
Impact of enhanced recovery pathways on safety and efficacy of hip and knee arthroplasty:A systematic review and meta-analysis
2022-04-06 01:31:38MarionJLFHeymansNanneKortBarbaraAMSnoekerMartijnGMSchotanus
World Journal of Orthopedics 2022年3期
INTRODUCTION
The numbers of hip and knee arthroplasties performed worldwide are growing as a result of the increased incidence of osteoarthritis[1-5].With the increasing life expectancy,hip and knee osteoarthritis will become a significant health issue in the upcoming years[6]and thereby arthroplasty surgeries will increasingly be performed.Clinical pathways(CPs)have been introduced to improve the quality of hip and knee arthroplasty,by optimizing recovery,minimizing variation in care,and reducing costs[7,8].Due to scientific advancement,innovation,and novel technologies,CPs for hip and knee arthroplasty are continuously being changed.The enhanced recovery pathways(ERP)are based on novel evidence,while regular pathways are not necessarily based on the latest evidence.Because the optimizations in CPs are accomplished with an increase in costs,time,and resources[9],but might also be able to reduce costs in the long term[10],it is essential to gain knowledge on the actual benefits of the ERP.Therefore,we included all ERP studies for hip and knee arthroplasty and investigated the impact of the optimization process.This study,as far as we know,is the most extensive systematic review(SR)and meta-analysis on CPs for hip and knee arthroplasty.
The purpose of this SR and meta-analysis was to investigate the effect ofcompared tofor total hip arthroplasty(THA),total knee arthroplasty(TKA),and/or unicompartmental knee arthroplasty(UKA)on(serious)adverse events[(S)AEs],readmission rate,length of hospital stay(LoS),clinician-derived clinical outcomes(Knee- and Hip Society Scores),patient reported outcome measures(PROMs),and costs.This present SR and meta-analysis is complementary to previous reviews[1,11-18].
MATERIALS AND METHODS
A review protocol was developed according to the Preferred Items for Reporting Systematic Reviews and Meta-Analysis(PRISMA-P)statement[19]and registered in PROSPERO,the International Prospective Register of Systematic Reviews,in September 2016(CRD42016040210).
Literature search
A systematic literature search in five key healthcare databases was conducted(MH).Embase.com,PubMed,Wiley/Cochrane Library,Clarivate Analytics/Web of Science,and Ebsco/CINAHL were searched from inception until June 10,2018.Three trial registers were searched to identify ongoing unpublished trials,including the World Health Organization portal,ClinicalTrials.gov,and PROSPERO.The first terms used,including all synonyms,were ‘knee arthroplasty’ or ‘hip arthroplasty’ combined with ‘clinical pathways’ or ‘enhanced recovery’ or ‘a(chǎn)mbulatory care’ or ‘outpatients’.There was no restriction on language or publication type or date.
And now the King s son had it carried away by his servants on their shoulders. And it happened that they stumbled over a tree-stump28, and with the shock the poisonous piece of apple which Snow-white had bitten off came out of her throat. And before long she opened her eyes, lifted up the lid of the coffin, sat up, and was once more alive. Oh, heavens, where am I? she cried. The King s son, full of joy, said, You are with me, and told her what had happened, and said, I love you more than everything in the world; come with me to my father s palace, you shall be my wife.
Eligibility criteria
Randomized controlled trials(RCTs)and observational studies written in English,comparing within the studies ERP with the foregoing regular pathway,including patients 18 years or older undergoing THA,TKA,and/or UKA,were included.At least one of the following outcomes needed to be evaluated for inclusion for one of the arthroplasties:(S)AEs,readmission rate,LoS,functional recovery,PROMs,and costs.Descriptive articles(historical articles)and studies investigating patients who underwent revision,fracture,or bilateral arthroplasty were excluded.
Study selection
The results of the literature search were collated and de-duplicated in RefWorks[20].All articles were screened on title and abstract independently by two reviewers(MH and MS).After retrieving and examining the full text of all potentially relevant articles,both reviewers indicated independently if the study should be included.Disagreements regarding study inclusion were resolved by consensus between the two reviewers.
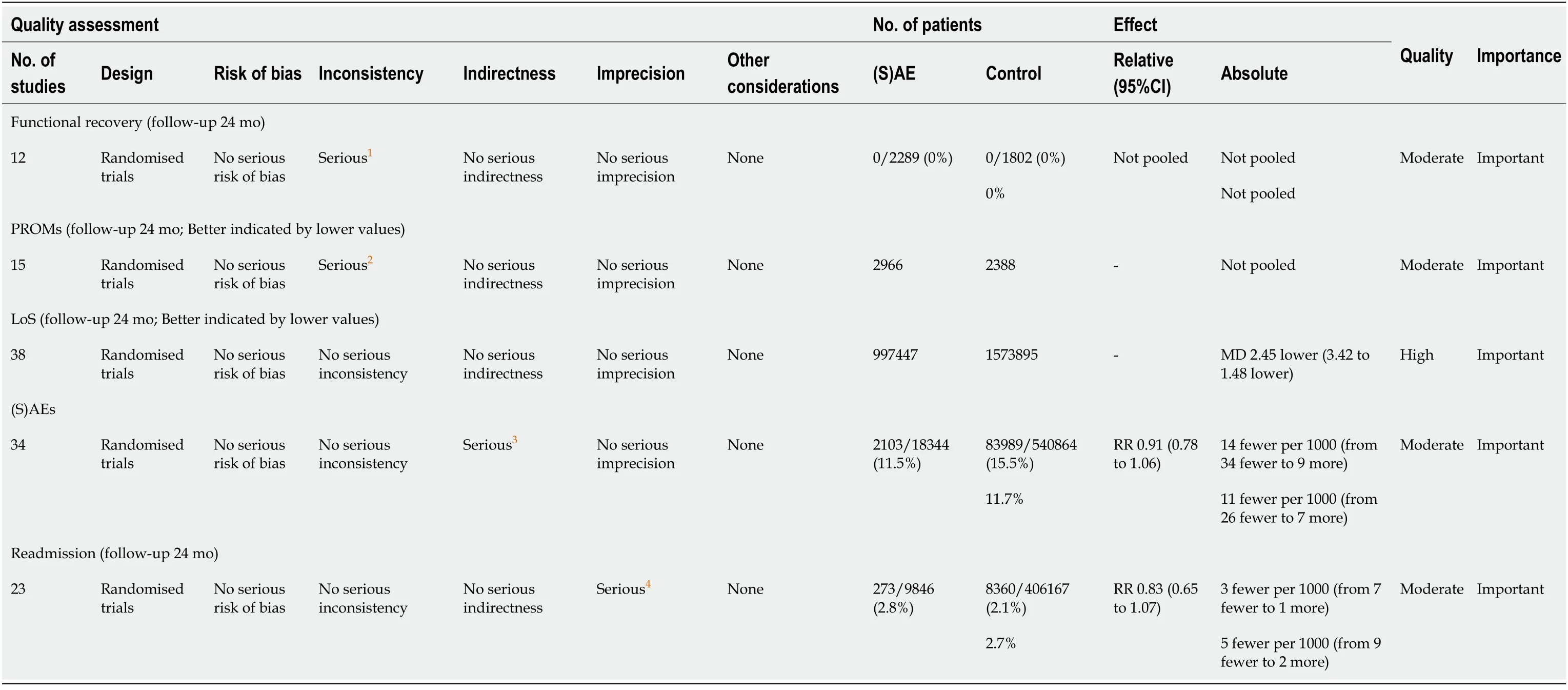
Sensitivity analyses of(S)AEs together with readmission rate resulted in a RR of 0.9(95%CI:0.7-1)with substantial heterogeneity(I= 84%,= 0.1).According to GRADE,there was moderate quality of evidence for(S)AE and readmission rate(Table 3).
