
Lymphoepithelial cysts of the pancreas:a management dilemma
2014-06-11 08:05:44
Leeds,UK
Introduction
Pancreatic lymphoepithelial cysts (LECs) are rare,benign lesions of the pancreas first described by Lüchtrath and Schriefers in 1985,[1]and are considered true cysts.Kavuturu et al[2]reported that in the 28 years since the first report of an LEC,109 cases have so far been documented in the literature.There have been several recent comprehensive reviews documenting the demographic features of LECs,which indicate a strong male preponderance,with lesions of variable size distributed throughout the head,body and tail of the pancreas.[2-4]Approximately half of the patients present incidentally with the remaining patients being associated with non-specific symptoms such as nausea,vomiting,diarrhoea,abdominal pain,weight loss,and fatigue.[2-4]
LECs are benign and do not possess malignant potential and thus accurate identification of these lesions is important to avoid unnecessary intervention.However,LECs share radiological and pathological features in common with other pancreatic cystic lesions,some of which are treated by surgical resection.
Until recently,there was no reliable means of preoperatively diagnosing LECs.The computed tomography(CT) appearances of LECs are those of a well-defined low-attenuation lesions,[2]often with septations or a multilocular appearance (60%),and they are frequently exophytic.[5]As the cysts often contain a large volume of keratinized material,the pre-contrast scan may show increased density and appear solid.[6-7]However,these features do not appear to be universal.
Endoscopic ultrasound (EUS) is of great value for the evaluation of pancreatic cystic lesions.[8]It has been suggested that LECs have diagnostic features including the presence of squamous epithelium overlying dense lymphoid tissue,with aspirates that may be white and frothy with acellular debris and cholesterol crystals.[2-4]Nasr et al,[9]in the largest single series evaluating EUS,noted that 6 of 9 patients with LECs could be managed non-operatively on the basis of EUS examination and aspiration cytology.However,others suggested that the results of EUS are not reliable,and in the absence of a squamous epithelium rich in lymphocytes it may be difficult to differentiate between LECs and other cystic neoplasms.[10]It is generally accepted that further work is required to clarify the role of EUS.[2,4]
Potentially,the most useful modality to establish a pre-operative diagnosis of LEC is magnetic resonance imaging (MRI),with a number of unique features having been identified.[11-13]The thick walls of the cysts are hypointense on T1 and T2 weighted images and enhance with administration of contrast and keratinous material,where present high intensity on T1 and low intensity on T2 sequences.[11]Nam and colleagues[12]used a diffusion-weighted MRI protocol,and found that LECs exhibited a profound restriction of water molecule motion on diffusion-weighted imaging,with or without wall enhancement on contrast-enhanced imaging.Kudo et al[13]who look at in/out-of-phase imaging reported a slight signal reduction during out-of-phase sequences compared with in-phase sequences,indicating the coexistence of fat and water.
The aim of this study was to review the medical histories and investigations of a cohort of patients with known LEC to identify features that may alert clinicians to the diagnosis of LEC.Given the rare nature of the lesions,two large volume dedicated pancreatic units contributed to the study.
Methods
Patients who had undergone resection of LECs were identified from the pathology department databases of two specialist pancreatic centers (Cleveland Clinic,Cleveland,Ohio,USA and St James's University Hospital,Leeds,West Yorkshire,UK).
Both departments have dedicated pancreatic multidisciplinary teams,and each case was discussed at a multidisciplinary forum consisting of consultant surgeons,radiologists,endoscopists,pathologists and oncologists.
Data collected included demographic details and mode of presentation whether symptomatic or incidental.For cross-sectional imaging studies,data evaluated included:location; size; number; presence of septations; presence of nodules; rim calcifications; and diameter of the pancreatic duct.Data collated following endoscopic ultrasound-guidedfine needle aspiration(EUS-FNA) included color,consistency,cytology,mucin and where aspirate allowed carcinoembryonic antigen(CEA) and amylase.
The indications for resection were recorded as the procedures undertaken,histopathological findings,morbidity and outcome.
Results
Six patients who were identified between February 2002 and March 2010 consisted offive males and one female.The median age was 60 years (range 48-70) at presentation.Table summarises the demographic details,investigations,management and outcome of each case.
Mode of presentation
All lesions of the 6 patients were identified on crosssectional imaging.Four lesions were found incidentally,and two were confirmed by imaging because of upper abdominal pain of the patients.No patient had symptoms of pancreatic exocrine or endocrine insufficiency.
