
Should we use similar perioperative protocols in patients undergoing unilateral and bilateral one-stage total knee arthroplasty?
2022-01-22 08:44:32ArtitLaoruengthanaPitiRattanaprichavejParinSamapathBhuwadChinwatanawongwanPariphatChompoonutprapaKritPongpirul
World Journal of Orthopedics 2022年1期
INTRODUCTION
Total knee arthroplasty (TKA) is widely accepted as one of the most effective and safe surgical procedures for treating severe osteoarthritis (OA) of the knee.Currently, advances in anesthesia, surgical techniques, and perioperative care, including multimodal pain management and accelerated rehabilitation, have improved functional recovery and shortened the length of the hospital stay for patients undergoing unilateral total knee arthroplasty (UTKA)[1].There have also been contemporary blood-conserving methods published that substantially decrease the rate of postoperative blood transfusions when kept below 10%[2-4].
Then he put on another, and whir, whir, whir, the wheel went round three times, and the second too was full; and so it went on till the morning, when all the straw was spun away, and all the bobbins were full of gold
Approximately 25% of patients undergoing UTKA have bilateral OA knees[5] and subsequently will undergo contralateral TKA within 1 year[6].Thus, bilateral onestage total knee arthroplasty (BTKA) is now in greater use as an alternative option for patients with bilateral OA knees because of the potential advantages that include single anesthesia, reduction in total hospitalization and rehabilitation time, as well as overall costs[7].However, the safety of BTKA is still debated because of perioperative morbidity that is associated with greater blood loss and a higher risk of cardiovascular adverse events than UTKA[8,9].Various blood-conserving strategies including regional anesthesia, tourniquet use and deflation after wound closure, femoral canal occlusion, and use of tranexamic acid (TXA) are commonly implemented in patients having BTKA with documented efficacy[10].However, recently published studies revealed that blood loss after BTKA ranged between 874 and 1067 mL, and blood transfusion rate ranged between 24% and 44% even if TXA was administered[11-13].
The substantial blood loss related to BTKA may subsequently cause occult hypoperfusion of vital organs such as the heart and kidneys.Conversely, requirements for blood transfusions may also increase the risk of complications such as allergic reaction, cardiovascular volume overload, and subsequent heart failure or pulmonary edema[14,15].The risk of myocardial infarction (MI) has been reported to significantly increase among the TKA group during the immediate postoperative phase when compared to the non-surgical group[16,17].Taking data from the National Hospital Discharge database, 1.1% of patients were diagnosed with cardiac complications in the 90 d after TKA, and BTKA had a higher rate than UTKA (2.0%1.7%)[18].Therefore, these findings may emphasize the need for extensive perioperative care and monitoring to avoid such complications in BTKA.
Bilateral one-stage total knee arthroplasty (BTKA) is a notable option for patients with bilateral end-stage knee arthropathy because of the potential advantages that include reduction in total hospitalization and rehabilitation time, as well as overall cost.
MATERIALS AND METHODS
The study received institutional review board approval for retrospective analysis of data recorded prior to initiation and has been registered as TCTR20181220001.The authors’ criteria for BTKA were painful bilateral end-stage OA knees, and therefore the selection of BTKA or UTKA was based upon patient preference.Consecutive patients who had undergone UTKA and BTKA for primary OA, performed by a single surgeon between January 2016 and December 2019, were enrolled in the study.The exclusion criteria of this study were patients with a history of prior knee surgery or previous knee infection.Participants with an American Society of Anesthesiologists (ASA) score > 3, known cardiopulmonary comorbidity or high-sensitivity Troponin-T (hs-TnT) > 14 ng/L, CKD stage ≥ 3, or significant renal impairment (serum creatinine > 1.5 mg/dL) were also excluded.
