
Highlighting COVID-19: What the imaging exams show about the disease
2021-07-02 08:36:34LorenaSousadeCarvalhoRonaldoTeixeiradaSilvaniorBrunaVieiraSilvaOliveiraYasminSilvadeMirandaNaraciaFonsecaRebouasMatheusSandeLoureiroSamuelLucaRochaPinheiroRegianeSantosdaSilvaPauloVictorSilvaLimaMedradoCorreiaMariaJ
World Journal of Radiology 2021年5期
Lorena Sousa de Carvalho, Ronaldo Teixeira da Silva Júnior, Bruna Vieira Silva Oliveira, Yasmin Silva de Miranda, Nara Lúcia Fonseca Rebou?as, Matheus Sande Loureiro, Samuel Luca Rocha Pinheiro, Regiane Santos da Silva, Paulo Victor Silva Lima Medrado Correia, Maria José Souza Silva, Sabrina Neves Ribeiro,Filipe Ant?nio Fran?a da Silva, Breno Bittencourt de Brito, Maria Luísa Cordeiro Santos, Rafael Augusto Oliveira Sodré Leal, Márcio Vasconcelos Oliveira, Fabrício Freire de Melo
Lorena Sousa de Carvalho, Ronaldo Teixeira da Silva Júnior, Bruna Vieira Silva Oliveira, Yasmin Silva de Miranda, Nara Lúcia Fonseca Rebou?as, Matheus Sande Loureiro, Samuel Luca Rocha Pinheiro, Regiane Santos da Silva, Paulo Victor Silva Lima Medrado Correia, Maria José Souza Silva, Sabrina Neves Ribeiro, Filipe Ant?nio Fran?a da Silva, Breno Bittencourt de Brito, Maria Luísa Cordeiro Santos, Rafael Augusto Oliveira Sodré Leal, Márcio Vasconcelos Oliveira, Fabrício Freire de Melo, Department of Instituto Multidisciplinar em Saúde, Universidade Federal da Bahia, Vitória da Conquista 45029-094, Bahia, Brazil
Abstract Coronavirus disease 2019 (COVID-19), a global emergency, is caused by severe acute respiratory syndrome coronavirus 2. The gold standard for its diagnosis is the reverse transcription polymerase chain reaction, but considering the high number of infected people, the low availability of this diagnostic tool in some contexts, and the limitations of the test, other tools that aid in the identification of the disease are necessary. In this scenario, imaging exams such as chest X-ray(CXR) and computed tomography (CT) have played important roles. CXR is useful for assessing disease progression because it allows the detection of extensive consolidations, besides being a fast and cheap method. On the other hand, CT is more sensitive for detecting lung changes in the early stages of the disease and is also useful for assessing disease progression. Of note, ground-glass opacities are the main COVID-19-related CT findings. Positron emission tomography combined with CT can be used to evaluate chronic and substantial damage to the lungs and other organs; however, it is an expensive test. Lung ultrasound (LUS) has been shown to be a promising technique in that context as well, being useful in the screening and monitoring of patients, disease classification, and management related to mechanical ventilation. Moreover, LUS is an inexpensive alternative available at the bedside. Finally, magnetic resonance imaging, although not usually requested, allows the detection of pulmonary,cardiovascular, and neurological abnormalities associated with COVID-19.Furthermore, it is important to consider the challenges faced in the radiology field in the adoption of control measures to prevent infection and in the follow-up of post-COVID-19 patients.
Key Words: SARS-CoV-2; COVID-19; Pneumonia; Pandemic; Radiology; Tomography
INTRODUCTION
In December 2019, several cases of a pneumonia of unknown cause with a clinical presentation compatible with conditions of viral etiology were reported in the city of Wuhan, Hubei province, China[1-4]. Later, it was found to be caused by a new type of coronavirus that was subsequently called severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), and the disease came to be called coronavirus disease 2019 (COVID-19)[5,6]. Since then, the number of cases has increased, becoming a major outbreak and a global emergency[7,8]. By 19 January 2021, more than 93956883 cases and 2029084 deaths have been confirmed by the World Health Organization[9].