Investigations and findings
CT characterized the lesions initially in all patients(Fig.1).The median size was 5.0 cm (range 3.0-6.9) withfive lesions located in the pancreatic tail and one in the body.The attenuation of the cysts varied between 23 and 52 Hounsfield units (Hu).There were no features of chronic pancreatitis or other pancreatic disease; the pancreatic duct was normal in each patient.
EUS identified that the lesions were homogenous in nature though one had septations within it (Fig.2).In half of the lesions,the cyst wall was seen to be irregular.Aspiration was attempted on all lesions;however pathologic analysis was not uniform.In each patient,aspiration was difficult or unsuccessful due to the viscous cyst content,and cyst fluid was in various colors.The level of CEA was analyzed only in one patient and found to be elevated (61 687 IU/L).Amylase analysis was completed in four patients,three of which had negative results and one had an elevated level (1600 IU/L).Five of six patients were analyzed for mucin:three showed negative results and two showed positive ones.Cytologic material was available in all patients and was non-diagnostic with normal and occasional in flammatory cells; however,the consistent feature was a largely acellular aspirate.
MRI was only performed in 3 patients in this series re flecting its historical nature and rarity of LECs.No specific diagnostic features were identified at the time of performance of the MRI scans; however,review of the imaging in the light of recent observations on the typical characteristic features of LECs confirmed that the cyst walls to be hypointense on un-enhanced T1/T2 weighted imaging (Fig.3).A mild degree of enhancement wasobserved following administration of the contrast agent gadolinium in each patient.The keratinous material within the cysts produced a high signal intensity of the cyst on T1 weighted sequences (Fig.4).
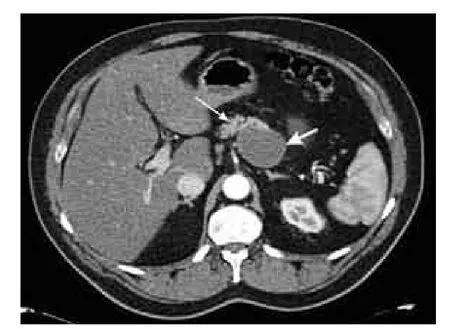
Fig.1.CT scan through the upper abdomen in pancreatic phase of enhancement.A normally enhanced pancreas (thin arrow).The cyst (thick arrow) arising from the superior border of the pancreas.The attenuation of cyst content was 42 Hu.Note faintly enhanced cyst wall.
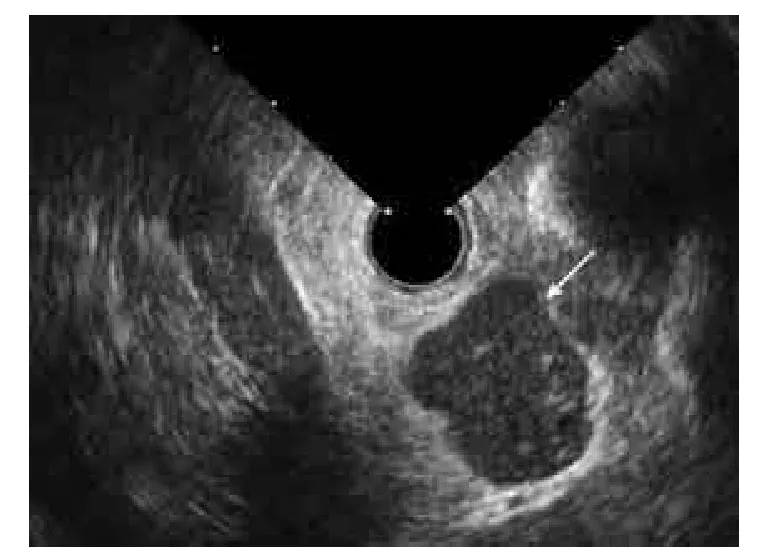
Fig.2.EUS showing a cyst containing fluid with low level echoes(arrow).
Pre-operative diagnosis,indications for treatment,and operative findings

Fig.3.T2 weighted image showing a low signal intensity cyst(thick arrow).Cysts are usually of high signal intensity similar to cerebrospinal fluid (CSF) (thin arrow).

Fig.4.T1 weighted image of the pancreas showing a relatively high signal intensity cyst (arrow).
The pre-operative diagnosis was mucinous cystic neoplasm in every patient.Distal pancreatectomy and splenectomy were performed in each patient (four laparoscopic).The indications for surgery included increase in size (n=2),atypical cytology (n=1),and nodularity or positive mucin/CEA analysis (n=3).At laparoscopy the pancreas appeared normal in all patients.The cystic lesions were not adherent to adjacent structures and resections were uncomplicated.All six patients were diagnosed histologically as having LEC.
