
Patient-specific instrumentation in total ankle arthroplasty
2022-04-06 01:31:28AntonioMazzottiAlbertoArceriSimoneZielliSimoneBonelliValentinaViglioneCesareFaldini
World Journal of Orthopedics 2022年3期
INTRODUCTION
The recent increase in the adoption of total ankle arthroplasty(TAA)reflects the improvements in implant designs and surgical techniques.Nonetheless,the outcomes of TAA have commonly been less satisfactory compared to those of other arthroplasties[1].Thus,the search for successful TAA continues,and in fact,the interest in implementing this new technology is growing.
The literature on the subject has shown that proper implant positioning and alignment are necessary for achieving good results in TAA.Even the mispositioning of a small implant component has a relevant impact on motion and contact pressure,which may lead to failure[2,3].
As a matter of fact,most of the current TAA instrumentations do not really address patient's variable anatomical features.When using a traditional system,the main parameter considered for tibial cutting block is represented by the tibial tuberosity as proximal reference and the middle of the anterior border of the tibiotalar joint as distal reference.The talar resection is performed with the foot in a visual neutral position[2,3].This technique allows an experienced surgeon to adopt a good implant positioning;however,many other factors should be considered in order to fully re-establish gait symmetry and natural ankle motion.
No, master, it is not the carriage. It is a band from my heart, which was put there in my great pain when you were a frog and imprisoned10 in the well. Again and once again while they were on their way something cracked, and each time the King s son thought the carriage was breaking; but it was only the bands which were springing from the heart of faithful Henry because his master was set free and was happy.
Much as with hip and knee arthroplasty,large efforts have been devoted to improving TAA surgical techniques,including the use of preoperative plans based on computer software,and patient-specific instrumentation(PSI),such as custom-made cutting guides.Cutting guides are customized with respect to each patient’s anatomy based on preoperative ankle computed tomography(CT)scans,and they drive the saw intra-operatively to improve the accuracy of bone resection and implant posi-tioning.