The SARS-CoV-2 is a β-coronavirus with spherical RNA and spike proteins that protrude on its surface[10]. It primarily infects the respiratory system but other organs such as the kidneys, heart, ileum, and spleen can also be infected[11]. The pathophysiological mechanisms involved in this process are complex, and includes virus attachment, recognition between specific cell receptors, and transmembrane Spike glycoprotein (S-protein) receptor-binding domain, along with protease cleaving by host cellular transmembrane serine protease (TMPRSS)[12]. Angiotensin-converting enzyme type 2 (ACE2) receptors are expressed in various human cells, including epithelial cells in the lungs, cardiomyocytes, neuronal and glial cells in the brain[13],glandular cells of the gastric, duodenal, and rectal epithelia, and enterocytes of the small intestine[14,15]. The main pathway by which SARS-CoV-2 enters cells is through the binding of S-protein to ACE2[14,15], and protein cleavage by enzymes, such as TMPRSS2[16].
The SARS-CoV-2 infection has variable clinical presentations, from asymptomatic to severe cases, which can lead to death[1,5]. The main symptoms involve fever, dry cough, dyspnea, and fatigue[17-20]. The gold standard diagnostic test for COVID-19 is the reverse transcription polymerase chain reaction (RT-PCR)[21,22]. However, due to the low availability of this diagnostic tool in some contexts, failures in sample collections, and the possibility of false-negative results, it has become necessary to use other methods to increase the accuracy of infection identification[23].
In this context, some imaging exams such as lung ultrasound (LUS), chest X-Ray(CXR), magnetic resonance imaging (MRI), and especially chest computed tomography (CT) have been very useful in the diagnosis of COVID-19[24]. It is noteworthy that in places of low prevalence of the disease or in asymptomatic individuals, imaging tests may have problems with false positive or missed detection.Thus, factors such as epidemiological data, clinical condition, laboratory tests and imaging exams can contribute to the screening of COVID-19, but for the final diagnosis the identification of viral RNA using RT-PCR is necessary[25,26].
CT is able to show important findings for early detection of the infection even when negative results are obtained in the RT-PCR, such as ground-glass opacities(GGO)[27]. It is worth mentioning that CXR is more often used in the evaluation of disease progression than in the detection of the infection itself due to its lower value in the early identification of GGO compared to CT[28]. LUS is a faster and safer method than the aforementioned methods and, even though it provides images with an inferior quality than those obtained with a CT scan, it has become very useful due to its practicality, as it is possible to perform this technique at the patient's bedside,whereas the other procedures involve displacement and longer periods of time[29]. Of course, all available resources for patient care should always be taken into consideration, but when dealing with a pandemic, it is of unequal importance to thoroughly evaluate aspects related to the speed and efficiency of diagnostic methods[30].
In the initial phase of the COVID-19 outbreak, when RT-PCR tests had limited availability, countries presented divergent opinions regarding the use of imaging exams in the diagnosis of the infection worldwide. With the increase in the availability of RT-PCR kits throughout the pandemic, the criteria for the use of imaging tests began to gain consensus. But, it is worth mentioning that the national guidelines vary according to factors such CT scanner availability, personal protective equipment availability, andtesting infrastructure[31]. Therefore, this review aims to describe the use of imaging exams for the detection of COVID-19, providing a broad overview on the main methods used in this context and discussing the challenges in the radiology field during the pandemic.
WHAT DO THE IMAGING EXAMS SHOW ABOUT THE DISEASE?
Although the detection of SARS-CoV-2 RNA using the RT-PCR remains the gold standard diagnostic method, the unspecific or asymptomatic initial stage of COVID-19 highlights the important role of imaging exams in assisting the early diagnosis, as well as in monitoring and identifying complications[32,29]. Figure 1 summarizes the main points regarding the imaging modalities used in COVID-19.
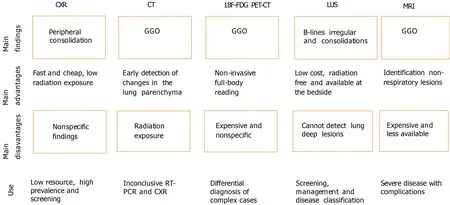
Figure 1 Highlights of imaging modalities in coronavirus disease 2019. CXR: Chest X-ray; CT: Computed tomography; 18F-FDG PET/CT: 18Ffluorodeoxyglucose positron emission tomography/CT; LUS: Lung ultrasound; MRI: Magnetic resonance imaging; GGO: Ground-glass opacities; RT-PCR: Real-time reverse transcription polymerase chain reaction.