Histopathology
Histological examination revealed well delineated,round lesions distinguishable from adjacent adipose and pancreatic tissue (Fig.5).Microscopically,the LECs werefilled with keratinous debris and lined by stratified squamous epithelium,surrounded by a rim of mature lymphoid tissue,comprising mainly T lymphocytes with intervening well-formed germinal centers containing B cells (Fig.6).
Outcome

Fig.5.Macroscopic appearance of LEC.

Fig.6.The cyst wall composed of con fluent lymphoid aggregates,lined by stratified squamous epithelium.
Four patients were uncomplicated.One patient developed a pancreaticfistula that presented with signs of sepsis,and subsequently a pancreaticopleuralfistula with empyema formation.[14]Following percutaneous drainage of the intra-abdominal collection and thorascopic washout with decortication,he recovered without complications.Three patients died subsequently,one of unrelated nasopharyngeal carcinoma,one of unrelated lymphomatous meningitis,and one of secondary to sepsis.The third patient had a history of chronic obstructive pulmonary disease and developed a postoperative pneumonia that progressed to multi-organ failure (MOF).She recovered from this complication and was discharged home.Four months later,she developed further chest-related sepsis,from which she developed MOF but did not recover on this occasion.
Discussion
Over the past two decades,there has been a greater appreciation of cystic pancreatic lesions because of the increased use and higherfidelity of cross-sectional imaging and a diverse group of cystic pancreatic lesions are currently recognised.[15]Accurate identification of these lesions is essential as the management of benign,indeterminate and malignant lesions is very different.However,despite an array of available technologies,the difficulty in differentiating benign cysts from those with malignant potential with non-invasive imaging has been well-described.[16]
The current series and the existing literature suggest that LECs are most commonly seen in elderly men.[2-4]They may be varied in size,number,locularity (60%multilocular),and location although in the series we reported they were large (all >3 cm),located within the body and tail of the pancreas,and unilocular (83%).Therefore,while the demographics may be robust there is no consensus on morphology.The cysts are characterized by squamous epithelia with a rich vane of sub-epithelial lymphoid tissue and the cyst contents are often white in color and may include keratinized material or cholesterol crystals.[2-4]None of the patients in our series exhibited cyst contentfitting the classic description.
The pathogenesis of LECs is uncertain at present.Osiro and colleagues[4]reviewed the literature and identified a number of theories about the pathogenesis of LECs .The 3 most common theories are:squamous metaplasia in an obstructed duct with subsequent cyst formation; origin from ectopic pancreas in a peripancreatic lymph node; and LECs due to fusion of misplaced branchial cleft cysts with the pancreas during embryogenesis.Raval et al[17]examined the expression of MUC genes in 9 patients undergoing resection of pancreatic cysts.They identified MUC1 and MUC4 in the LECs suggesting that they may have originated from the pancreatic duct as a result of squamous metaplasia and later cyst formation since these MUC genes are usually expressed in normal stratified squamous epithelium,pancreatic squamous metaplasia and squamoid cysts of the pancreas,but MUC4 is not normally seen in the adult pancreas.Furthermore,the group demonstrated a possible etiology of the raised level of CEA seen in 3 of their patients,as they identified not only MUC5AC-positive goblet cells but also the positive staining the squamous epithelium of LECs or CEA and carbohydrate antigen 19-9 (CA19-9) in all patients.This was particularly significant in patients with elevated levels of cyst CEA.Bédat et al[18]reported 2 patients with pancreatic LECs linked to HIV infection.They suggested testing all patients with pancreatic LECs for the presence of HIV.Interestingly,their patients were younger males (45 & 48 years) and both contacted HIV as young adults,so they were not characteristic of the population demographics for pancreatic LECs.Therefore,Bédat and colleagues' proposal may be premature and further evidence is required to justify such a policy.LECs of the parotid have been reported in patients with HIV infection and are said to be pathognomonic of the disease.[19]However,Wu et al[20]found no such relationship in a series of 64 parotid LECs.No patients in our series were known to have HIV or shown any manifestations of the condition.