Nevertheless,there is no unanimous agreement regarding the indication and efficacy of PSI in TAA[4].The purpose of this review article is therefore to assess the current literature on PSI in TAA.In particular,we will discuss the following topics:(1)Current implants with PSI;(2)Templating and preoperative planning strategies;(3)Alignment and sizing;(4)Clinical outcomes;(5)Cost analysis;and(6)Comparison with standard techniques.
TYPES OF IMPLANTS
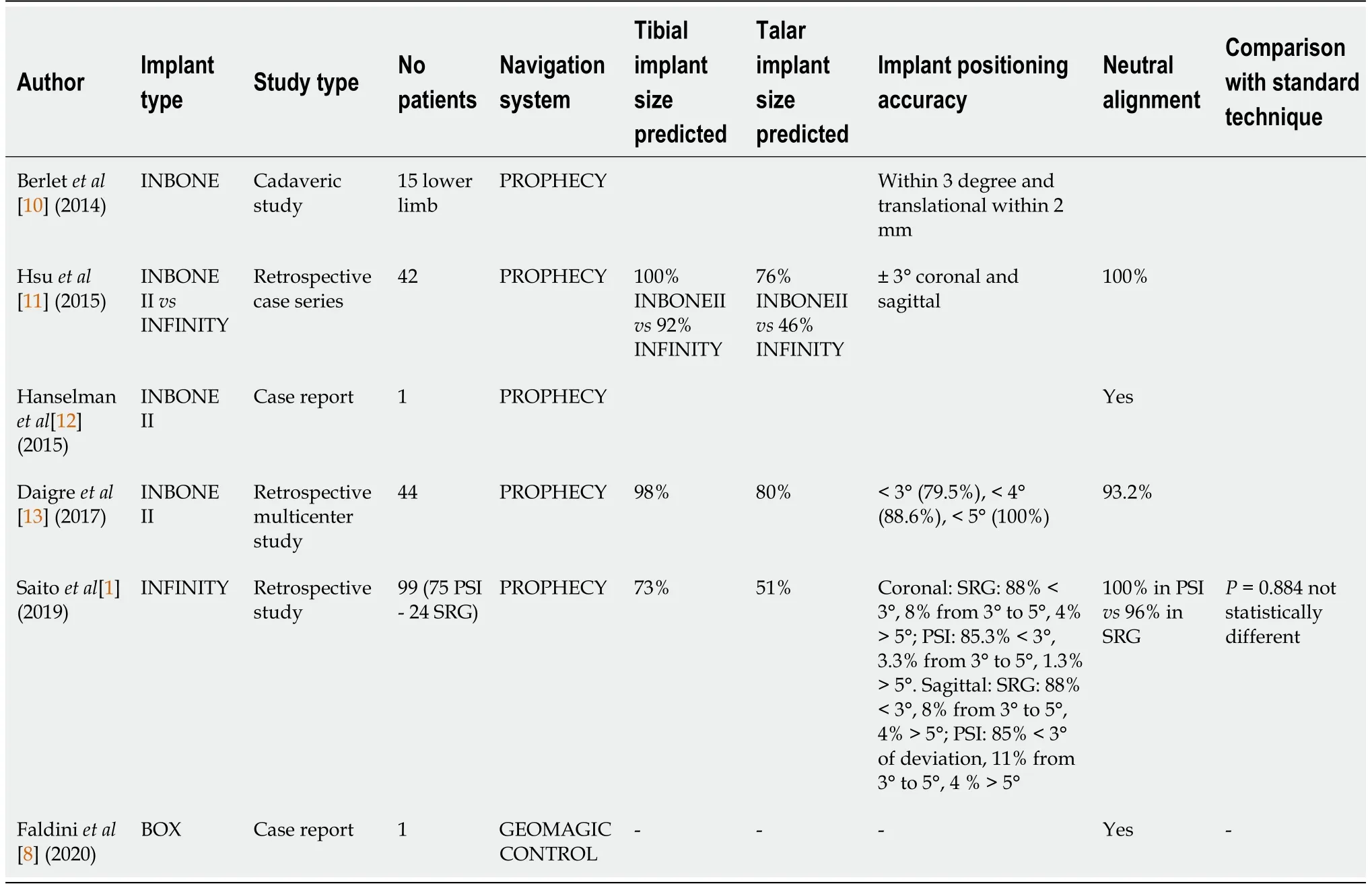
Only three implants with PSI for TAA are currently available(Table 1):The INFINITY TAA(Wright Medical Technology Inc,Arlington,TN,United States).The INBONE II Total Ankle System(Wright Medical Technology Inc),and a custom-made version of the BOX TAA(MatOrtho,Ltd.,Leatherhead,United Kingdom).
The INFINITY TAA
This implant has a 2-component fixed bearing design,with a low-profile tibia and talar resurfacing,and requires minimal bone resection.The tibial resurfacing component is made of titanium alloy and presents three angled pegs,whilst the talar component has two pegs and is made of cobalt chrome alloy.The INFINITY TAA can be implanted using a CT scan-derived PSI through the PROPHECY Preoperative Navigation System(Wright Medical Technology Inc)[5,6].
The INBONE II total ankle system
This preoperative planning strategy has been proposed in other clinical studies,demonstrating overall positive accuracy and reproducibility[1,11,13].
Custom-made version of the BOX TAA
Adams[20]compared computer-assisted tibia preparation with standard techniques in a cadaveric study.Results showed that the conventional and computer-navigated tibial measurements were not different in the 95% confidence interval for CT,fluoroscopy,or radiographic assessments.
Then she was astounded, for she knew that the looking-glass never spoke falsely, and she knew that the huntsman had betrayed her, and that little Snow-white was still alive.
Considering the low number of implants available on the market,there are also few studies in the pertaining literature regarding PSI for TAA,as reported in Table 1.
TEMPLATING AND PREOPERATIVE PLANNING STRATEGIES
Templating in joint prosthetic surgery facilitates alignment optimization,helps in the selection of the correct implant size,and leads to more reliable and consistent prosthesis placement,theoretically lowering the risk of intra-operative complications.
