
Non-operative management of isolated liver trauma
2014-06-11 08:05:46
Nanjing,China
Introduction
Liver parenchyma and its vasculature are fragile and very susceptible to blunt and penetrating trauma which makes the liver the most frequently injured abdominal organ.[1]Hemorrhagic shock due to uncontrollable bleeding of vessels and parenchyma is the major cause of death within the first 36 hours after injury.[2]The management of liver trauma in the early 1900s was observation and expectant treatment and later on,mainly operative intervention.[3]The current practice is either selective surgery or non-operative management (NOM),depending on the grade of the trauma.NOM of liver trauma was first reported in 1972,and has been one of the most significant changes in the treatment of liver trauma over the past three decades.[4,5]In recent years,the overall mortality in large series of patients who sustained liver trauma has ranged from 10% to 15%.[6,7]Although the mortality of liver trauma has decreased in the past decades,the selection criteria for NOM are constantly evolving,and conservative approaches are being increasingly adopted.
Several studies on patients with liver trauma suggested that early deaths are due to uncontrolled bleeding from associated intra- and extra-abdominal injuries; whereas late deaths result from head injury and sepsis with multi-organ failure.[8-10]Patients with liver trauma usually have complicated injuries,and the results of NOM have been in fluenced by coexisting trauma.[6,7]The aim of this study was to determine the success rate,mortality and morbidity of NOM in patients with isolated liver trauma.
Methods
A retrospective analysis was performed on all the patients treated for liver trauma in our unit between January 2007 and April 2012.The medical records of patients with isolated liver trauma were extracted.Isolated liver trauma was defined as liver injury with no other intra- or extra-abdominal involvement.The success rate,mortality and morbidity of patients who underwent NOM or surgery were reviewed.
The grade of liver trauma was determined according to the scaling system of the American Association for the Surgery of Trauma (AAST).[11]Failure of NOM was defined as the need of surgical intervention to manage bleeding at any time during hospitalization or in the follow-up period.All patients were followed up by phone calls for six months.Data analysis was performed by SPSS 18.0 (SPSS Inc.,Chicago,IL,USA).All results were reported as mean±standard deviation.
The patients with hemodynamic instability underwent emergent surgery.The selection criterion for NOM was hemodynamic stability,which was defined as a systolic pressure >90 mmHg after adequate resuscitation (1 L of intravenous fluids within 1 hour).The treatment algorithm of NOM involved monitoring patients in an ICU with serial physical examinations and hematocrits.Red blood cell (RBC) transfusions were given when hemoglobin levels were less than 7 g/L.[12]Heart rate,blood pressure,respiratory rate,central venous pressure and urinary output were monitored.Acidosis was corrected promptly; rewarming blankets and warm intravenous fluids were used to avoid hypothermia when core temperature was lower than 36 ℃.[13]Somatostatin was used in the patients with biliaryfistulas to decrease choleresis.Unlike conventional approaches,we corrected coagulopathy according to the result of thromboelastography (TEG)instead of prothrombin time (PT) and activated partial thromboplastin time (APTT).Blood products,including fresh frozen plasma,platelet and cryoprecipitate,were intravenously infused according to the results of TEG.The patients who had hemoperitoneum underwent ultrasound guided percutaneous peritoneal drainage in order to determine the volume of hemoperitoneum.The catheter was removed when hemoperitoneum resolved as determined by ultrasonic monitoring or operation if needed.Hepatic artery angiography embolization was used when computed tomography (CT) scanning demonstrated contrast extravasation.
Results
Between January 2007 and April 2012,there were 268 patients treated for liver trauma in our unit.Among them,187 had multiple injuries and were excluded from this cohort.Of the remaining 81 patients,9 with grade IV-V liver injuries underwent emergent operation because of hypovolemic shock and 72 received NOM.
