
Ehlers-Danlos syndrome: prevalence and outcomes in gender affirming surgery - a single institution experience
2022-07-21 01:18:38AlirezaNajafianIsabelCylinderBreannaJedrzejewskiCraigSineathZbigniewSikoraLeighMartinDanielDugiGeolaniDyJensUrsBerli
Plastic and Aesthetic Research 2022年5期
Alireza Najafian, Isabel Cylinder, Breanna Jedrzejewski, Craig Sineath, Zbigniew Sikora, Leigh H. Martin, Daniel Dugi, Geolani W. Dy, Jens Urs Berli,
1Division of Plastic Surgery, Department of General Surgery, Oregon Health & Science University, Portland, OR 97239, USA.
2Department of Urology, Oregon Health & Science University, Portland, OR 97239, USA.
Abstract Aim: Patients with Ehlers-Danlos Syndrome (EDS) are considered to have an increased risk for wound healing complications. Surgeons may therefore be hesitant to offer elective surgeries, including gender-affirming surgeries (GAS), to EDS patients. At our center, we frequently encountered patients presenting for GAS evaluation with the co-existing diagnosis of EDS. This study aims to establish the prevalence of EDS diagnosis in our GAS patients and compare their post-operative complications to patients without EDS diagnosis.Methods: This is a single-institution retrospective case-control study on all patients who underwent GAS from 2016-2020. Data include EDS diagnosis, demographics, operation, and complications (including minor wound healing issues).Results: Of 1363 patients presenting for GAS, 36 (2.6%) had EDS diagnoses and were matched with 108 control patients. Major complications requiring surgical intervention in the OR occurred in 6 patients (4.2%), (2.8% EDS vs.5.4% controls; P= 0.63), while 8.3% of EDS and 14% of controls required minor interventions (P= 0.38). The rate of wound healing issues of any severity was 28% in EDS vs.47% in control groups (P= 0.04).Conclusion: The prevalence of EDS diagnosis in our patient population is 132 times the highest reported prevalence in the general population. Wound healing issues and the need for additional post-operative interventions in the group with EDS diagnosis were not significantly different from the control group. Our findings suggest that patients with a diagnosis of EDS undergoing GAS have comparable outcomes to patients without EDS. Concerns for postoperative complications should not be a barrier to offering GAS to patients presenting with an EDS diagnosis.
Keywords: Ehlers-Danlos, gender, transgender, gender affirmation, surgery, outcomes
INTRODUCTION
Transgender and gender diverse individuals experience incongruence between their sex assigned at birth and gender identity, which may lead to gender dysphoria. Gender affirming surgery is one modality that can assist in decreasing gender dysphoria and aligning patients’ birth anatomy with their gender identity[1,2].
The exact etiology of gender incongruence and resultant gender dysphoria (GD) is not fully understood and remains a topic of an ongoing investigation. Genetic susceptibility to the development of GD has been posited: researchers are currently exploring whether genes and genetic variants could play a role in the neurodevelopmental pathways leading to GD in some patients[3]. These findings remain controversial and likely do not take the full scope of etiologies into account[4,5]. However, several psychological and somatic conditions with known genetic susceptibilities have been described to co-occur with GD. Recent research has suggested a possible association between GD and type 1 diabetes (T1DM): one study reported the prevalence of T1DM to be 9.4-fold higher in adolescents with GD than those without[6]. The exact mechanisms of these associations remain unknown and require further research[7]. However, it does raise the question as to whether GD may be associated with other genetically modulated conditions and, if so, how that may influence surgical management of GD.
