Current trends and perspectives in interventional radiology for gastrointestinal cancers
2021-11-01 07:21:30ElisaReitanoNicoladeAngelisGiorgioBianchiLetiziaLaeraStavrosSpiliopoulosRobertoCalbiRiccardoMemeoRiccardoInchingolo
World Journal of Radiology 2021年10期
Elisa Reitano, Nicola de'Angelis, Giorgio Bianchi, Letizia Laera, Stavros Spiliopoulos, Roberto Calbi, Riccardo Memeo, Riccardo Inchingolo
Elisa Reitano, Division of General Surgery, Department of Translational Medicine, University of Eastern Piedmont, Novara 28100, Italy
Nicola de'Angelis, Giorgio Bianchi, Unit of Minimally Invasive and Robotic Digestive Surgery,"F. Miulli" General Regional Hospital, Acquaviva delle Fonti 70021, Italy
Letizia Laera, Department of Oncology, "F. Miulli" General Regional Hospital, Acquaviva delle Fonti 70021, Italy
Stavros Spiliopoulos, 2nd Department of Radiology, School of Medicine, National and Kapodistrian University of Athens, Athens 12461, Greece
Roberto Calbi, Department of Radiology, "F. Miulli" General Regional Hospital, Acquaviva delle Fonti 70124, Italy
Riccardo Memeo, Unit of Hepato-Pancreatic-Biliary Surgery, "F. Miulli" General Regional Hospital, Acquaviva delle Fonti 70021, Italy
Riccardo Inchingolo, Interventional Radiology Unit, "F. Miulli" General Regional Hospital,Acquaviva delle Fonti 70021, Italy
Abstract Gastrointestinal (GI) cancers often require a multidisciplinary approach involving surgeons, endoscopists, oncologists, and interventional radiologists to diagnose and treat primitive cancers, metastases, and related complications. In this context,interventional radiology (IR) represents a useful minimally-invasive tool allowing to reach lesions that are not easily approachable with other techniques. In the last years, through the development of new devices, IR has become increasingly relevant in the context of a more comprehensive management of the oncologic patient. Arterial embolization, ablative techniques, and gene therapy represent useful and innovative IR tools in GI cancer treatment. Moreover, IR can be useful for the management of GI cancer-related complications, such as bleeding,abscesses, GI obstructions, and neurological pain. The aim of this study is to show the principal IR techniques for the diagnosis and treatment of GI cancers and related complications, as well as to describe the future perspectives of IR in this oncologic field.
Key Words: Interventional radiology; Radiology; Colorectal cancer; Gastric cancer;Malignancy; Embolization
INTRODUCTION
Gastrointestinal (GI) cancers are currently among the five most common cancers worldwide for both men and women[1]. According to the GLOBOCAN 2018, colon cancer and gastric cancer represents respectively the 3and 5most common cancers[2,3]. Some GI, such as the pancreatic cancer (PC), are rarer but burdened by a high mortality rate[4]. PC represents the thirteen most common cancer and the seventh most common cause of cancer-related death[4]. The incidence of GI cancer shows significant geographical variations, with colorectal cancer incidence higher in Western Countries and North America[3,5], whereas gastric cancer incidence is higher in Asia and Africa[2]. These geographical differences are mainly linked to environmental and lifestyle factors such as nutritional habits, alcohol intake, genetics, and obesity[2,5].
Nowadays, the “gold standard” management of cancers involves a multi-specialist staff consisting of oncologists, surgeons, endoscopists, and radiologists to provide a multi-disciplinary diagnostic and treatment approach to the oncologic patient.
Interventional radiology (IR) is getting a key role in oncologic patients' cares, being an essential tool in both the initial diagnosis and the subsequent treatment, as well as in the management of the related complications[6]. IR provides adequate diagnostic samples through a minimally invasive access, which can be obtained under imagine guidance by percutaneous and needle aspiration[7]. Therapeutic applications of IR in oncology are mainly focused on local cancer treatment, including radiofrequency (RF)ablation or trans-arterial chemoembolization (TACE)[8]. Cancers complications, such as pain, bleeding, organ obstructions, or venous thrombosis can also be managed by IR, with the eventual placement of gastrostomy or jejunostomy in selected patients[9,10].