The average age of the 72 patients was 35.9±10.8 years (range 17-69); these patients included 55 men and 17 women.Liver trauma consisted of traffic (n=30),industrial (n=22),falls (n=8),assault (n=4),sports(n=5) and penetrating injuries (n=3).Six patients had liver trauma of grade V (8.3%),18 grade IV (25.0%),29 grade III (40.3%),15 grade II (20.8%),and 4 grade I (5.6%).The average volume of hemoperitoneum was 1537±692 mL (range 430-3360) (Table 1).The patients who received NOM underwent contrast-enhanced CT scanning of the abdomen (Fig.1).The peak levels of alanine aminotransferase,aspartate aminotransferase,and total bilirubin were 1520.0±794.9 U/L (range 237-3054),1054.1±531.6 U/L (range 172-2132),and 23.4 ±10.5 μmol/L (range 8.8-61.1),respectively.The shortest reaction time was 16.7±7.8 minutes (range 5.3-34.7,normal 5-10),the shortest kinetic time was 9.8 ±5.7 minutes (range 1.5-20.4,normal 1-3),and the levelof maximum amplitude (MA) was 50.1±6.7 mm (range 40.2-67.3,normal 50-70) (Fig.2).There were 17 (23.6%)patients with hypothermia,and 41 patients (56.9%)with acidosis.Forty-eight patients received an average of 7.4±6.2 U (range 3-18) RBC transfusions.

Table 1.Patient characteristics according to the management firstly performed
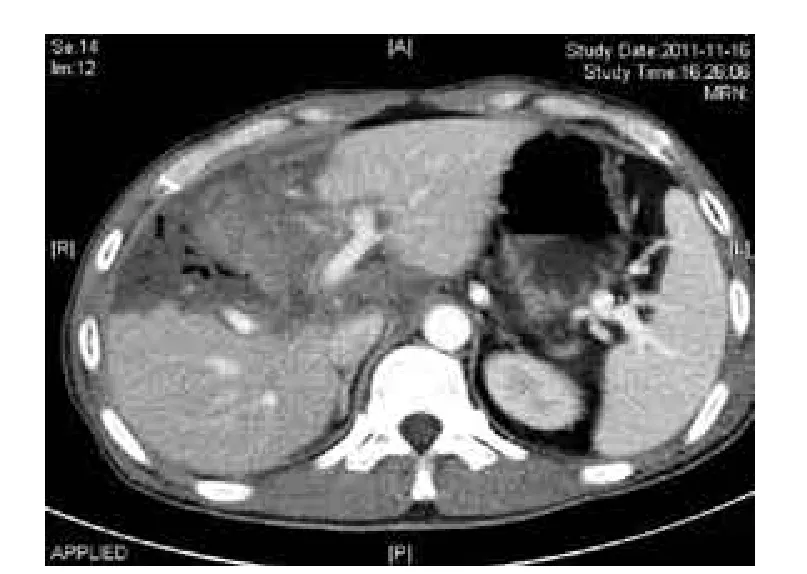
Fig.1.Contrast-enhanced CT scanning of grade IV blunt liver trauma.
All patients who underwent NOM survived.Seventy out of 72 patients were managed successfully without operation,including 5 patients with grade V,17 with grade IV and 48 with grade I-III liver trauma.The overall success rate of NOM was 97.2%.The success rates of NOM in the patients with grade I-III,IV and V liver trauma were 100%,94.4% and 83.3%,respectively.Thirty-five patients underwent hepatic angiography because of extravasation of contrast material on CT scanning.Of these patients,24 (68.6%) required embolization (Fig.3,Table 2).In the 24 patients,bleeding was stopped in 22 patients,and 2 patients(1 grade IV and 1 grade V) needed operation because of hemorrhagic shock.The success rate of hepatic angioembolization (HAE) was 91.7%.Among the 70 patients who were managed successfully without operation,7 had complications.The overall morbidity of NOM for liver trauma was 10.0%.No patient with grade I-II liver trauma had complications.One patient with grade III liver trauma had a biloma.Three patients with grade IV liver trauma had complications including 2 bilomas and 1 biliary fistula.Three of 6 patients with grade V liver trauma had complications including 1 biloma and 2 biliaryfistulas (Table 3).Three biliaryfistulas were due to the injury of the right hepatic duct identified by endoscopic retrograde cholangiopancreatograhpy (ERCP),and were resolved by subsequent surgery in which cholangiojejunostomy was performed.Because the diameter was <3 cm,and there were no clinical symptoms,4 patients with bilomas were treated conservatively.

