
Antibiotic resistance and molecular typing of clinical Staphylococcus aureus isolates from Malaysian military hospital
2023-06-26 09:37:00NorSyazaSyahirahAmatJunaidiNikNoorulShakiraMohamedShakrinMohammadFahmiDamanHuriAhmadZakwanKamarudinMohdNasirMohdDesaWanMohdZinWanYunus
Nor Syaza Syahirah Amat Junaidi, Nik Noorul Shakira Mohamed Shakrin,2?, Mohammad Fahmi Daman Huri,Ahmad Zakwan Kamarudin, Mohd Nasir Mohd Desa, Wan Mohd Zin Wan Yunus
1Faculty of Medicine and Defence Health, Universiti Pertahanan Nasional Malaysia (UPNM), Kem Sungai Besi, 57000 Sungai Besi, Kuala Lumpur,Malaysia
2Centre for Tropicalization (CENTROP), Universiti Pertahanan Nasional Malaysia (UPNM), Kem Sungai Besi, 57000 Sungai Besi, Kuala Lumpur,Malaysia
3Pathology Department, Tuanku Mizan Armed Forces Hospital (TMAFH), 53300 Kuala Lumpur, Malaysia
4Faculty of Medicine and Health Sciences, Universiti Sains Islam Malaysia (USIM), Persiaran Ilmu, Putra Nilai, 71800 Nilai, Negeri Sembilan,Malaysia
5Department of Biomedical Science, Faculty of Medicine and Health Sciences, Universiti Putra Malaysia, 43400 Serdang, Selangor, Malaysia
6Faculty of Defence Science and Technology, Universiti Pertahanan Nasional Malaysia (UPNM), Kem Sungai Besi, 57000 Sungai Besi, Kuala Lumpur, Malaysia
ABSTRACT Objective: To determine the antibiotic resistance profile (ARP)of Staphylococcus (S.) aureus isolates and molecular typing of the methicillin-resistant S.aureus (MRSA) isolates from Tuanku Mizan Armed Forces Hospital (TMAFH), Kuala Lumpur.Methods: The ARP and presence of the pvl gene were determined for 209 S.aureus isolates from clinical specimens.Of these, 123 were methicillin-susceptible S.aureus (MSSA) isolates and 86 were MRSA isolates.All MRSA isolates were characterized using SCCmec typing and spa typing.Descriptive analysis was performed to compare the demographic data with the phenotypic and genotypic variables of the S.aureus isolates.Results: No vancomycin-intermediate and -resistant S.aureus(VISA and VRSA, respectively) were detected among the study isolates.The MSSA isolates showed low resistance rates to all tested antibiotics, were commonly invasive (28/42, 66.7%), and mostly harboured pvl (35/42, 83.3%).Meanwhile, MRSA isolates showed high resistance to penicillin (86/86, 100%), ampicillin (86/86,100%), sulbactam/ampicillin (86/86, 100%), cefuroxime (81/86,94.19%), cefoperazone (76/86, 88.37%), azithromycin (56/86,65.12%), and erythromycin (54/86, 62.79%).The majority of MRSA isolates were of SCCmec type IVh (65/86, 75.58%), spa type t032(55/85, 63.95%), and grouped into spaCC-t022 (66/85, 77.65%).The t032 type was found to be associated with resistance traits to azithromycin and erythromycin (P<0.05).We also found several spa types that are typically associated with hospital-, community-, and livestock-associated MRSA co-existing in our MRSA population.Conclusions: This study reflected the consistent absence of VISA and VRSA and corroborated the clonal shifting of MRSA isolates in the Malaysian MRSA isolates.
Keywords: Staphylococcus aureus; Methicillin-resistant Staphylococcus aureus; spa typing; SCCmec typing; Antibiotic resistance
1.Introduction
Staphylococcus (S.) aureus is a Gram-positive bacterium known as the normal flora and a human pathogen that causes mild to life-threatening infections such as skin and soft tissue infections(SSTIs) and toxic shock syndrome[1].One of the important toxins is Panton-Valentine leucocidin (PVL), composed of bicomponent,LukS-PV and LukF-PV, encoded by the lukF-PV and lukS-PV genes, respectively.These two components are secreted before they assemble on neutrophil membranes to form a pore-forming heptamer, leading to neutrophil lysis.The toxin is usually linked to SSTIs, community-acquired infections, recurrent infection without predisposing factors, and severe infections, such as necrotising pneumonia and severe musculoskeletal infection[2].
One key feature that renders S.aureus infection a major concern is its ability to acquire resistance to antibiotics.Methicillin-resistant S.aureus (MRSA) is a strain of S.aureus that has become resistant to methicillin and other beta-lactam antibiotics and is usually multidrugresistant.There are difficulties in the treatment of MRSA infections in hospitals due to the limited antibiotic options.Vancomycin has been the drug of choice in the treatment of MRSA infections.Unfortunately, due to its extensive usage, there were reports of the emergence of MRSA isolates that have reduced susceptibility to vancomycin[1].The MRSA can be classified as hospital-acquired MRSA (HA-MRSA) or community-acquired MRSA (CA-MRSA)based on the acquisition mode.The presence of mobile genetic elements in S.aureus, particularly MRSA, reflects the high pace of their changing epidemiology, putting pressure on the demand for accurate and rapid clonal dissemination investigations.Molecular epidemiology offers insights into the origin and distribution of infection through the molecular classification method[3].These criteria are important for monitoring the local MRSA population,allowing epidemiologists and their clinical counterparts to devise an effective infection control and prophylaxis strategy.