CXR
The reduced capacity of CXR to reveal GGO, an early finding in the disease, limits its use in COVID-19 diagnosis. However, extensive consolidations, which are visible in the CXR, are common as the disease progresses[33].
Despite the sparse data in the literature on radiography in the COVID-19 context[34], the consolidation is the most common finding in the radiographs of infected patients, being predominantly observed in peripheral areas of the lower zones[35], with a peak of severity 10-12 d after the onset of symptoms[36]. Among 9 patients in Korea, the CXR detected parenchymal abnormalities in three of them, most with peripheral consolidation that was later confirmed by CT[37]. Moreover, a severity score can be used to quantify the extent of infection, with a score assigned to each lung that ranges from 0 to 4 according to the extent of lung involvement: 0 = no involvement; 1 corresponding to less than 25%; 2 = 25%-50%; 3 = 50%-75% and 4 to more than 75%. The scores obtained for each lung are then added together to provide the final gravity points[36].
A study published in October 2020 showed that chest radiographs may be reliable in predicting results from definitive COVID-19 diagnostic methods, particularly in places with limited resources and a high number of cases[38]. Radiography is the fastest and cheapest method to evaluate COVID-19 patients and it is broadly available in clinics, emergency rooms, and hospitals worldwide[39,40]. Moreover, this method is associated with a low exposure to ionizing radiation in users. In addition, the portable X-Ray units, whose mobility and cleaning are easy, have been considered as facilitating resources in emergencies[41].
However, the CXR abnormalities observed in COVID-19 are nonspecific and may overlap with findings from other infectious diseases such as influenza[42,43]. Thus, the analysis of imaging patterns on chest radiography in SARS-CoV-2 infection is complex, time-consuming, and prone to error. This evaluation is a challenge that must be considered, mainly due to the lack of specialized radiologists[39,41]. Therefore, an artificial intelligence (AI) algorithm could be used and programmed to distinguish COVID-19 pneumonia from non-COVID-19 pneumonia through CXR images[44]. The main goal of AI, when gathering imaging data and clinical information is to read image studies accurately, preferably as a screening tool[34].
A study observed sensibility and specificity of 95% and 71%, respectively, for the association between COVID-19 pneumonia with the involvement of 4 or more zones and clinical deterioration, in both critical and non-critical patients[45]. An analysis performed to determine the CXR diagnostic precision in comparison to RT-PCR in 569 patients with suspected SARS-CoV-2 infection showed, in the initial CXR, 61%sensibility and 76% specificity in the hospital environment[46]. In November 2020, an evaluation of the CXR associated with AI support for COVID-19 detection reported an increase in the diagnostic sensibility from 47% to 61%, even though the specificity reduced from 79% to 75%. This is a promising result for the possible use of AI to enhance the accuracy of this exam[39]. In conclusion, the CXR may be indicated in situations of low resources and high prevalence of the disease.
CT
There is a vast amount of information regarding CT findings in COVID-19 reported in different studies around the world[47]. It is known that the characteristics of the lung fields at CT scan change over time, with different presentations according to the stage and severity of the pulmonary infection[48].
The main feature found on a CT scan as a consequence of COVID-19 is the presence of GGO, with a predominantly bilateral and peripheral distribution[49]. Vascular enlargement is seen in GGO, representing interstitial peribronchovascular edema/inflammation and possible increased cardiac diameter[50].
In the initial stage of COVID-19, chest CT is characterized by single or multiple scattered patchy or agglomerated GGOs[51]. Subsequently, there may be an increase in the number and extent of lesions[52]. As far as the disease progresses, images show diffuse consolidation of the lungs, air bronchograms, and bronchial dilation. The resolution of the GGO and pulmonary consolidation occurs gradually, with some residual opacities remaining characteristic of fibrosis[53].
Chest CT may be useful for early diagnosis in cases of clinical suspicion, indefinite pulmonary abnormalities on CXR, and unavailable or negative RT-PCR test, and in the follow-up of severe cases[54].
A study used a chest CT severity score (CT-SS) that is based on the sum of scores from 20 regions of the lung. Each region receives a score from 0 to 2 according to the intensity of parenchymal opacification. A CT-SS threshold value of 19.5 was identified as a reliable cut-off to detect severe COVID-19, suggesting that this method may be useful in identifying people who need hospitalization[55]. Another method that aims to facilitate and standardize the assessment of patients with moderate-to-severe symptoms of COVID-19 on CT images is the COVID-19 reporting and data system(CO-RADS), which is determined according to the level of suspicion of pulmonary involvement, varying from CO-RADS 1 (very low) to CO-RADS 5 (very high).Moreover, there are some extra classifications: CO-RADS 0 for technically insufficient tests and CO-RADS 6 for cases confirmed by RT-PCR[56]. Figure 2 summarizes the aforementioned scores.
