
Endoscopic ultrasound-measured muscular thickness of the lower esophageal sphincter and long-term prognosis after peroral endoscopic myotomy for achalasia
2020-12-10 04:08:18YeLiaoTingYueXiaoYuFanWuJingingZhangBaoZhenZhangYiDanWangShengWangXiangLiuSiYuSunJinTaoGuo
World Journal of Gastroenterology 2020年38期
Ye Liao, Ting-Yue Xiao, Yu-Fan Wu, Jing-ing Zhang, Bao-Zhen Zhang, Yi-Dan Wang, Sheng Wang, Xiang Liu, Si-Yu Sun, Jin-Tao Guo
Abstract
Key Words: Peroral endoscopic myotomy; Achalasia; Endoscopic ultrasound
INTRODUCTION
Achalasia is currently the most common primary esophageal motility disease[1]. While its etiology remains uncertain, achalasia is characterized by the destruction of inhibitory ganglion cells in the myenteric plexus, causing severe myopathy in smooth muscles and leading to aperistalsis and impaired relaxation of the lower esophageal sphincter (LES)[1,2]. In addition, thickened lower esophageal muscularis propria (LEMP) has been observed in individuals with achalasiain vivoand during autopsies[3-7]. LEMP hypertrophy may be a response to esophageal functional obstruction or a primary lesion[2]. Hence, LEMP thickness is thought to be associated with the diseasestate.
Existing treatments for achalasia, including pharmacotherapy, clostridium botulinum injection, endoscopic balloon catheter dilation, and Heller myotomy, target the compulsory release of the stenosis segment of the LES. Peroral endoscopic myotomy (POEM) has emerged as an increasingly utilized treatment approach, especially in patients with multiple comorbidities who cannot undergo laparoscopic or open surgical interventions[8,9]. POEM is considered safe for patients as young as 3 years old, with no upper age limit, according to several efficacy studies with a maximum follow-up period of 3 years[10-13].
Despite its safety, patients who undergo POEM are at risk for disease recurrence[14-16], although there is no recognized predictor. However, treatment history, type of mucosal damage, and reflux symptoms were included in a newly developed risk prediction scoring system[17]. Considering that the POEM procedure is performed directly on the muscularis propria and LEMP thickness is associated with the postprocedural balloon catheter dilation outcome[7], LEMP thickness is thought to be associated with POEM outcome. However, no correlation between muscle thickness and prognosis at 1 year after POEM has been reported[18,19], and few studies with longer follow-up periods include assessment of the relationship between LEMP thickness and POEM outcomes.
Therefore, this study aimed to examine the relationship between LEMP thickness, measured by endoscopic ultrasound (EUS), and patient characteristics including longterm prognosis after POEM for achalasia at our health center in the past 7 years.
MATERIALS AND METHODS
Patients
All medical records of patients who underwent POEM to treat achalasia at Shengjing Hospital of China Medical University from January 2012 to September 2018 were retrospectively reviewed. The inclusion criteria were diagnosis of achalasia and record of LEMP thickness measured by EUS examination before POEM. The exclusion criteria were as follows: (1) History of gastrointestinal open surgery; (2) Gastrointestinal malignancy; (3) Coagulopathy or other systemic disorders that precluded safe use of general anesthesia; and (4) Unwillingness to provide informed consent.
From the patient medical charts, demographic information, disease duration defined by time of symptom onset to POEM procedure, symptoms, Eckardt scores[20], degree of esophageal dilation based on the upper gastrointestinaltract X-ray, endoscopy findings, thickness of LEMP according to EUS findings, and treatment outcomes were collected for analysis.
Ethics
This study was approved by the Institutional Review Board and the Ethics Committee of China Medical University. All patients voluntarily chose their therapeutic course and provided written informed consent for the POEM procedure. Written informed consent was obtained from the parents or guardians of patients younger than 18 years of age.
Symptom evaluation
Clinical symptoms of all patients were evaluated according to the Eckardt score before and after the procedure. The Eckardt score is the sum of the symptom scores for dysphagia, regurgitation, retrosternal pain (with a score of 0 indicating the absence of symptoms, 1 indicating occasional symptoms, 2 indicating daily symptoms, and 3 indicating symptoms at each meal), and weight loss (with 0 indicating no weight loss, 1 indicating a loss of < 5 kg, 2 indicating a loss of 5-10 kg, and 3 indicating a loss of > 10 kg)[20]. Therefore, scores could range from 0 to 12, with 0 representing no symptoms.