Dissemination of S.aureus from the military establishment to the civilian community or vice versa imposed a serious healthcare burden as well as an operational burden, particularly because of the high cost of treatment and the impaired operational preparedness of the military.Military personnel are at increased risk of staphylococcal diseases because they have a greater risk of harm or injury due to the nature of their work or activities.In addition, they are at increased risk of staphylococcal diseases due to their close proximity in barracks and deployments to areas with endemic diseases.Thus,epidemiological antibiotic susceptibility profiles and molecular typing are important to identify the prevalence of specific S.aureus clones and determine their resistance patterns for disease prevention and control measures.However, information on the phenotypic and genotypic characteristics of clinical S.aureus from a military hospital in Malaysia remains scarce.Therefore, this study investigated the antibiotic susceptibility profile and genetic characteristics of S.aureus strains isolated from clinical samples at the Tuanku Mizan Armed Forces Hospital (TMAFH), Kuala Lumpur.The associations between the S.aureus antibiotic susceptibility profile, genetic characteristics, specimen site of isolation, and patient demographic data were also investigated.
2.Materials and methods
2.1.Isolates
Frozen clinical isolates of S.aureus from January 2019 to December 2019 were obtained from various isolation sites of patients admitted to the TMAFH, Kuala Lumpur.The TMAFH in Wangsa Maju spans 40 acres of land.It can accommodate up to 282 inpatients of the Malaysian Armed Forces and their immediate families.This ultramodern military hospital is owned and operated by the Ministry of Defence (MoD) of Malaysia.The complete clinical provenance of the isolates was not available except for the patient’s age, type of acquisition, and isolation sites.Invasive isolates were those obtained from sterile sites (blood, tracheal aspirate, pleural fluid, tissue,intravenous catheter, bone, and breast aspirate).The remaining were classified as non-invasive isolates (wound and pus, umbilicus swab,high vaginal swab, urine, nasal swab, throat swab, and eye swab).
A positive culture collected more than 48 hours after hospitalisation,a history of prior hospitalisation, or a history of medical operations are all considered indicators of HA-MRSA.Meanwhile, CA-MRSA is defined as MRSA cases without risk factors related to healthcare obtained within 48 hours of admission.
All S.aureus strains were identified using standard bacteriological methods.Isolates were subcultured on Columbia agar with 5% defibrinated sheep blood and incubated overnight at 37 ℃.Biochemical tests such as mannitol fermentation, catalase test, coagulase test,DNase production, and Gram stain were used for the identification of S.aureus.S.aureus ATCC 25923 and S.epidermidis ATCC 12228 were used as positive and negative controls, respectively, for the phenotypic identification of S.aureus.
2.2.Antibiotic susceptibility testing (AST)
Antibiotic susceptibility testing (AST) of the isolates was done on Muller Hinton agar (MHA, Oxoid, UK) using the disc diffusion method or Kirby-Bauer’s method, as described by the Clinical Laboratory Standard Institute (CLSI) using standard antimicrobial discs (Oxoid, UK).Isolates with an inhibition zone of ≤21 mm diameter around the cefoxitin (30 μg) disc were considered MRSA strains.Susceptibilities to ampicillin (10 μg), azithromycin (15 μg), ampicillin/sulbactam (10 μg/10 μg), cefoperazone (75 μg), cefuroxim (30 μg), fusidic acid (10 μg), rifampin (5 μg),clindamycin (2 μg), erythromycin (15 μg), gentamycin (10 μg),linezolid (30 μg), vancomycin (30 μg), oxacillin (1 μg), and penicillin (10 μg) were determined respectively.The zone sizes were measured and interpreted according to CLSI guidelines.S.aureus ATCC 25923 and S.aureus (MRSA) ATCC 33591 were used as quality control strains.
2.3.Genomic DNA extraction
Prior to subsequent molecular procedures, genomic DNA of the bacterial strains was extracted using GF-1 Bacterial DNA Extraction Kit (Vivantis Technologies, Malaysia) and the Biospin Bacteria Genomic DNA Extraction Kit (Bioer Technologies, China)according to the manufacturers’ instructions.
2.4.Genetic confirmation of S.aureus, MRSA, and detection of pvl
All S.aureus isolates underwent DNA amplification of the Staphylococcus genus-specific 16S rRNA gene and the S.aureus species-specific nuc gene for genetic confirmation of S.aureus and the presence of the mecA gene for genetic confirmation of MRSA.These amplifications were done using multiplex PCR primers and protocols, as described by Zhang et al[4].The details of primer pairs and their use to amplify the appropriate target gene were listed in Table 1.Multiplex PCR amplification of the 16S rRNA gene, nuc,and mecA was performed in a final volume of 20 μL containing 1 μL of DNA template (approximately 20 ng), 1.25 μM of each 16S rRNA primer, 1.25 μM of each nuc primer, 0.5 μM of each mecA primer, 10 μL of commercial PCR mastermix, and 6 μL of nuclease-free water.The presence of pvl was determined by PCR using published primers from the same report pvlF (5’ATCATTAGGTAAAATGTCTGGAC ATGATCCA-3’) and pvlR (5’-GCATCAAGTGTATTGGATAGCA AAAGC-3’) yielding a 433 bp PCR product.The PCR amplification of the gene was performed in a final volume of 20 μL containing 1 μL of DNA template (approximately 20 ng), 0.25 μM of each primer, 10 μL of commercial PCR mastermix, and 8 μL of nucleasefree water.The thermal cycling conditions were set at initial DNA denaturation at 94 ℃ for 1 minute, followed by 30 cycles of 94 ℃for 30 seconds, 60 ℃ for 30 seconds, and 72 ℃ for 45 seconds, with a final extension at 72 ℃ for 60 seconds.All PCR products were electrophoresed on a 2% agarose gel with ViSafe Red Gel Stain(Vivantis Technologies) for 90 min at 75 V.