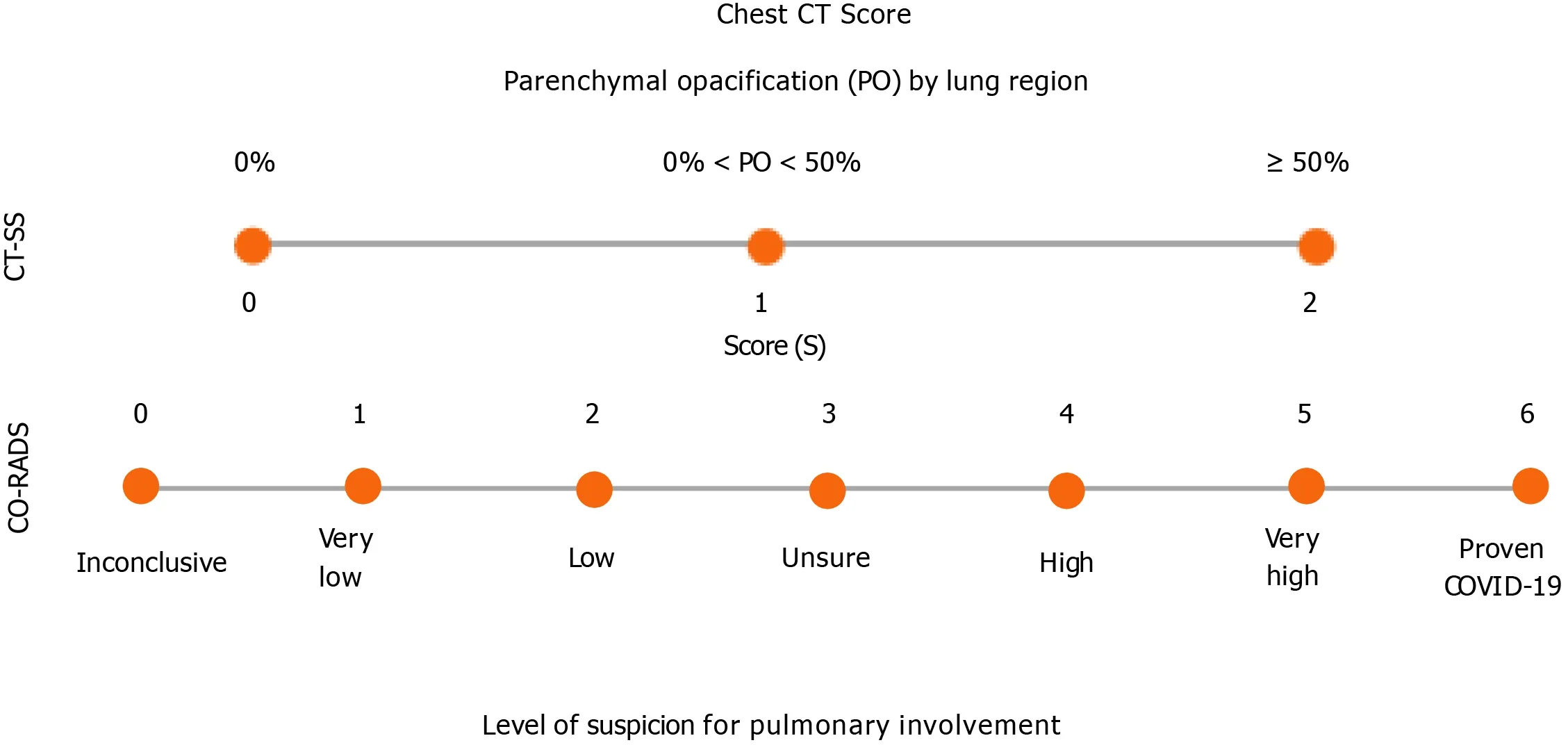
Figure 2 Summary of chest computed tomography scores to assess coronavirus disease 2019. CT-SS: Computed tomography severity score;COVID-19: Coronavirus disease 2019; CO-RADS: COVID-19 Reporting and Data System; PO: Parenchymal opacification.