All the UTKA and BTKA were performed by a single surgeon with identical pre-, peri-, and postoperative protocols.Regional anesthesia, prophylactic intravenous antibiotics (ATB), and tourniquet control at 250 mmHg were applied for all patients.A medial parapatellar approach was performed through an approximately 10 cm midline skin incision, the cruciate ligaments were excised, and conventional instruments were then used to prepare the proximal tibial and distal femoral bone cuts by using extramedullary and intramedullary reference guides, respectively.A bone plug was applied to occlude the opening hole of the distal femur after finishing all the bone cuts.Soft tissue balancing was performed to achieve appropriate flexion and extension gaps.The patella was selectively resurfaced.Before prosthesis implantation, local infiltration anesthesia (LIA) was induced by injecting Bupivacaine (0.5% Marcaine; AstraZeneca, Sweden), 30 mg of ketorolac tromethamine (ketorolac tromethamine 1 mL; SiuGuan, Taiwan), and sterile normal saline solution into the anterior and posterior compartment of the knee with the 2:1 ratio technique.All the patients received a fixed bearing, posterior stabilized prosthesis which was implanted with bone cement.A vacuum drain was then applied, and 15 mg/kg of topical tranexamic acid was poured into the knee joint before closure of the arthrotomy.The drain was clamped for 3 h and subsequently removed at 24 h after the surgery.
It appeared that they were working into the tapestry all the stories the Fairies liked best, and they began to try and teach me to help them, but from the first class, where they tried me to begin with, I sank lower and lower, and not even the most simple stitches could I learn
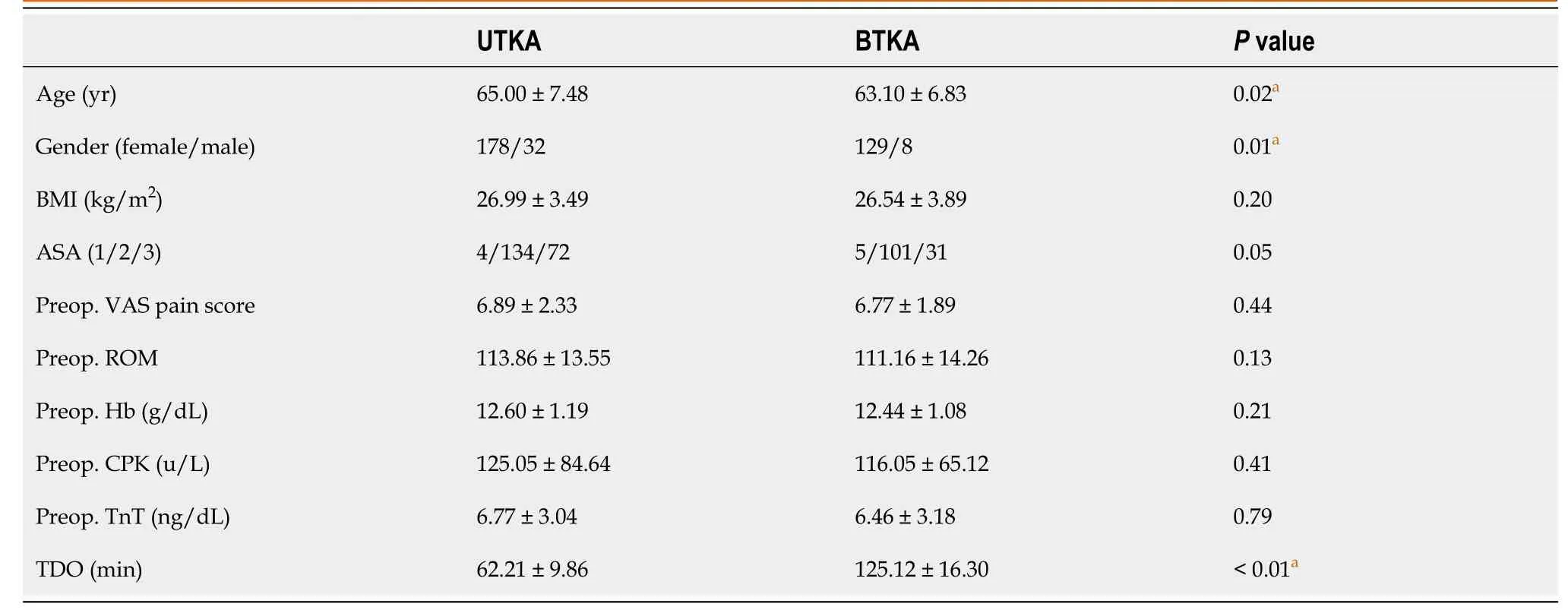
There were 210 UTKA and 137 BTKA included for analysis.The demographic and perioperative characteristics are briefly summarized in Table 1.Patients in the BTKA group were younger and more predominately female, and had a longer total duration of operation (TDO).