Table 1.List of primers used for genetic confirmation of methicillinsusceptible Staphylococcus aureus and methicillin-resistant Staphylococcus aureus.
2.5.SCCmec typing and spa typing
All MRSA strains were typed using SCCmec and spa typing.S.aureus ATCC 700699 was used as an internal control for the typing methods.SCCmec typing was determined using multiplex PCR[5].PCR and sequences of the X region of the spa gene published in previous work were used to determine the spa type of the MRSA isolates[6].The spa types were then deduced using the spa typing plugin of the Ridom SeqSphere+ v6.0.2 software (Ridom, Germany).
2.6.Association between antibiotic susceptibility profile,genetic characteristics, specimen site of isolation, and patient demographic data
The Statistical Package for the Social Sciences (SPSS) software(version 26.0) was used for data analysis.The comparison of variables, such as the isolates’ phenotypic and genotypic characteristics, the patient’s age, the site of isolation, and the type of acquisition, was determined by Chi-square or Fisher's exact tests,where appropriate.The P value of < 0.05 (two-tailed) was taken as the significance level.A minimum spanning tree (MST) was constructed using the Ridom SeqSphere+ v6.0.2 software (Ridom,Germany) based on the spa sequences of the isolates.The obtained spa types were clustered if the cost was less than or equal to 4,and spa types with fewer than four repeats were excluded from the analysis.
3.Results
3.1.Isolates
A total of 209 S.aureus isolates were successfully recovered and viable.The demographic data of patients from TMAFH infected with S.aureus are tabulated in Table 2.The mean age of patients with S.aureus infections was (51.7±18.8) years, ranging from 14 days to 90 years.

Table 2.Comparative analysis of the Staphylococcus aureus strains between the patient’s demographic data, site of infection, and infection acquisition with antibiotic susceptibility pattern and methicillin susceptibility.
The scope of the study was based solely on the patient’s demographic data, isolation site, type of acquisition, and phenotypic and genotypic profiles of the isolates.The phenotypic characteristics include an antibiotic susceptibility profile, methicillin susceptibility,and a multidrug resistance pattern.Meanwhile, the genotypic characteristics include the presence of mecA, pvl, SCCmec type, and spa type.Isolates obtained from sterile sites (blood, tracheal aspirate,pleural fluid, tissue, intravenous catheter, and breast aspirate) were accumulated as isolates of the invasive site (110/209, 52.6%), while the remaining isolates from other sites were considered non-invasive isolates (99/209, 47.4%).
Based on the criteria suggested by the Centres for Disease Control and Prevention (CDC)[7], 16 out of 209 (7.7%) S.aureus isolates were hospital-acquired, and the remaining (193/209, 92.3%) were community-acquired.S.aureus infections were most common in patients aged 41 and above (155/209, 74.2%) and in men (139/209,66.5%).
3.2.Antibiotic susceptibility testing (AST) profile
The AST results showed that all isolates were susceptible to linezolid and vancomycin.Among the isolates, the study documented the highest resistance rates to penicillin, ampicillin and sulbactam/ ampicillin (86/209, 41.1%), and all of these isolates were phenotypically and genetically confirmed as MRSA based on cefoxitin susceptibility and mecA gene detection.The remaining 123 isolates (58.9%) were MSSA.A percentage of 39.2% (82/209) of S.aureus isolates were resistant to cefuroxime, followed by those resistant to cefoperazone (77/209, 36.8%), azithromycin (61/209,29.2%), erythromycin (58/209, 27.8%), fusidic acid (31/209, 14.8%),gentamycin (25/209, 12.0%), and rifampicin (5/209, 2.4%).Figure 1 shows the antibiotic resistance and rate of multidrug resistance of the MSSA and MRSA isolates.About 33 out of 209 (15.8%) of the S.aureus isolates were non-susceptible to at least one of three or more antimicrobial categories, defined as multidrug-resistant (MDR).All MDRs in this study were MRSA isolates (33/86, 38.4%).Apart from being susceptible to linezolid and vancomycin, the MSSA isolates (33/86, 38.3%) in the current study were also susceptible to penicillin, ampicillin, sulbactam/ampicillin, gentamycin, and rifampicin.

Figure 1.The proportion of antibiotic resistance and multidrug resistance(%) of the clinical Staphylococcus aureus isolates from Tuanku Mizan Armed Forces Hospital.MSSA: Methicillin-susceptible Staphylococcus aureus,MRSA: Methicillin-resistant Staphylococcus aureus, AMP: ampicillin,PEN: penicillin, SAM: sulbactam/ampicillin, CFP: cefoperazone.CXM:cefuroxime, AZM: azithromycin, ERY: erythromycin, CLI: clindamycin,FUS: fusidic acid, GEN: gentamycin, LNZ: linezolid, VAN: vancomycin,MDR: multidrug resistant.
