
How well did Norwegian general practice prepare to address the COVID-19 pandemic?
2021-01-12 07:44:08IngvildVattenAlsnesMortenMunkvikDanaFlandersNicolasyane
Ingvild Vatten Alsnes , Morten Munkvik , W Dana Flanders, Nicolas ?yane
ABSTRACT
Objectives We aimed to describe the quality improvement measures made by Norwegian general practice (GP) during the COVID-19 pandemic, evaluate the differences in quality improvements based on region and assess the combinations of actions taken.
Design Descriptive study.
Setting Participants were included after taking part in an online quality improvement COVID-19 course for Norwegian GPs in April 2020. The participants reported whether internal and external measures were in place: COVID-19 sign on entrance, updated home page, access to video consultations and/or electronic written consultations, home office solutions, separate working teams, preparedness for home visits, isolation rooms, knowledge on decontamination, access to sufficient supplies of personal protective equipment (PPE) and COVID-19 clinics.
Participants One hundred GP offices were included. The mean number of general practitioners per office was 5.63.
Results More than 80% of practices had the following preparedness measures: COVID-19 sign on entrance, updated home page, COVID-19 clinic in the municipality, video and written electronic consultations, knowledge on how to use PPE, and home office solutions for general practitioners. Less than 50% had both PPE and knowledge of decontamination. Lack of PPE was reported by 37%, and 34% reported neither sufficient PPE nor a dedicated COVID-19 clinic. 15% reported that they had an isolation room, but not enough PPE. There were no geographical differences.
Conclusions Norwegian GPs in this study implemented many quality improvements to adapt to the COVID-19 pandemic. Overall, the largest potentials for improvement seem to be securing sufficient supply of PPE and establishing an isolation room at their practices.
INTRODUCTION
In Norway, the first confirmed case of COVID-19 was recorded on 26 February and the first COVID-19 death occurred on 12 March 2020. The COVID-19 pandemic has made a great impact on the Norwegian society from mid- March 2020. The prevalence of COVID-19 was by far highest in the South- East and West of Norway. To handle the pandemic, many changes had to be implemented, and like other parts of the world these included general practice (GP).1In particular, ad hoc measures were taken to prevent transmission of the virus, mostly based on GPs’ own initiative, although the local authorities were in charge of COVID-19 clinics and the distribution of personal protective equipment (PPE). According to Norwegian health authorities, 5% of GP consultations in early March 2020 were online consultations, whereas the corresponding rate by the end of April 2020 was almost 60%. This corresponds well to other countries where the aim was 70% online text or video consultations to avoid virus transmission.1Some GP offices in Norway have already been using video consultations for quite a while, whereas others had to set these up quickly.2As in other countries, vulnerable patient groups are usually provided with medical care through GPs.3To be able to provide such care, many changes were important. In addition to converting physical consultations to online, an important change was establishing separate COVID-19 clinics in the municipalities. Patients with airway symptoms or fever were referred to and evaluated in these clinics to avoid COVID-19 exposure to other patients at GP practices. These, among other measures, were necessary to keep providing good primary care services for both COVID-19 suspected cases and to the rest of the population. Around 90% of Norwegian GPs are self- employed and responsible for organising their practice in accordance with both normal and extraordinary situations. Self- employed GPs are remunerated by a mix of capitation and fee for service. They are responsible for following up patients of all age groups and will refer patients to hospitals when necessary, but diagnose, treat and monitor most conditions themselves. As in other parts of the world many GPs reorganised their practice within a short time frame.4Previous pandemics have also shown the willingness of GPs to reorganise their practice.5It is clear that GPs play a key role in both the prevention and management of a pandemic.6Nonetheless, this is the first viral pandemic that has affected Norway in this manner, and it is important to describe how Norwegian GPs responded, and possibly consider what was done well and what could be improved at a later time.
The primary aim of this study was therefore to describe some of the quality improvement measures made by Norwegian GPs in their clinics. The second aim was to evaluate whether GP offices prepared differently in different parts of the country, as the prevalence of COVID-19 in Norway differs greatly geographically. Finally, the third aim was to study the combinations of different measures to assess and if necessary provide recommendations for improvement.