The patient's total blood volume (TBV) was calculated by the equation of Nadler[22].The difference between preoperative and lowest postoperative Hb was applied with the Hb balance method to determine PBL[2].
Males: TBV (mL) = [0.0003669 × height(cm)] + [32.19 × body weight (kg)] + 604
Females: TBV (mL) = [0.0003561 × height(cm)] + [33.08 × body weight (kg)] + 183
With a little kick from the inside he started the kettle off, and down the hill it rolled full tilt24; and when the fox came up, all that he saw was a large black kettle spinning over the ground at a great pace
You see, you can make anything happen if you commit to it and take action. Miracles like this happen every day-even in a city where there are no vans.
She was buried; two large tears rolled over the cheeks of theearnest man, and in the parsonage it was empty and still, for itssun had set for ever. She had gone home.
Serum Hb level that drops below 9.0 g/dL is indicated for blood transfusion for both the UTKA and BTKA at our institution.A hs-TnT level > 14 ng/L is considered as possible for MI in our laboratory system.Any complications and readmission rates at 90 d after the index surgery were recorded.
Statistical analysis
All demographic data and measured outcomes are summarized with descriptive statistics.Continuous data are presented as the mean and standard deviation, and Student’s-test was used to compare between the UTKA and BTKA groups.Categorical data which are presented as counts and percentages were compared by using Chi-square or Fisher’s exact test.Repeated-measures analysis of variance was applied to compare the time-dependent variables including VAS, ROM, SLR, Hb, CPK, and hs-TnT between groups.Thecomparisons of all pairwise points in time were applied to account for multiple testing with Bonferroni adjustments.A multiple logistic regression analysis was performed to determine which of these variables, including age, gender, body mass index (BMI), ASA physical status classification, and preoperative Hb, were the predictive factors for allogeneic blood transfusion.The sample size of the UTKA and BTKA groups had 99.5% power to detect a difference of 200 mL in PBL, which could significantly impact on blood transfusion rate, with standard deviation (SD) of 400 mL, and 95.4% power to ascertain a difference of 1.0 for VAS with SD of 2.5, with type I error of 5%.Stata/MP 15.0 software (StataCorp LP, College Station, TX, United States) was used for all statistical analyses.Statistical significance was defined as< 0.05.
The ball of apprehension4 in our stomachs grew during this takeoff in our overloaded5 aircraft. As we climbed up to our bombing altitude of twenty-six thousand feet, the other five planes in the squadron that I was leading joined us. Over the English Channel, the guns were test-fired and radio checks completed. We sped toward our target and dropped our load.
RESULTS
Data collected for analysis were patient demography, visual analogue scale (VAS) scores of postoperative pain, morphine consumption, range of knee motion (ROM), straight leg raise (SLR), length of stay (LOS), and laboratory evaluation comprising serum hemoglobin (Hb), blood transfusion rate, creatine phosphokinase (CPK), and hs-TnT preoperatively and at 24, 48, and 72 h after the surgery.
Blood loss
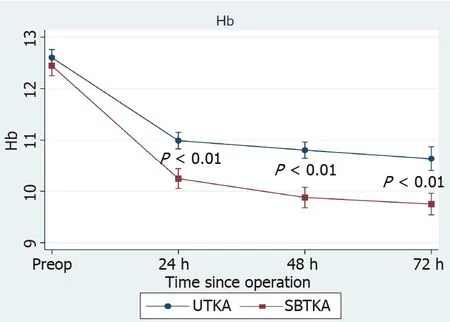
The postoperative Hb level of both groups gradually dropped and reached the lowest point at 72 h after the surgery.BTKA was associated with a significantly lower level ofHb than UTKA at 24, 48, and 72 h postoperatively (Figure 1).The PBL of the UTKABTKA group was 646.45 ± 272.26 mL1012.40 ± 391.95 mL (< 0.01), respectively.