At our Transgender Health Program, we have noted a substantial number of patients with GD seeking gender-affirming surgeries (GAS) who presented with a diagnosis of Ehlers-Danlos syndrome (EDS). EDS is a clinically and genetically heterogeneous group of disorders resulting from a defect in the synthesis or structure of fibrillar collagen, which manifest as varying constellations of symptoms, including soft and hyperelastic skin, hypermobile joints, vascular dysfunction, and kyphoscoliosis[8]. All forms of EDS except for the hypermobile subtype have molecular classifications that can be confirmed with genetic testing[9]. Additionally, EDS has been demonstrated to have an association with postural tachycardia syndrome (POTS), mast cell activation disorders, urological disorders (urinary incontinence, bladder diverticulum), gynecological disorders (pelvic organ prolapse, irregular menses and bleeding), and an increased risk of hemorrhage[10-15]. The prevalence of EDS in the general population is estimated at 1 in 5000 to 1 in 20,000[16]. Diagnosing EDS is challenging and heavily reliant on clinical presentation and family history; genetic testing is predominantly reserved for diagnosis of the vascular subtype[17].
Because EDS affects the strength of skin and other organs (i.e., vascular structures), patients with EDS have been considered to have a higher risk for perioperative complications including anesthesia-related issues and wound healing complications[18]. Traditionally, caution has been taken when offering elective surgery to this patient population[19]. However, given the rarity of EDS, there is a paucity of evidence regarding the outcomes of elective surgeries in patients with EDS. There have been no prior studies describing the prevalence of EDS in patients with GD, or the risk of surgical complications in this population. An existing EDS diagnosis, whether correctly diagnosed or not, may present a significant barrier to receiving medically necessary GAS.
The primary aim of our study was 2-fold: to evaluate the prevalence of EDS in patients with GD that underwent GAS at our institution, and to assess whether patients with EDS demonstrated a higher rate of postoperative healing complications following GAS. Given the range and complexity of gender-affirming procedures, outcomes of the surgeries presented here may serve as a surrogate for outcomes of other reconstructive surgeries.
METHODS
Study design
This is a retrospective case-control study. Institutional review board approval was obtained from Oregon Health & Science University. We identified all patients with a diagnosis of GD who underwent GAS at our institution between 2016 to 2020; patients were identified using CPT codes for pertinent gender-affirming surgeries and ICD-10 codes for gender dysphoria. All patients with the co-diagnosis of EDS were included. Genetic testing was not assessed as an inclusion criterion. Data was collected through a review of patients’ electronic health records, including intra-operative records and post-operative follow-up visits. Data included the presence of an EDS diagnosis, demographics, comorbidities (i.e., POTS, T1DM), type of surgery received, surgical complications, and management thereof. We included the following GAS procedures: chest masculinization, chest feminization, phalloplasty, metoidioplasty, vaginoplasty, vulvoplasty, orchiectomy, and facial feminization including laryngeal chondroplasty. In patients who underwent more than one surgery, we considered the most extensive surgery as the index operation.
Measured outcomes included wound healing issues (hypertrophic scar, keloid formation, wound separation), surgical site infection, hematoma and seroma. Complications were further classified into minor and major complications based on the Clavien-Dindo classification of surgical complications: those requiring interventions without the need for general anesthesia (grade ≤ IIIa) and those requiring interventions under general anesthesia (grade ≥ IIIb)[20].
Statistical analysis
Independentt-test and the Kruskal-Wallis test were used to analyze normally and non-normally distributed variables, respectively. Normally distributed variables are presented as mean ± standard deviation, and nonnormally distributed variables are expressed as median and interquartile ranges. Counts and proportions were analyzed using chi-square and Fisher exact tests. All statistical analyses were performed using Stata? Data Analysis and Statistical Software: Release 12 (StataCorp LP, College Station, TX, USA). AP-value of < 0.05 was considered to be statistically significant.
RESULTS
Baseline data
Of 1363 patients who underwent GAS, 36 patients with a diagnosis of EDS were identified and matched with 108 patients without EDS based on the type of procedure. The EDS group had a statistically significantly higher prevalence of mental health comorbidities when compared with the non-EDS group [(89% (32 of 36)vs.65% (70 of 108);P= 0.006)]. There were no significant differences in other baseline characteristics between groups, including age, sex assigned at birth, gender identity, body mass index, smoking status, or diagnosis of diabetes mellitus [Table 1].