MATERIALS AND METHODS
On 30 March 2020, Norwegian GPs were offered a course consisting of an online and self- organised meeting about COVID-19. The course was offered by the Norwegian Centre for Quality Improvement in Clinical Practices (SKIL). SKIL is a non- profit organisation that delivers tools for quality improvement to clinical practices and is owned by the Norwegian Medical Association. The online course contained information on where to find updated information regarding COVID-19 and important measures to ensure patient safety during a pandemic. During the subsequent meeting, participants checked and planned improvements concerning COVID-19 in their own practices. Participants received educational credits for participating (Continuing Medical Education, CME).
Invitations to participate were advertised through newsletters from both SKIL and the Norwegian Medical Association. The course was offered for free to all participants signing up until 9 April, and thereafter a fee (approximately £45) was added.
Participants
By 30 April, 187 participants from 107 different clinics had completed the digital course and the subsequent meeting, including finalising the accompanyingquestionnaire. Seven of these clinics were excluded from the analyses because they were not public GP practices. The mean number of general practitioners per practice was 5.63 (range 1–19). Fifty- seven of the practices were from the south- eastern region, 27 were from the western region and 19 were from the middle or northern regions. The central and northern regions were merged as they are similar both geographically and how they were affected by the virus. The questionnaire consisted of a total of 40 checkpoints to ensure patient safety, as well as a reflection question on what participants wanted to improve. Additionally, the questionnaire asked about the use of online consultation methods and included an evaluation form (see online supplemental material).

Table 1 Description of clinics in general practice (GP) and measures of preparatory actions to address COVID-19, by health region
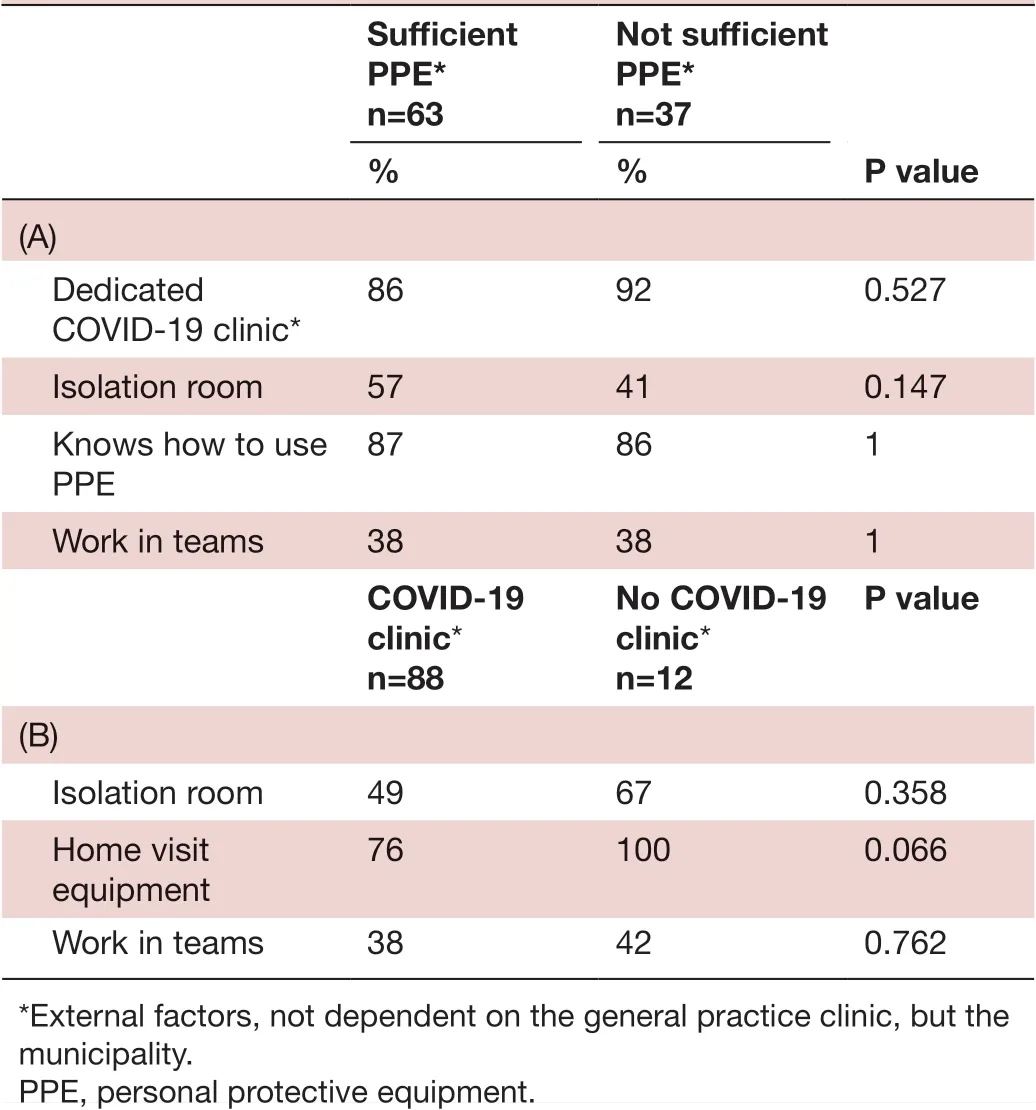
Table 2 Descriptions of and associations (A) between sufficient supplies of PPE and relevant variables and (B) between access to dedicated COVID-19 clinic and relevant variables
Statistical analyses
Descriptive analyses were performed to study the implemented safety measures. χ2tests were conducted to evaluate the statistical significance of any potential differences between the regions. χ2tests were also used to investigate whether external factors (access to PPE and municipality- organised COVID-19 clinics) were significantly associated with important internal safety measures. Some of the numbers had expected values less than 5, hence exact p values were used. There were no a priori variables or confounders to adjust for. Statistical analyses were conducted using SPSS V.25.