The association of S.aureus strains based on the patient’s demographic data, isolation site, type of acquisition, antibiotic resistance pattern, and methicillin susceptibility were tabulated in Table 2.The MDR isolates were statistically more common in patients aged 41 and above,(χ2=5.375, P=0.017).Meanwhile, no significant association is found between MDR S.aureus with isolates from invasive sites and type of acquisition.The MRSA isolates were statistically common in patients aged 41 and above (χ2=5.375,P=0.020) and CA infections (χ2=24.781, P<0.001).
Then, MRSA isolates were further stratified into HA-MRSA and CA-MRSA for comparative analysis according to the patient’s demographic data, site of infection, and antibiotic pattern amplification using the Fisher's exact test (Table 3).No significant relationship was detected between the parameters and the types of MRSA (HA-MRSA and CA-MRSA isolates).
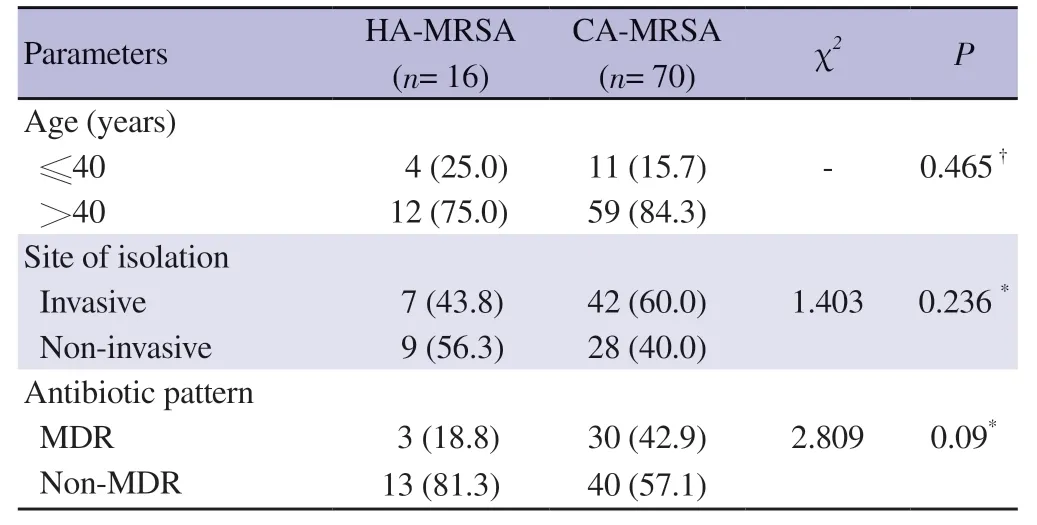
Table 3.Comparative analysis of the CA-MRSA and HA-MRSA isolates in relation to the patient’s demographic data, site of isolation, and antibiotic pattern.
3.3.Distribution of pvl
Interestingly, 42 of the 209 isolates (20.1%) harbour the pvl (pvl+)gene.Most of the pvl+ isolates were isolated from patients aged above 40 (23/42, 54.8%), non-invasive site (28/42, 66.7%), non-MDR (40/42, 95.2%), and MSSA (35/42, 83.3%), with significant associations, respectively (Table 4 and Table 5).Further investigation of the isolation sites revealed that all non-invasive sites of the pvl+isolates were from wound and pus specimens (28/42, 66.7%).A significant association of the presence of pvl with CA infection(40/42, 95.2%) was recorded (χ2=4.807, P=0.028).

Table 4.Distribution of pvl amplification among Staphylococcus aureus clinical isolates from Tuanku Mizan Armed Forces Hospital based on the patient’s demographic data, isolation site invasiveness, and infection acquisition.

Table 5.Distribution of pvl amplification among Staphylococcus aureus clinical isolates from Tuanku Mizan Armed Forces Hospital.
3.4.Molecular typing based on SCCmec typing and spa typing
All MRSA strains were successfully typed using the SCCmec typing method.Almost all MRSA isolates were SCCmec typeⅣ (85/86, 98.8%), and only one isolate was SCCmec type Ⅲ.Meanwhile, 90.6% (77/85) of the SCCmec type Ⅳ were subtyped SCCmec type Ⅳh, while the remaining were of subtype Ⅳa.
Table 6 summarises the distribution of spa types of MRSA from this study.A total of nine spa types were discovered from 85 MRSA isolates.The t032 strain (55/86, 64.0%) predominates the MRSA isolates in this study.The X region of the spa gene remained undetected in one of the MRSA isolates despite multiple attempts of spa gene amplification.The SCCmec type Ⅲ from an isolate in this study was spa typed as t421.Concurrently, 66 MRSA isolates (77.6%) were grouped into a cluster with spa type t022 as the founder, or spaCC-t022, and 19 isolates (22.1%) were evaluated as singletons (Figure 2).