Compared with the CXR, CT is more sensitive for detecting changes in the lung parenchyma in the early stages of the disease, besides enabling the monitoring of disease progression and possible differential diagnoses[57]. However, special attention is needed for non-infectious etiologies and other infectious causes, such as non-COVID-19 viral pneumonia,, and pulmonary granulomatous infections that may be similar to CT findings in COVID-19.In these cases, clinical manifestations, laboratory tests, and immunological status should also be considered to assist in the differential diagnosis[58].
Furthermore, evidence shows that some patients with a CT pattern suggestive of COVID-19 pneumonia initially have a negative RT-PCR test result, suggesting the need to repeat the diagnostic tests if there is high clinical suspicion[59]. In this sense, it is even considered that chest CT should be performed in symptomatic patients who will undergo surgery in a context that requires a quick diagnosis and RT-PCR is not available. This is important considering the high perioperative mortality of patients infected with SARS-CoV-2[60].
Despite the potential advantages of CT, factors such as the period needed to clean the imaging exam rooms, the risk of viral transmission for healthcare professionals,and radiation exposure to the patient must also be considered[61]. There is no standard for the radiation dose in cases of COVID-19, but some studies suggest singlephase, non-contrast, low-dose chest CT, which varies depending on factors such as the patient’s body habitus, in those of small and medium size, for example, volume CT dose index < 3 mGy can be sufficient[62].
Regarding diagnostic accuracy, a meta-analysis that included studies with high-risk patients for COVID-19 reported a relatively high sensitivity of chest CT ranging from 92.9% to 97%, whereas specificity was poor, varying from 25% to 71.9%[63]. It is important to emphasize that these studies are influenced by several factors such as patient selection, disease prevalence, and medical interpretation, influencing the generalization of these results[64]. A French study[65], for example, suggested that chest CT has an important role in early diagnosis in areas with a high prevalence of COVID-19. However, Kim[66] indicated that in low-prevalence settings, many false positives can occur with the use of chest CT. Table 1 summarizes diagnostic accuracy values of CXR and CT for COVID-19.
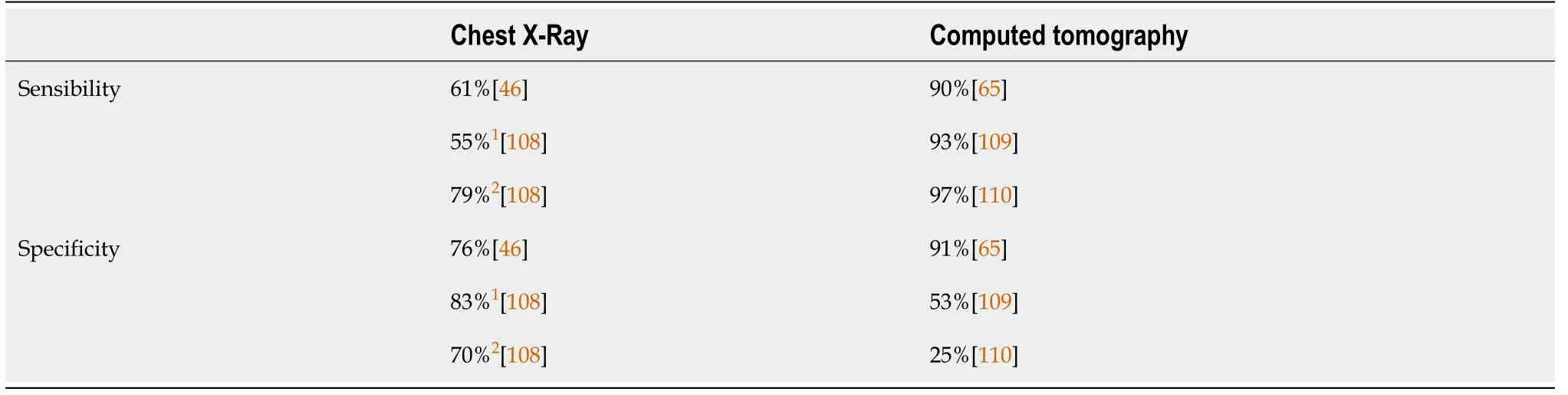
Table 1 Sensibility and specificity of chest X-Ray and computed tomography for diagnosing COVID-19
Positron emission tomography combined with CT
Although positron emission tomography combined with CT (PET/CT) and the use ofF-fluorodeoxyglucose (F-FDG) tracer in PET/CT are more complex than a simple chest CT, these imaging exams can provide morphological and functional information on infectious and inflammatory diseases[67]. The cells of the inflammatory process pick upF-FDG, which showed potential in the differential diagnosis of complex cases, as well as lung lesions caused by SARS-CoV-2[68].