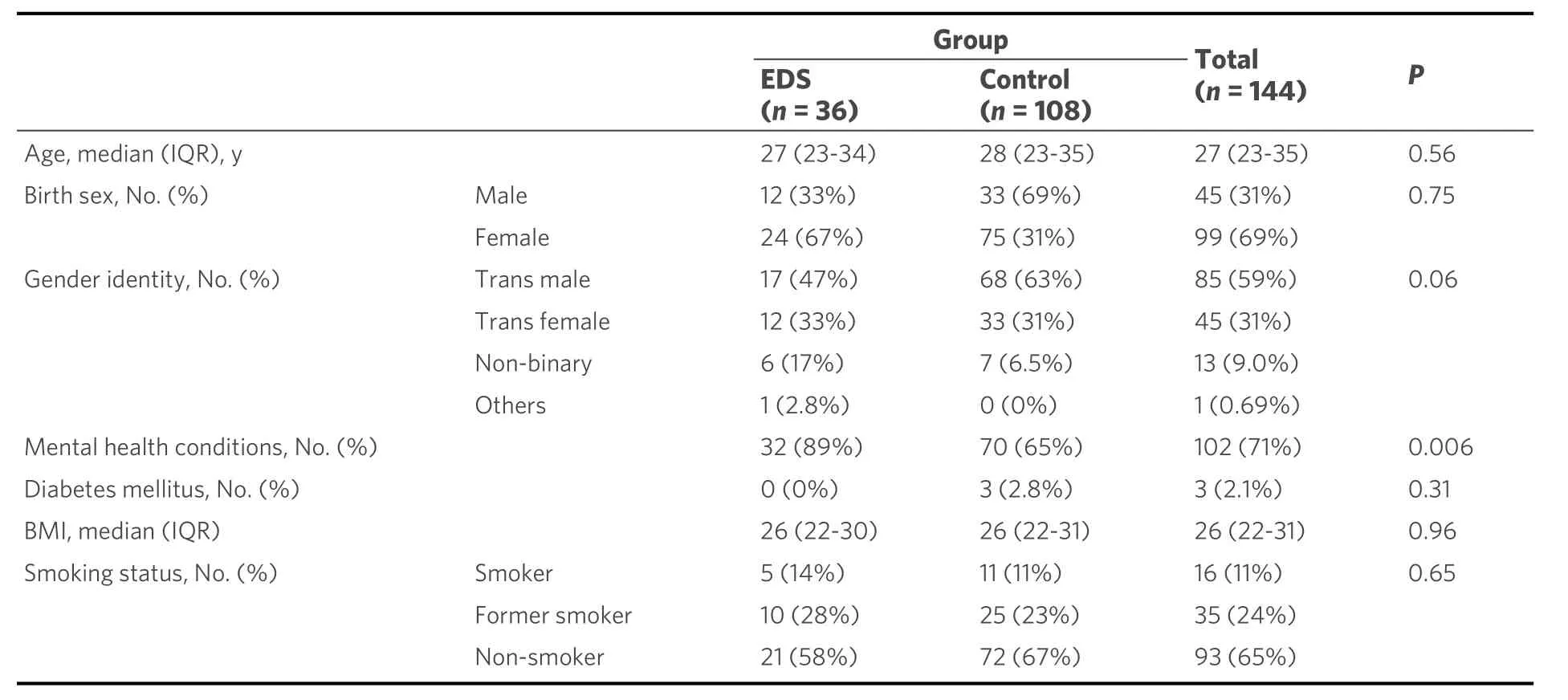
Table 1. Baseline characteristics of patients with EDS and the control group
In the EDS group, chest masculinization was the most common index procedure performed (58%, 21 of 36), followed by orchiectomy (17%, 6 of 36); chest feminization and phalloplasty (8.3% each, 3 of 36); and vaginoplasty, metoidioplasty, and facial feminization (2.8% each, 1 of 36) [Figure 1]. The control group was matched based on the index procedure and therefore had the same distribution of procedures.
