
Primary hepatic leiomyosarcoma: A case report and literature review
2022-10-08 05:42:44HassanAhmedHassaanBariUmerNisarSheikhMuhammadIrfanBasheer
World Journal of Hepatology 2022年9期
Hassan Ahmed, Hassaan Bari, Umer Nisar Sheikh, Muhammad Irfan Basheer
Hassan Ahmed, Hassaan Βari, Department of Surgical Oncology, Shaukat Khanum Memorial Cancer Hospital and Research Centre, Lahore 54782, Pakistan
Umer Nisar Sheikh, Muhammad lrfan Βasheer, Department of Pathology, Shaukat Khanum Memorial Cancer Hospital and Research Centre, Lahore 54782, Pakistan
Abstract BACKGROUND Primary hepatic leiomyosarcoma (PHL) is a rare tumor with a very low incidence of about 0.2%.CASE SUMMARY A 48-year-old diabetic, hypertensive, and morbidly obese female patient presented with a history of abdominal pain and weight loss for 2 mo. She had no history of fever, jaundice, or other liver disease(s). Clinical examination revealed a palpable mass in the epigastrium. Imaging evaluation with a contrast-enhanced computed tomography (CT) scan of the abdomen and pelvis revealed an illdefined enhancing hyper vascular hepatic mass of 9.9 cm × 7.8 cm occupying the left hepatic lobe with evidence of central necrosis, compression effect on the left hepatic vein, and partial wash-out on delayed images. On further workup, the maximum standardized uptake value on positron emission computed tomography scan was 6.4, which was suggestive of malignancy. The remaining part of the liver was normal without any evidence of cirrhosis. Ultrasound-guided biopsy of the mass showed smooth muscle neoplasm suggestive of leiomyos-arcoma. After optimization for co-morbidities, an extended left hepatectomy was planned in a multidisciplinary team meeting. On intraoperative ultrasound, the left hepatic lobe was entirely replaced by a large tumor extending to the caudate lobe with a compression effect on the middle and left hepatic veins. Final histopathology showed nodular and whorled white tumor comprised of spind-led/fascicular cells with moderate to severe pleomorphism and focal necrosis. The mitotic index was greater than 20 mitoses per 10 high-power fields. The resection margins were free of tumor. Immunohistochemistry (IHC) depicted a desmin-positive/ caldesmon-negative/discovered on gastrointestinal stromal tumor 1-negative/ cluster of differentiation 117-negative profile, confirming the definitive diagnosis as PHL.CONCLUSION This case report highlights the rare malignant mesenchymal hepatic tumor. To confirm PHL diagnosis, one requires peculiar histopathological findings with ancillary IHC confirmation. Management options include adequate/complete surgical resection followed by chemotherapy and/or radiotherapy.
Key Words: Leiomyosarcoma; Immunohistochemistry; Hepatectomy; Surgical resection; Case Report
lNTRODUCTlON
Primary hepatic leiomyosarcoma (PHL) is a rare mesenchymal hepatic tumor whose clinical manifestations are often nonspecific and remain asymptomatic until there is a significant increase in tumor size causing a mass effect. This manuscript presents a case report of a 48-year-old woman with PHL.
CASE PRESENTATlON
Chief complaints
A 48-year-old woman presented to the outpatient clinic with complaints of abdominal pain associated with weight loss.
History of present illness
The patient’s symptoms started 2 mo prior with recurrent episodes of abdominal pain without any specific aggravating or relieving factor(s).
History of past illness
She had no documented history of fever, jaundice, liver disease(s), blood transfusion, tattooing, or alcohol abuse.
Personal and family history
Her co-morbidities included diabetes, hypertension, and obesity. She had no family history of carcinoma.
Physical examination
On examination, there was a palpable mass in the epigastrium. The rest of the clinical examination was unremarkable, without any signs of disease elsewhere in the body.
Laboratory examinations
Complete blood count, serum biochemical profile, coagulation profile, and carbohydrate antigen 19-9 were normal. Viral serology was nonreactive.