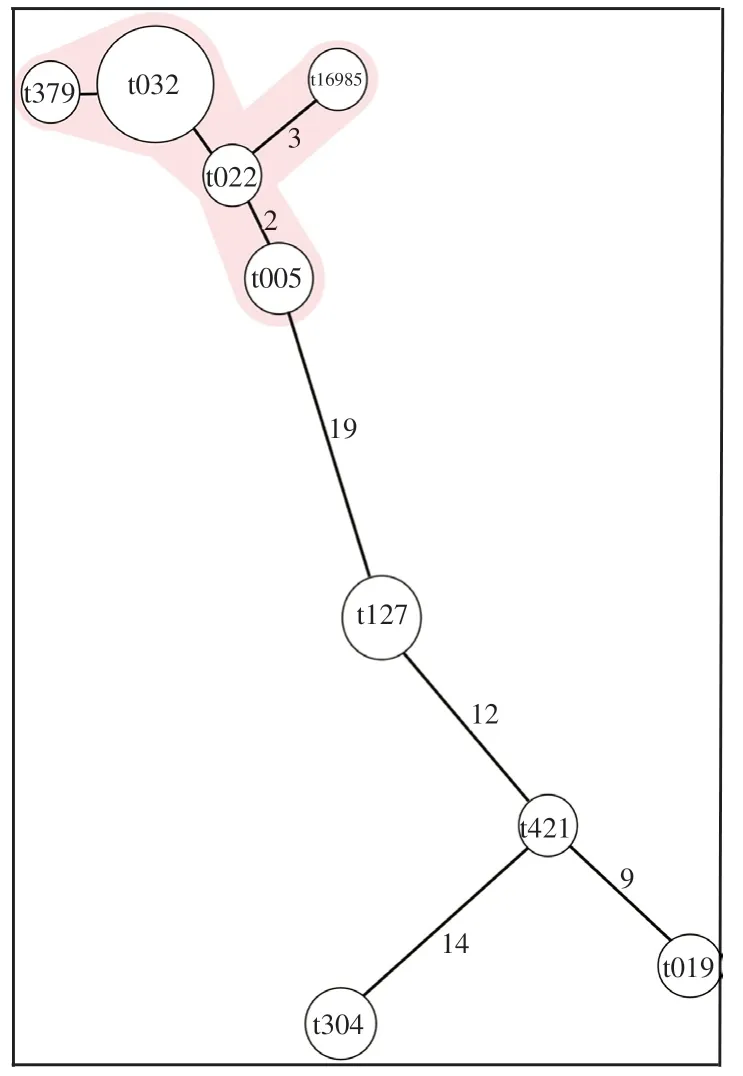
Figure 2.Minimum spanning tree (MST) of the clinical methicillinresistance Staphylococcus aureus isolates from Tuanku Mizan Armed Forces Hospital.Each node represents a spa type; the size of the circle represents the number of isolates assigned to each spa type, and the number at the branch indicates the distance.The associated clonal complex (CC) is displayed in pink shading.

Table 6.Genetic characteristics of the methicillin-resistant Staphylococcus aureus isolates in relation to antibiotic susceptibilities.
Strain t032 in this study colonised many specimens (blood,bone, nasal swab, throat swab, tissue, wound, and pus) and showed no association with any specific site when the data were analysed using the Fisher's exact test (P=0.743).Other spa types that were also grouped in spaCC-t022 also showed a similar distribution concerning the site of isolation, except in the lower extent (t005 isolated from tissue and wound and pus; t022 from bone, tracheal aspirate, and wound and pus cultures; and t16385 from tissue and wound and pus cultures).All isolates with spa types t127 and t304 were found in blood specimens only, while all t019 isolates were found in wound and pus sites.
The predominant MRSA strain, t032, showed high resistance to cefoperazone, cefuroxime, azithromycin, and erythromycin.The t304, t005, and t16985 isolates were mostly MDR.Meanwhile, almost half of the t032 strains (22/55, 40.0%) were MDR.The pvl+ MRSA is observed in t005 (4/7, 57.1%), and t019 (3/7, 42.9%).Table 6 tabulates the proportions of SCCmec type and spa type based on antibiotic resistance rate and pvl.
3.5.Clonality analysis of MRSA spa type t032
The clonal similarity of the largest spa-type portion of the spaCC-t022 (SCCmec Ⅳh-t032) was investigated.Based on the antibiotic resistance profile, all SCCmec Ⅳh-t032 strains can be classified into four distinct groups (Figure 3).GroupⅠis resistant to a combination of ampicillin, sulbactam/ampicillin,penicillin, cefoperazone, and cefuroxime; GroupⅡis resistant to ampicillin, sulbactam/ampicillin, penicillin, cefoperazone,cefuroxime, azithromycin, and erythromycin; GroupⅢis resistant to ampicillin, sulbactam/ampicillin, penicillin,cefoperazone, cefuroxime, azithromycin, erythromycin, and fusidic acid; and GroupⅣis resistant to ampicillin, sulbactam/ampicillin, penicillin, cefoperazone, cefuroxime, azithromycin,erythromycin, and gentamycin.GroupsⅠandⅡhave a wide range of isolation sites, while most of those GroupⅢcome from wounds and pus, and Group Ⅳ is mainly from blood.Group I comprises an almost equal level of HA-MRSA and CA-MRSA,GroupⅡleans more towards CA-MRSA, while GroupsⅢandⅣ are all CA-MRSA.

Figure 3.Detailed characteristics of the t032 strains based on the antibiotic resistance profile, presence of pvl, site of isolation, and type of acquisition.Stratification of the t032 based on antibiotic resistant profile produced significant GroupⅠ,Ⅱ,Ⅲ, and Ⅳ.AMP: ampicillin, PEN: penicillin, SAM:sulbactam/ampicillin, CFP: cefoperazone, CXM: cefuroxime, AZM: azithromycin, ERY: erythromycin, CLI: clindamycin, FUS: fusidic acid, GEN:gentamycin, pvl: Panton-Valentine leucocidin gene, HA: hospital-acquired, CA: community-acquired.