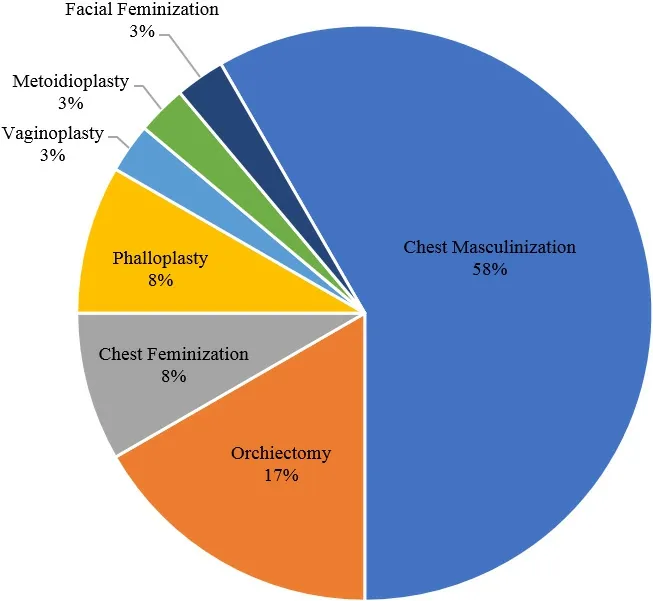
Figure 1. Gender-affirming surgeries performed. Thirty-six patients with a diagnosis of EDS were matched with 108 patients without EDS based on the type of procedure. EDS: Ehlers-Danlos syndrome.
EDS patient characteristics
Of 1363 patients who underwent GAS, 36 (2.6%) patients had the diagnosis of EDS. 67% of those were in patients who were female sex assigned at birth. Of these, 26 of 36 (72%) were diagnosed with hypermobile EDS, 1 of 36 (2.8%) with classical EDS, and 9 of 36 (25%) had an unspecified type of EDS. Six of 36 (17%) EDS patients reported a family history of EDS. Other associated diagnoses were found in the EDS group, including POTS [19 of 36 (53%)], chronic pain [24 of 36 (67%)], fibromyalgia [9 of 36 (25%)], dysautonomia [5 of 36 (14%)], and history of joint surgery [4 of 36 (11%)] [Table 2].
Complications
A total of six patients (4.2%) developed complications requiring surgical intervention (3 hematomas, one return to the OR for venous flap congestion, one nipple-areolar revision and one dog ear revision). This was not significantly different between two groups [1 (2.8%) in EDSvs.5 (4.6%) in control group;P= 0.63]. The rate of wound healing issues of any severity was significantly lower in the EDS group than in the control group [28% (10 of 36)vs.47% (51 of 108);P= 0.04]. Other complication profiles were not significantly different between the two groups [Table 3]. The breakdown of complications based on the type of surgery is presented in Table 4.