Imaging examinations
An initial imaging evaluation with a contrast-enhanced computed tomography (CT) scan of the abdomen and pelvis showed an ill-defined heterogeneous contrast-enhancing and hyper vascular mass in the left lobe of the liver with extension up to the middle hepatic vein and compression effect on the left hepatic vein. The approximate measurement of the mass was 9.9 cm × 7.8 cm with central necrosis in the mass and partial wash-out on delayed images. The tumor encased the left portal vein branch at its point of bifurcation; however, the main portal vein and its right branch were not involved. No signs of hepatic cirrhosis were identified on imaging studies (Figure 1).
Positron emission tomography-CT (PET-CT) scan showed a maximum standardized uptake value (SUV) of the left hepatic mass of 6.4. The remaining liver had a standard baseline hepatic SUV (hepatic parenchymal baseline reference activity was up to 2.96 SUV).
No significant abnormality was seen above or below the diaphragm. In addition, the lungs, gastrointestinal (GI) tract, adrenal glands, kidneys, ovaries, and uterus did not show any evidence of primary disease or metastasis. No metastasis was found elsewhere in the body.
Ultrasound-guided biopsy was done, which showed cores of liver tissue with a proliferation of tumor cells having spindled-shaped nuclei with features of pleomorphism, up to 10 mitosis/10 high-power fields (HPFs), and necrosis. These findings suggested a spindle cell neoplasm raising a differential diagnosis of GI stromal tumor (GIST) and leiomyosarcoma. A panel of Immunohistochemical stains were applied that depicted a desmin-positive/caldesmon-negative/discovered on GIST1-negative (DOG1-)/cluster of differentiation 117-negative (CD117-) profile, thereby supporting the definitive diagnosis of PHL.
MULTlDlSClPLlNARY EXPERT CONSULTATlON
The case was discussed for management discussion in GI and hepatobiliary multidisciplinary team (MDT) meetings. According to MDT recommendations, surgical resection of the liver mass was planned, as there was no clinical and radiological evidence of metastatic disease or unknown primary disease elsewhere in the body.
FlNAL DlAGNOSlS
The definitive preoperative diagnosis of the presented case was PHL in the absence of clinical and radiological evidence of metastatic disease or unknown primary disease elsewhere in the body.
TREATMENT
A formal extended left hepatectomy was performed. Staging laparoscopy was negative for metastasis, followed by a traditional laparotomy using a Mercedes Benz incision. The total operating time was 540 min with a blood loss of 300 milliliters.
Intraoperatively, the left lobe of the liver was involved by a large tumor extending inferiorly to the caudate lobe (left side only) and superiorly up to the middle hepatic vein (MHV). MHV and its branches were sacrificed. An en bloc resection was achieved with an intact capsule (Figure 2). Resection margins were confirmed to be free of the tumor with the help of intraoperative ultrasound. Enlarged hilar nodes (hepatic artery lymph node) and periportal lymph node were also removed separately. No distant metastasis or aortocaval nodes were found per operatively.

Figure 2 Resected specimen.
Final diagnosis and histopathology
Grossly, the left hepatectomy specimen measured 18 cm × 12.5 cm × 9.5 cm. Serial slicing of the specimen revealed a tumor (10.5 cm × 7.5 cm) with a nodular and whorled white appearance. The hepatic capsule was intact without any evident perforation. The microscopic evaluation revealed a cellular tumor with a fascicular array of tumor cells having spindle-shaped nuclei with a moderate-tosevere degree of cellular pleomorphism and more than 20 mitoses per 10 HPFs. Necrosis was focally seen. Lympho vascular invasion was not identified (Figures 3 and 4). All three regional lymph nodes (hepatic artery, periportal, and gallbladder neck) were negative for metastasis.