Clinical pathways
We divided the CPs into ERP and regular pathways.It is challenging to get consensus on a definition for ERP[32],because of the different concepts of care under different health care systems.CPs with rapid or enhanced recovery,fast-track,day care,or outpatient surgery,including novel experimental evidence,are an updated version of the regular pathway and were defined as ERP.These pathways are continually evolving,aiming to improve the standard of care.Several factors may streamline these ERP,during the pre-,peri-,and/or post-operative stage.We used the definitions as stated by Galbraith[11]for the specific elements of ERP.The regular pathways,maintaining the standard or non-optimized program and containing the previous evidence,prescribe care as usual.The regular pathways were considered to be the initial procedures.A pragmatic approach was chosen to distinguish between regular and enhanced.Results between ERP and regular pathways were compared for(S)AEs,LoS,functional recovery,PROMs,and costs.
Outcomes
The following data were extracted systematically from the included papers by both reviewers(MH and MS):Author,publication year,study design,procedure,clinical pathways,number of participants,patients’ characteristics,country,and outcomes.We determined AEs as patient events and wound disorders,surgical and/or prosthesis related[3].SAEs were reported as undesired medical events,not necessarily associated with the treatment[22].Classification as AE or SAE was analyzed together as one outcome measure in(S)AE.Readmission rate was registered as the number of readmissions related to the hip or knee surgery.LoS was evaluated as time in days between hospital admission and discharge.Clinical outcomes were assessed in terms of functional recovery and with the use of PROMs.Costs included only intramural hospital costs and were reported in the monetary unit of the study.
Risk of bias
For all included studies,a risk-of-bias(RoB)table was used to identify potential sources of bias with the use of the Cochrane Collaboration tool[23]or the ROBINS-I tool[24]for RCTs and non-randomized studies,respectively.Two authors(MH and MS)independently assessed the RoB.The outcomes of all studies were reported using Grading of Recommendation,Assessment,Development and Evaluation(GRADE)[25].
Statistical analysis
Pigeons are considered death omens89 in some superstitions91. A strange pigeon, especially if white, alighting on the house or flying in front of one indicates death (Opie & Tatem 1989).Return to place in story.
RESULTS
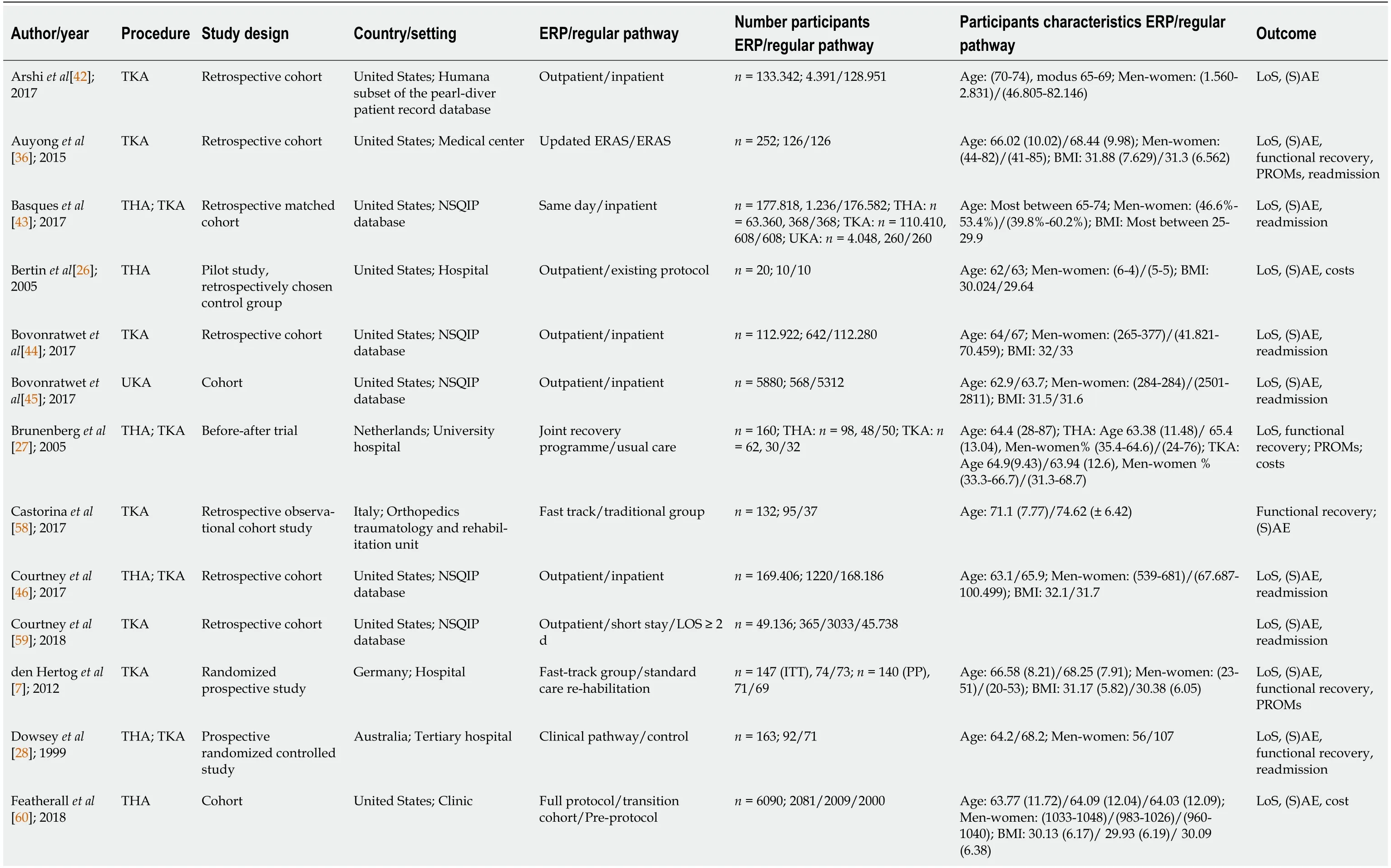
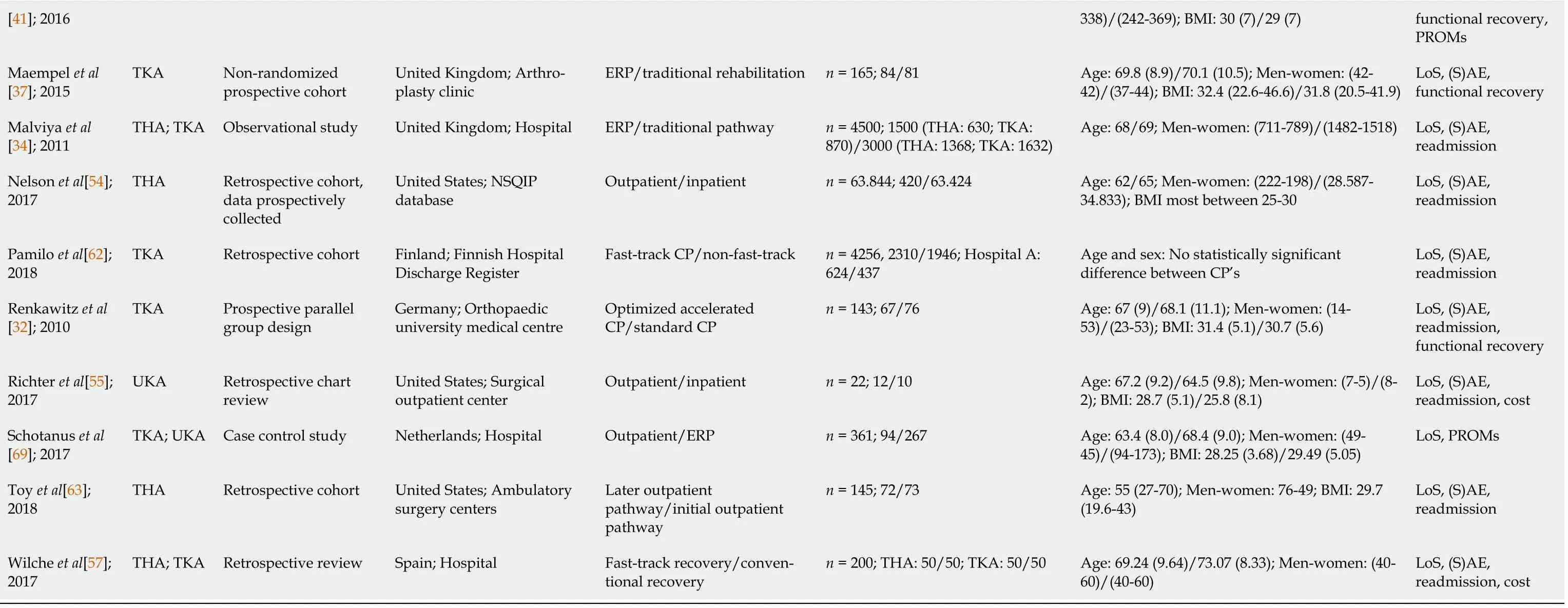
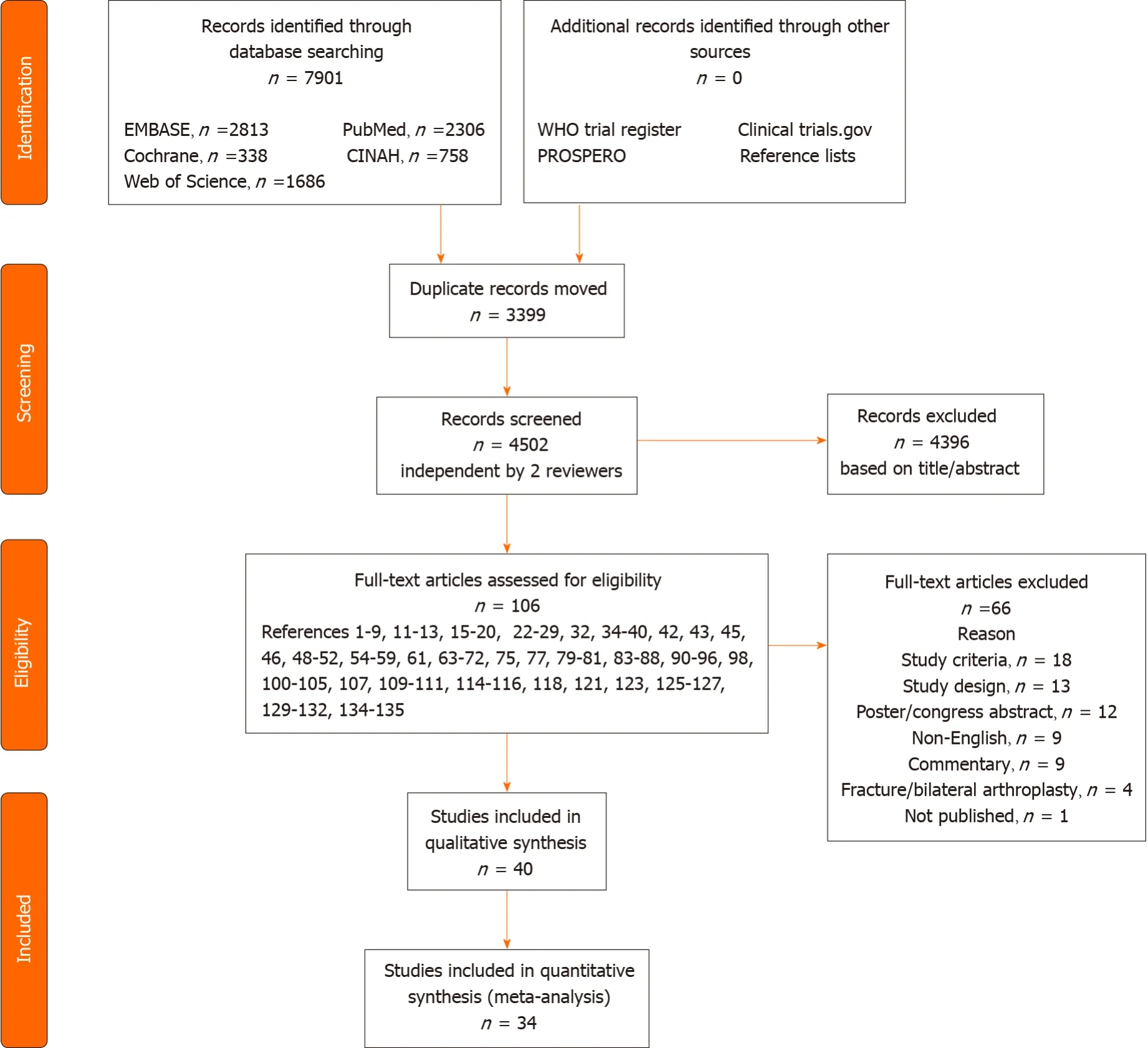