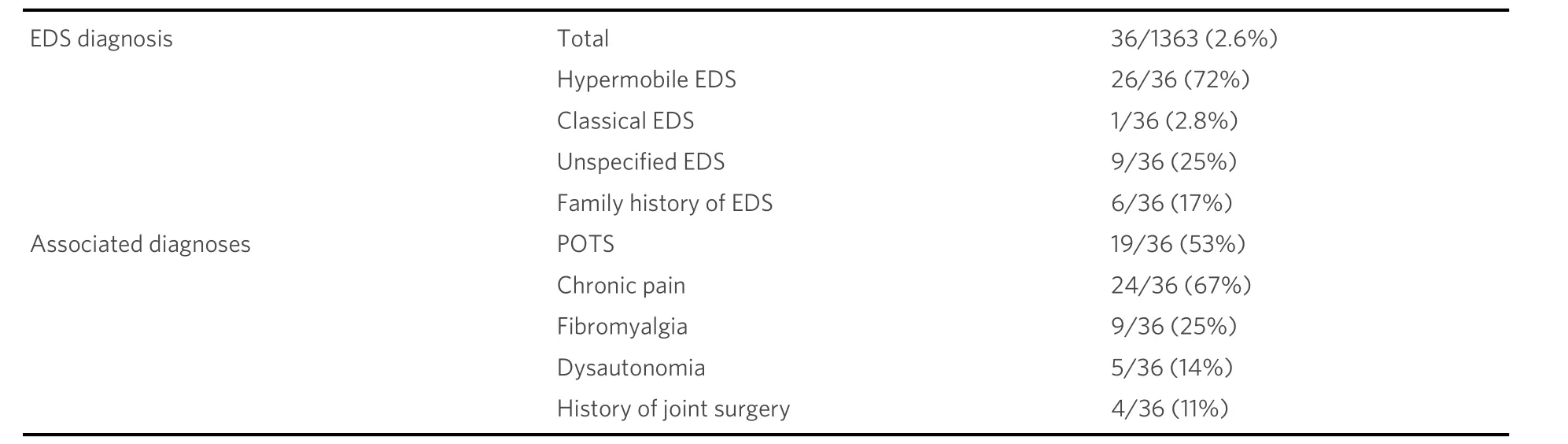
Table 2. EDS patient characteristics

Table 3. The complication rate in EDS and control group
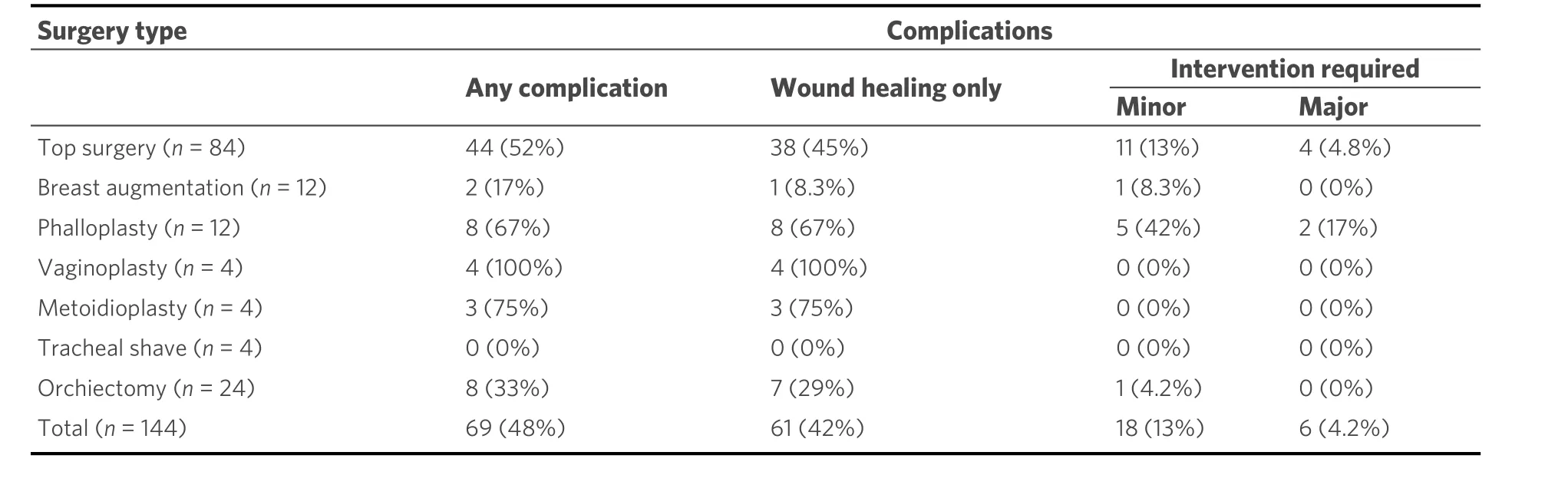
Table 4. Breakdown of complications based on the type of surgery
Minor and major complications classified based on Claviden-Dindo Grade. Complications classified as minor if they required intervention, not under general anesthesia (Clavien-Dindo Grade ≤ IIIa); major complications required intervention under general anesthesia (Clavien-Dindo Grade ≥ IIIb).
