanistic considerations for the use of monoclonal antibodies for cancer therapy
- Cancer metabolic reprogramming: importance, main features,and potentials for precise targeted anti-cancer therapies
- Instructions for Authors