The full search strategies can be found in the Supplementary material(Databases and search strings).This systematic search identified 7901 references.The literature search and selection process are shown in Figure 1.After removal of duplicates,4502 references remained for screening on title and abstract.Of these,106 full-text articles were assessed for eligibility.No additional records were identified by checking reference lists.Eventually,40 studies were included[3,7,26-63].A summary of the characteristics of these studies is given in Table 1.
We included five RCTs[7,28,30,35,38],six prospective cohort studies[31,33,37,41,50,52],thirteen retrospective cohort studies[36,42-44,46,51,53,54,57-59,62,63],five observational cohort studies[27,34,45,47,60],four case control studies[3,48,49,56],four comparative studies with prospective[32,61]and retrospective designs for the standard CPs[39,55],and one each prospective pilot study[26],prospective follow-up study[29],and propensity score matched study[40].Nine articles studied THA[26,29,38,41,50,52,54,60,63],nineteen studied TKA[3,7,30-33,36,37,39,42,44,48,49,51,55,58,59,61,62],six studied UKA[3,43,45,48,55,56],and eleven studied both hip and knee arthroplasty[27,28,34,35,40,43,46,47,53,56,57].Of the included studies,which were published between 1999 and 2018,eighteen were conducted in the United States[26,30,31,36,38,40,42-46,51,53-55,59,60,63],five in the Netherlands[3,27,48,50,56],three each in the United Kingdom[34,37,41],Germany[7,32,33],and Canada[35,49,61],two in Spain[29,57],and one each in Australia[28],Malaysia[39],Italy[58],New Zealand[47],Denmark[52],and Finland[62].The setting varied from a hospital[3,26,27,34,41,47,48,50,56,57,60-62]to a medical[36,40,42,43-46,53,54,59]or orthopedic center[7,35,37,38,51,52,55,58,63],a tertiary[28,30,49]or a university hospital[29,32,33,39],or a single institution[31].
Outcomes were summarized using RevMan 5.3[21].We extracted all data used from the original studies.To quantify the statistical heterogeneity in the studies,theIvalue was used.Only if studies were sufficiently clinically,methodologically,and statistically homogenous,the data were pooled in a meta-analysis.In case of considerable heterogeneity(>75%),a qualitative analysis was performed[23]and outcomes between included studies were described.In the situation where one of the sensitivity analyses showed no considerable heterogeneity(<75%),a meta-analysis was performed on this outcome.For the meta-analysis,we used a random effects model and report relative risk(RR)with 95%confidence interval(CI).We present the results within forest plots,subdivided for type of arthroplasty(THA,TKA,and/or UKA).If no distinction between the different arthroplasties was possible,analysis for the combined group were included as a subgroup(THA and/or TKA and/or UKA).In a sensitivity analysis,we also combined(S)AE with a follow-up time of 30 d or more and readmission rate as one combined outcome,as they are interrelated in clinical practice.Studies for(S)AE with a follow-up time of 30 d or more were analyzed because of their clinical relevance.value ≤ 0.05 was considered statistically significant.