Ethical considerations
SKIL’s data protection officer approved the procedure for data handling before this was performed. All participants signing up to SKIL’s activities are informed of and consent to SKIL’s data handling procedures. Measures were taken so that no results could be tracked to individual participants or practices. Not at any time did SKIL gather, extract or store any data points or information concerning individual patients.
RESULTS
Table 1 describes the offices, including their size, and the proportion that have implemented certain preparatory measures, stratified by health region. Among 100 GP clinics in Norway, 56 were located in the South- East, 26 in the West, and 18 in the Central and North of Norway. There were no differences in the measured preparatory actions in the clinics based on health region nor with regard to office size. All clinics had a sign on the front door informing about COVID-19, and 94% had updated information on their home pages. Consultations could be done as written asynchronous online consultations in 85% of the clinics and by video in 88% of the clinics. All clinics could offer consultations using phones. Sufficient supplies of PPE were reported by 63%, while 87% reported that they were competent in the use of PPE, including correct dressing and undressing. Knowledge of how to decontaminate a room was reported by 73% of the clinics, while 51% had a dedicated isolation room in their clinic. Necessary equipment to make home visits was available in 79% of the clinics, while 39% of the clinics divided their staff to work in teams in order to limit the number of personnel that would need to be quarantined if exposed to SARS- CoV-2. As many as 98% had a home office option for at least one of the doctors in their practice, while only 36% had a home office option for at least one of the health secretaries in their practice. Public COVID-19 clinics were available in 88% of participating clinics.
Table 2A,B presents the proportions with or without sufficient supplies of PPE in relation to the presence of a COVID-19 clinic, isolation room, knowledge on how to use PPE and whether the personnel were organised in mutually exclusive teams. Only 55% both have sufficient PPE and the knowledge to use it, and 36% reported both having an isolation room and sufficient PPE. COVID-19 clinics were available in 88%, and 43% had both access to an isolation room in their own clinic and public COVID-19 clinics. However, 8% of the total number of GP offices did not have access to either a COVID-19 clinic or an isolation room. Working in teams combined with access to COVID-19 clinics was reported by 33% of practices, while 5% worked in teams with no access to a COVID-19 clinic.