This article aims to analyse the current roles of IR in GI cancer management and provide an extensive overview of the current literature on the topic. In this article, only cancers located in the GI tract (from the esophagus to the colon) will be considered.Liver, pancreas, and biliary tract will not be taken into account, as they should require a separate discussion.
IR IN THE DIAGNOSIS OF GI CANCERS
The adequate treatment of GI cancers depends on a timely definitive diagnosis and the staging of the disease[11]. Imaging techniques improved the assessment and staging of cancers, but the histological analysis represents the gold standard for the definitive diagnosis of this disease. Biopsies samples are required to assess the biomarker status of different solid GI cancers and should be performed not only for the initial diagnosis but at multiple end-points, to detect the cancer progression, predict the prognosis and guide the next-line therapy[12]. The improvement of the histological and cytological analysis, especially in the field of immunochemical examination, enables the identification of the primary tumor site and predicts the sensitivity to chemotherapeutic drugs[13].
Minimally invasive techniques have a prominent role in this contest. Endoscopy currently represents the first-level procedure for the histological diagnosis of GI cancers. However, lesions located within the submucosa or subserosa (such as lymphoma or gastrointestinal stromal tumours), may be difficult to diagnose with this approach[14]. Cancers located in the small bowel or colon could be not always reachable by the endoscope, due to their location or to stenosis of the lumen[14]. In this case, biopsies can obtain by interventional radiologists through direct visualization under image guidance of the masses, allowing the safe passage of the needle and minimising the trauma to the surrounding areas. In biopsy planning, imaging techniques help to define lesion location, accessibility, and suitability for biopsy also providing the identification of the mass to sample, in the context of multiple lesions[6]. In case of metastasis on the liver, not accessible by endoscopy, IR-biopsy can help to identify the primary tumour and define a tissue diagnosis[6].
The choice of imaging guidance modality is multifactorial and there are different options. Ultrasonography (US) is a fast and cost-effective technique, that guarantees real-time imaging, allowing the monitoring of the needle trajectory to the target lesion,without radiation exposure. US-guided percutaneous biopsy provides the diagnosis of solid abdominal organ lesions located in the spleen, pancreas, or lymph nodes, with high diagnostic accuracy and low complications and mortality rates[15]. Moreover, US is useful in guiding biopsies with intracavitary access and must be considered as a diagnostic alternative tool for the diagnosis of low rectal lesions and stromal tumours[16]. The success of US depends on different factors, such as the operator experience[16]. However, different studies suggested US superiority to computed tomography(CT)-guided biopsies, in case of lesions visible with ultrasounds[15,16]. CT-guided biopsy provides a more defined anatomical image, allowing a more precise needle localization when compared to US, showing to be particularly useful in case of pelvic or deep biopsies, which can be difficult to be performed using US. However, CTguided biopsies have a low real-time guidance capability to track the needle and the target location, requiring intermittent sweeps of the region of interest to confirm the location of the needle during the procedure, thus increasing the biopsy time. The principal disadvantage of the procedure is clearly linked to the radiations exposure expecially for the patients, with radiation dose-related to different factors such as the total scan time, the peak tube kilovoltage (kVP), and milliamperage (mA), the part of the body that must be scanned and the size of the patient[17]. CT-fluoroscopy is an alternative method resulting from technical advantages of the common CT, which allows near real-time imaging of the needled trajectory, reducing the procedural time.Fluoroscopic images are acquired at a lower mA, reducing the radiation dose to the patient, but increasing the radiation dose to the staff, due to the proximity of the physician to the x-ray source during the procedure[18]. However, recent available fusion image guidance systems allow decreasing the radiation exposure through realtime projection during the US-guided biopsies of a needle on to pre-existing CT or magnetic resonance imaging (MRI) image, improving at the same time the accuracy of the procedure[19]. Cone-beam computed tomography (CBCT) guided biopsy,represents the last frontier in the field of IR. Although its extensive use in pleural and pulmonary masses, its virtual navigation system allowed to increase the diagnostic accuracy of the target lesion through a 3D visualization and real-time guidance of the needle trajectory[20], with initial applications also for the diagnosis of GI lesions[21].
IR IN GI CANCERS TREATMENT
Arterial embolization
Arterial embolization (AE) is a useful therapeutic option for hypervascular cancer treatment. Therefore, AE is widely used in liver metastasis treatment, instead of primary GI cancers[22].