How was he to find his father and mother, and bring them back to life, if they were lying at the bottom of that horrible water? He turned away sadly and wandered back into the streets, hardly knowing where he was going; when a voice behind him cried: Stop, prince, I have caught you at last! It is a thousand years since I first began to seek you
I must be more tired than I thought, he said to himself, and, after telling them to be sure to wake him next morning at eight o clock, he went to bed


Risk of bias
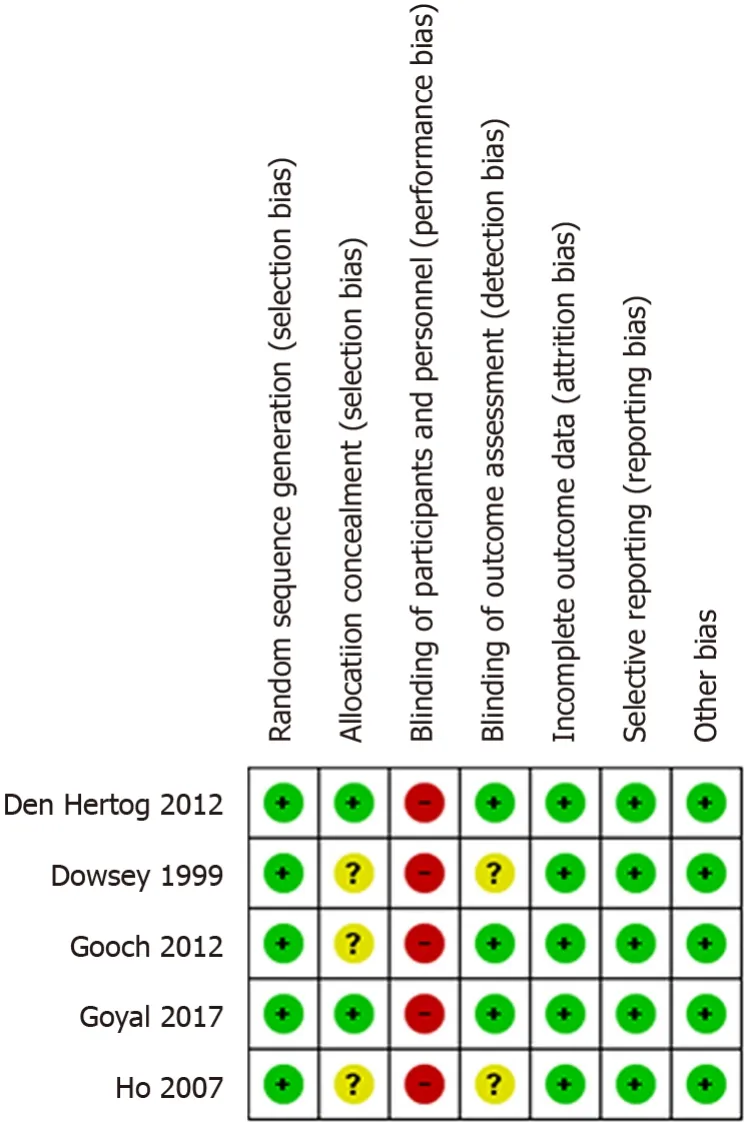
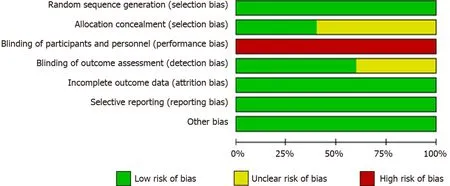
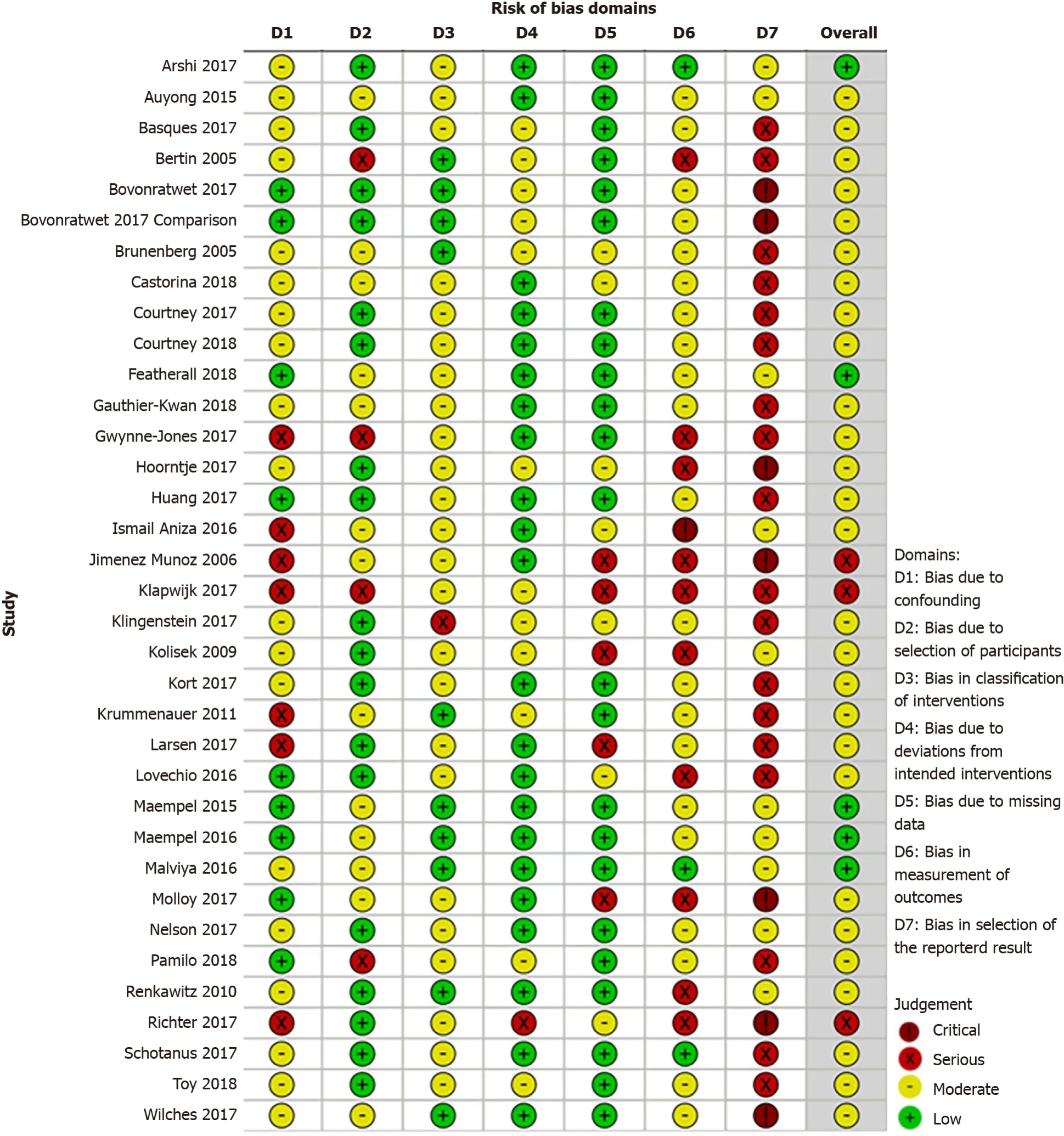
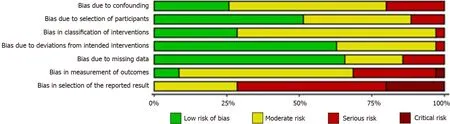
The methodological quality is presented in a RoB summary(Figures 2 and 4)and as percentages(Figures 3 and 5)for the RCTs and non-randomized studies,respectively.Blinding of participants and personnel was not possible because of the content of the CPs.Selection bias was unclear in three RCTs(60%)and blinding of outcome in two RCTs(40%).Five non-randomized studies were of high quality with a low RoB,whereas three were of low-quality with a serious RoB.All low-quality studies had bias due to confounding.A serious or critical bias in the selection of the reported results was found in the majority of studies(71%).In 31% of the studies,the outcome could have been influenced by knowledge of the applied CPs.Five studies reported missing data(14%),and four had bias due to selection of participants(11%).Overall,the methodological quality of the included studies ranged from average togood.
Heterogeneity
The studies varied clinically(,patient characteristics and CPs)and methodologically.Different measurement tools were used,and outcome measures were reported in different ways across studies.Therefore,a meta-analysis was only feasible with studies that used the same measurement tools.For this study,data for the sensitivity analyses were pooled for(S)AEs and readmission rate.A qualitative analysis was performed for the results of LoS,functional recovery,PROMs,and costs.
(S)AEs and readmission rate
Thirty-five studies examined AEs,SAEs,or both[3,7,26,28-32,34-47,49-52,54,55,57-63]and twenty four examined readmission rate[3,28,31,32,34,36,38,39,40,43-47,49,51-52,54,55,57,59,61-63].The follow-up timevaried from 8 d up to 24 mo postoperatively.