There was once a fisherman and his wife who lived together in a little hut close to the sea, and the fisherman used to go down every day to fish; and he would fish and fish
Blood transfusion rates in UTKA and BTKA were 10.48% (22/210) and 40.88% (56/137), (< 0.01), respectively.For UTKA, 18 of 69 (26.09%) patients with preoperative anemia (defined as preoperative Hb < 12 g/dL in females and < 13 g/dL in males) received blood transfusion compared to 6 of 141 (4.26%) patients without anemia (< 0.01).Twenty-eight of 43 (65.12%) patients with preoperative anemia in the BTKA group required a transfusion, whereas patients without anemia had a transfusion rate of approximately 1 in 4 (26/94, 27.67%;< 0.01).The multivariate analysis demonstrated that preoperative Hb [odd ratio (OR): 0.33, 95% confidence interval (CI): 0.22-0.50,< 0.01] and BMI (OR: 0.90, 95%CI: 0.81-0.99,= 0.03) were predictive factors for blood transfusion in the BTKA group, whereas preoperative Hb (OR: 0.21, 95%CI: 0.12-0.37,< 0.01) was only a determinant in the UTKA group when using similar perioperative blood management and cut-off values for transfusion.
Postoperative pain and recovery
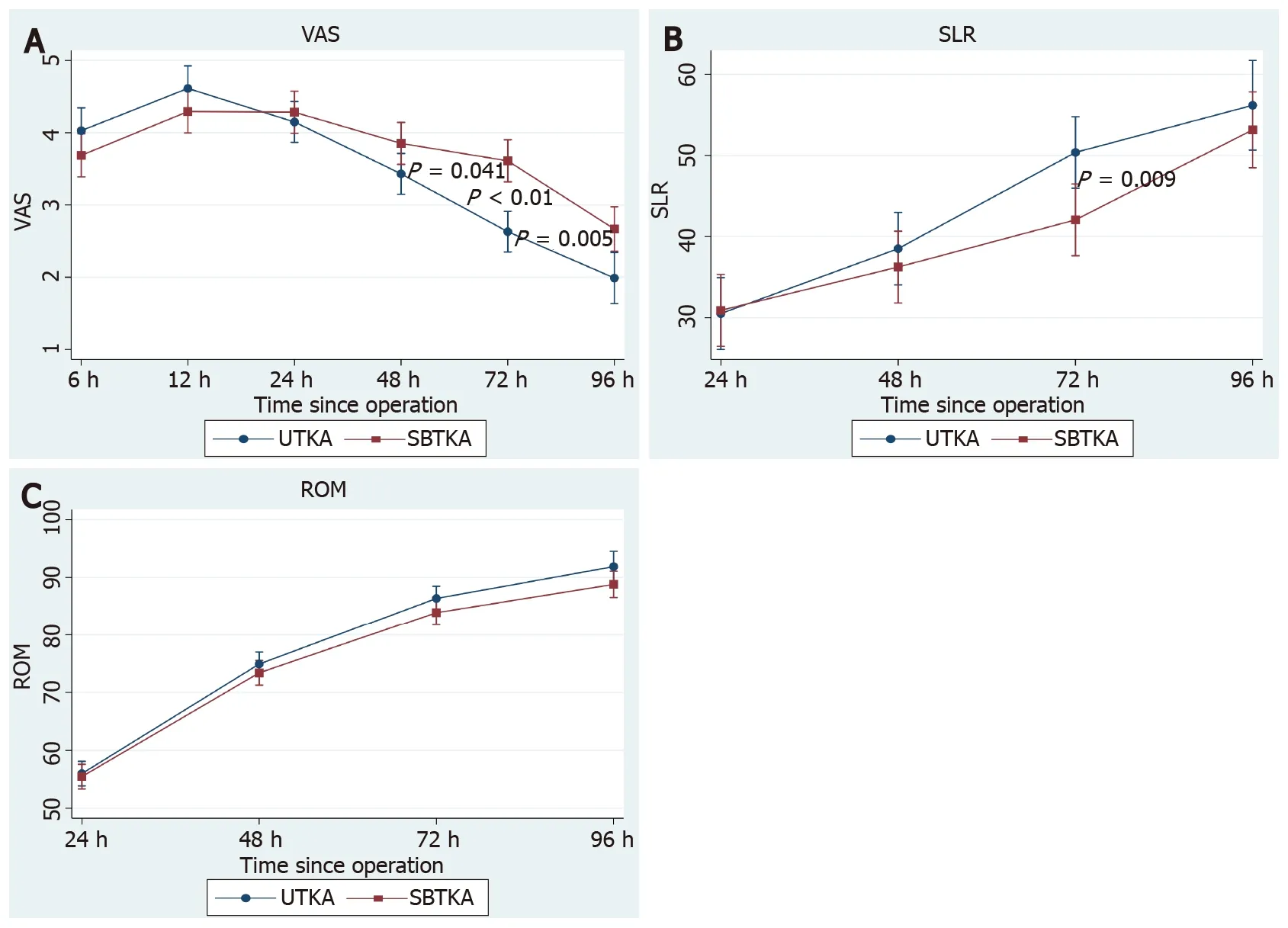
There was no difference between the UTKA and BTKA groups regarding VAS scores at 6, 12, and 24 h, but the BTKA group had significantly higher VAS scores than the UTKA group at 48, 72, and 96 h after surgery (Figure 2A).The BTKA group had a significantly lower degree of SLR than the UTKA group at 72 h; however, the ROM was comparable between groups throughout the study period (Figure 2B and C).Total morphine consumption in the UTKABTKA group was 11.93 ± 9.2013.81 ± 10.81 (= 0.16) at 24 h, and 16.78 ± 13.2419.51 ± 15.47 (= 0.15) at 48 h postoperatively.The incidence of postoperative nausea and vomiting (PONV) during the first 24 h in the UTKA and BTKA groups was 38.79% (90/142) and 46.47% (112/129) (= 0.09), respectively.The UTKA had an LOS of 4.01 ± 0.97 d, which was significantly shorter than that of the BTKA group (5.17 ± 1.32 d;< 0.01).
Cardiac biomarkers
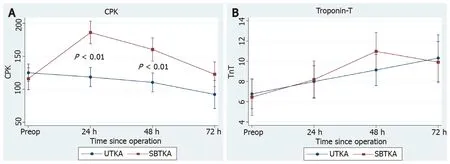