Table 3A–C shows that 37% reported not having sufficient supplies of PPE, and 11% did not know how to decontaminate a room and did not have sufficient supplies, although 4% (of the total) in this group had an isolation room. Of the clinics 63% reported sufficient PPE, and approximately a quarter of these did not know how to decontaminate a room. However, almost half ofthose who did not know how to decontaminate had an isolation room. Three- fourths of the participants identified potential for improvement during the course (data not shown).
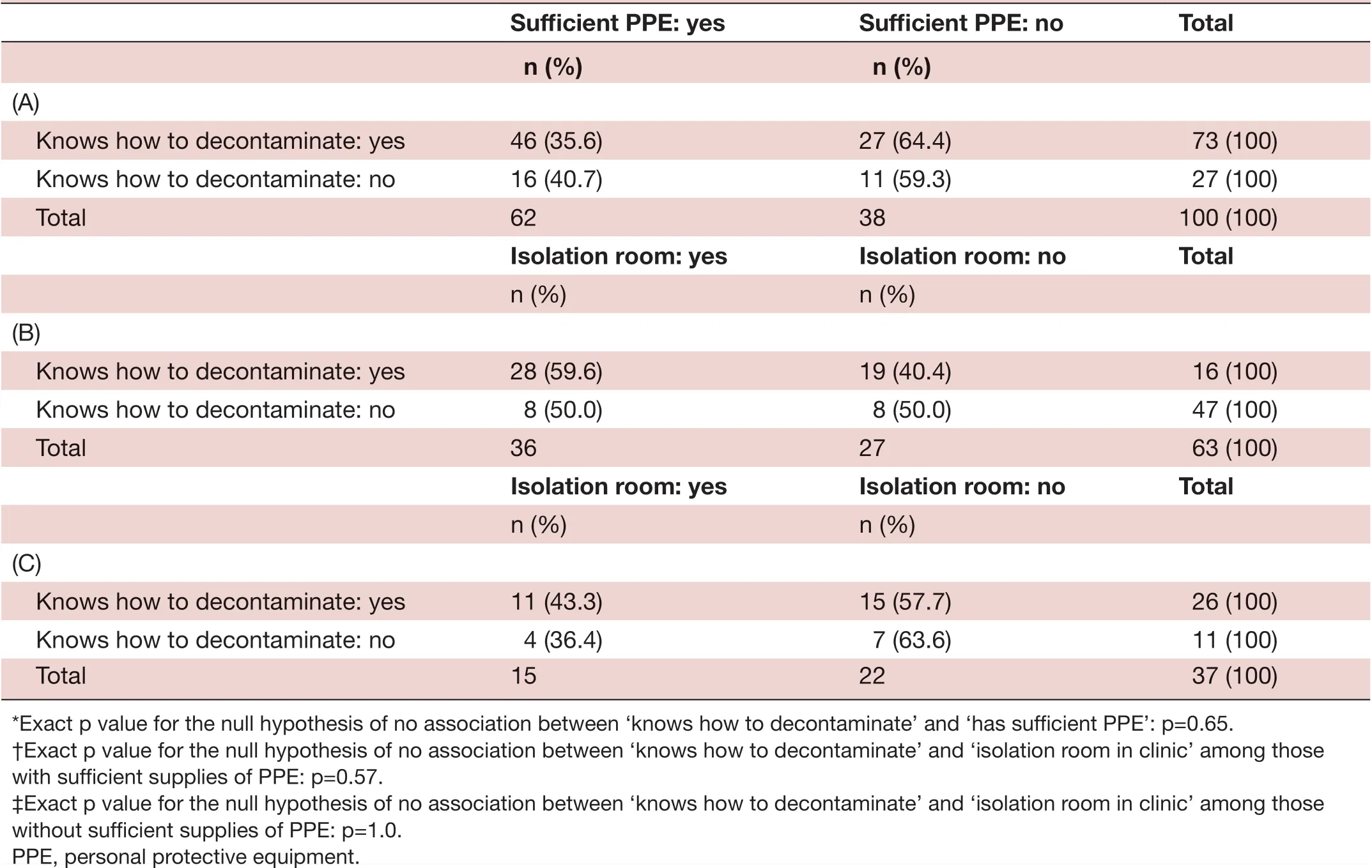
Table 3 Descriptions of and associations (A) between ‘knows how to decontaminate’ and ‘has sufficient supplies of PPE’*, (B) between ‘knows how to decontaminate’ and ‘isolation room in clinic’ among those with sufficient supplies of PPE?, and (C) between ‘knows how to decontaminate’ and ‘isolation room in clinic’ among those without sufficient supplies of PPE?