Then he called one of his lords-in-waiting, who was so high-bred, that when any in an inferior rank to himself spoke to him, or asked him a question, he would answer, “Pooh,” which means nothing.
The most important findings of the present SR and meta-analysis were that the use of ERP yielded similar or improved outcomes for patients with hip and/or knee arthroplasty.In the ERP,there were less(S)AEs and a lower readmission rate when compared to the regular pathways.The readmission rate in the ERP was statistically significant different in favor of the knee arthroplasties without heterogeneity.There were improved results for clinician-derived outcomes and PROMs,reduced LoS,and saved costs compared to regular pathways.
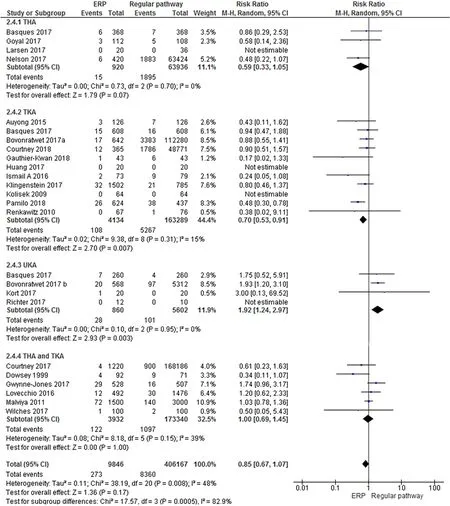
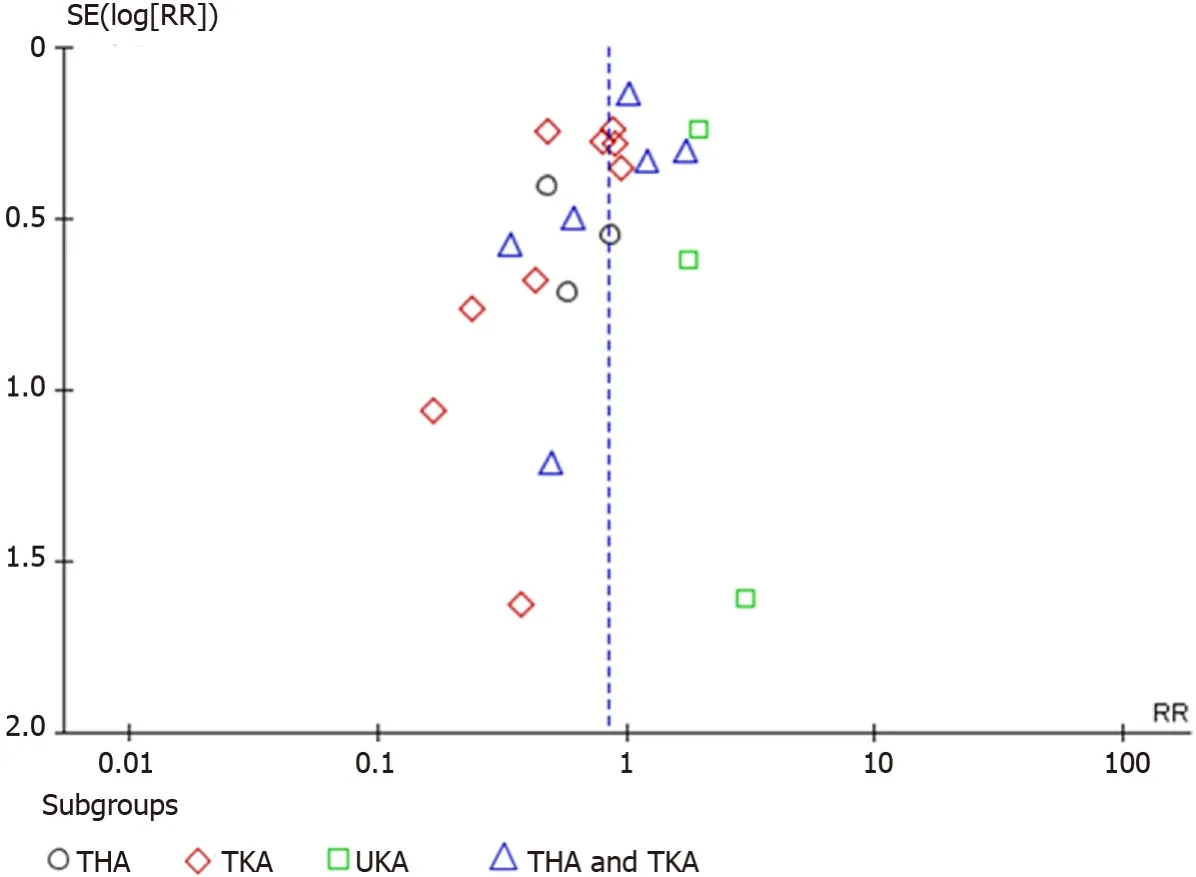
The analyses for readmission rate were homogenous(I= 48%,= 0.2).The readmission rate in ERP was statistically significant different in favor of the knee arthroplasties without heterogeneity(TKA:I=15%,= 0.01;UKA:I= 0%,= 0.01).The plots for readmission rate for THA,TKA,UKA,and the combined subgroups(THA and TKA)are shown in Figures 8 and 9.
The gardener was watching; but as the angel was standing by, he was afraid and thought the maiden14 was a spirit, and was silent, neither did he dare to cry out, or to speak to the spirit
One reviewer(MH)extracted and added data into Review Manager(RevMan)[21]and the other(MS)verified the accuracy of the data;disagreements were resolved by discussion and if no agreement was reached,by the involvement of a third reviewer(BS).
Length of hospital stay
Thirty-eight studies described LoS[3,7,26-34,36-57,59-63].A reduced LoS was found in all ERPs,of which 20 studies reported a statistically significant reduction ranging between 0.5-10.1,3.2-10.0,2.8-7.1,and 2.6 d for the THA[29,41,50,52,60,63],TKA[7,30,32,36,37,39,62],the combined outcome of THA and TKA[27,28,34,47,53,57],and UKA[3],respectively.The overall median LoS reduced up to 6.5 d.For regular pathways,the median values were between 0.5 and 16 d and the mean values were between 1.5 to 19.5 d.All the analyzed arthroplasties showed high heterogeneity for LoS(>I= 98%).The GRADE table shows high evidence for LoS(Table 3).
Clinician-derived outcome and PROMs
Functional recovery was assessed in 13 studies for THA[38,41,50],TKA[7,31,32,36,37,58,61],and the combined subgroup THA and TKA[27,28,35],respectively.The Harris Hip Score,Range of Motion,and scores from the American Knee Society were mostly reported.Four articles studied THA[38,41,50,52],six studied TKA[7,31,33,36,56,61],and three each studied UKA[3,48,56]and both THA and TKA[27,35,47]regarding the PROMs,using similar measurement types.The Western Ontario and McMaster Universities Osteoarthritis Index(WOMAC)questionnaire,EuroQual,Oxford Knee Score,and pain scales were mostly used as PROMs.
The follow-up time differed from the first postoperative day up to 24 mo postoperatively.In view of the clinician-derived outcomes and PROMs,the results in the ERP were similar or improved for THA[41,50,52],TKA[31-33,58,61],UKA[48],and the combined group THA and TKA[27],or were statistically significant better than those in the regular pathways for TKA[7,36,56],UKA[3],and the combined group THA and TKA[35,47].Moderate quality for functional recovery and PROMs is presented in GRADE(Table 3).
Costs
Nine observational studies analyzed costs[26,27,30,33,49,53,55,57,60].The reduction in LoS resulted in statistically significant cost savings for THA in an ERP compared to the regular pathways[26].Preadmission,physical therapy,and home care charges resulted in a saving for the combined group(THA and TKA)per patient[27]and reduced hospital costs after TKA[30].Hospital costs were reduced significantly in patients operated for knee arthroplasty in an ERP because of the reduction in room costs,fewer laboratory tests,used medications,physical therapy,and meal costs[30,49,55].The cost reduction per patient for knee arthroplasty was in favor of the ERP[27,30,33,49,55,57],with a range between €109 and $20573.The cost savings per patient for hip arthroplasty was also higher for the ERP[26,27,57,60]with a range between €581 and $2500.The ERP resulted in a statistically significant economic saving for both knee and hip arthroplasty[49,55,57,60]without affecting complication rate[34],functional improvement,and satisfaction of the patient operated after THA or UKA[26,55].The individual cost/benefit relation was inferior only in one TKA study[33].