Fig.2.TEG data of a patient with severe liver trauma showing coagulopathy.
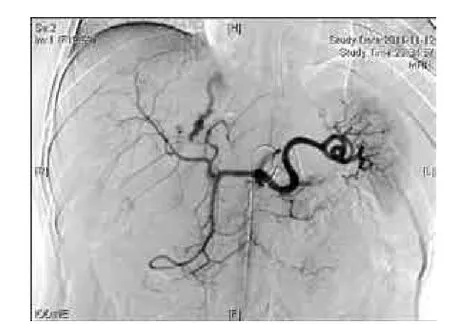
Fig.3.Angiography of grade IV blunt liver trauma.
Eleven patients underwent operation due to hemodynamic instability,including 9 direct surgery and 2 failed NOM.The 9 patients had an average volume of hemoperitoneum of 1942±308 mL (range 1400-3010).In these patients,concomitant right hepatic vein injury occurred in 4,left hepatic vein in 1,portal vein in 1,ruptured gallbladder in 3 and common bile duct laceration in 1.After angiography,ruptured gallbladders were excised and the continuity of the common bile ducts was restored with interrupted suture.All patients received hepatic packing which was removed by reoperation 3 days later.Two patients (18.2%) died after operation due to multi-organ dysfunction syndrome.Eight postoperative complications occurred in 5 patients,hemorrhage in 3,intra-abdominal abscess in 1,and biliaryfistulas in 4 (Table 3).Postoperative hemorrhage happened in 3 patients on day 2 after gauze removal,of which 2 patients were treated by HAE,and 1 required another hepatic packing.

Table 2.A summary of patients successfully treated with NOM

Table 3.Complications of the patients according to the managementfinally performed
Discussion
The paradigm for management of liver trauma has shifted over the past decades,from mandatory operation to selective NOM.This paradigm shift has been attributed to several factors:(1) the recognition that 50%-80% of liver injuries stop bleeding spontaneously,(2) the successful NOM in children,and (3) the significant development of CT scanning,interventional radiology and critical care.[5,14]A recent review of the National Trauma Data Base in America showed that 86.3% of all liver injuries were managed conservatively.[15]In the current series,72 patients with liver trauma whose hemodynamics were stable were selected for NOM.This included 53 patients with grade III-V and 19 patients with grade I-II liver trauma.The volume of hemoperitoneum in the patients who had abdominal free fluid was 1537±692 mL (range 430-3360)compared with those underwent surgery (1942±308 mL,range 1400-3010).The NOM success rate in the patients with grade I-III liver trauma (n=48) was 100%;in those with grade IV and V was 94.4% and 83.3%,respectively.The overall success rate of NOM was 97.2%which is higher than that reported in other studies.[16-18]We conclude that the liver trauma patients with stable hemodynamics can be treated without operation with a high success rate.The grade of liver trauma and the volume of hemoperitoneum are not significant parameters for selecting NOM.These conclusions are consistent with those reported elsewhere.[4,19]
CT scanning is currently the standard evaluation modality for stable patients with abdominal injury.[20,21]Hoff et al[22]reported a sensitivity of 92%-97% and a specificity of 98.7% in liver trauma.The finding of extravasation of contrast material within the liver parenchyma on CT scanning is indicative of active hemorrhage.Fang et al[23]reported that 75% of patients with contrast extravasation and hemodynamic instability required operation.Embolization of hepatic arterial bleeding could control bleeding from 68%to 87%.[23]In the current study,patients with stable hemodynamics were diagnosed by contrast-enhanced CT.Thirty-five patients underwent hepatic arterial angiography because of extravasation of contrast material on CT scanning,and 24 required embolization.The hemorrhage was stopped in 22 patients.The success rate of HAE was 91.7%.