The BTKA group showed significantly higher CPK than the UTKA group at 24 h and 48 h after the surgery (Figure 3A).For the hs-TnT, it was gradually rising during 72 h after the UTKA and it was rising to a peak at 48 h after the BTKA, but the hs-TnT level was not significantly different between groups along the study period (Figure 3B).Nonetheless, there were 12 patients (5.71%) who had hs-TnT > 14 ng/L during the first 72 h after the UTKA compared to 17 patients (12.41%) following the BTKA (= 0.04), but no patient presented cardiovascular symptoms and signs, or abnormal electrocardiogram indicating MI.
Complications and readmission at 90 d
During the 90 d after the index surgery, there was one superficial infection, one cerebrovascular event, and two deep vein thromboses (DVT) in the UTKA group.For the BTKA group, one patient experienced peptic ulcer bleeding, one had DVT in the unilateral leg, and one had periprosthetic joint infection (PJI) which was successfully treated by two-stage revision TKA.Additionally, each group had one patient who required readmission due to severe pain at the surgical site.
DISCUSSION
Bilateral one-stage TKA potentially increases the rate of complications which are related to more soft tissue trauma, blood loss, postoperative pain, and cardiovascular adverse events, and therefore this is still a concerning issue for some patients and surgeons[8,9].However, recent studies reported that BTKA in selected patients is as safe as the staged procedure, but proper patient screening, and perioperative care and monitoring to avoid complications and mortality are still controversial[23,24].In the current study, BTKA was associated with significantly greater blood loss and higher allogeneic blood transfusion rates, as well as higher CPK levels, when compared to the UTKA group.The BTKA group tended to have higher hs-TnT levels at 48 h despite not reaching statistical significance.After 48 h, the BTKA group had a significantly higher VAS score than the UTKA group, and the SLR at 72 h after the BTKA was also worse than that after the UTKA.The LOS of the BTKA group was also significantly longer than that for the UTKA group.Nevertheless, the total morphine use, ROM, complications, and 90-d readmission rate were not different between the groups.