Imagine-guided cancer treatment represents a minimally invasive alternative or adjunct to surgery in the management of GI tumours[23,24]. AE consists of the identification of the arterial supply of a solid tumour in CT or MRI and the devascularization of the pathological tissue through transcatheter embolization[24]. Vessels occlusion can be achieved using polyvinyl alcohol, blood clots, coils, and liquid embolic introduced into the tumour bed through fluoroscopic arterial catheterization in IR[25,26]. The interruption of the cancer supplies induced hypoxia and inhibits the tumour growth. Therefore AE can be used in conjunction with ablative treatments or as an alternative to surgery[26]. Indeed, in the case of hypervascular cancers, this technique helps to reduce operative blood loss[27]. AE has a prominent role in the treatment of hepatic metastasis, especially from colon or rectal cancer[28-30]. In this context, a modification of this technique, the TACE, allowed the infusion of a single or combination of chemotherapy agents in the hepatic pathological tissue through the selective hepatic artery embolization[31-33]. This technique reduces the systematic dose of chemotherapy agents, allowing them to reach a higher local concentration.TACE should be repeated for more sessions until the complete devascularization of the pathological tissue[32]. Finally, separate mention should be given to the radioembolization, despite its use is limited to hepatic pathological tissue. It consists of betaradiation emitting radio-isotopes directly into the mass employing microspheres (glass or resin) resulting in selective tissue necrosis[32].
Ablative techniques
Local cancers ablation is an alternative technique for early stages or not candidate for surgical resection[34]. Tumour ablation mediated by IR allowed pathological tissue necrosis in different modalities, including RF, microwave, and cryotherapy[34]. RF ablation (RFA) is mainly applied in liver metastasis of gastric and colon cancers[35,36]. RFA consists of the administration of electrical energy to a tissue, through an electrode connected in a closed-loop circuit to a monopolar or bipolar energy source[8]. The tissue reached a temperature higher than 60 degrees Celsius with consequent thermal damage. RFA is a safe technique with a lower mortality rate (0.3%) and complication rate (2.2%)[8], with an efficacy, described also in the context of skeletal,renal, and lung metastasis with curative or palliative purpose[37-39]. Conversely to RFA, cryotherapy induces cell necrosis by applying subfreezing temperatures, using nitrogen or argon gas under high pressure[40]. The process of freezing-thawing must be repeated to obtain an effective ablation due to the mechanical stress-induced to the cell membranes[41]. CT identifies the ablated zone in real-time as a low-density area[41]. Acting by a mechanism of osmosis and necrosis, different studies suggested that the intracellular content that remains intact allows inducing an immune-specific reaction with an onco-suppressive effect outside the ablated tissue. However, these considerations are based on preclinical studies[42,43], and prospective clinical trials are needed to confirm these data. Microwave ablation is based on the application of electromagnetic energy within a range of at least 915 MHz, agitating the water molecules in target tissue and inducing cell death through coagulation necrosis[44].Despite microwave showed equivalent or higher clinical efficacy if compared to RFA,however, RFA showed lower recurrence rates and a higher survival rate achieving extensive necrosis after few sessions, with less post-procedural pain[45,46]. In any case, the decision of which ablation methods should be used, must take into consideration several factors such as the tumour type and location (especially the proximity to vulnerable areas) and patients’ comorbidities.
Gene therapy
Advanced in immunology and molecular oncology led to the development of gene therapy. It consists of the administration of genetic agents into a tissue in order to stimulate the immune response, reduce the oncogenic expression, modulate the angiogenesis or modify the response to chemotherapeutics[47]. The selective arterial injections of genetic agents are followed by the vessel embolization, to assure the administration of the substance directly into the mass, limiting the adverse effects and increasing the local dwell time[47]. Genetics agents are typically transferred into the cell through vector agents which allow them to cross cell membranes[48]. Vectors are usually plasmids, phospholipidic agents, or viruses like adenovirus, Epstein-Barr virus, and retroviruses (which provided a lasting genetic expression)[48]. However,clinical studies on gene therapies are very limited and, although the results look promising (especially in the treatment of liver metastases), further studies are needed to confirm the data[48,49].