Hemorrhage can result in hypothermia,coagulopathy and acidosis,so called lethal triad.Each exacerbates the others.The vicious cycle rapidly deteriorates the patients and causes death.Mortality increases significantly in trauma patients with a core temperature less than 34 ℃ and approached 100% when less than 32 ℃.[24]In this series,warm blankets and intravenous fluids were used to avoid hypothermia when core temperatures were lower than 36 ℃.
Various coagulation problems can appear when liver injury occurs.This may be due to the hemorrhage,or to liver dysfunction,which causes both qualitative and quantitative alterations in pro- and anticoagulants,and platelets.Reduced degradation of activated components,hyperfibrinolysis and deficient metabolism of citrate in the blood components may also play a role.We monitored blood coagulation of the patients through the results of TEG.In contrast to conventional coagulation tests which assay only clot formation time in a plasma environment,TEG assesses overall hemostasis,the cumulative effects of procoagulant,anticoagulant proteins, fibrinogen and platelets. Component measurements of the TEG re flect specific phases of clot formation.[25]In many studies,TEG shows superior properties compared to conventional coagulation parameters.[26]Prolonged reactive time suggests clotting factor deficiency or heparin effect.The kinetic time re flects the time from initialfibrin formation required to reach specific clotfirmness and is proportional tofibrinogen concentrations and platelet count.The maximum amplitude re flects maximal clot strength and is proportional to the amount and function of platelet.Blood products were infused to liver trauma patients to correct coagulopathy according to the results of TEG which could have resulted in a shorter time to correct coagulopathy.The appropriate correction of coagulopathy promotes the formation of blood clotting for hemostasis.
During operation,measures to rapidly control bleeding are essential.Methods to control damage with liver packing and staged re-operation have become standard treatment in patients requiring emergent laparotomy for severe liver trauma.[27]Perihepatic packing controls profuse hemorrhage in up to 80% of patients undergoing laparotomy.[28,29]In this study,all 11 patients who underwent operation received hepatic packing,and bleeding was controlled in 8 (72.7%) of them.
Some studies[4,30]reported that the complication rates of liver trauma were low in most series of blunt liver injury,ranging from 0 to 7%.However,as the majority of patients in those studies had lower grade liver traumas,the findings cannot be extrapolated to patients with high grade lesions.In the current series,80.6% (50/62) of grade III-V and all patients with grade I-II liver trauma underwent NOM without complications.The complication rates were 10.0% and 45.5% in the patients who underwent NOM and surgical treatment,respectively.Li Petri et al[31]reported a series of 53 patients with complex liver trauma,in which 29 patients underwent operation and 24 patients were treated conservatively.No patients who underwent NOM had complications,whereas 7 subjects (29.2%) who were surgically treated had liver related complications,including 4 bile leaks and 3 intra-abdominal abscesses.The complication rate of surgical treatment was higher than that of NOM.The patients who received operation had a higher probability of hemodynamic instability and a higher grade of liver injury than those who received NOM.Perioperative contamination might lead to abscess.
In the current study,aside from 9 patients with hemodynamic instability who underwent emergent operation,72 patients (88.9%) received NOM with a success rate of 97.2%.The results of NOM for isolated liver trauma were excellent.We consider that:(1)NOM could and should be used in not only mild,but also moderate to severe liver trauma patients with hemodynamic stability; (2) The grade of liver injury and the volume of hemoperitoneum are not suitable criteria for selecting NOM; (3) Bleeding in cases of severe liver trauma is frequently accompanied by life-threatening complications.HAE combined with correction of hypothermia,coagulopathy and acidosis are important aspects of the conservative treatment for liver trauma.