F-FDG PET/CT plays an important role in the evaluation of infectious and inflammatory lung diseases, including the detection of involved pulmonary segments,estimating the extent of the lesion, monitoring progression and responses to treatment[69]. In COVID-19, PET/CT could be used as a non-invasive full-body reading to assess chronic and substantial damage to the lungs and other organs[68]. In a previous study, 38.46% of patients submitted toF-FDG PET/CT were diagnosed with COVID-19 before undergoing RT-PCR. Therefore, the authors concluded that the test can possibly identify SARS-CoV-2 infection when the findings, clinical history,and epidemiological context are related[70]. Moreover, this exam should also be done to evaluate the impact of possible damage, especially in patients from groups at increased risk for severe disease who present with respiratory symptoms[71]. Previous studies have reported that the main COVID-19 imaging findings were accidentally detected in cancer patients submitted to the exam[72,73]. When these findings were correlated with clinical and epidemiological data, they strongly suggested the SARSCoV-2 infection[70], facilitating the patient’s management.
The main imaging findings reported usingF-FDG PET/CT in COVID-19 are the presence of GGOs with areas of focal consolidation, mainly in the peripheral regions,as well as an interlobular septal thickening in one or both lungs[74,75]. Furthermore,positiveF-FDG lymph nodes in the mediastinal, hilar, and subclavian regions can also be observed[74]. In the early stages, COVID-19 pneumonia presents with segmental GGO and nodal involvement in the peripheral and posterior regions of the lungs, while disease progression is accompanied by an increase in the number oflesions as well as in their extension and density. In addition, a mosaic paving pattern and air bronchogram sign have also been identified[76].
TheF-FDG PET/CT exam has important disadvantages. The test is still expensive and inaccessible for some people, especially those living in poor countries[77]. In addition, the low physical half-life, approximately 110 min, ofF-FDG is a problem,because this limitation prevents the examination from being carried out in places distant from the producers of this tracer[78]. Another important difficulty associated with the use of this substance is that it is unable to differentiate distinct populations of immune cells and it is not specific for viral infections[72]. Thus, these limitations are very relevant when considering performing this exam.
The level of accuracy of this imaging exam in the diagnosis of COVID-19 is still uncertain. Therefore, further studies using larger cohorts are needed to understand the usefulness of this exam in COVID-19[68]. Of note, the long-term follow-up of patients is very important to identify possible chronic damage caused by COVID-19 and the role ofF-FDG PET/CT in detecting such damage[71].
LUS
LUS has evolved over the years in the diagnosis of lung diseases, becoming in the current COVID-19 pandemic an alternative mode of first-line imaging because it is a viable and highly accurate imaging exam when used at the bedside[79]. It has the advantage of being an economical alternative, more accessible to low and middleincome countries, available at the bedside, in real time, and free of radiation risks[30,80]. LUS can also assist in the screening of symptomatic patients, classification of disease severity, monitoring of patients with pulmonary findings, management related to mechanical ventilation, and treatment allocation and evaluation[81].
The challenges of using ultrasound include prolonged operator exposure and the need for scanner plates and transducers that need to be completely disinfected, in addition, another limitation of this exam is that it cannot detect deep lesions in the lung[81,82]. Although a limited number of studies have evaluated this method in COVID-19, this procedure has high sensitivity and a high level of accuracy as a diagnostic tool for pneumonia, with a sensitivity of 93% and a specificity of 95% in the evaluation of patients with the disease. Some studies have also shown high sensitivity(93%-98%) for acute respiratory distress syndrome[82]. Thus, LUS is comparable to CT,but CT shows intra-pulmonary and apical lesions more clearly and comprehensively than LUS[29]. LUS is considered advantageous for detecting smaller lesions and peripulmonary effusions as well as pleural injuries, and is a dynamic and easily accessible method[34].