Minor and major complications classified based on Claviden-Dindo Grade. Complications that required intervention were classified as minor if they did not need intervention under general anesthesia (Clavien-Dindo Grade ≤ IIIa); major complications required intervention under general anesthesia (Clavien-Dindo Grade ≥ IIIb).
DISCUSSION
Our investigation revealed the prevalence of Ehlers-Danlos syndrome in patients seeking gender-affirming surgery at our institution to be 132 times the highest reported prevalence in the general population. The rate of post-operative complications and the necessity for subsequent intervention in EDS patients were comparable to that of the control group.
Surgical complications in Ehlers-Danlos syndrome
The literature is relatively scarce with regards to associated surgical complications in patients with EDS, with the majority of studies dedicated to vascular surgery complications for vascular EDS. One study demonstrated that both open and endovascular surgery can be safely performed in patients with vascular EDS, with a possible role in the early and prophylactic treatment of vascular anomalies in these patients[21]. However, the data are not clear on this subject; a literature review published in 2016 showed that open and endovascular repair of vascular disorders were associated with higher complication rates in patients with vascular EDS[22]. A review of all published EDS reports from 1975 to 1995 included 45 vascular surgery patients with 12 patient deaths from vascular complications after endovascular or open repairs, indicating that vascular complications should be treated non-operatively when possible and simple vessel ligations should be conducted rather than complicated vascular reconstruction surgeries when possible[23].
Several studies also describe the impact of EDS on gestational outcomes. One retrospective survey of adverse events during pregnancy showed patients with EDS to have a higher rate of complications, including 20% of patients having third- or fourth-degree vaginal lacerations after pregnancy, which is ten times the rate of severe vaginal lacerations in the general population[24]. Another published literature review from 2018 showed pregnancy to be overall well-tolerated in patients with hypermobile EDS but with some increase in complications attributed to joint hypermobility, abnormal collagen in blood vessels, and fragility of skin and tissue[25].
Meanwhile, an animal study of five dogs and five cats with connective tissue dysplasia found no difference in wound healing when compared to those without the EDS-like disorder[26]. A study of 279 pediatric patients with EDS undergoing spine surgeries showed no difference in wound complications when compared to their peers[27,28].
Although many of these studies describe increased surgical complications in EDS patients, no guidelines have demonstrated EDS as a strict contraindication to surgery. Our data did not demonstrate a statistically significant higher prevalence of wound healing issues of any severity or major complications requiring surgical intervention under general anesthesia in EDS patients presenting for GAS.
Gender-affirming surgery in EDS patients
At our institution, we began providing comprehensive GAS in 2016. Initially, we were hesitant to offer complex genital gender-affirming surgeries to individuals with an EDS diagnosis based on traditional teaching that those patients were at higher risk for wound healing complications. Similarly, we saw patients who had been denied access to surgery at other institutions based on their EDS diagnosis. Due to the tremendous impact a denial of care can have on patients’ mental health, we started offering chest masculinization to patients with an EDS diagnosis, as we deemed the consequences of wound healing issues to be minimal. Given that our experience did not confirm the mentioned wound healing concerns, we proceeded to expand our surgical offerings to include genital gender-affirming procedures for patients with EDS diagnoses. This study confirms that, at least in this cohort, our approach to surgical care for patients who present for GAS and have associated EDS diagnosis is safe. We want to emphasize that we did not have any patients who suffered from vascular EDS. Based on the cited studies, those patients may present a different risk profile.