IR in the treatment of GI cancers complications
IR has also a role in the minimally invasive treatments of different GI cancers complications, avoiding reoperations and allowing a speeding recovery time[50]. Therefore, IR plays a key role in the field of oncology, contributing to revolutionize the postoperative management of these patients. Indeed, IR allows management of possible complications, which would otherwise require a new surgery, in a minimally invasive way.
IR also provides a palliative treatment in advanced GI cancers stages, through diminishing pain or allowing symptoms reduction[9,51].
Bleeding
Besides the role of AE and its modification in the treatment of hepatic pathological tissues, its use in GI cancers is limited to acute bleeding treatments[23,52]. Bleeding from advanced gastric cancers accounts for 1% to 8% of the upper gastrointestinal bleedings (UGIB), causing delays in chemotherapy and increasing transfusion requirements[53,54]. Moreover, endoscopy represents the gold standard for UGIB,being able to recognize the exact source of bleeding[55]. However, in presence of profuse bleeding masking the exact source, endoscopy may fail to stop it[56,57]. Due to advances in angiography systems and haemostatic materials, IR embolization is recognized as an alternative modality in patients in whom endoscopy fails or is not indicated[58,59] IR embolization is also used in the treatment of lower gastrointestinal bleedings (LGIB), defined as bleeding originating distal to the ligament of Treitz[60].The introduction of super-selective embolization with coaxial microcatheter systems and embolic agents (such as pledgets of absorbable gelatine sponge, polyvinyl alcohol,or other spherical particulates, micro-coils, and liquid embolic agents) represents a useful tool in LGBI[60,61]. According to the American College Guidelines[62] in the treatment of LGIB, it should be considered in high-risk patients with ongoing bleeding who do not respond adequately to the volume resuscitation and who are unlikely to tolerate bowel preparation and colonoscopy (Figure 1). Although its major complication is ischemia, it should be preferred as a first-line approached in these selected patients[63]. A new frontier for the treatment of LGIB is CBCT embolization,which allowed a fast identification of the bleeding site and simplifying the placement of the microcrater in the vessel, without requiring sequential angiography[64]. The indications and possible complications of these techniques are the same as the traditional AE, with the theoretical advantage of greater safety and efficacy due to the modern and accurate tools[64].
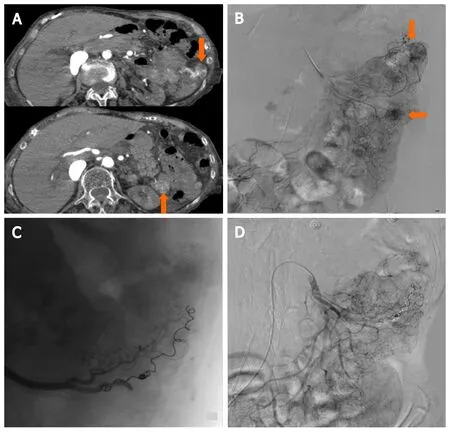
Figure 1 87-year-old female with distal duodenum/proximal jejunum Ca presents with severe recurrent melenas. Endoscopic hemostasis failed in high risk surgical patients with hemodynamic instability and normal coagulation state, requiring embolization after transfusion and hemodynamic stabilization(stabilized blood pressure 90 mmHg with inotropes, HR: 110/min. Hb 6.4). A: Computed tomography-Angio: Two active bleeding sites at proximal jejunum (arrows);B: Selective digital subtraction angiography (DSA) from superior mesenteric artery depicting the bleeding sites (arrows); C: Selective catheterization of the feeding artery with microcatheter and two 3 mm micro coils deployed; D: Lesions are not depicted at final DSA.
AE represents a useful tool also for postoperative bleeding, allowing to stop the bleeding avoiding surgical reoperation, with minimally invasive access[65]. Another possible complication of surgery is the arteriovenous or arterio-enteric fistulas, lifethreatening conditions[66]. Although conventional angiography is rarely used as the first-line imaging modality for its diagnosis, angioembolization allowed minimally invasive management of the fistula and to avoid major surgery[67].
Finally, in the event of an arterial bleeding from pseudoanurysm, endovascular treatment with covered self-expanding stent-grafts placement was reported as an effective method. It is performed under local anesthesia, which avoids the need for general or locoregional anesthesia in unstable, high-risk patients[65,66].