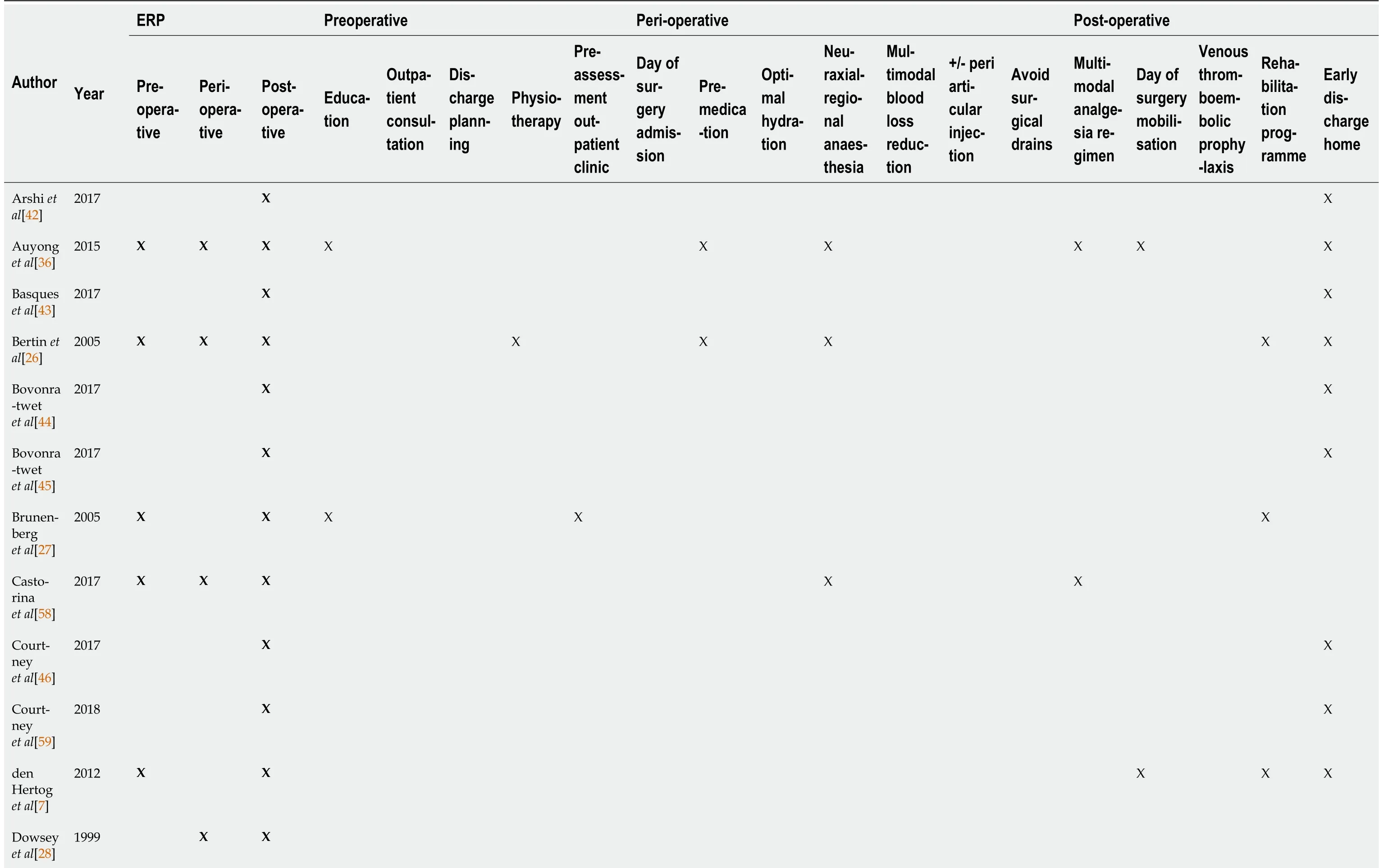
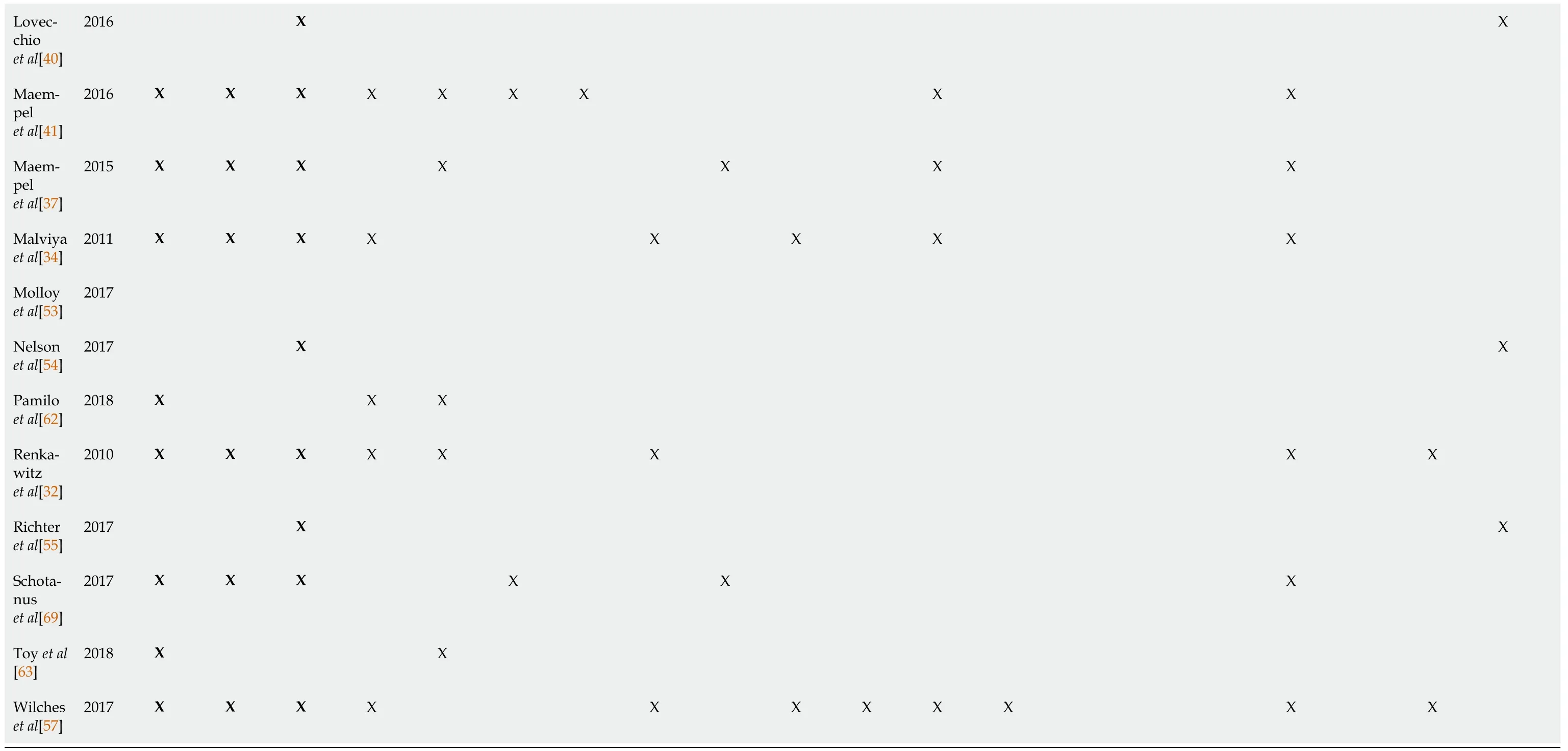
The total sample size consisted of 2223534 patients undergoing hip or knee arthroplasty;997765 patients were treated according to ERP compared with 1225769 patients with regular pathways(Table 1).Overall,more female patients were included(60.1%).Of 5095(0.2%)patients,sex was not reported.The mean age was 65.1 years for patients with ERP and 66.5 years for those with regular pathways.The mean body mass index was similar for both CPs(30 kg/m).In ERP,25 studies applied enhanced elements during the pre-operative phases,mostly for education[27,32-36,41,47,50,52,57,61,62],19 applied during the peri-operative phase,for pre-medication or neuraxial-regional anesthesia[3,26,34-37,41,47,50,57,58,60],and 35 during the postoperative phase,mostly for the rehabilitation program or early discharge home[3,7,26,27,29,31,32,35,36,38,40,42-49,51,54,55,57,59-61].An overview of the pre-,peri-,and postoperative management during ERP is listed in Table 2.