PBL (mL) = TBV (mL) × (Hb– Hb)/Hb+ sum of blood products transfused (mL), where Hb(g/dL) is the preoperative Hb, and Hb(g/dL) is the postoperative Hb.
Generally, BTKA is known for its association with inevitably greater blood loss than UTKA.Advances in surgical techniques, use of TXA, and change in transfusion thresholds have substantially reduced postoperative transfusions following UTKA[3].Recently, TXA is widely respected as an effective anti-fibrinolytic agent and has been demonstrated as having advantages when used in BTKA[25].Although TXA is effective for reducing blood loss following BTKA, when it is applied either intravenously (IV) or intra-articularly (IA), the ideal regimen of TXA is still not well defined[13].Arora[26] revealed no difference in average drop of Hb and blood transfusion rate between patients undergoing BTKA with IV-TXA or IA-TXA.Also, combined IA and IV TXA administration in BTKA did not show superior efficacy in blood loss reduction[27].Therefore, the intraoperative IA-TXA use alone, in our study, should be sufficient to control blood loss, while avoiding potential complications related to systemic administration of TXA.However, our transfusion rate in BTKA is still quite high at 40.88%.Chalmers[28] retrospectively reviewed 475 patients who underwent BTKA and received double doses of TXA and contemporary blood management.They found that BTKA is still associated with a blood transfusion rate of approximately 1 in 5, and 50% of patients with a preoperative Hb < 12.5 required blood transfusion.Accordingly, we identified the preoperative Hb as a predictive factor for allogeneic transfusion in BTKA.Particularly, approximately 1 out of 3 patients in our study had preoperative anemia, and this finding may underline the opportunity for further improvement and for addressing this modifiable risk factor before BTKA.Delasotta[29] demonstrated that giving three preoperative doses of epoetin-α could significantly increase Hb levels and reduce blood transfusions in BTKA.Intravenous iron supplementation has also been reported for its efficacy in reducing the rate of transfusion in BTKA when combined with IA-TXA administration[30].Other determinants including female gender, preoperative Hb level, operative time, and drain use have also been identified as risk factors for blood transfusion in BTKA[11,28].In addition, soft tissue surface and intramedullary canal violation have been revealed as a possible significant source of bleeding[11,31-33].Nevertheless, the efficacy of fibrin sealant applied to the bleeding soft tissue is unclear for blood loss reduction in BTKA[31], and also outcomes of emerging technologies such as computer-assisted or accelerometer-based navigation are still equivocal[13,34].
Significant pain after UTKA has been noted and this has been an issue frequently concerning patients as to whether the intensity of pain and disablement, during convalescence from BTKA, is worse than that of UTKA.Shetty[20] reported that BTKA had significantly higher VAS pain scores than UTKA on the first postoperative day.However, the VAS, ROM, and SLR were equal in both groups at the time of discharge.Other researchers found a 1-point higher VAS in the BTKA group during day 1, with 20% more narcotic use for the first 48 h, and patients in the BTKA group lagged behind the UTKA group in ambulatory milestones by approximately 36 h[21].In the present study, we found that the UTKA and BTKA group had comparable pain intensity, morphine consumption, and knee function during the first 24 h after the surgery by using the same multimodal pain management.The neuroaxial anesthesia, LIA that was induced by injecting with bupivacaine and ketorolac tromethamine, and opioid-sparing analgesia with a multidrug regimen may be an explanation of the effective pain control during the first 24 h after UTKA and BTKA.Despite that, patients in the BTKA gradually developed higher pain scores afterwards and had worse SLR at 72 h.Higher postoperative CPK levels might reflect the certainty of more muscle injury in the BTKA, and so may indicate the need for intensive pain control extended beyond 48 h after the surgery.Intravenous administration of non-steroidal anti-inflammatory drugs (NSAIDs) is commonly used because of their efficacy in controlling post-TKA pain and may be administered up to 72 h after the surgery.Recently, Parecoxib, which is a selective cyclooxygenase-2 (COX-2) inhibitor, has been demonstrated to be effective in the reduction of post-TKA pain with the additional advantage of having less platelet inhibition and is consequently associated with less blood loss when compared to conventional NSAIDs[2].Furthermore, intravenous corticosteroid and acetaminophen were also revealed as useful adjuncts for mitigating pain after TKA[35,36].