Abscess drainage
An intrabdominal abscess could be the first cancer presentation[68] as well as a postoperative complication[50,69]. In both cases, IR is a reliable minimally invasive alternative to surgery, although the feasibility of this technique depends on the abscess location and the consistency of the contents of collections[70]. In case of deep-seated abscess or abscess located close to vulnerable structures, CT-guided percutaneous drainage is the gold standard (Figure 2). Despite the limit of a non-real-time image, it allowed the best image-depiction of the collection and the adjacent organs[7]. In the case of easily accessible abscesses, US-guided drainage must be preferred and should always be the first procedure in patients with simple abscesses[71]. US and CT can be combined with fluoroscopy to avoid guidewire kinking during the procedure and to monitor the placement of catheters[70]. The abscess can only be aspirated, or a catheter can be left in place for few days, especially when contamination or communication with the bowel or urinary tract is suspected[70]. Deep-seated abscess with interposition of organs can be drained with a surgical approach or the intervening organ can be traversed with a catheter[72]. This approach is not suitable for almost all abdominal organs, except the stomach and the liver[72,73]. Finally, transvaginal and transrectal drainage with US or CT guidance allows access to deep-seated abscesses beside the vagina or rectum, often resulting from gynecological or rectal cancers, and inaccessible with percutaneous methods[74,75]. Percutaneous abscess drain placement for abdominal and pelvic collections could be achieved also with cone-beam CT, with equivalent successful rate and radiation dose of conventional CT positioning and the advantage of reduced procedural time[76].
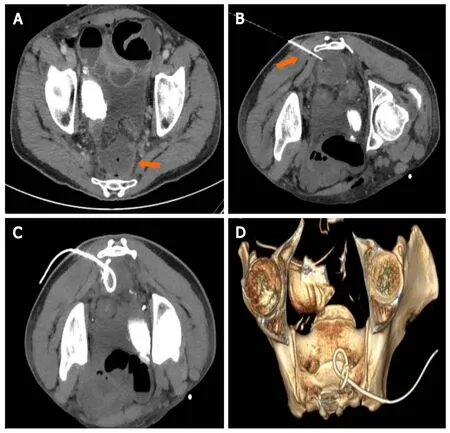
Figure 2 Presacral collection following rectal surgery. A: Axial computed tomography (CT) scan demonstrating a 4 cm × 3 cm presacral fluid collection(arrow), with small air bubbles; B: Patient in prone position, a Chiba needle is inserted with a trans-gluteal approach under CT guidance; C and D: Mip CT images and 3D Volume rendering reconstruction confirming the exact 8Fr drainage positioning.
GI obstructions
Oesophageal or gastric cancers determining luminal obstruction, dysphagia, or swallowing impairment, are frequently cause of intolerance of the oral intake,requiring nutritional support through a gastrostomy or gastrojejunostomy[77]. The first percutaneous radiologic gastrostomy (PRG) was performed in 1981 using fluoroscopic guidance to avoid bowel and solid organs, without the need for upper endoscopy[10].
IR showed higher technical success and safety rates, with the advantage to be performed in patients not eligible for endoscopy or surgical procedures[10]. PRG complications are similar to the percutaneous endoscopic gastrostomy (PEG),including infections (23%) and the discomfort on feeding (33%)[78,79] and less frequent complications such as haemorrhage, ileus, aspiration of feed, and tube occlusion[10].
The tube dislocation is relatively common, with the possibility of easy tube reinsertion in the same tract if this is established for more than 2 wk. Alternatively,early tube dislodgment requiring repeated gastric puncture[79]. Gastrostomy and gastrojejunostomy can be performed also in small bowel obstruction with a decompression purpose with a success rate higher than 98%[80] (Figure 3). In patients with ascites, a paracentesis must be performed to reduce the peritoneal liquid, to reduce the possibility of complications such as peritonitis or peri-catheter leakage[80,81]. Contraindications for PRG are the same as PEG, including coagulopathy as an absolute contraindication and immunosuppression as a relative one[10]. In the last years, different studies, suggested the positioning of gastroduodenal and colonic selfexpanded stent under fluoroscopic-guide as a palliative treatment, in oncologic patients with no indication for surgery[82,83]. Self-expanded stent are extensively used in the palliative treatment of duodenal and rectal occlusions, as given the smallest diameter of these segments, a malignant obstruction can easily occur at these levels[82].