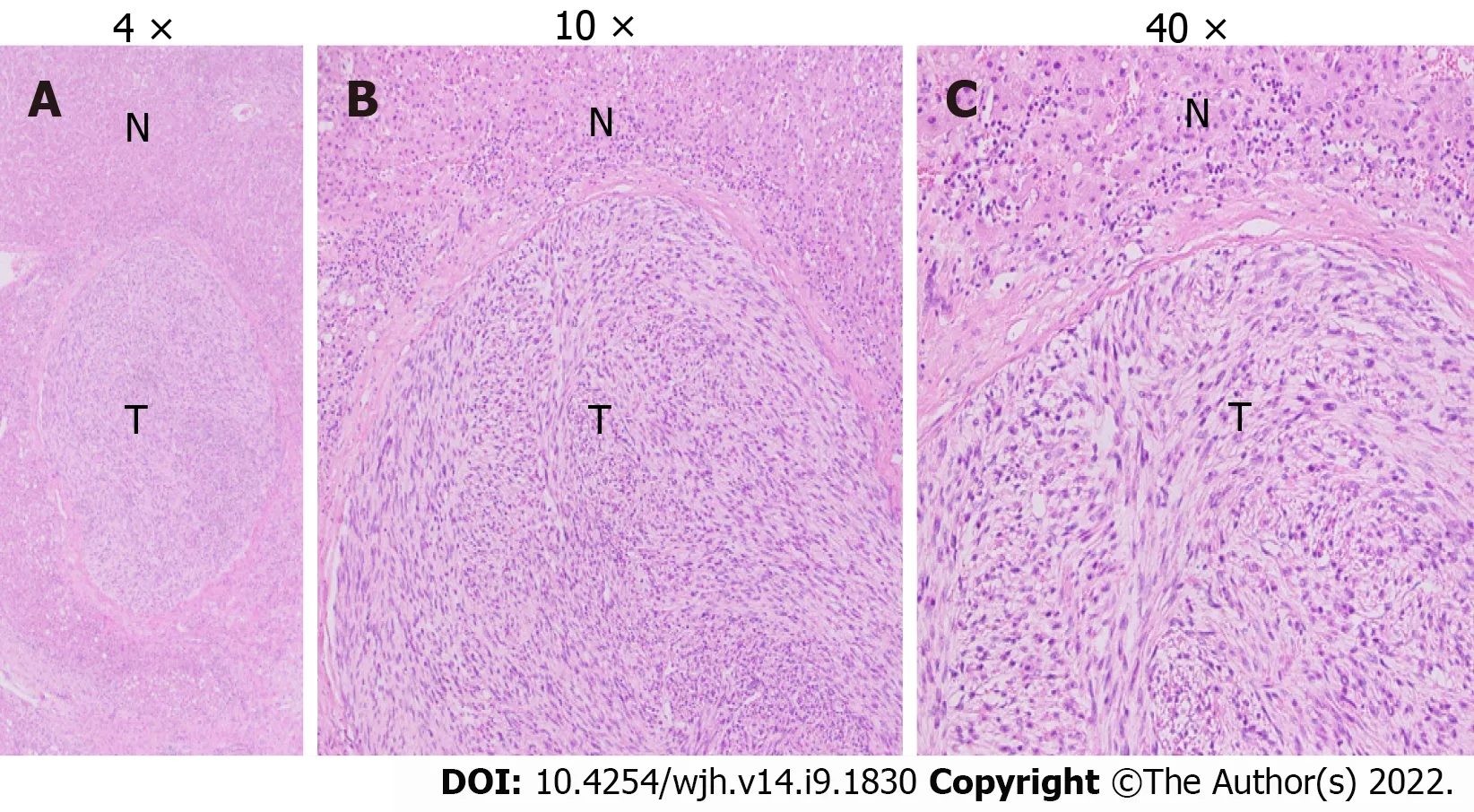
Figure 3 Leiomoyosarcoma, subsequent resection specimen. A: Original magnification: 4 ×, scale bar: 100 μm; B: The above figures show liver parenchyma with a central nodule/tumor fascicular array of cells having spindle-shaped nuclei, moderate degree nuclear atypia (original magnification: 10 ×; scale bar: 100 μm); C: Mitoses marked as T, and normal liver hepatocytes marked as N (original magnification: 40 ×; scale bar: 100 μm).