4.Discussion
The risks of S.aureus colonisation and infection, particularly SSTI,are known to be high in the military cohort due to the crowded living conditions, inadequate personal hygiene, skin injury, environmental contamination, and a misunderstanding of the skin wound aetiology[8].Being the main referral hospital for nationwide military healthcare facilities, the patient population of TMAFH comprises a high number of military personnel than the public and tertiary hospitals.Although military service members are mainly circulated among civilians, i.e., living in the same residential area as civilians,molecular studies involving S.aureus isolates from military hospitals are of interest due to the scarce studies in Malaysia.Hence, the S.aureus isolates in this study can be compared with S.aureus isolates from other public and tertiary studies.
The World Health Organisation (WHO), in their 2014 report, stated that the proportion of MRSA in hospitals exceeds 20% in all WHO regions.Likewise, a military hospital in another country reported that 74.6% of its wound infections were caused by S.aureus[9].The National Surveillance of Antibiotic Resistance Report (NSAR)reported an increase in MRSA infection rate from 18% in 2016 to 19.8% in 2017 in several hospitals and laboratories in Malaysia and a steadily decreasing rate in recent years from 19.4% in 2018 to 14.9% in 2020[10].
In the current study, MRSA accounted for 41.1% of S.aureus infections.The data are consistent with previous findings that the frequency of MRSA in Malaysia ranges from 17% to 44.1%[11,12],and the MRSA rate of the global military hospitals and healthcare facilities ranges from 23.2% to 50.0%[13,14].In contrast, the national MRSA rate for the same year of this study, i.e., 2019, was reported at a much lower frequency, i.e., 15.0%[15].The variation in MRSA prevalence may be attributed to different sampling strategies,sample sizes, study populations, interpretation protocols, antibiotic use, and bacteriological procedures.Nevertheless, all target genes were consistent with their phenotypic identification of the isolates in the molecular confirmation of S.aureus and MRSA.Methicillin resistance among the S.aureus isolates in this study was caused by the presence of mecA.
Almost half (42.6%) of the S.aureus in this study were isolated from wound and pus specimens.The findings are similar to a recent study on isolates from a hospital on the east coast of Peninsular Malaysia, where most S.aureus isolates were from pus specimens(67.7%)[16].However, the 2019 NSAR report stated that the national S.aureus infection was mainly from the blood, albeit at a much lower (20.2%) prevalence, which is contradictory to this study[15].The variation might be attributed to the higher burden of the participating hospitals and laboratories in terms of the number of patients and infection severity.A readily exclusive patient population of the military hospital with a less severe infection may have been treated at the primary care level, contributing to fewer superficial infections requiring treatment from the secondary and tertiary treatment facilities.Consequently, this study reported similar results to the national report, where most MRSA was isolated from blood.
S.aureus could spread throughout the hospital and community.In this study, S.aureus, including MRSA, was largely isolated from the community (92.3% and 81.4%, respectively).This finding is similar to a long-term multicenter study from the United States of America(USA), where the community-onset S.aureus and MRSA isolates were higher than the hospital-onset infection[17].However, other study reported contradictory finding[18-20].
The MSSA isolates in this study showed full susceptibility to penicillin, ampicillin, and sulbactam/ampicillin and low resistance to other beta-lactam antibiotics (cefoperazone and cefuroxime,0.81%).A recent study reported that 16% of their MSSA isolates were penicillin-sensitive[20], whereas some reported a prevalence of 15.6% and less than 10%[13,21].However, the penicillin-sensitive S.aureus (PSSA) isolates in this study were not tested for minimum inhibitory concentration (MIC) of the penicillin and whether the isolate was a penicillinase-producing strain.Report on the full sensitivity of penicillin, ampicillin, and sulbactam/ampicillin among S.aureus isolates in Malaysia and elsewhere are scarce.The high sensitivity level to beta-lactam antibiotics might be due to antibiotic selective pressure caused by restricted usage of the antibiotics[17].Nonetheless, researchers have recently discovered that penicillinsusceptible MSSA prevalence, particularly in bacteraemia, is progressively growing in various countries[21].A total of 63 out of 123 of the penicillin-sensitive MSSA isolates in this study were obtained from invasive samples and 43 from blood specimens.Similarly, data on MSSA isolates resistance to cefoperazone and cefuroxime are little to none due to their rarity of usage for S.aureus prophylaxis[22].The only report on cefoperazone susceptibility was among MRSA isolates, where 86.7% of their MRSA isolates were resistant to the antibiotic.
In this study, a low number of MSSA isolates were resistant to fusidic acid (7.3%).The resistance rate was much lower than isolates of recent research, which reported a resistance rate of 17.4% to fusidic acid among their MSSA isolates[13].However, the same study found much lower resistance to fusidic acid among their MRSA isolates than the MRSA isolates in this study.Likewise, MSSA isolates from a tertiary hospital in Klang Valley have over three-fold the prevalence of fusidic acid resistance (24%) than this study[20].In addition, the national reports revealed a decreasing trend in the fusidic acid resistance rate from 2015, and the fusidic acid resistance rate of S.aureus (4.31%) in this study fit the national trend[15].
A lower resistance rate (less than 30%) to clindamycin, gentamycin,and rifampicin was seen among the MSSA and MRSA isolates.This result is similar to a study in a tertiary hospital in the Klang Valley[20].In accordance with the present results, the NSAR revealed the gradual decline of clindamycin, gentamycin, and rifampicin resistance rates from 2015 to 2019 (five-year interval)[15].
The prevalence of the pvl gene among S.aureus isolates is important as the association of the pvl gene with the severe form and recurrence of S.aureus infection has been described[23].The pvl+ S.aureus in this study was 20.1%, with significant domination in the MSSA isolates.The discovery was comparable with a study in another military hospital in Asia[24].On the contrary, the low level of pvl+(less than 10%) in the MRSA isolates is consistent with several studies from Malaysia[11,23].