EUS evaluation
All EUS evaluations were performed by experienced technicians using a 360° Radial-Array Ultrasound Gastroscope (EG-3870URK; PENTAX Medical, Tokyo, Japan) and an ultrasound scanner (EUB 6500; Hitachi, Tokyo, Japan). The thickness of the muscularis propria at the esophagogastric junction (EGJ) was assessed before POEM, and a thickness of ≥ 3 mm was considered thickened. The cutoff value for the muscular thickness was determined according to the ordered sample cluster method based on age, disease duration, preoperative Eckardt score, and postprocedural outcome. The completeness of the myotomy was verified by EUS after POEM.
Endoscopic procedure of POEM
POEM procedures were performed by three experienced therapeutic endoscopists.
Patients fasted for 24-48 h and were forbidden from drinking water for 4-6 h before the procedure. If gastroscopy or EUS revealed any liquid or food residue in the esophagus, a decompression tube was indwelled for at least 24 h before POEM, and nutrients were introduced intravenously. During the procedure, patients were placed in the left recumbent position under general anesthesia with tracheal intubation. The POEM procedure was performed as follows: (1) A submucosal injection (Boston Scientific, United States) of a mixture of saline and methylene blue was administered into the esophageal wall at 12-15 cm above the EGJ; (2) A submucosal tunnel passing over the EGJ was created using a hook knife (KD-620LR; Olympus Corp., Tokyo, Japan) or a triangle tipped knife (KD-640L; Olympus) extending 3 cm into the proximal stomach; (3) Inner circular myotomy began 2-3 cm below the tunnel entry and ended at the cardia; and (4) After careful hemostasis using hemostatic clips (FD-410LR; Olympus), several metal clips [ROOC-D-26-195; Micro-Tech (Nanjing) Co., Ltd., Jiangsu, China] were applied to close the mucosal entry. CO2was used as the endoscope air supply. Prophylactic antibiotics and proton pump inhibitors were administered intravenously for at least 2 d after the procedure.
Assessment of therapeutic response and follow-up
Follow-up for all patients was conducted by telephone calls or clinic visits, and clinical symptoms were assessed using the Eckardt score. The procedure was considered effective, and the patient was in clinical remission if the postoperative Eckardt score was ≤ 3. Relapse was defined as a rise in the Eckardt score to > 3 after a period of clinical remission[15]. For patients who underwent the procedure twice, the first set of data was used to analyze the disease recurrence rate.
Statistical analysis
Statistical analyses were performed using SPSS version 25.0 software (IBM, Armonk, NY, United States). Normally distributed continuous variables are expressed as the mean ± SD and were compared using at-test. Categorical data were compared using the chi-squaretest and are expressed as numbers (percentages). The association between age and disease duration was analyzed by univariate logistic regression analysis. Recurrence-free survival was investigated using the Kaplan–Meier estimate of time-to-event and compared using a log-rank test. After confirming that the possible risk factors satisfied the proportional hazard hypothesis, the Cox proportional hazards model was used to evaluate risk factors for clinical recurrence.P< 0.05 was considered statistically significant. The ordered sample cluster analysis was performed using DPS version 7.05 software (Zhejiang University, Hangzhou, China)[21].
RESULTS
Muscle features of the lower esophageal sphincter in patients with achalasia
Eighty-two patients (32 males and 50 females aged 17-78 year with a mean age of 46.5 ± 14.9 year) and a total of 85 procedures were included. The average disease duration was 102.4 ± 127.2 mo (range, 1-516 mo). All patients denied having a previous diagnosis of esophageal disease. Six patients had a history of an endoscopic procedure. Of all patients, 63 (76.8%) had a thickened LEMP.
Data on the correlation between patient background and LEMP thickness are shown in Table 1. Significant differences in age (48.4 ± 14.4 yearsvs40.4 ± 15.2 years,P< 0.05) and disease duration (126.63 ± 138.49 movs37.79 ± 35.52 mo,P< 0.05) were observed between the thickened and non-thickened LEMP groups, and both variables were associated with thickened LEMP. Specifically, older patients with longer disease duration were more likely to have a thickened LEMP. In addition, there was a positive correlation between patient age and duration of the disease (Figure 1).