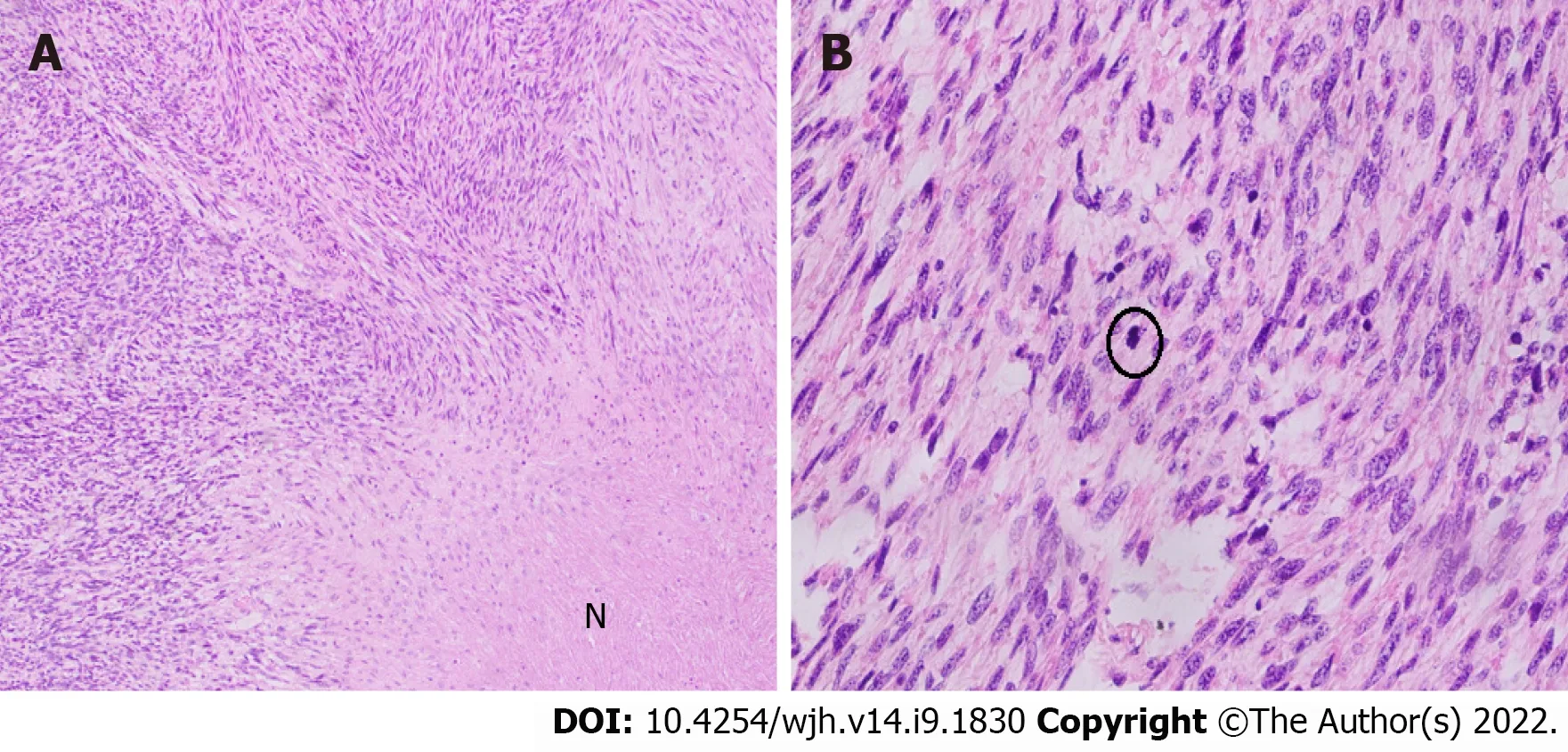
Figure 4 Hematoxylin and eosin stain of leiomoyosarcoma. A: Hematoxylin and eosin stain of leiomoyosarcoma, resected specimen, a section of the liver shows fascicular array of cells with spindle-shaped nuclei (Original magnification: 100 ×; scale bar: 100 μm); B: A moderate degree nuclear atypia, and mitoses (encircled) along with areas of necrosis marked as N (original magnification: 400 ×; scale bar: 100 μm).
Immunohistochemical stain
Desmin (clone DE-R11, Ventana; Roche Diagnostics, Indianapolis, IN, USA), a marker of smooth muscle differentiation, was positive in tumor cells; and caldesmon (clone E-89; Cell Marque Co., Rocklin, CA, USA) was negative in tumor cells. In addition, CD117 (clone EP-10; Leica, Wetzlar, Germany) and DOG1 (clone SP31; Cell Marque) were also negative in tumor cells, ruling out the possibility of the closest differential diagnosis of GIST (Figure 5).