DISCUSSION
The main findings of this study are that among the 100 GP clinics in Norway, most had quickly implemented important measures to reduce the risk of COVID-19 transmission to both health personnel and other patients. Most of the practices had a sign about COVID-19 on the front door, updated home page, access to a dedicated COVID-19 clinic in the municipality and the option to conduct consultations through video or in writing, knowledge on how to use PPE, and an option for home office for general practitioners. Some preparedness measures should sensibly be combined, and it is reasonable to assume that the choices made by medical professionals are not in contradiction to a logic. It was therefore somewhat surprising that the combination of having PPE and at the same time knowledge on decontamination was low, at just under 50%. The use of PPE and knowledge about how to decontaminate are essential to avoid transmission of the virus among healthcare workers and visiting patients, and it is interesting that this only applies to 50% of the participating GPs in this study. Not having sufficient supplies of PPE was reported by 37% of the clinics, and 34% report neither sufficient PPE nor a dedicated COVID-19 clinic in the municipality. Of the clinics, 15% reported that they had an isolation room, but not enough PPE. Interestingly, there were no differences between implemented measures by clinics based on which health region they were located. Overall, the largest potentials for improvement seem to be securing sufficient supply of PPE and establishing an isolation room at their practices.
A strength of this study is that it includes 100 GP offices with more than 500 general practitioners in total. This represents about 10% of the public primary care doctors in Norway. To our knowledge, there have been no studies on quality measures implemented to address the COVID-19 pandemic in GP clinics, and hence this study is original. The endpoints are reliable, and it is easy for the participants to answer yes or no. The most obvious weakness of the study is the selection of participants. There is likely to be participation bias as the doctors most interested in COVID-19 will attend such a course and fill out the worksheet and may thus represent clinics which have implemented more quality measures than the rest. On the other hand, the need to improve the quality of the practice might also have recruited participants with improvement potentials. There were no a priori confounders to adjust for, as there are no established associations between COVID-19 and these quality measures. None of the findings presented in the tables is statistically significant. This may be a reflection of the fact that the GPs included in this study implemented most of the changes similarly.
To our knowledge this is the first study to address safety measures for COVID-19, and we can thus not compare our findings. The study adds to the growing body of knowledge about COVID-19 and describes how GP practices rapidly adapted to organisational challenges due to the COVID-19 pandemic. This is reflected by GP colleagues in Hong Kong who have also conducted measures towards response efficacy.7It also raises concern about the supply of PPE, which seems to be a global phenomenon.38In a publication by Razaiet al9there is for example a description on how to handle COVID-19 suspected cases in a GP clinic, with isolation rooms, use of PPE, waste bag for clothes and so on. There is also a segment on home visits.9These pieces of advice are very useful for GPs, and in our study we have attempted to look into whether GPs follow such advice or whether some of the actions taken are random, such as setting up an isolation room when there is no access to PPE or knowledge about decontamination within the staff. Another British publication points to the lack of PPE and also the general lack of specific guidance to GPs.4As mentioned previously, we found that access to PPE and having knowledge of decontamination were just under 50%. This may lead to the assumption that some offices tried to comply with government advice in a short time frame to address the COVID-19 pandemic, rather than to have a holistic and well- thought- through response. It will be interesting to see in the future whether this perhaps changes, as our data were from the first 6 weeks after heavy restrictions were implemented. Moreover, the British publication states that UK GPs turn to video and telephone consultations at an unprecedented pace, which one must say also seems to be the case in the 100 Norwegian GP clinics in our study. A recent Cochrane review states that it is easier for healthcare workers to adapt to infection prevention and control when they see the value of it.10As the prevalence of COVID-19 has been highest in the South- East and West of Norway, we wanted to see whether these regions were more motivated to implement changes in their GP clinics. However, our results show that, among the 100 included clinics, there were no differences in quality measures based on location. Nevertheless, the measures taken among GPs operating in areas with the highest COVID-19 prevalence may have had a favourable effect on limiting the transmission of the virus, as the death rate has flattened towards the end of April.11Such positive results could stimulate other clinics to prepare similarly even though local prevalence is low. The fact that most GPs are self- employed might have affected their willingness and effectiveness to rapidly reorganise their practices to adapt to the new situation. Being self- employed may affect the leniency to make changes to the organisation of their practices. We would expect that they would be more resilient to change due to economy, but as most practices have readily changed during the COVID-19 pandemic it seems this is not the case. Two publications by Greenhalghet al1213point to the use of video consultation. It has certain elements that are better than telephone alone, but with obvious limitations compared with physical consultation. Nonetheless, it has been widely implemented in our study population.