Some of the radiological features of LECs may theoretically allow the diagnosis to be made preoperatively.Abdominal CT demonstrates a cystic lesion,often arising from the periphery of the pancreas.The attenuation of LECs is often in the range 20-50 Hu.[2-4,6,7]Indeed the range for the current patients was 23-52 Hu.In some patients,the lipid nature of cyst content may be suggested by the recognition of areas of fat attenuation on CT.[7]A measurement of attenuation is helpful as both in flammatory and neoplastic cystic lesions have attenuation values of 10-15 Hu,which re flect the predominant water content.EUS-FNA has developed as an important tool for differentiation of the etiology of pancreatic cystic lesions and is part of the investigation protocol of most pancreatic units.[8]In our patients,the cyst content varied,and no diagnostic pattern was seen apart from the observation that the fluid was difficult to aspirate.Importantly,the creamy thick material described by Nasr et al[9]was not observed and cytological examination,performed in all cases,did not show the classical features of an LEC,namely squamous epithelium with a rich lymphocytic infiltrate.[2-4]In our series,one of the LECs had a markedly elevated cyst CEA level and 2 had mucin.These features as reported previously lead to a diagnostic dilemma as mucinous neoplasms have to be considered.[20]Nasr et al[9]noted that 6 of 9 patients with LECs could be managed nonoperatively on the basis of EUS examination and aspiration cytology,such results are not universal.However,the current data[2,4]including ours would suggest that EUS is not a reliable modality for the preoperative diagnosis of LECs.Recent development of MRI in detecting pancreatic cystic lesions including LECs may be helpful to obtain a pre-operative diagnosis as MRI has greater soft tissue resolution,and the signal intensity on T1 and T2 weighted images may re flect the histopathological appearances of LECs.[11-13]The findings of 3 MRIs performed in our series were in consistent with those on a hypointense cyst wall by T1 weighted imaging after administration of contrast.The other diagnostic feature was also confirmed with keratinous material producing a high signal intensity on T1 sequences.This feature may help to distinguish LECs from other pancreatic cystic lesions,which are generally of very high signal intensity on comparable sequences.At present MRI has been incorporated into routine use.
Despite the existence of the literature suggesting that a pre-operative diagnosis of LEC may be dependent on imaging studies,in our experience,the presence of additional features can lead to operations in these cases.In two of our patients with asymptomatic cysts,an increase would have been possible in size of the cysts on sequential cross-sectional imaging.In the remaining patients whose pancreatic cyst had been an asymptomatic finding,the presence of nodules,poor circumscription and enhancement of the cyst wall,and atypical cytology lead to resection of the cysts as these features are suspicious of malignancy in mucinous cystic lesions.In the two patients with abdominal pain,one had a cyst containing mural nodules,and the other had mucin and a significantly elevated level of CEA.The radiological and aspirate features include the presence of 5 of 6 unilocular cysts,whereas the literature suggests that the majority of cysts are multilocular.It is suspected that lesions may be mucinous cystic neoplasm,which was predominant in women.[15]Furthermore,as all cysts were greater than 3 cm in diameter,namely 5 cm or greater,they fell within the Sendai guidelines for excision.[21]
In conclusions,LECs as uncommon pancreatic cystic lesions with a predominance in men,are normally present in the sixth or seventh decade of life.They do not have a consistent presenting symptom profile,and features on EUS and CT are equivocal.Evaluation with MRI may provide a signature that allows LECs to be diagnosed pre-operatively,which in turn may allow reassurance and avoid operative intervention.However,many LECs are likely to be diagnosed post-operatively.
Acknowledgement:Thanks to C.S.Verbeke,Department of Histopathology,Karolinska Institute,Stockholm,Sweden for providing histopathology images.
Contributors:SAM and MSG proposed the study.MJ and RKJ performed research and wrote the first draft.MJ collected and analyzed the data.MSG reviewed the original draft.All authors contributed to the design and interpretation of the study and to further drafts.MJ is the guarantor.
Funding:None.
Ethical approval:Not needed.
Competing interest:No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
1 Lüchtrath H,Schriefers KH.A pancreatic cyst with features of a so-called branchiogenic cyst.Pathologe 1985;6:217-219.
2 Kavuturu S,Sarwani NE,Ruggeiro FM,Deshaies I,Kimchi ET,KaifiJT,et al.Lymphoepithelial cysts of the pancreas.Can preoperative imaging distinguish this benign lesion from malignant or pre-malignant cystic pancreatic lesions?JOP 2013;14:250-255.
3 Sewkani A,Purohit D,Singh V,Jain A,Varshney R,Varshney S.Lymphoepithelial cyst of the pancreas:a rare case report and review of literature.Indian J Surg 2010;72:427-432.
4 Osiro S,Rodriguez JR,Tiwari KJ,Rodriguez II,Mathenge N,Tubbs RS,et al.Is preoperative diagnosis possible? A clinical and radiological review of lymphoepithelial cysts of the pancreas.JOP 2013;14:15-20.
5 Zaheer A,Pokharel SS,Wolfgang C,Fishman EK,Horton KM.Incidentally detected cystic lesions of the pancreas on CT:review of literature and management suggestions.Abdom Imaging 2013;38:331-341.