Figure 5 Fascicular array of cells with spindle-shaped nuclei. A: Moderate degree nuclear atypia (original magnification: 100 ×; scale bar: 100 μm); B: Mitoses (encircled) (original magnification: 100 ×; scale bar: 100 μm); C: Immunostaining of desmin highlighting spindle-shaped cells (original magnification: 100 ×; scale bar: 100 μm); D: Caldesmon-negative (original magnification: 100 ×; scale bar: 100 μm).
OUTCOME AND FOLLOW-UP
The postoperative recovery of the patient was uneventful. She was discharged on the 6thpostoperative day. The patient remained asymptomatic until the follow-up visit after 6 mo. No short- or long-term postoperative complications were reported. CT and PET-CT scans were performed during this followup visit, which showed no evidence of recurrence and metastases. The patient was later presented in the MDT of Sarcoma, where it was decided to keep the patient under bi-annual surveillance, and no adjuvant treatment was recommended.
DlSCUSSlON
Sarcomas from the liver are rare, constituting only 1%-2% of all primary hepatic malignant tumors[1,2]. Leiomyosarcoma accounts for 8%-10% of all hepatic sarcomas, whereas other hepatic sarcomas including angiosarcoma, fibrosarcoma, liposarcoma, embryonal sarcoma, malignant fibrous histiocytoma, carcinosarcoma, and epithelioid hemangioendothelioma collectively comprise nearly 70%-80% of hepatic sarcomas[3]. Hepatic leiomyosarcomas are generally metastatic, arising from the GI tract, uterus, retroperitoneum, or lungs, requiring careful staging[2]. To the best of our knowledge, only about 70 cases, including case series, have been published internationally, including our patient (Tables 1 and 2)[1].
Leiomyosarcoma potentially originates from the smooth muscle cells in the round ligament, intrahepatic blood vessels, and bile ducts. Tumors arising from intrahepatic veins have a worse prognosis because they tend to progress to Budd-Chiari syndrome. The differentiation between benign leiomyoma and low-grade leiomyosarcoma is based on mitotic figures per HPF, although variation occurs according to the site of origin[3,4].

Table 1 Management outcomes of published case reports of primary hepatic leiomyosarcoma
There is no apparent sex predilection with an approximate male-to-female ratio of 1:1 in the literature review of cases reported to date including our patient. Age at the time of presentation is variably reported with a range of 5 mo to 86 years (mean age of 51.3 years)[5,6].
No specific pathological causes of PHL have been identified to date, although the literature review shows an association with multiple etiological factors, including immunosuppression due to acquired immunodeficiency syndrome. Epstein-Barr virus infection is reported in two cases and a previous history of immunosuppression postrenal transplant in 1 case. The other reported associations include hepatitis C virus infection, exposure to thorotrast, and previously treated Hodgkin’s lymphoma[7-11].

Table 2 Management outcomes of published case series of primary hepatic leiomyosarcoma
PHL usually pursues an indolent course being asymptomatic initially until they enlarge in size causing non-specific symptoms such as abdominal pain or discomfort, a palpable mass, fever, jaundice, anorexia, nausea or vomiting, and weight loss. The literature review revealed a single patient presenting as an emergency due to acute intraabdominal hemorrhage following tumor rupture. There is usually a single mass, although there are cases with multiple masses. Tumor size varies significantly ranging from 0.6 cm to 30 cm in the largest dimension (mean and median diameters of 10.3 cm and 9.1 cm, respectively). In our case, the tumor size was 10 cm in its largest dimension. The distribution of PHL within the liver segments and lobes also differs, with 2/3rdcases involving the right lobe and 1/3rdcases involving the left lobe. The case presented here involved the left lobe of the liver[6,11-16].
Histological examination usually shows intersecting bundles of spindle-shaped cells with hyperchromatic nuclei and mitotic figures. Immunohistochemistry shows positive results with smooth muscle actin, desmin, and vimentin, whereas cytokeratins, neuron-specific enolase, S-100 protein, αfetoprotein, CD34, CD117, and DOG1 were not expressed.