CONCLUSION
GP clinics in Norway rapidly adapted to the COVID-19 pandemic. Municipality support (presence of a COVID-19 clinic), external supply lines (sufficient PPE) and physical factors (dedicated isolation rooms) seem to be the largest potentials for improvement. Still, in the early phase of the COVID-19 pandemic most GP offices seem to have implemented many important measures to ensure patient and staff safety. Hopefully, by evaluating what has been done so far it will be possible to implement further adaptations wisely. It is necessary to continue to do research on how COVID-19 has affected GPs, and by doing so setting the groundwork for evidence- based guidelines to be used in future pandemics.
AcknowledgementsWe would like to acknowledge the Centre of Quality Improvement in Medical Practices and the participants who contributed to the questionnaire, making this study possible.
ContributorsIVA, MM and WDF contributed to the design, analyses and writing of the manuscript. N? contributed to the idea, design and writing of the manuscript.
FundingIVA and MM received a grant from the Research Fund for Primary Care in Rogaland, Norway (part of the Norwegian Medical Association) to evaluate the responsiveness of Norwegian GP offices in the face of the COVID-19 pandemic. Otherwise the authors received no external funding to conduct this work.
Competing interestsWDF owns a company, Epidemiologic Research & Methods, which does consulting work. He knows of no conflicts of interest with this work.
Patient consent for publicationNot required.
Ethics approvalAccording to the Norwegian Act on Medical and Health Research, the study did not require approval from the Regional Committee for Medical and Health Research Ethics because data were originally gathered as part of a quality improvement (QI) initiative and not primarily for research purposes. This was also the conclusion by the Regional Committee for Medical and Health Research Ethics (ref 2019/422) done for a similar and recent study that has been submitted and is currently under review.
Provenance and peer reviewNot commissioned; externally peer reviewed.
Data availability statementData are available upon reasonable request.
Supplemental materialThis content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer- reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Open accessThis is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY- NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non- commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non- commercial. See: http:// creativecommons. org/ licenses/ by- nc/ 4. 0/.
ORCID iDsIngvild Vatten Alsnes http:// orcid. org/ 0000- 0002- 2136- 6664 Morten Munkvik http:// orcid. org/ 0000- 0002- 5687- 583X
 Family Medicine and Community Health2020年4期
Family Medicine and Community Health2020年4期
- Family Medicine and Community Health的其它文章
- Perceived barriers and primary care access experiences among immigrant Bangladeshi men in Canada
- The process of transprofessional collaboration: how caregivers integrated the perspectives of rehabilitation through working with a physical therapist
- Reformulation and strengthening of return- of- service (ROS) schemes could change the narrative on global health workforce distribution and shortages in sub- Saharan Africa
- New hypertension and diabetes diagnoses following the Affordable Care Act Medicaid expansion
- Family medicine residency training in Ghana after 20 years: resident attitudes about their education
- Exploring the structure of social media application- based information- sharing clinical networks in a community in Japan using a social network analysis approach