DISCUSSION
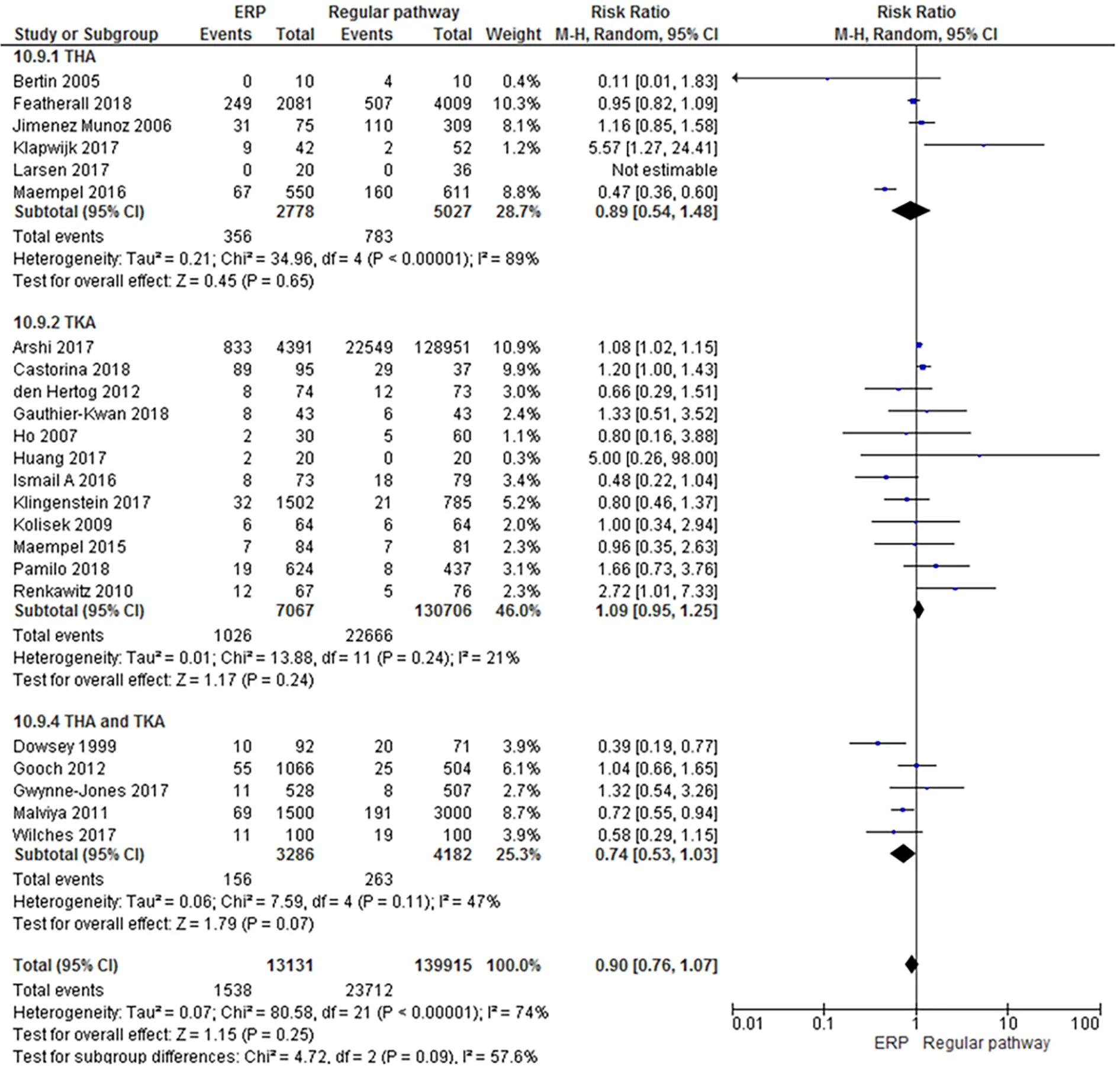
In the ERP,there were less(S)AEs(RR:0.9;95%CI:0.8-1)and a lower readmission rate(RR:0.8;95%CI:0.7-1)when compared to the regular pathways.The analyses for overall(S)AEs resulted in considerable heterogeneity(I= 83%,= 0.2).Studies of(S)AEs with a follow-up time of 30 d or more yielded a RR of 0.9(95%CI:0.8-1),with substantial heterogeneity(I= 74%,= 0.3)(Figures 6 and 7).Only the THA subgroup showed heterogeneity(I= 89%,= 0.7)while the TKA(I= 21%,= 0.2)and the combined groups(THA and TKA;I= 47%,= 0.1)were homogeneous.
Then the witch got up and laid about her among the plates and dishes, so that the pieces flew about their ears, just as she had done when she was cheated the first time
Multiple enhancements can be taken during the pre-,peri-,or post-operative program,to upgrade a regular pathway to enhanced,with respect to local situations.Continuously looking for improvements is important for successful hip and/or knee CPs.
Explanation of findings
The overall methodological quality varied due to the inclusion of five RCTs and 35 observational studies.The studies were heterogeneous regarding patient populations,hospital resources and procedures,multi-disciplinary teams,surgical and anesthetic techniques,practice variation,and followup times.Most of the heterogeneity was probably due to methodological differences between the included studies.The included studies were published throughout the past 20 years,the view of hospital stays after an operation and discharge criteria have been changed over time.And,the obtained data came from different healthcare systems from different countries,from retrospective studies or from national registries.Nevertheless,even within all this practical and methodological variation,the outcomes indicated a positive effect in favor of ERP.
The results of the meta-analysis demonstrated less(S)AEs in patients following the ERP,with fewer readmissions compared to the regular pathways(= 0.25).Substantial heterogeneity was present when AE and SAE were analyzed together and separately for the different arthroplasties(THA,TKA,and both combined).This heterogeneity was probably due to the lack of definition in primary studies.Also,not all studies made a distinction between AE and SAE.For further investigation,consensus on terminology is recommended.Compared to our findings,another study found statistically significant fewer complications for the ERP compared to the regular pathway[18].Because of the relative high risk of postoperative complications,careful patient selection for outpatient joint arthroplasty is crucial to obtain successful outcomes[42,44-46,54,63].
All studies showed a reduction in LoS after implementing ERP.In half of these studies,this reduction was statistically significant,which is in line with previous SRs[13,17,18].LoS can be influenced by preoperative patient education and patient expectations[11,27,28,31,36,37,41,48,57,62,64,65],training in home-based rehabilitation settings[3],and a positive influence from relatives[28,52,53].The discharge also influenced LoS from the hospital to a rehabilitation center or a center with care facilities instead of discharge to the home environment[28,32,33,47,50].The reduction of LoS allowed more joint replacements without additional bed capacity and could therefore have a potential positive economic effect[34].
Implementation of CPs for hip and knee arthroplasty were associated with similar or improved outcome for clinician-derived outcome and PROMs.These outcomes represent the best subjective measurement of clinical outcome[66].However,there is no single best outcome measurement tool after arthroplasty.Besides the positive results of PROMs,various scores are not capturing changes due to a lack of power as averse to a lack of change,floor and ceiling effects[67].It could therefore be that further improvement in one of the CPs was not detected.In order to characterize the objective changes in physical activity after arthroplasty in detail,activity monitoring can be used to capture changes over time and to detect potential objective differences[68,69].