While pre-operative templating is of great importance in planning hip and knee arthroplasty,its role in TAA is less clear.
The advantages of PSI in clinical outcomes are still theoretical and need to be confirmed.Conversely to primary arthritis of the hip and knee,end-stage ankle arthritis was frequently post-traumatic and generally involves younger patients.For this reason,looking at the joint replacement,ankle patients are reported to produce greater common physical demands than hip and knee ones;hence,the duration of implants for ankle patients needs to be increased by roughly 10 years.Therefore,obtaining a more accurate anatomic alignment with PSI may reduce the incidence of eccentric wear,component loosening,subsidence,and failure,and indirectly improve longevity and clinical outcomes[10].
Differently from standard techniques,preoperative planning using PSI for TAA is initiated by obtaining preoperative ankle CT imaging,according to manufacturer established protocols,in order to create the patient-specific 3D model.Although with some differences,all computer navigation systems require preoperative CT scans from the knee through the mid-foot.
CT scans allow us to assess preoperative coronal plane deformity,sagittal plane deformity,and rotational deformity,as well as permitting an evaluation of MAT,and AAT alignments.
On the coronal plane,varus or valgus deformity should be determined(neutral alignment is considered as less than 5 degrees of varus or valgus[4]).The tibial slope must be measured in the sagittal plane considering the anterior distal tibial angle,the angle between the AAT,and the line connecting the distal points on the anterior and posterior tibial articular surface(normal values:83.0 ±3.6 degrees)[15].
The first study using the PROPHECY system was conducted by Berlet[10]in 2014 in order to evaluate the reproducibility of tibia and talus patient-specific guide placement and variation between the pre-operative plan and real component position.Fifteen cadaveric lower extremities were scanned and imported into a CAD environment which created the 3D models based on the ankle CT scan.The 3D bone models were combined with the 3D CAD models of the implants and instrumentation to perform a virtual TAA after choosing the appropriate implant size and position.Patient-specific guides were then manufactured to define the resection planes,and the final implant position was recorded.Mean deviation among pre- and post-operative implant position was less than 2° and 1.4 mm[10].
In the past,ankle coronal and sagittal plane deformities represented a contraindication to TAA[17].The recent literature shows a trend toward extending the indication of TAA even in the case of severe deformities.During the templating,deformity correction must be evaluated and addressed.Realignment procedures can be performed before TAA surgery or simultaneously to the prosthesis implantation,acting on bone or soft tissue structures depending on patho-anatomy[18,19].
In addition,during pre-operative planning,the prosthesis size and corresponding bone cuts to prepare implant accommodation and its best possible position should always be considered[8].
If it had not been for the little Princess there is no saying what would have become of him, he was so miserable3, but there she was to be brought up, and luckily the good Fairy Lolotte, in spite of all that had passed, was willing to come and take charge of her, and of her little cousin Prince Vivien, who was an orphan4 and had been placed under the care of his uncle, King Gridelin, when he was quite a baby
Very few reports have evaluated the reliability of templating with PSI.In 2007,Adams[20]were the first to apply computer-assisted surgery for TAA in a cadaver study.Seven matched-pair lower extremities were used.One leg from each pair was randomized for the conventional tibial preparation arm of the study,using the external alignment guide and tibial cutting block from the Scandinavian Total Ankle Replacement system(STAR,Waldemar Link GmbH &Co.,Hamburg,Germany).Since dedicated TAA software did not exist at the time of the study,the other leg from each matched pair underwent computer-assisted tibial cut preparation using the VectorVision navigation system(BrainLAB,Munich,Germany)with total knee arthroplasty software.Pre-operative CT data was used to assess the tibial mechanical axis.In both groups,the accuracy of the tibial plafond preparation relative to the tibial shaft axis in both the coronal and sagittal planes was determined by fluoroscopic,radiographic,and CT analysis.Although the conventional and the computer-assisted measurements were not statistically different when compared to one another,the development of computer-navigation software specific to TAA continued.