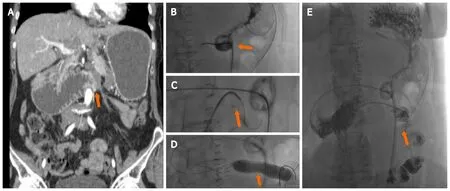
Figure 3 Upper gastrointestinal cancers obstruction. A: A 60 yr female with stage 4 ovarian cancer, with peritoneal carcinomatosis causing occlusion at the Treitz level (arrow); B and C: After percutaneous insertion of a decompressive gastrostomy, an angiografic catheter was advanced at the level of the occlusion and crossed using an hydrophilic guidewire (arrow); D and E: A ballon dilatation (18 mm × 6 cm) was performed (D, arrow) and a 5 fr catheter was left in place to ensure enteral nutrition (E, arrow).
The positioning of the stent under fluoroscopy-guidance allowed to approach the obstruction and the safe placement of the stent, without the need of bowel preparation in case of colonic stents[82]. The use of angiographic catheters with variable head shapes and easily shapable guide-wires can facilitate passing the angulated obstruction, which is the most common cause of endoscopic failure[82,83].
Pain control
Pain represents a significant source of morbidity in oncologic patients, especially in advanced stages, with an incidence ranging from 40% to 90%. According to the World Health Organization, opiates remain the first choice drugs in these patients. However,those patients with non-controlled pain or with intolerable analgesic effects could also benefit from interventional pain control techniques[84,85]. Upper abdominal visceral cancers are often poorly responsive to analgesic therapy. In these cases, nerve block or celiac ganglion neurolysis can reduce pain, especially related to pancreatic, gastric, and oesophageal cancers[86] (Figure 4). The substances most often employed in IR include local alcohol or phenol, which induce permanent nerve destruction, and triamcinolone, which reversibly blocks nocireceptors[87]. CT represents the most commonly used image-modality to guide the celiac axis block, with either an anterior or posterior approach, according to the operator experience[87]. The most frequent complications of these techniques are diarrhea (73%) and orthostatic hypotension(12%)[87].
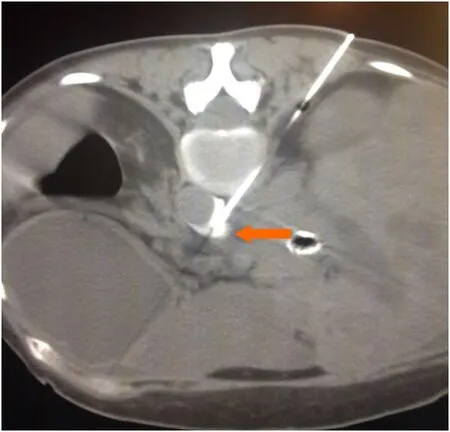
Figure 4 Celiac plexus alcohol neurolysis. In a patient with metastatic pancreatic cancer and non-controlled pain, an 18G Chiba needle (arrow) is inserted under computed tomography-guidance with a paravertebral approach; ethanol (95%-100%) is injected into the antecrural space after confirming the needle position with diluted iodinate contrast medium.
FUTURE PERSPECTIVES
IR showed an exponential growth in the last years and represents a useful tool in the treatment of oncologic patients. Its role in the context of GI cancers is increasingly relevant, allowing for the diagnosis and treatment of cancer and related complications,with a minimally-invasive approach. The introduction of ablation techniques and monitoring devices contributed to the effectiveness and safety of IR procedures,allowing for the treatment of lesions close to sensitive structures, often difficult to be accessed by other approaches. IR is a very useful tool also in the treatment of GI cancer complications,, bleeding from the digestive tract that cannot be reached by endoscopy[56].
Given the increasing relevance of IR in GI cancers management, the inclusion of interventional radiologists in the multidisciplinary oncologic staff is considered of paramount importance. Specific training programs, also including the use of simulators, are necessary to support the IR learning curve.
CONCLUSION
IR is a medical specialty which uses minimally-invasive technique in GI cancer management. Given its prominent role, the IR specialist should always be considered as an essential player in the multidisciplinary staff responsible for the treatment of the oncologic patient.
ACKNOWLEDGEMENTS
The entire manuscript has been written and amended by a native English speaker(Martin Mariappan MD).