This study indicated that patients in the ERP had a substantial reduction in hospital costs,mainly explained by the shorter stay.With a hip arthroplasty incidence of 468000,national cost savings of CP implementation would amount to greater than $1.2 billion annually in costs from a payer perspective in the United States[60].For joint arthroplasty,the mean hospital cost from 2002-2013 increased about 50%,as a result of rising total joint arthroplasties and prices of implants[53].Long waiting lists and the contribution to health expenditure growth since joint replacement are expensive interventions,and the increasing economic burden on public healthcare providers should also be taken into account[1,70].Besides,the improvement of CPs is accomplished with investment in training,knowledge,and adjustments to daily practice for the surgeon,nurse,and physiotherapist[3,58,71].Establishing the real cost and saving obtained by a CP can be complicated.Savings also depend on charge systems and reimbursement[55,57].
” Kay’s fingers were very artistic4; it was the icy game of reason at which he played, and in his eyes the figures were very remarkable5, and of the highest importance; this opinion was owing to the piece of glass still sticking in his eye
Strengths and limitations
The lack of a clear definition for regular pathways and ERP makes it difficult to pool results and compare between large groups of studies.By pointing out the enhanced aspects,we tried to solve this limitation as much as possible.
Due to the high heterogeneity,it was only possible to perform a meta-analysis for(S)AEs and readmission rate for the different arthroplasties.Although a cut-offIvalue of 75% has been chosen beforehand,we also present results that exceed this limit,to indicate the trend,(S)AEs with a follow-up of 30 d or more in the THA(I= 89%,= 0.7).
Some limitations should be noted.Due to methodological as well as statistical heterogeneity,a metaanalysis could not be performed for most outcomes.In most of these studies,a high RoB was present,which could have overestimated our results.Selection bias occurred due to the lack of randomization.Performance bias was present because the staff and patients were not blinded to the CP strategy.Clinical bias during data collection was possible because data from large databases were used.Reporting bias is a problem in primary studies because of the selective reporting of outcomes.
The strengths of this review include an extensive literature strategy.All included studies compared outcomes from an enhanced recovery pathway with a regular pathway.Data from a large population of over 2 million patients were analyzed,including both hip and/or knee arthroplasty,with different follow-up times and outcome measures.Even,an update with the recent literature will provide comparable insights to continuously updating CPs to achieve the most optimal results for patients,professionals,and organizations.
CONCLUSION
Based on the present SR and meta-analysis,it can be concluded that ERPs for hip and/or knee arthroplasty can result in less SAEs with reduced readmission rate and length of stay,and similar or improved clinical outcomes and PROMs with financial benefits,when compared to regular pathways.
ARTICLE HIGHLIGHTS
Research background
Over the past 20 years,clinical pathways(CPs)for total knee and hip arthroplasty have been evolved and optimized.Based on novel evidence and new standards,at this moment we can safely discharge patients on the day of surgery.Whereas in the past,2-wk bed rest was the standard.
Research motivation
A clinical pathway is a stochastic process that needs to be updated with the latest evidence so the hospital,orthopedic surgeon,and other staff involved in this multidisciplinary approach will be satisfied,with financial benefits for the hospital and improved outcome for the patients.Although,these days in modern medicine,orthopedic surgeons,nurses and hospital staff still needs to be convinced by these optimized CPs.For this reason,we did this systematic review and meta-analysis.
Research objectives
The aim of the present review was to compare the effect of enhanced recovery pathways with regular pathways for adult patients with elective hip and/or knee arthroplasty for(serious)adverse events[(S)AEs],readmission rate,length of hospital stay(LoS),clinician-derived clinical outcomes,patient reported outcome measures(PROMs),and costs.
Research methods
A systematic literature search was conducted in EMBASE,PubMed,Cochrane Library,Web of Science,and CINAHL.All relevant studies were considered for analysis based on the defined eligibility criteria.For the included studies,the risk of bias was assessed.Data for sensitivity analysis were pooled for(S)AE and readmission.A qualitative analysis was performed for the results of LoS,clinician-derived outcome,PROMs,and costs.
Research results
A total of 40 studies were included,34 in meta-analysis and 40 in qualitative analysis,with data of more than 2 million patients.The meta-analysis presented less(S)AEs in patients following the enhanced recovery pathways(ERP),with fewer readmissions when compared to the regular pathways.The readmission rate was statistically different in favor for the knee arthroplasties without heterogeneity.A reduced LoS was found in all ERP,and in half of these studies,this reduction was statistically significant.The implementation of CPs for hip and knee arthroplasty was associated with similar or improved outcome for clinician-derived outcome and PROMs.ERP were reported to be cost effective.The overall outcomes of all studies reported using Grading of Recommendation,Assessment,Development and Evaluation,presented moderate or high quality of evidence.
Research conclusions
The implementation of ERP for hip and/or knee arthroplasty results in improved clinical and patient related outcomes with financial benefits,compared to regular pathways.
Research perspectives
Based on the results presented,we recommend orthopedic surgeons worldwide,to keep optimizing their standard pathway with the latest evidence.This paper highlights the importance that regular pathways for hip and knee arthroplasty continuously need to be updated according to the latest scientific evidence,which can result in improved clinical outcomes with satisfied patients and financial benefits for patients,healthcare organizations,and hospital management.In this context,high-quality care for hip and/or knee arthroplasty can be achieved.
FOOTNOTES
Heymans MJ designed the study,gathered and analyzed the data,wrote the initial draft of the manuscript,and managed the study;Kort NP is initiator of pathway optimization;Snoeker BA ensured the accuracy of the data;Schotanus MG conceived the study,analyzed the data,and wrote the manuscript;Kort NP,Snoeker BA,and Schotanus MG revised the manuscript;and all authors read and approved the final manuscript.
One author(Kort NP)is a paid consultant for Stryker and Zimmer-Biomet.The other authors declare that they have no conflicts of interest to disclose.
Then he called one of his lords-in-waiting, who was so high-bred, that when any in an inferior rank to himself spoke to him, or asked him a question, he would answer, “Pooh,” which means nothing.
Every step she took was as the witch had said it would be, she felt as if treading upon the points of needles or sharp knives; but she bore it willingly, and stepped as lightly by the prince’s side as a soap-bubble, so that he and all who saw her wondered at her graceful-swaying movements
The authors have read the PRISMA 2009 Checklist,and the manuscript was prepared and revised according to PRISMA 2009.
The troll, therefore, sentenced the king, either to answer three questions that he would put to him, or have his head taken off, as was agreed on in the old bond
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial(CC BYNC 4.0)license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See:http://creativecommons.org/Licenses/by-nc/4.0/
Netherlands
Marion JLF Heymans 0000-0002-0096-5203;Nanne P Kort 0000-0001-9769-371X;Barbara AM Snoeker 0000-0002-5420-9200;Martijn GM Schotanus 0000-0002-3975-6337.
Wang JJ
To my Lord Marquis of Carabas, replied the reapers, and the King was very well pleased with it, as well as the Marquis, whom he congratulated thereupon. The Master Cat, who went always before, said the same words to all he met, and the King was astonished at the vast estates of my Lord Marquis of Carabas.
Wang TQ
18. Came to a large town: Zipes translates it as city (Complete 193).According to Biedermann, in the symbolgoly of the psyche61, the city stands for the regularized center of a person s life, which can often be reached only after long travels, when a high degree of emotional maturity62 has been attained63 and the gate to the spiritual center of one s life can be traversed (72).
Li X
 World Journal of Orthopedics2022年3期
World Journal of Orthopedics2022年3期
- World Journal of Orthopedics的其它文章
- Surgical treatment of femoral deformities in polyostotic fibrous dysplasia and McCune-Albright syndrome:A literature review
- Plate vs reverse shoulder arthroplasty for proximal humeral fractures:The psychological health influence the choice of device?
- Diagnostic role of Xpert-MTB RIF assay in osteoarticular tuberculosis:A retrospective study
- Comparative study of intertrochanteric fracture fixation using proximal femoral nail with and without distal interlocking screws
- Ilizarov bone transport combined with the Masquelet technique for bone defects of various etiologies(preliminary results)
- Accuracy of shoulder joint injections with ultrasound guidance:Confirmed by magnetic resonance arthrography