The present study showed that the pvl+ phenotype was linked to non-MDR S.aureus.A study in Myanmar demonstrated that the pvl+ MSSA isolates were resistant to fewer antibiotics than the ST59 pvl- MRSA and MSSA[25].Nevertheless, the association of pvl+ S.aureus isolates being MDR was recorded in India[26], signifying that different S.aureus strains might cause the association variation due to geographical area.
Several studies associate the presence of pvl with SSTI, including in the military population[27].This study found an association between pvl+ isolates with wound and pus specimens, attributed to SSTI,and our occurrence of pvl+ (66.7%) was lower than the prevalence reported by a recent study in China involving their military hospital isolates (93.4%)[24].Another significant aspect of pvl is its association with CA infections, either MSSA or MRSA[27,28], as proven in this study.
Apart from the presentation of pvl, CA-MRSA isolates are susceptible to a wide range of antibiotics[29].It was observed that the CA S.aureus isolates from this study, including the CA-MRSA,were mostly non-MDR.However, the co-occurrence of MDR CAMRSA was noted in this study.This study supports previous findings that the once distinguishable characteristics between CA-MRSA and HA-MRSA have become indiscriminate[12].Therefore, according to some experts, antibiotic susceptibility profiles are no longer helpful for differentiating HA and CA isolates[12].Altogether, S.aureus isolates from the hospital or community settings require equal attention as both possess the ability to be MDR.
The most common SCCmec type in the current study was SCCmec type Ⅳ, specifically SCCmec type Ⅳa.Ismail et al.and Sukri et al.reported that most MRSA isolates from two hospitals in the Klang Valley were of SCCmec type Ⅳ[29,30].This could explain the dominance of SCCmec type Ⅳ in TMAFH was typically linked to CA-MRSA[31].SCCmec type Ⅳ is also the major circulating MRSA strain in Singapore due to clonal shifting from previously predominating SCCmec type Ⅲ[32].The SCCmec type Ⅳ MRSA strains have the smallest SCCmec cassettes compared to SCCmec types of HA-MRSA strain clones, with the cassette in the former having simpler genetic content, lesser antibiotic resistance genes,“tougher”, and multiply progressively[31].
The relevance of SCCmec typing lies in its ability to provide valuable information about the epidemiology and transmission of MRSA for informing infection control measures and foreseeing the antibiotic resistance pattern of the MRSA since different SCCmec types are associated with different levels of resistance to various antibiotics, SCCmec types Ⅰ, Ⅱ, and Ⅲ were mostly found in HA-MRSA isolates from around the world, whereas SCCmec types Ⅳ, Ⅴ, and Ⅶ were mostly found in CA-MRSA isolates[32].Previously, HA-MRSA and CA-MRSA could be discriminated by their characteristics, such as the latter is more susceptible to antibiotics and usually infect immunocompetent and young people.The distribution of SCCmec types from this study overlapped with the SCCmec types of HA-MRSA and CA-MRSA.The only SCCmec type Ⅲ in the current study was CA-MRSA, contradictory to the fact that SCCmec type Ⅲ is an HA-MRSA clone.In addition, 16 isolates of SCCmec type Ⅳ were assigned as HA-MRSA.This finding complicates the strategies for preventing MRSA dissemination,particularly among the community.
Altogether, the spa region was successfully amplified, except for a SCCmec Ⅳ MRSA (1.2%) isolate.The finding is similar to a spa typing study in Malaysia, where 2.7% of the MRSA isolates were assigned as non-typeable[30].The plausible causes of unsuccessful spa typing could be that mutation of the primer binding region or alteration of the IgG-binding region contained in the spa gene reduced the efficiency of the widely utilized spa primer[33].Moreover, the inability to amplify the spa region due to spa-deficient isolates led to ineffective spa typing[33].
Since the early age of MRSA molecular characterisation studies in Malaysia, t037 predominated the MRSA isolates[34].Intriguingly,the t032 replaced the t037 MRSA clones in the Malaysian hospitals.Ismail et al.and Jones et al.demonstrated that most MRSA isolates were typed as t032[16,30].Ismail et al.investigated the second phase of MRSA molecular characterisation from a tertiary hospital after an 8-year interval (2009 vs.2017)[30].They reported a temporal shift of predominating MRSA clones, from t037 in 2009 to t032 in 2017.Interestingly, this study showed that the change is persistent.Previously, the molecular transition also occurred in other countries,such as Singapore, the USA, and the United Kingdom (UK)[31].Additionally, this strain was reported as the cause of the MRSA outbreak during the COVID-19 pandemic in Germany[35], revealing that the MRSA strain is resilient amid heightened general hygiene.The consistent predomination of MRSA clone between the military hospital in our study and other public hospitals indicated that the MRSA strain was geographically associated rather than cohortdependent.Another study that studied the MRSA population in the military and public hospitals in Brazil in parallel found the similar result[36].Another possible reason is in-service and retired military personnel as well as their beneficiaries are living within the public population, hence, the findings may not exclusively represent military environment.In future work, it may be useful to study particular aspects of comparing the civilian MRSA population with an exclusive military environment.