The evaluation of patients with COVID-19 using LUS often shows signs that include various forms of B-lines (often separated and coalescing), an irregular or fragmented pleural line, subpleural consolidations, pleural effusions, and absence of pulmonary slippage. These findings are variable and non-pathognomonic for SARS-CoV-2 infection[34]. The specificity for this disease occurs when irregular bilateral vertical artifacts and multifocal white lung signs are present, suggesting interstitial-alveolar damage[83]. The demonstration of B-lines are described as laser-like hyperechoic artifacts that resemble a "comet tail" or "light beam" and have been commonly observed in cases of COVID-19 pneumonia; these B-lines may be associated with an interstitial syndrome and decreased aeration and when the confluents may appear as a"white lung" equivalent to the frosted glass opacities of CT. These characteristics suggest a more severe loss of lung aeration[84,29].
LUS has been a promising alternative, which can be performed very quickly, is noninvasive, can be used to identify probable COVID-19 patients in association with RTPCR and to identify pulmonary involvement and possible complications, differentiating acute signs of respiratory failure from normal function[80,85]. These characteristics aid in the management of the patient, whether in defining the need for hospitalization, ventilation or another specific therapy, and of great importance in the current pandemic[85].
MRI
MRI is not often performed in COVID-19, unlike CT[86]. However, when requested, a thoracic MRI is obtained with the respiratory navigator during the expiratory phase,thus providing valuable information for clinical evaluation[87]. MRI allows the detection of minute and fine aspects of the pulmonary parenchyma. Moreover, it detects pleural effusion and lymphadenopathy, and is a promising diagnostic tool in the detection of pulmonary nodules[88].
The most common finding in the thoracic MRI scan is GGO, which comes up due to slight interstitial thickening, edema, and hyaline membranes in the lung and may come together to form interlobular septum consolidation. This consolidation in COVID-19 occurs when there is increased density in the alveoli, and is multifocal,segmental, irregular, subpleural or peribroncovascular[88,89].
Due to the presence of the ACE2 receptor in other systems, the affinity between SARS-CoV-2 and ACE2, as well as other systemic consequences of this infection, can lead to cardiotoxicity and cardiovascular injury or thromboembolic event[90]. For this reason, greater attention should be paid to the possibility of some myocardial involvement even in recovered patients who had cardiac symptoms[91]. Within this framework, MRI has been of great value in patients with cardiovascular conditions,such as arrhythmias, fulminant myocarditis, and acute coronary syndromes[92].
In this context, cardiovascular MRI (CMR) allows the visualization of several myocarditis characteristics, such as contractile dysfunction, inflammatory edema,pulmonary artery filling defects, and necrosis[92,93]. The main methods are conventional cine images, T2-weighted sequences, parametric T1 and T2 maps, and late gadolinium enhanced images. Thus, CMR allows an anatomical and functional evaluation, revealing the different patterns of cardiac tissue damage, whether inflammatory or ischemic[93].
Moreover, MRI has become a very efficient tool in the investigation of a possible relationship between SARS-CoV-2 and nervous system abnormalities. Some studies have already suggested a neurotropism of the virus in infected patients who present with persistent severe anosmia and dysgeusia[94]. In this context, significant differences are observed in the signal intensity emitted at MRI of the olfactory bulb in patients with anosmia, presenting a T2/FLAIR hyperintensity[95].
The olfactory bulb MRI is very enlightening as it provides visualization of anatomical details and allows monitoring of the volume reduction of the bulb and respiratory tract that is directly linked to the clinical picture and presentation of anosmia[96]. This finding may be related to an initial inflammatory reaction of the nasal mucosa by the virus, as well as in the neuroepithelium of the olfactory fissure, in patients with a total loss of smell, affecting neural smell as was noted on MRI of anosmic patients[95].
It is important to note that, despite its importance, MRI is less available and more expensive than CT. However, its use is essential in the screening and monitoring of some serious neurological complications resulting from COVID-19 such as stroke,encephalitis, encephalopathy, and Guillain Barré syndrome[97].
The main indications for MRI are cases with worsening of the disease such as in the occurrence of acute necrotizing encephalopathy, with medial portion hypersignal of the thalamus on T2-weighted MRI and FLAIR sequences as well as in the subinsular region and medial portion of the temporal lobes from gadolinium ring uptake on T1-weighted sequences[89]. Furthermore, the aforementioned radiological signals are often detected in patients seeking MRI for other reasons. Thus, the radiologist’s ability to recognize those characteristic findings is crucial to detect them even in patients without a prior COVID-19 diagnosis[86].