The first PSI system for TAA that was able to provide a preoperative plan is the PROPHECY INBONE II and PROPHECY INFINITY Preoperative Navigation System.As in other forms of navigation-assisted surgery,the software generates a highly accurate rendering of the patient’s bony anatomy.This technology allows the surgeon to interact with the computer model and develop the surgical strategy through stepwise considerations.This process identifies loose bodies,the osteophytes’location,size,and shape,the presence of bone deficits,the 3-plane nature of any preexisting deformity,and the desired features,position,and size of the final implants.
The PROPHECY template calculates the preoperative deformity and the MATthe AAT based on anatomic landmarks.Anatomic landmarks are established in order to determine tibia/talus alignment achieving neutral axes.According to Berlet[10],the tibia landmarks are:The proximal tibia,the distal tibia,the proximal anatomic canal,and the distal medial and lateral gutter.The talus landmarks are:The talar neck,and the proximal medial and lateral gutter.These landmarks are used to combine the 3D bone model with 3D computer-assisted design(CAD)models of the implants and instrumentation to perform a virtual TAA implantation.Implant positioning is usually based on the AAT[13],but the choice is at the discretion of the surgeon[17].Once templating and preoperative planning are approved,patient-specific guides that reference bony anatomy are built through selective laser sintering.
Mom reached into her purse and pulled out the envelope. She passed it to Darlene, Darlene gave it to me, and I handed it to Ocy. Ocy put it in the offering.
The interior was lit up with thousands and thousands of candles, and his wife was dressed in cloth of gold and was sitting on a much higher throne, and she wore three great golden crowns
All these measurements can deviate significantly depending on several factors,such as congenital or post-traumatic femoral or/and tibial deformities[16].More frequently,in the presence of coronal deformity,AAT deviation from the MAT is accentuated.
This implant is an evolution of the original INBONE design and consists of an intramedullary fixedbearing two-component design with a polyethylene bearing surface locked into the tibial baseplate.The system retains some main features of the INBONE I design and instrumentations,including the modular tibial stems,thicker polyethylene bearings,and intramedullary guidance.In addition,the INBONE II total ankle system has certain enhancements,including sulcus articulation,additional talar fixation,anteroposterior long tibial trays,trial reduction placement of the talar component,and boneremoval instrumentation.This new sulcus design has twice as much coronal plane stability as the saddle design of the INBONE I TAA;moreover,it has two 4-mm anterior pegs in addition to the single talar stem design of the INBONE I component,resulting in increased rotational stability[7].The INBONE II total ankle system can be implanted using a CT scan-derived PSI through the PROPHECY Preoperative Navigation System(Wright Medical Technology Inc).
When she recovered her senses she was more than ever convinced that he was dead, since even Melinette was no longer near her, and no one was left to defend her from the odious60 old Enchanter
More recently,a new and complete TAA customization process was introduced by Faldini[8],consisting of patient-specific 3D-printed implants and instrumentation.Images obtained from a CT scan were processed for a 3D customized model of the ankle and the BOX ankle prosthesis(MatOrtho,United Kingdom).Using GeoMagic Control(3D Systems,SC),TAA was performed virtually by selecting the most suitable size for each implant according to the dimensions of the joint about to be replaced.Through the use of GeoMagic Control,it was possible to retrieve the corresponding bone resections and the corresponding PSI,designed to perfectly fit the frontal bone of the ankle and embed all required guides for bone preparation.The obtained models were printed in Acrylonitrile Butadiene Styrene by additive manufacturing for a final check.Upon approval of the planning procedure,the models were sent for final state-of-the-art additive manufacturing(the metal components using cobaltchromium-molybdenum powders,and the guides using polyamide).
Overall,preoperative three-dimensional bone imaging,and MAT and AAT axis determination are important aspects of planning and templating for PSI.
BUT how fared little Gerda during Kay’s absence? What had become of him, no one knew, nor could any one give the slightest information, excepting the boys, who said that he had tied his sledge1 to another very large one, which had driven through the street, and out at the town gate. Nobody knew where it went; many tears were shed for him, and little Gerda wept bitterly for a long time. She said she knew he must be dead; that he was drowned in the river which flowed close by the school. Oh, indeed those long winter days were very dreary2. But at last spring came, with warm sunshine. “Kay is dead and gone,” said little Gerda.