The safety of BTKA is still debated.Chen[24] recently demonstrated that patients aged > 80 years with an ASA score ≥ 3 who received careful screening for cardiopulmonary disorder and contemporary perioperative management for BTKA, had significantly decreased incidences of major and minor complications.Gromov[37] reported a 0% incidence of mortality in 284 selected patients without cardiopulmonary compromise, and they also found that ASA score ≥ 3 was a risk factor for 90-d readmission and prolonged LOS whereas higher BMI was a weak predictive factor for readmission.Lindberg-Larsen[23] conducted a study to compare outcomes after simultaneous and staged bilateral TKA in propensity-scores matched patients from nine centers.Of 232 matched patients in each group, perioperative complications and re-operation rates were significantly higher after simultaneous bilateral TKA.However, there was no difference in the rate of readmission within 30 d as well as the mortality between groups.In the present study, the hs-TnT level, which is a biomarker for cardiac muscle injury, was not different between UTKA and BTKA when patients had an ASA score ≤ 3 and preoperative hs-TnT within normal values.Although there were 12 and 17 patients after the UTKA and BTKA who had hs-TnT > 14 ng/L, no patients in either group presented symptoms and signs of cardiovascular complications.Hence, serial testing of cardiac biomarkers may be indicated only when patients have suspected clinical presentation[38].Additionally, Hb evaluation seems to be unnecessary for non-anemic patients who undergo UTKA, due to the very low risk for blood transfusion.However, we suspect that Hb testing at 48 h after BTKA may be appropriate as a reflection of ongoing blood loss that is possibly linked to cardiac stress because the hs-TnT was rising to a peak at 48 h after BTKA when the Hb level was dropping.For other complications, the risk of PJI and DVT was not different between BTKA and UTKA when similar prophylaxis ATB and anticoagulants were applied.Nevertheless, further investigation may be needed to develop well-defined guidelines for perioperative monitoring in patients undergoing BTKA to decrease potential morbidity and mortality.
Nonetheless, we realized some limitations of the present study.First, this investigation is retrospective with some limitations accorded by study design, even if the selection of BTKA or UTKA as patient preference might be better accommodated with our real-life practice.Second, both study groups comprised predominantly female patients.However, previous studies found that gender has no effect on blood loss and functional recovery following TKA[12,39].Third, variation of thresholds or cut-off values for blood transfusion among individual institutions may result in a different transfused rate.Indeed, the incidence of patients with preoperative anemia in our study seems to be higher than previously reported[3] and thereby may be a reason for higher transfusion rates than those reported in other studies[4,28].Lastly, our sample size might not be sufficient to assess the exact risk of cardiovascular events and thromboembolism after UTKA and BTKA.
For postoperative management, intravenous patient-controlled analgesia morphine (100 mL solution containing 50 mg of morphine sulphate) was injected as an ondemand bolus of 1 mL with a 5 min lockout period, 30 mg of ketorolac was given intravenously every 8 h, and 500 mg of oral acetaminophen was administered three times a day.After 48 h, all the catheters were discarded, and 2 mg of morphine were injected every 8 h with an additional 2 mg of morphine used for a breakthrough pain throughout hospitalization.Also, oral medications including 250 mg of naproxen twice a day and 500 mg of acetaminophen three times a day were given.All patients were administered with low molecular weight heparin for the first 48 h and combined with oral warfarin for 10 d.Rehabilitation including active ankle pump was started after the surgery, and a continuous passive motion device was utilized on the day after surgery.Every patient was encouraged to attempt early ambulation with gait aids as able to be tolerated.
CONCLUSION
Following similar perioperative management, the blood transfusion rate in BTKA is 4-fold that required in UTKA.Also, BTKA is associated with higher pain intensity at 48 h postoperatively and prolonged LOS when compared to UTKA.Hence, patients undergoing BTKA may require more extensive perioperative management for blood loss and pain, even if they have no higher risk of complications and 90-d readmission than those receiving UTKA.