CHALLENGES FOR THE RADIOLOGY DEPARTMENT
Infection control protocols
Radiologists, as they are among the health professionals exposed to COVID-19, must be aware of the infection control protocols, in order to prevent viral spreading among patients or between patients and healthcare professionals[31,98].
Firstly, an infection control team should be established for the radiology department[99]. It is important to use personal protection equipment (PPE), which is divided into categories according to the radiologists’ contact with patients[99]. In this sense, disposable protective caps, surgical masks, and goggles must be worn by everyone, as well as good hand hygiene[100]. For health professionals whose protection is level one, that is, people who manage registration and screening for review, disposable latex gloves and, if possible, N95 masks are recommended[100]. In levels two and three, which include those who perform diagnostic examinations such as X-Ray and CT in confirmed or suspected patients, should use the aforementioned PPE, plus a face shield as well as a disposable apron and shoe protectors[101,102].Moreover, the people who are responsible for cleaning equipment and places, and those involved in the safe disposal of infectious medical waste, must use level two PPE[103]. Figure 3 illustrates the PPE indicated to prevent infection in the radiology room.
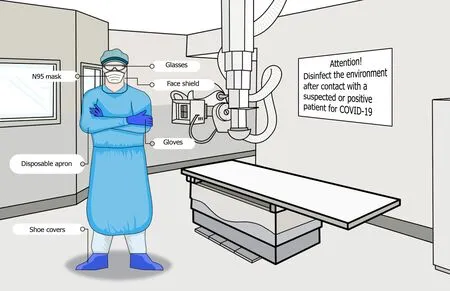
Figure 3 Safety measures to prevent infection in the radiology department. COVID-19: Coronavirus disease 2019.
The removal of clothing should be carried out after contact with suspected or confirmed individuals, and new PPE is required to proceed with a new service. The patients must always wear surgical masks[101,103]. The equipment and the environment that the patient had contact with must undergo a decontamination process[82], using soap and water or a disinfectant such as alcohol and, after cleaning,it is recommended that the room be left unused for 1 h for air circulation[43,99].
Follow-up post-COVID-19
Another challenge that emerges for the radiologists during the pandemic is the postinfection follow-up,, to control complications and assist patients during recovery.Given the lack of concrete evidence on the long-term effects of COVID-19, the British Thoracic Society guidelines determined two follow-up algorithms[104]: (1) In patients who had the most severe COVID-19 pneumonia, it is suggested that a clinical review should be conducted between 4 to 6 wk after discharge and, if CXR still shows abnormalities, new radiography must be performed within 6-8 wk; (2) In patients who had mild or moderate COVID-19 pneumonia, it is suggested that CXR be performed 12 wk after discharge[105].
However, a study of 110 patients followed for 8 to 12 wk after admission, pointed out that CXRs are not necessary in those who did not need oxygen during infection,because they are unlikely to present any abnormalities[106].
Another study noted that point-of-care ultrasound findings, performed after hospital discharge, assist in monitoring the progress of severe COVID-19 pneumonia.During follow-up, besides LUS, chest CT was used for patients with suspected residual lung injury as well as CT pulmonary angiography and echocardiography for patients with residual thromboembolic disease[107].
CONCLUSION
The COVID-19 pandemic has brought several challenges to health care systems. Due to the high rate of viral transmission, early diagnosis is essential to monitor and isolate the patient, reducing the risk of further contamination. In the initial phase of the pandemic, with the limited availability of RT-PCR tests, imaging techniques were important tools to assist in the diagnosis of COVID-19. Even with the improved availability of RT-PCR tests, over time, imaging remains useful not only for diagnosis but also for assessing disease progression and severity. Even in countries with financial and technical difficulties, imaging exams, if well managed, can assist in the diagnosis and monitoring of patients, enabling better results and reducing health costs. As the pandemic advances, some challenges are perpetuated, such as the need to maintain control to prevent and reduce risks of contamination in the radiology department, and others arise, such as the monitoring of post-COVID-19 patients.However, different to the initial phase of the pandemic, accumulated knowledge has enabled a better understanding of the main imaging findings associated with COVID-19 and the regional guidelines provide guidance on the proper use of imaging modalities considering the reality of each location. In addition, the use of AI has contributed to a more accurate diagnosis in the radiology field.