Several issues regarding PSI templating and preoperative planning strategies must still be addressed.First,different PSI image acquisition methodologies may influence the results.As a matter of fact,cutting guides are usually produced from a non-weightbearing preoperative CT scan.A weight-bearing CT scan,such as cone beam CT,may produce changes to the plan.
Other factors should also be considered:Dissimilar CT image resolutions and planning software,differences in the production methods used for the cutting blocks and their types,margin of error on the part of the manufacturer,and surgeon learning curve may affect the PSI outcomes,and influence the results.
Full-length weight-bearing lower limb imaging is rarely considered,though a complete lower limb alignment evaluation seems to be crucial in order to provide the most appropriate ankle alignment[14].
Lastly,it would be interesting to clarify whether pre-operative templating is more accurately performed using an AP radiograph or 3D imaging using CT scans,and to investigate if preoperative weight-bearing radiographs correlate with the PSI guide measurements.
ALIGNMENT AND SIZING
PSI was introduced as an innovative approach to also improve ankle alignment,and the accuracy and reproducibility of implant placement and sizing.
The literature has already shown that adequate TAA implant alignment and positioning are essential for achieving good clinical results[15,21].Even a small implant component malpositioning could result in a significant impact on motion and contact pressure,which may determine its failure[2].
Advocates for PSI in TAA argue that the advantages conferred by patient-specific cutting block also translate to subsequent improvements in implant positioning,reduced surgical time,and clinical outcomes.
There is still a good amount of controversial debate in the literature regarding whether PSI improves the reliability of achieving neutral ankle alignment and more accurate implant sizing.
In the cadaver-based study performed by Berlet[10],PSI led to a reliable and reproducible position of TAA component and ankle alignment.The mean prosthesis alignment variations between pre-operative plans and final location were all within ± 3 degrees.
Hsu[11]reported similar results in a retrospective case series of 42 consecutive TAAs using preoperative CT scan-derived patient-specific plans and guides(PROPHECY).Of the 42 TAAs,29 intramedullary referencing implants(INBONE II)and 13 low-profile tibia and talar resurfacing implants(INFINITY)were used.The study revealed that postoperative weight-bearing alignments were in a range of ± 3° from the expected coronal and sagittal alignments reported in the surgical plans following CT scans.Moreover,neutral alignments were gained for all TAAs,independently of preoperative coronal deformity.
Surgical plans have forecasted the real tibial component size utilized in 29 of 29(100%)INBONE II cases and in 12 of 13(92%)INFINITY cases.Conversely,plans were more inaccurate for talar component and predicted the real talar component size utilized in 22 of 29(76%)INBONE II cases and 6 of 13(46%)INFINITY cases.In all cases of predicted tibia or talar size mismatch,surgical plans estimated one implant size larger than the one that was actually used.
In 2015,Hanselman[12]reported the case of a 54-year-old man with a 29° varus hindfoot deformity treated by TAA using an INBONE II implant with PROPHECY PSI.Three months post operation,a neutral alignment was achieved,with a coronal plane angle of 1.8°.
In 2017,Daigre[13]reported on a retrospective multicenter study of 44 TAAs(INBONE II)using PROPHECY PSI.In 79.5% of cases,the postoperative tibial implant position corresponded to the preoperative plan within 3° of the planned aim,within 4° in 88.6% and 5° in 100% of cases.The preoperative navigation system aided to reach a postoperative neutral alignment in 93.2% of cases.The tibial component coronal size was properly predicted in 98% of cases,whereas the talar component was correctly predicted in 80% of cases.
But the eyes of the skull suddenly began to glimmer and to glow like red coals, and wherever the three turned or ran the eyes followed them, growing larger and brighter till they flamed like two furnaces, and hotter and hotter till the merchant s wife and her two wicked daughters took fire and were burned to ashes. Only Vasilissa the Beautiful was not touched.