ARTICLE HIGHLIGHTS
Research background
Furthermore, significant pain after UTKA has been noted and inadequate pain control has been demonstrated to be associated with inferior functional outcomes at 2 years after TKA[19].Thus, postoperative pain has been an issue frequently concerning patients as to whether the intensity of pain and disablement during convalescence from BTKA are worse than that following UTKA.Nevertheless, there has been limited evidence comparing postoperative pain and functional recovery after BTKA and UTKA, and the known results are still equivocal[20,21].Therefore, the objective of the present study was to compare the perioperative outcomes including perioperative blood loss (PBL), cardiac biomarkers, pain intensity and functional recovery, and complications between patients undergoing UTKA and BTKA with a similar perioperative protocol.The authors hypothesized that patients undergoing BTKA may require additional perioperative care and monitoring to improve outcomes.
She taught it to kneel before her, and then she whispered in its ear: Kneel, little calf, kneel; Be faithful and leal, Not like Prince Fickle, Who once on a time Left his fair Helena Under the lime
Research motivation
Despite previously acknowledged benefits, there is an issue frequently concerning patients as to whether the intensity of pain and disablement during convalescence from BTKA is worse than that following unilateral total knee arthroplasty (UTKA).Also, the risk of cardiovascular morbidity and other complications are subjects that lead some surgeons to refrain from BTKA.Thus, our objective was to identify what perioperative aspects of BTKA need to be improved and handled differently than for UTKA.
Research objectives
To compare the perioperative outcomes including perioperative blood loss (PBL),cardiac biomarkers, pain intensity, functional recovery, and complications between UTKA and BTKA by using an identical perioperative protocol.
Research methods
All patients who had undergone UTKA and BTKA for primary osteoarthritis that had been performed by a single surgeon with identical perioperative protocols between January 2016 and December 2019 were retrospectively reviewed.The exclusion criteria of this study included patients with an American Society of Anesthesiologists score >3, known cardiopulmonary comorbidity or high-sensitivity Troponin-T (hs-TnT) > 14 ng/L, CKD stage ≥ 3 or significant renal impairment (serum creatinine > 1.5 mg/dL),prior knee surgery, and previous knee infection.
Research results
Patients who received BTKA had significantly higher PBL with a 4-fold greater transfusion rate.As well, the patients in the BTKA group had higher visual analogue scale scores at 48, 72, and 96 h after the surgery and a higher postoperative creatine phosphokinase level.Consequently, a longer length of hospital stays than those who had UTKA was required.However, there was no difference regarding the postoperative hs-TnT level and complications.
The king again summoned the brothers before him, and asked whether it was true that they had said that they could get for him a boar whose bristles were of gold and silver time about
Research conclusions
Patients who undergo BTKA may require more extensive perioperative care for blood loss and pain than those patients who undergo UTKA.
Research perspectives
Future prospective studies may be required to develop a particular perioperative protocol in patients undergoing BTKA to decrease potential morbidity and mortality.
ACKNOWLEDGEMENTS
We thank Mr.Roy I Morien of the Naresuan University Graduate School for his assistance in editing the English expression and grammar in this document.We also thank Passakorn Teekaweerakit, MD, Watcharapong Eiamjumras, MD, Thanawat Tantimethanon, MD, Panapol Varakornpipat, MD, and Kongpob Reosanguanwong, MD, for their technical assistance.
 World Journal of Orthopedics2022年1期
World Journal of Orthopedics2022年1期
- World Journal of Orthopedics的其它文章
- Long-term outcomes of the four-corner fusion of the wrist: A systematic review
- Comparing shoulder maneuvers to magnetic resonance imaging and arthroscopic findings in patients with supraspinatus tears
- High-resolution, three-dimensional magnetic resonance imaging axial load dynamic study improves diagnostics of the lumbar spine in clinical practice
- Can bedside needle arthroscopy of the ankle be an accurate option for intra-articular delivery of injectable agents?
- Epidemiology and incidence of paediatric orthopaedic trauma workload during the COVID-19 pandemic: A multicenter cohort study of 3171 patients
- Management of proximal biceps tendon pathology