The degree of esophageal dilation in 53 patients was evaluated, while the rest of the patients underwent barium esophagraphy at other medical centers and were not included. Of these, 21 (39.6%), 24 (45.3%), and 8 (15.1%) patients exhibited degrees I, II, and III dilations, respectively.
Therapeutic effect of POEM and long-term prognosis
The overall POEM success rate was 94.12% (80/85 procedures). There was only one reported case of post-procedure infection, which was resolved using conservativetreatment. The EUS data confirmed complete myotomy after POEM in 62 cases. Sixty patients had follow-ups between 8 and 87.5 mo (mean: 35.4 ± 17.2 mo)after the procedure. Five patients with Eckardt scores > 3 refused further follow-up after their symptoms were relieved. There were no significant differences in age, sex, disease duration, preoperative Eckardt score, or LEMP thickness between the effective (n= 55) and ineffective (n= 5) groups. The relapse rate was 12.73% (7/55 cases). Five patients, four of whom had a thickened LEMP, had symptom recurrence within 12 mo after the procedure. One patient who had a thickened LEMP relapsed after 24 mo while another, who did not have a thickened LEMP, relapsed after 30 mo. Overall, the effectiveness (absence of relapse) of POEM was 87.3% up to 87 mo postoperatively (Figure 2).
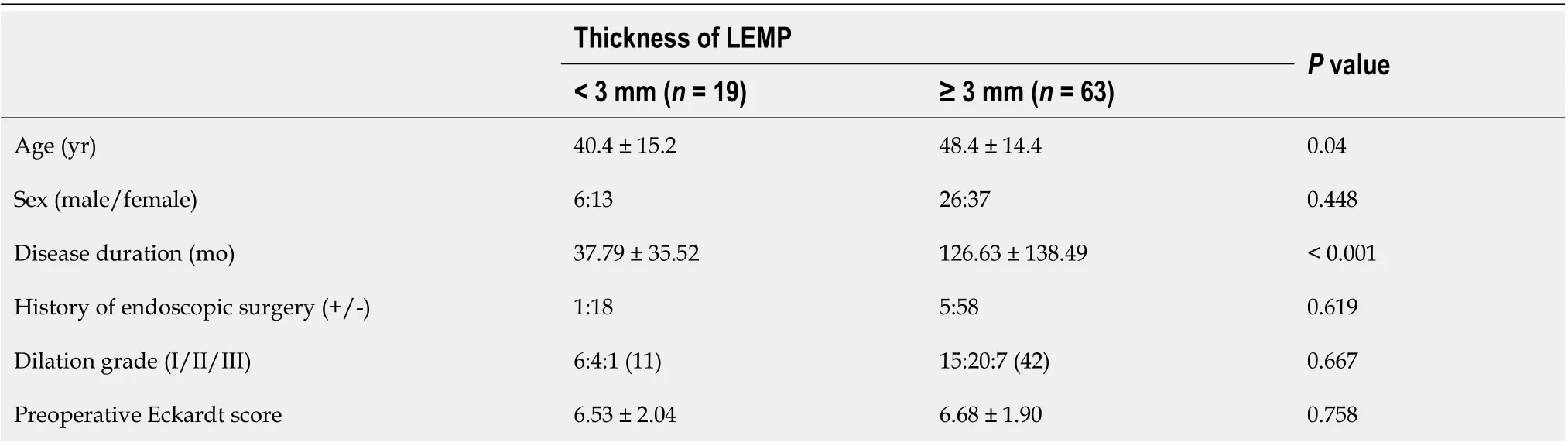
Table 1 Comparison of characteristics between patients with non-thickened and thickened lower esophageal muscularis propria
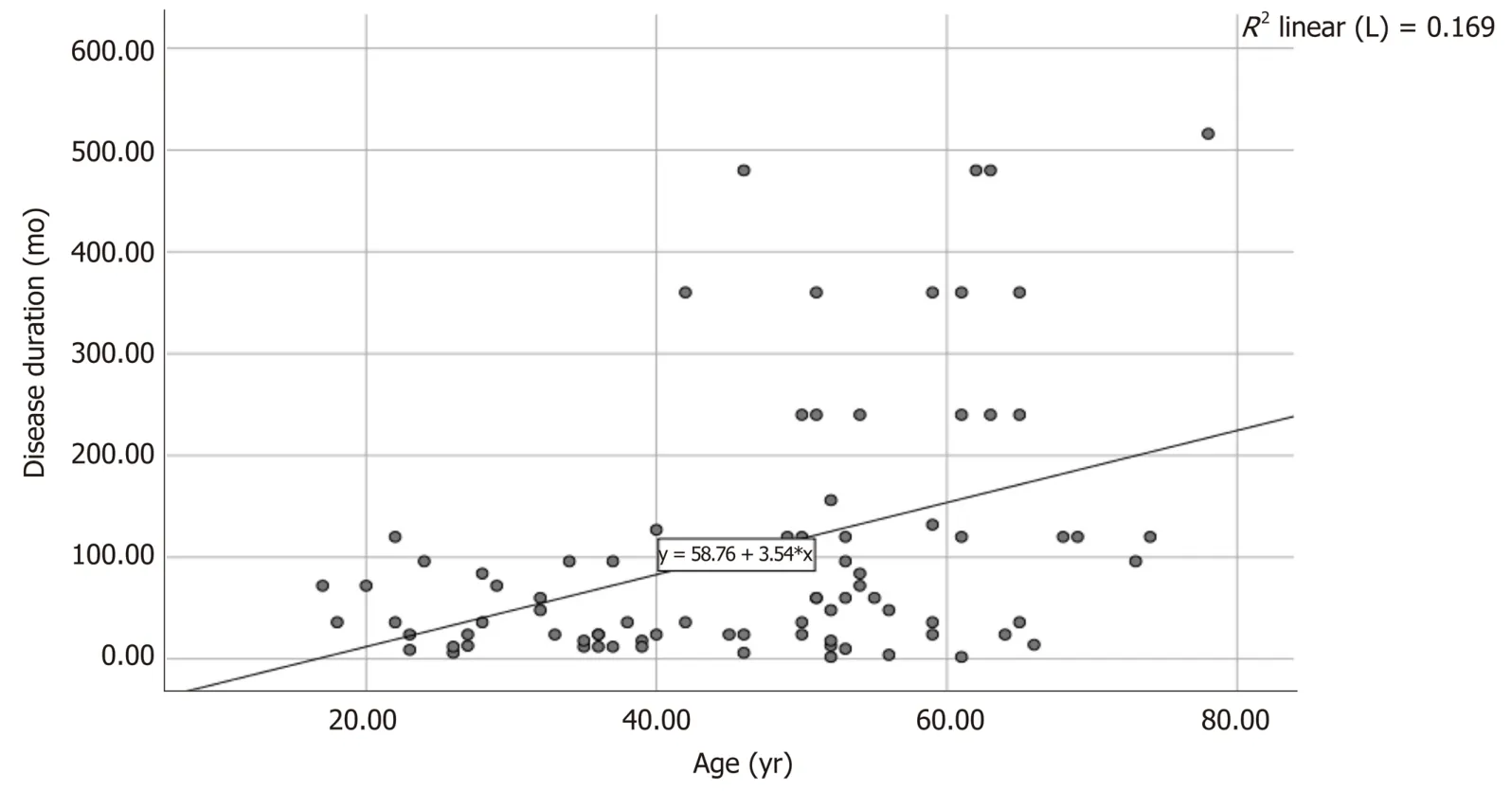
Figure 1 Correlation between age and disease duration in individuals with achalasia (P < 0.05, R2 = 0.169).
Patients with symptomatic recurrence were younger and had shorter disease duration. The relapse rate in patients without a thickened LEMP tended to be higher than patients with a thickened LEMP (2/11 patientsvs5/44 patients). However, no significant difference was found. Data on patient characteristics according to POEM outcomes are shown in Table 2 and Figure 3. Younger age (hazard ratio = 0.92; 95% confidence interval: 0.865-0.979;P< 0.05) and male gender (hazard ratio = 7.173; 95% confidence interval: 1.277-40.286;P< 0.05) were found to be associated with recurrence according to Cox regression analysis (Table 3).