Dissemination of MRSA global lineage is common due to intercontinental migration[37].The evaluation suggests that the obtained results were as anticipated.Several pandemic MRSAs were observed in this study, i.e., EMRSA-15 (t005) and the Southwest Pacific clone (t019).Similarly, MRSA strains proven to predominate in several countries on different continents were also detected,e.g., t127 and t022 from the European countries and t304 from the Middle-East countries[38,39].In addition to circulation in the human population, t127 was also reported in animals and animal handlers,indicating that it could act as a reservoir for the transmission of livestock-associated MRSA (LA-MRSA) strain to humans[40].These strains were proven to invade an MRSA population, become persistent, and cross species, which may eventually replace the predominant MRSA and subsequently change the environment of the MRSA in a population.Hence, continuous surveillance of MRSA clones is recommended to monitor for such events in the local setting and to help inform transdisciplinary public health policies and strategies mobilized by the One Health approach.
Different geographical regions have different antibiotic resistance profiles and molecular characteristics of MRSA strains, which further produce varied disease outcomes[18].Hence, investigation of the association between the genotype of the MRSA strains and other characteristics may contribute to the clinical prognosis of MRSA infection.The likeliness of a specific MRSA strain infection,particularly the SCCmec type Ⅳ, t032 and spaCC-t022 strains, was independent of age, antibiotic pattern, presence of pvl, specimen invasiveness, and type of infection acquisition.Previous studies have reported that MRSA strains and clinical characteristics are not associated[16].Further research into this area may be useful to validate the findings.
The t032 was isolated from various sites of isolation, and its comparison with other spa types from this study revealed no statistically significant difference in the strain with the specific site of isolation.This observation was also supported by Jones et al.[16].The same study stipulated that the strain has no affinity for specific foci of infection.
Previous studies showed that the clonal replacement of MRSA isolates was concurrent with the change in antibiotic resistance profiles of MRSA isolates[30].Therefore, different MRSA clones exhibit different antibiotic profiles.In the current study, t032 strains were significantly linked to isolates resistant to macrolide antibiotics (azithromycin and erythromycin).Despite no association being recorded, higher resistance to cephalosporin antibiotics(cefoperazone and cefuroxime) was also observed.Disregarding the resistance to beta-lactamases, half of the t032 isolates from South Africa were resistant to erythromycin, but only four out of 24 of the t032 isolates were resistant to azithromycin[32].In comparison,the MRSA t032 strain from Ismail et al.was significantly resistant to erythromycin, clindamycin, and ciprofloxacin, while the isolates from Germany had higher resistance to erythromycin, clindamycin,ciprofloxacin, and moxifloxacin[30,41].The variable antibiotic resistance profile of the t032 isolates could be attributable to phylogeographic variation and the antibiotic treatment course of the study settings.Further study on this matter, perhaps using a larger sample size, should be done to better visualize the antibiotic resistance profile exhibited by this strain.In addition, this study was limited to the data obtained from a single armed forces hospital among several others nationwide.Thus, the S.aureus characteristics may not represent the entire military cohort.
In conclusions, this study represents the first phenotypic and genotypic analysis of S.aureus infection at a major military hospital in Malaysia.Although no vancomycin-intermediate and vancomycinresistant S.aureus were detected from the clinical isolates, the strains were of CA infection.The pvl occurred mostly in the MSSA isolates, stipulating that MSSA can be virulent, considering that pvl harbouring strains were commonly associated with severe and persistent S.aureus infections.This highlights the importance of an effective infection control policy to prevent the circulation of CA infection and virulent strains within the hospital.This study found that the SCCmec IVh-t032 clone predominates the MRSA isolates,indicating that currently, the MRSA genetic environment in the military hospital is congruent to the current MRSA isolates from other Malaysian tertiary and public hospitals.The spa typing and phenotypic analysis of the MRSA also revealed the dissemination of global endemic MRSA lineage in the hospital and suggested that molecular marker is no longer relevant to distinguish HA-MRSA and CA-MRSA.The presence of LA-MRSA signifies the importance and relevance of the One Health perspective for the surveillance and management of the S.aureus infection.
Research ethics approval
This study has been reviewed and approved by the Research Ethics Committee of Universiti Pertahanan Nasional Malaysia (UPNM),with the ethics reference number UPNM/JKEP13/2020.
Conflict of interest statement
All authors report no conflict of interest.
Funding
The study was funded by the UPNM Short Term Grant(UPNM/2019/GPJP/SP/1).
Acknowledgements
The authors fully acknowledged the Ministry of Higher Education(MOHE) and UPNM for the approved funding, which made this research feasible.The authors would like to thank the technical staff at every institution involved for their assistance.
Author’s contribution
NSSMS contributed to the study’s conception and design.NSSAJ and NNSMS were involved in reviewing the definition of intellectual content and literature research.NSSAJ, NNSMS, MNMD and WMZWY were responsible for experimental studies and data analysis.NSSAJ, NNSMS, MFDH and AZK contributed to data acquisition at TMAFH.Manuscript preparation and data analysis(statistical analysis) were done by NSSAJ.Manuscript editing was done by NSSAJ and NNSMS.NSSAJ, NNSM, MFDH, AZK,MNMD and WMZWY were involved in manuscript review.All authors have read and approved the final manuscript for publishing.
 Asian Pacific Journal of Tropical Medicine2023年5期
Asian Pacific Journal of Tropical Medicine2023年5期
- Asian Pacific Journal of Tropical Medicine的其它文章
- Electrocardiographic changes in dengue fever
- Autoimmune complications and clinical outcomes of herpes simplex encephalitis in children: A case series
- Hepatitis B vaccination status and associated factors among health science students
- Faunal richness and checklist of sandflies (Diptera: Pyschodidae) in India