Acknowledgement:The authors thank Mr.Zhen-Guo Zhao for his assistance with data collection.
Contributors:LJS and LN proposed the study.LM performed research and wrote the first draft.YWK,WXB and JW collected and analyzed the data.All authors contributed to the design and interpretation of the study and to further drafts.LN is the guarantor.
Funding:None.
Ethical approval:This retrospective study was approved by Medical Ethics Committee of Jinling Hospital.
Competing interest:No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
1 Yanar H,Ertekin C,Taviloglu K,Kabay B,Bakkaloglu H,Guloglu R.Nonoperative treatment of multiple intraabdominal solid organ injury after blunt abdominal trauma.J Trauma 2008;64:943-948.
2 Chen RJ,Fang JF,Lin BC,Hsu YP,Kao JL,Chen MF.Factors determining operative mortality of grade V blunt hepatic trauma.J Trauma 2000;49:886-891.
3 Pringle JH.V.Notes on the arrest of hepatic hemorrhage due to trauma.Ann Surg 1908;48:541-549.
4 Velmahos GC,Toutouzas KG,Radin R,Chan L,Demetriades D.Nonoperative treatment of blunt injury to solid abdominal organs:a prospective study.Arch Surg 2003;138:844-851.
5 Stein DM,Scalea TM.Nonoperative management of spleen and liver injuries.J Intensive Care Med 2006;21:296-304.
6 Tai NR,Boffard KD,Goosen J,Plani F.A 10-year experience of complex liver trauma (Br J Surg 2002; 89:1532-1537).Br J Surg 2003;90:486-487.
7 Croce MA,Fabian TC,Menke PG,Waddle-Smith L,Minard G,Kudsk KA,et al.Nonoperative management of blunt hepatic trauma is the treatment of choice for hemodynamically stable patients.Results of a prospective trial.Ann Surg 1995;221:744-755.
8 Parks RW,Chrysos E,Diamond T.Management of liver trauma.Br J Surg 1999;86:1121-1135.
9 Bender JS,Geller ER,Wilson RF.Intra-abdominal sepsis following liver trauma.J Trauma 1989;29:1140-1145.
10 Bender JS,Levison MA.Death following non-operative management of blunt liver trauma.Injury 1991;22:418-419.
11 Moore EE,Cogbill TH,Jurkovich GJ,Shackford SR,Malangoni MA,Champion HR.Organ injury scaling:spleen and liver (1994 revision).J Trauma 1995;38:323-324.
12 Hébert PC,Wells G,Blajchman MA,Marshall J,Martin C,Pagliarello G,et al.A multicenter,randomized,controlled clinical trial of transfusion requirements in critical care.Transfusion Requirements in Critical Care Investigators,Canadian Critical Care Trials Group.N Engl J Med 1999;340:409-417.
13 Finkelstein RA,Alam HB.Induced hypothermia for trauma:current research and practice.J Intensive Care Med 2010;25:205-226.
14 Stylianos S.Evidence-based guidelines for resource utilization in children with isolated spleen or liver injury.The APSA Trauma Committee.J Pediatr Surg 2000;35:164-169.
15 Tinkoff G,Esposito TJ,Reed J,Kilgo P,Fildes J,Pasquale M,et al.American Association for the Surgery of Trauma Organ Injury Scale I:spleen,liver,and kidney,validation based on the National Trauma Data Bank.J Am Coll Surg 2008;207:646-655.
16 Navsaria PH,Nicol AJ,Krige JE,Edu S.Selective nonoperative management of liver gunshot injuries.Ann Surg 2009;249:653-656.