DISCUSSION
Although several previous studies have demonstrated that LEMP thickness is associated with POEM procedure duration and outcomes, the present study adds to the literature by specifically examining the relationship between LEMP thickness andlong-term outcomes, including disease relapse after POEM. The results from the present retrospective chart review and statistical analysis suggest that non-thickened LEMP may be associated with increased disease recurrence. In addition, there is a correlation between older age, longer disease duration, and thickened LEMP.
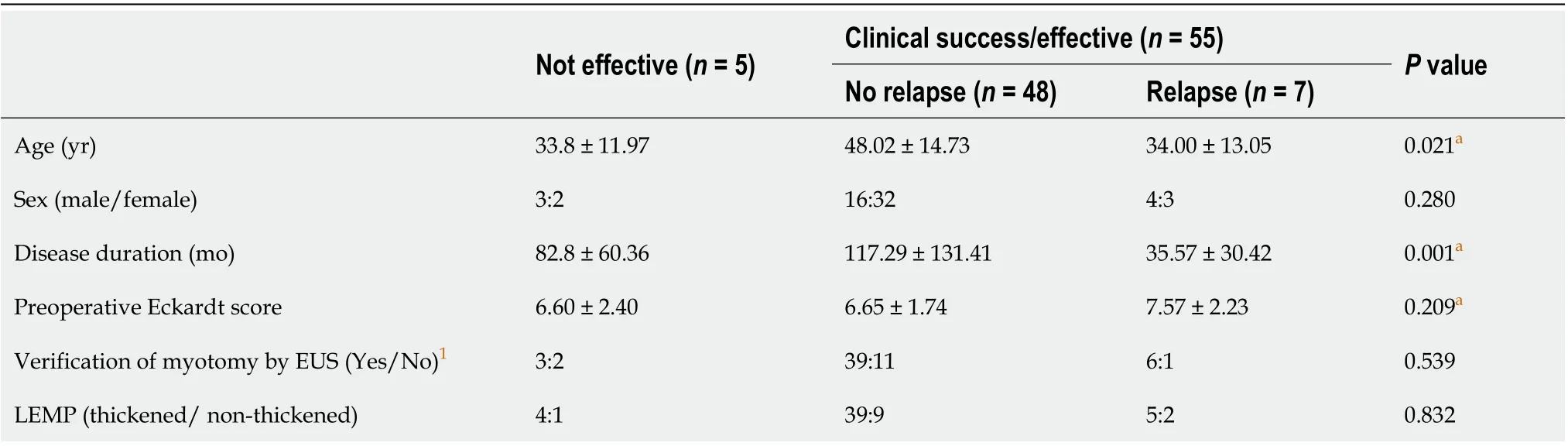
Table 2 Comparison of characteristics in patients with different outcomes after peroral endoscopic myotomy
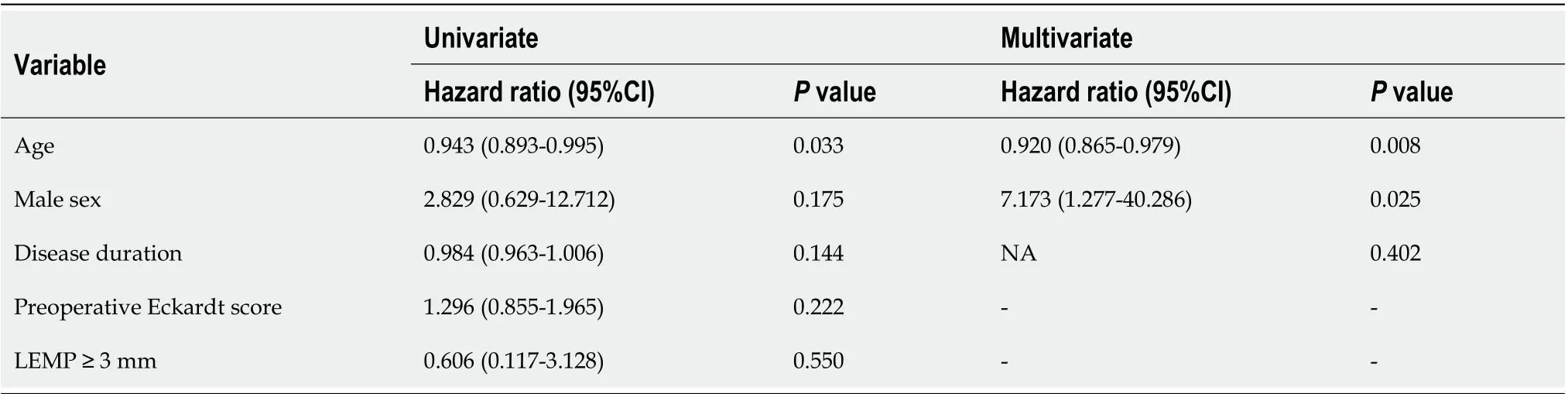
Table 3 Risk factor analysis for recurrence using the Cox proportional hazards model
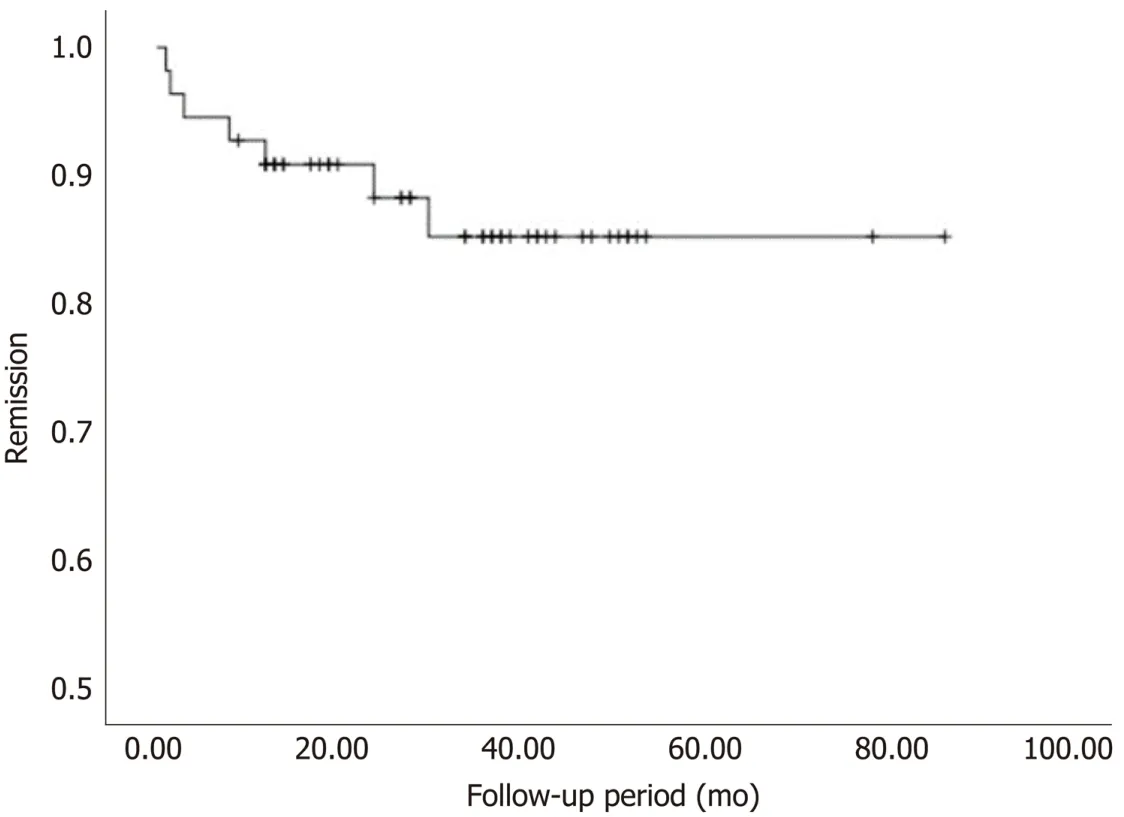
Figure 2 Kaplan–Meier analysis of recurrence after peroral endoscopic myotomy.
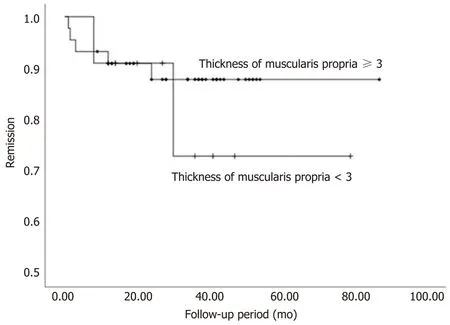
Figure 3 Kaplan–Meier estimate of time to recurrence according to muscularis propria thickness.