Ultrasonography usually shows hypoechoic or heterogeneous echogenic mass. CT findings generally describe a hypodense and sometimes heterogeneous mass with inhomogeneous and often peripheral enhancement after intravenous contrast administration, which may show regions of cystic degeneration, demonstrated in our case[17]. Ferrozziet al[18] reported that hemorrhagic necrosis, along with cystic degeneration and necrosis, are likely to be secondary to tumor growth. Magnetic resonance imaging characteristically displays homogeneous or heterogeneous hypointense T1-weighted images and hyperintense T2-weighted images[19]. PET-CT scan SUV max can be correlated with the tumor size, tumor-node-metastasis staging, and histology subtype[20]. In our case, the SUV max of the primary tumor was 6.4, with a baseline hepatic parenchymal SUV of 2.96.
Therapeutic options vary depending upon the tumor size and/or stage on initial presentation. Hepatic resection (wedge resection, segmentectomy, lobectomy, or extended hepatectomy with the intention of R0 resection) remains the only potentially curative surgical option for non-metastatic including our case. However, 4 patients with tumors confined within the liver had liver transplantation[14,21].
Some authors have also reported that adjuvant chemotherapy consisted of various drugs, including doxorubicin and ifosfamide, which help to attain prolonged survival after complete resection. In addition, three cases have been treated with radiotherapy as part of a combined adjuvant treatment along with chemotherapy[5,22-24].
Transarterial chemoembolization and transarterial infusion of epirubicin and carboplatin were also reported in individual cases as treatment modalities for PHL[25].
The median survival is 37.5 mo with a 5-year survival rate of about 40%; two large case series reported 67% disease-specific survival at 5 years after R0 resection. Matthaeiet al[14] in a case series, reported more than 10 years of survival after hepatectomy. Chiet alreported a median overall survival of 19 mo with 1-, 2-, and 5-year survival rates of 61.2%, 41.1%, and 14.5% respectively[26].
Age is another crucial predictive factor for prognosis, with patients below 50 years achieving better survival. Currently, no effective therapeutic options have been reported for unresectable PHL. Fujitaet al[9] reported a patient with metastatic leiomyosarcoma surviving 3 mo after diagnosis, who received only palliative and conservative therapy.
CONCLUSlON
In conclusion, PHL is a rare malignant disease with often delayed presentation, relatively poor prognosis, and aggressive metastatic potential. The most preferred management options include surgical excision combined with chemotherapy and radiotherapy. However, very little is known about the efficacy of available therapeutic options because of the rarity of the disease. Therefore, in-depth studies are required to assess its causative, prognostic, and predictive parameters.
FOOTNOTES
Author contributions:Ahmed H and Bari H were the patient’s surgeons, reviewed the literature, and contributed to manuscript drafting; Sheikh UN and Basheer MI performed the histopathological analyses and interpretation; All authors issued final approval for the version submitted.
lnformed consent statement:Informed written consent was obtained from the patient to publish this report and any accompanying images.
Conflict-of-interest statement:The authors have no conflicts of interest to declare.
CARE Checklist (2016) statement:The authors have read the CARE Checklist (2016), and the manuscript was prepared and revised according to the CARE Checklist (2016).
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:Pakistan
ORClD number:Hassan Ahmed 0000-0002-0244-8939; Hassaan Bari 0000-0001-7098-6942; Umer Nisar Sheikh 0000-0001-6305-2252; Muhammad Irfan Basheer 0000-0001-5873-7759.
S-Editor:Wang LL
L-Editor:Filipodia
P-Editor:Wang LL
 World Journal of Hepatology2022年9期
World Journal of Hepatology2022年9期
- World Journal of Hepatology的其它文章
- Analysis of hepatitis C virus-positive organs in liver transplantation.
- A retrospective study on use of palliative care for patients with alcohol related end stage liver disease in United States
- Hereditary hemochromatosis: Temporal trends, sociodemographic characteristics, and independent risk factor of hepatocellular cancer- nationwide population-based study
- Liver magnetic resonance imaging for evaluation of response to treatment after stereotactic body radiation therapy of hepatocellular carcinoma
- Modified preoperative score to predict disease-free survival for hepatocellular carcinoma patients with surgical resections
- Decrease in liver cancer incidence rates in Βamako, Mali over 28 years of population-based cancer registration (1987-2015)