When comparing PSI with the Standard Referencing Guide(SRG)on a retrospective analysis of 99 INFINITY TAAs,Saito[1]reported that the absolute variation of the tibial component from the intended alignment was 1.6 ± 1.2 degrees in the coronal plane,and 1.9 ± 1.5 degrees in the sagittal plane.
The PSI preoperative plan correctly predicted the implant size in 73% of cases for the tibial component,and in 51% for the talar component,whereas among the mismatched cases,the plan tended to predict an implant size larger than what was actually utilized for both implants.
Considering the reported data,imprecision of the computerized navigation system in predicting the talar implant size still exists.Some authors propose to justify the talar component mismatch with the matter of gutter debridement:An aggressive debri-dement may affect the sizing of the talar component,leading to smaller talar sizes[1,11,13].
CLINICAL OUTCOMES
Theoretically,the advantages that PSI confers on TAA should translate into impro-vements in clinical outcomes.However,given that PSI is still a novel technique,the current literature is lacking in longterm studies that can assess the differences in instrumentation techniques.
A single case report deals with clinical outcomes.Hanselman[12]reported good clinical results at 8 mo in a 54-year-old man using the INBONE II Prophecy TAA system.The patient was ambulating without assistance and the ankle range of motion was 40°.
Traditional preoperative planning methods for TAA are based on antero-posterior(AP)and lateral weight-bearing radiographs.Standard technique uses the tibial tuberosity as a point of reference and is based on the principle that the mechanical axis of the tibia(MAT)should equal the anatomical axis of the tibia(AAT)[14].
More than once it happened that when the king was in a bad temper, he let it out on the poor queen, and said that here they were now, getting old, and neither they nor the kingdom had an heir, and it was all her fault
COMPARISON WITH STANDARD TECHNIQUES
Kakkar[22]described how an implant misalignment could result in eccentric overloads.Traditionally,every arthroplasty system purpose is to reach a neutral axis[23].According to certain authors[24,25],neutral coronal ankle alignment is defined as less than 5 degrees of valgus to less than 5 degrees of varus.
A three-component implant,with cast cobalt-chrome-molybdenum alloy components fixed to the body of the talus and the distal portion of the tibia,along with an interposed mobile biconcave meniscal bearing,designed to be compatible with the movements of isometric fibers within the calcaneofibular and tibiocalcaneal ankle ligaments[8,9].The custom-made BOX TAA can be implanted using a CT scanderived PSI with GeoMagic Control(3D Systems,Inc).
In 2019,Saito[1]performed a retrospective analysis of 99 patients comparing the utilization of PSI with the SRG.The accuracy of the tibial component placement was similar between the two groups.Neutral ankle alignment was obtained postoperatively for all cases in the PSI group,and for all but one patient in the SRG group,who had 5.7° of varus deviation post operation.The use of PSI had to be abandoned intraoperatively in three cases(3.8%).Operative time(167190 min,= 0.040)and fluoroscopy time(85158 s,<0.001)were significantly decreased in the PSI group.
COST ANALYSIS
Any new technology,in addition to demonstrating clinical improvements,must undergo an economic analysis to reveal the added cost to the healthcare system in relation to its expected benefits.
Even more wonderful to me was my grandfather s ritual. He meticulously3 wound that clock with a special key each day. That key was magic to me. It kept our family s magnificent clock ticking and chiming, a part of every holiday and every tradition, as solid as the wood from which it was made. I remember watching as my grand-father took the key from his pocket and opened the hidden door in the massive old clock. He inserted the key and wound-not too much, never overwind, he d tell me solemnly. Nor too little. He never let that clock wind down and stop. When we grandkids got a little older, he showed us how to open the door to the grandfather clock and let us each take a turn winding4 the key. I remember the first time I did, I trembled with anticipation5. To be part of this family ritual was sacred.
Promoters of PSI suggest that PSI will reduce the overall costs of TAA.Although this technology has added associated costs,mostly because of preoperative CT imaging and the creation of custom-made cutting guides,the reduced operative time,the lower processing costs due to fewer sterile trays,the decrease in radiation exposure[4],the reduction in perioperative complications[26],and the better alignment leading to fewer revision surgeries represent the main advantages that can translate to reduced healthcare costs.