17 Petrowsky H,Raeder S,Zuercher L,Platz A,Simmen HP,Puhan MA,et al.A quarter century experience in liver trauma:a plea for early computed tomography and conservative management for all hemodynamically stable patients.World J Surg 2012;36:247-254.
18 Scollay JM,Beard D,Smith R,McKeown D,Garden OJ,Parks R.Eleven years of liver trauma:the Scottish experience.World J Surg 2005;29:744-749.
19 Duane TM,Como JJ,Bochicchio GV,Scalea TM.Reevaluating the management and outcomes of severe blunt liver injury.J Trauma 2004;57:494-500.
20 Becker CD,Mentha G,Terrier F.Blunt abdominal trauma in adults:role of CT in the diagnosis and management of visceral injuries.Part 1:liver and spleen.Eur Radiol 1998;8:553-562.
21 Poletti PA,Mirvis SE,Shanmuganathan K,Killeen KL,Coldwell D.CT criteria for management of blunt liver trauma:correlation with angiographic and surgical findings.Radiology 2000;216:418-427.
22 Hoff WS,Holevar M,Nagy KK,Patterson L,Young JS,Arrillaga A,et al.Practice management guidelines for the evaluation of blunt abdominal trauma:the East practice management guidelines work group.J Trauma 2002;53:602-615.
23 Fang JF,Chen RJ,Wong YC,Lin BC,Hsu YB,Kao JL,et al.Pooling of contrast material on computed tomography mandates aggressive management of blunt hepatic injury.Am J Surg 1998;176:315-319.
24 Jurkovich GJ,Greiser WB,Luterman A,Curreri PW.Hypothermia in trauma victims:an ominous predictor of survival.J Trauma 1987;27:1019-1024.
25 Reikvam H,Steien E,Hauge B,Liseth K,Hagen KG,St?rkson R,et al.Thrombelastography.Transfus Apher Sci 2009;40:119-123.
26 Karakoc D,Hamaloglu E,Ozdemir A,Dogrul A,Ozenc A.The effect of hepatectomy on coagulation:an evaluation by thromboelastography.Eur J Gastroenterol Hepatol 2010;22:43-48.
27 Carmona RH,Peck DZ,Lim RC Jr.The role of packing and planned reoperation in severe hepatic trauma.J Trauma 1984;24:779-784.
28 Nicol AJ,Hommes M,Primrose R,Navsaria PH,Krige JE.Packing for control of hemorrhage in major liver trauma.World J Surg 2007;31:569-574.
29 Tugnoli G,Casali M,Villani S,Biscardi A,Borrello A,Baldoni E.The "damage control" in severe hepatic injuries:our experience.Ann Ital Chir 2003;74:529-534.
30 Pachter HL,Knudson MM,Esrig B,Ross S,Hoyt D,Cogbill T,et al.Status of nonoperative management of blunt hepatic injuries in 1995:a multicenter experience with 404 patients.J Trauma 1996;40:31-38.
31 Li Petri S,Gruttadauria S,Pagano D,Echeverri GJ,Di Francesco F,Cintorino D,et al.Surgical management of complex liver trauma:a single liver transplant center experience.Am Surg 2012;78:20-25.
 Hepatobiliary & Pancreatic Diseases International2014年5期
Hepatobiliary & Pancreatic Diseases International2014年5期
- Hepatobiliary & Pancreatic Diseases International的其它文章
- Lymphoepithelial cysts of the pancreas:a management dilemma
- WNT5A modulates cell cycle progression and contributes to the chemoresistance in pancreatic cancer cells
- Prognostic significance of epidermal growth factor-like domain 7 in pancreatic cancer
- Post-pancreaticoduodenectomy hemorrhage:risk factors,managements and outcomes
- Laparoscopic liver resection under hemihepatic vascular in flow occlusion using the lowering of hilar plate approach
- Long-term results of liver transplantation for over 60 years old patients with hepatitis B virus-related end-stage liver disease