6 Kim WH,Lee JY,Park HS,Won HJ,Kim YH,Choi JY,et al.Lymphoepithelial cyst of the pancreas:comparison of CT findings with other pancreatic cystic lesions.Abdom Imaging 2013;38:324-330.
7 Fukukura Y,Inoue H,Miyazono N,Kajiya Y,Fujiyoshi F,Yano T,et al.Lymphoepithelial cysts of the pancreas:demonstration of lipid component using CT and MRI.J Comput Assist Tomogr 1998;22:311-313.
8 Walsh RM,Zuccaro G,Dumot JA,Vargo J,Biscotti CV,Hammel J,et al.Predicting success of endoscopic aspiration for suspected pancreatic cystic neoplasms.JOP 2008;9:612-617.
9 Nasr J,Sanders M,Fasanella K,Khalid A,McGrath K.Lymphoepithelial cysts of the pancreas:an EUS case series.Gastrointest Endosc 2008;68:170-173.
10 Zieli?ska-Pajak E,Liszka L,Pajak J,Go?ka D,Lampe P,Pilch-Kowalczyk J,et al.Two cases of lymphoepithelial cyst of the pancreas: first - a cyst coexisting with a primary gastric lymphoma,second - incidentally found pancreatic cyst.Z Gastroenterol 2008;46:1188-1193.
11 Shinmura R,Gabata T,Matsui O.Lymphoepithelial cyst of the pancreas:case report with special reference to imaging--pathologic correlation.Abdom Imaging 2006;31:106-109.
12 Nam SJ,Hwang HK,Kim H,Yu JS,Yoon DS,Chung JJ,et al.Lymphoepithelial cysts in the pancreas:MRI of two cases with emphasis of diffusion-weighted imaging characteristics.J Magn Reson Imaging 2010;32:692-696.
13 Kudo D,Hashimoto N,Toyoki Y,Narumi S,Hakamada K.Usefulness of in-phase and out-of-phase magnetic resonance imaging for the detection of pancreatic lymphoepithelial cyst.Hepatogastroenterology 2011;58:1403-1405.
14 Roberts KJ,Sheridan M,Morris-Stiff G,Smith AM.Pancreaticopleuralfistula:etiology,treatment and long-termfollow-up.Hepatobiliary Pancreat Dis Int 2012;11:215-219.
15 Basturk O,Coban I,Adsay NV.Pancreatic cysts:pathologic classification,differential diagnosis,and clinical implications.Arch Pathol Lab Med 2009;133:423-438.
16 Visser BC,Yeh BM,Qayyum A,Way LW,McCulloch CE,Coakley FV.Characterization of cystic pancreatic masses:relative accuracy of CT and MRI.AJR Am J Roentgenol 2007;189:648-656.
17 Raval JS,Zeh HJ,Moser AJ,Lee KK,Sanders MK,Navina S,et al.Pancreatic lymphoepithelial cysts express CEA and can contain mucous cells:potential pitfalls in the preoperative diagnosis.Mod Pathol 2010;23:1467-1476.
18 Bédat B,Genevay M,Dumonceau JM,Frossard JL,Forget J,Morel P,et al.Association between lymphoepithelial cysts of the pancreas and HIV infection.Pancreatology 2012;12:61-64.
19 Steehler MK,Steehler MW,Davison SP.Benign lymphoepithelial cysts of the parotid:long-term surgical results.HIV AIDS(Auckl) 2012;4:81-86.
20 Wu L,Cheng J,Maruyama S,Yamazaki M,Tsuneki M,Lu Y,et al.Lymphoepithelial cyst of the parotid gland:its possible histopathogenesis based on clinicopathologic analysis of 64 cases.Hum Pathol 2009;40:683-692.
21 Tanaka M,Chari S,Adsay V,Fernandez-del Castillo C,Falconi M,Shimizu M,et al.International consensus guidelines for management of intraductal papillary mucinous neoplasms and mucinous cystic neoplasms of the pancreas.Pancreatology 2006;6:17-32.
 Hepatobiliary & Pancreatic Diseases International2014年5期
Hepatobiliary & Pancreatic Diseases International2014年5期
- Hepatobiliary & Pancreatic Diseases International的其它文章
- Non-operative management of isolated liver trauma
- WNT5A modulates cell cycle progression and contributes to the chemoresistance in pancreatic cancer cells
- Prognostic significance of epidermal growth factor-like domain 7 in pancreatic cancer
- Post-pancreaticoduodenectomy hemorrhage:risk factors,managements and outcomes
- Laparoscopic liver resection under hemihepatic vascular in flow occlusion using the lowering of hilar plate approach
- Long-term results of liver transplantation for over 60 years old patients with hepatitis B virus-related end-stage liver disease