Only one study analyzed the costs of PSI in TAA.Hamid[1]identified a cost-savings threshold of$863 below which PSI was less costly than SR instrumentation.However,only the objective reduction of costs resulting from a decrease in operative time was considered.
CONCLUSION
PSI for TAA may represent an additional tool for surgeons and patients.However,the current literature does not allow us to confirm the superiority of PSI over standard techniques,and there are still several questions to be answered.
[AUTHOR S NOTE: On August 3, 1990, I received a phone call from Roger s son Randy and his wife Fran. They were calling from a hospital in Gainesville, Florida. Fran had just given birth to their first son. Fran and Randy wanted me to know that they named their son Andrew and asked i f I would be his godfather. To this day I still can t believe that the grandson o f my childhood hero Roger Maris is my namesake and my godson.]
Surgical experience is always necessary in order to consider all the factors influencing lower limb alignment,and bone,soft tissue,or ligament balancing.Moreover,blindly trusting PSI can potentially lead to mistakes in implant placement and sizing.For this reason,a surgeon should always know the SR and select a different implant size or abandon PSI when necessary.
Based on the current data from the pertaining literature,the main strengths of PSI for TAA are represented by good reproducibility and accuracy of implant positioning,good neutral alignment and correction of pre-existing deformities[27],shorter operative and fluoroscopy exposure time,and therefore,a potential decreased risk of complications as well as cost reductions[1].
Let it be in two months, answered Don Giovanni, for the time was nearly up that the devil had fixed13, and he wanted a whole month to himself to wash off the dirt of the past three years
The insufficiency of corroborating literature and scarcity of studies(in two cases financed by the manufacturer)[10,13]represent the current and main limitations of PSI.Moreover,it is not clear whether PSI may be more useful in order to restore ankle neutral alignment when dealing with complex deformities involving the whole lower limb.
Further prospective,randomized,and multicenter studies are therefore necessary to better evaluate PSI and confirm its routine use in TAA.
FOOTNOTES
Mazzotti A and Arceri A conceived the presented idea;Mazzotti A made substantial contributions to study conception and design,and data acquisition,analysis,and interpretation,drafted the manuscript,and revised it critically;Arceri A coordinated and supervised manuscript preparation;Zielli S provided documentation,and helped shape the research,analysis,and manuscript;Bonelli S provided documentation and critical feedback;Viglione V contributed to the design and implementation of the research;Faldini C revised the manuscript critically and gave final approval of the version to be published;and all authors read and approved the final manuscript.
The authors declare that they have no competing interests.
The fisherman went home, and when he came near the palace he saw that it had become much larger, and that it had great towers and splendid ornamental12 carving13 on it
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial(CC BYNC 4.0)license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See:https://creativecommons.org/Licenses/by-nc/4.0/
Italy
Antonio Mazzotti 0000-0001-9974-4787;Alberto Arceri 0000-0002-6486-6300;Simone Zielli 0000-0003-0867-1338;Simone Bonelli 0000-0001-6704-8509;Valentina Viglione 0000-0002-0539-1333;Cesare Faldini 0000-0001-8152-4778.
Wang JJ
Wang TQ
Wang JJ
 World Journal of Orthopedics2022年3期
World Journal of Orthopedics2022年3期
- World Journal of Orthopedics的其它文章
- Impact of enhanced recovery pathways on safety and efficacy of hip and knee arthroplasty:A systematic review and meta-analysis
- Surgical treatment of femoral deformities in polyostotic fibrous dysplasia and McCune-Albright syndrome:A literature review
- Plate vs reverse shoulder arthroplasty for proximal humeral fractures:The psychological health influence the choice of device?
- Diagnostic role of Xpert-MTB RIF assay in osteoarticular tuberculosis:A retrospective study
- Comparative study of intertrochanteric fracture fixation using proximal femoral nail with and without distal interlocking screws
- Ilizarov bone transport combined with the Masquelet technique for bone defects of various etiologies(preliminary results)