In our cohort, the classical and hypermobile subtypes were the most common diagnosis, which is consistent with the literature’s description of EDS demographics in the general population[29]. Notably, hypermobile EDS has not been found to have a genetic basis, but has been linked to chronic joint pain and autonomic dysfunction including POTS[9,30-32]. A limitation that has to be stated is that we have no means of confirming the often-empirical diagnosis of EDS. However, in our series, 67% of patients were diagnosed with chronic pain and 11% had previous joint surgery, indicating that at least a substantial amount of our cohort indeed have some form of connective tissue disorder. Interestingly, 53% of our patients in the EDS group also carried the diagnosis of POTS, a co-diagnosis rate 1.3 to 3.5 times higher than reported in other EDS cohorts. There was no statistically significant difference in the prevalence of T1DM in patients diagnosed with EDS and the control group.
Limitations and future directions
We acknowledge that our cohort is relatively small and that larger cohort studies are needed to assess complication rates of GAS in EDS patients. We also recognize that the absence of clear diagnostic guidelines for EDS introduces the potential for over- or under-diagnosis. Due to the retrospective nature of this study, data collection was limited to pre-existing patient-reported diagnoses of EDS, and information on confirmatory genetic testingvs.clinical diagnosis was not consistently available in the medical records.
These limitations notwithstanding, our study demonstrates a high rate of co-occurring EDS and GD, and no difference in wound healing or other post-operative complications among individuals with EDS who underwent GAS. Many surgeons may hesitate or even decline to offer complex genital GAS to patients diagnosed with EDS; however, these essential surgeries were provided to this patient population in our cohort without an increase in adverse events. With growing awareness and presentation of patients with EDS paired with a high prevalence of EDS in patients with GD, the historic paradigm about surgical risks related to EDS diagnosis may present an additional barrier to gender-affirming care. Thus, it is our hope that the findings of this study may improve access to gender-affirming care for transgender and gender diverse individuals with EDS. Our observation of the co-occurrence of EDS and GD in this cohort may warrant further study to explore the relationship between these two diagnoses.
In conclusion, at our institution, the prevalence of Ehlers-Danlos syndrome in patients seeking genderaffirming surgery was found to be 132 times the highest reported prevalence in the general population. The rate of post-operative complications and need for additional post-operative interventions was not found to be significantly different in patients diagnosed with EDSvs.the control group. Our findings suggest that patients diagnosed with EDS have comparable surgical outcomes to the control group, and concern for post-operative complications should not be a barrier to undergoing gender-affirming surgery.
DECLARATIONS
Acknowledgements
Authors would like to acknowledge Yiyi Chen for assistance with statistical analysis, and Gaines Blasdel for assistance with critical review of this study. We also would like to thank our patients for their contribution to this study.
Authors’ contributions
Made substantial contributions to conception or design of the study: Najafian A, Dugi D, Dy GW, Berli JU Performed data acquisition: Najafian A, Jedrzejewski B, Cylinder I, Sikora Z, Martin LH, Sineath C
Performed data analysis and interpretation: Najafian A, Berli JU
Drafted or substantively revised the manuscript: Najafian A, Cylinder I, Jedrzejewski B, Sikora Z, Berli JU
Availability of data and materials
Not applicable.
Financial support and sponsorship
None.
Conflicts of interest
All authors declared that there are no conflicts of interest.
Ethical approval and consent to participate
Oregon Health & Science University IRB protocol #00021260
Consent for publication
Not applicable.
Copyright
? The Author(s) 2022.
 Plastic and Aesthetic Research2022年5期
Plastic and Aesthetic Research2022年5期
- Plastic and Aesthetic Research的其它文章
- Ethical challenges in vascularized composite allotransplantation of the lower extremity: lessons learned from hand transplantation and implications for the future
- Introduction to special issue “Recent Advances in Skin Anti-Aging Agents”
- AUTHOR INSTRUCTIONS
- Peripheral nerve allograft: how innovation has changed surgical practice
- Current concepts in microsurgical soft tissue reconstruction of lower extremity trauma in a singlevessel extremity
- Soleus muscle flap for reconstruction of lower extremity trauma. Workhorse or glue factory?