In previous reports, no significant correlation has been found between the severity of achalasia evaluated by Eckardt score and LEMP thickness[19,22]. However, age, pneumatic dilation history, and male sex have been reported as predictors of a thickened LEMP in several studies[6,19,22,23]. Similarly, the present study showed a positive association between age and muscle thickness. In addition, the present analysis found an association between disease duration and LEMP thickness, as patients with a thickened LEMP had a significantly longer disease course. The results may be attributed to differences in patient characteristics among the studies as we also found a positive association between age and disease duration. Thus, the thickened LEMP could be due to prolonged exposure to reactive hyperplasia since longer disease duration means longer stimulation time. The reversibility of the LES hypertrophy after POEM provides supporting evidence for this theory[18].
The thickness of the LEMP may be associated with procedural outcomes and postoperative prognosis. We were not able to statistically evaluate the relationship between POEM-related complications and muscle thickness due to the small sample population. Previous studies have shown, without statistical significance, that there tended to be a positive association between muscle thickness, procedure duration, and complication rate[24]. As for postoperative prognosis, symptomatic recurrence has been reported to occur between 2-5 years after POEM[14]. A medium-term recurrence rate of 18% was reported in a 2-year follow-up study. Although no explanations for recurrence were given, there was an association between younger age and increased rate of relapse[16]. Watanabeet al[18]reported no significant difference in clinical outcomes between patients with thick and those with thin LEMP in a 1-year follow-up study, observing no cases of recurrence.Liet al[15]reported a cumulative recurrence rate of 13.7% at 5 years post-POEM that correlated with disease duration and interventional treatment history. In the same study, age and symptom severity showed no correlation with achalasia relapse.
Since the analysis of the present study confirmed a relationship between patient characteristics and LEMP thickness, the effect on recurrence was also analyzed. Although there was no statistical significance, there was a slightly higher relapse rate in patients with non-thickened LEMP. The lack of statistical significance may be due to the treatment of the muscle thickness measurements as discontinuous data. Patients with a younger age and shorter disease duration had an increased rate of relapse. This may be explained by the better healing ability in younger individuals and the fact that patients with shorter disease duration did not have adequate reactive hyperplasia of the LES after esophageal functional obstruction. Our results may suggest that POEM in patients with a certain LEMP thickness caused by reactive hyperplasia has a lower disease recurrence rate.
Cox analysis showed that disease duration was not associated with recurrence, whereas age remained an effective predictor. This may be explained by the co-linear relationship between age and disease duration. Male sex was also a risk factor for recurrence, although the large confidence interval may indicate that this was a result of a sampling error. Besides, the extent of myotomy was not associated with POEM prognosis[25]. Therefore, our result is still reliable, although we are not able to discuss the effect of the degree of myotomy on prognosis after POEM as all patients enrolled underwent myotomy of the same degree in this study. Our result, which shows that younger age is associated with increased recurrence, concurs with the findings of Werneret al[16]but contradicts those of Liet al[15,16]. Therefore, the association between age, disease duration, and relapse after POEM remains unclear, and further large-scale validation studies are needed.
The Chicago classification, based on high-resolution manometry, is a predictor of achalasia treatment outcomes. Subtype II has the best prognosis, whereas the prognosis of subtype I is slightly poorer and subtype III can be difficult to treat[26]. Patients within the achalasia subtypes tend to have similar LEMP thicknesses[19,24]. The difference in prognostic efficacy between LEMP thickness and subtype is still unclear. However, some participants in our study were not available for manometry. To include a larger sample size in the present study, we did not evaluate the relationship between Chicago classification and POEM prognosis, nor did we compare the subtypes with LEMP thickness. We expect future studies to reveal the relationship between achalasia subtypes, LEMP thickness, and POEM prognosis.
LEMP thickness may help in diagnosing achalasia. A thickened LEMP in patients with achalasia was first observed in an autopsy[4]and with the development of EUS, measurement of the intrinsic muscle layer thicknessin vivois feasible[8,27-30]. Using a 7.5-MHz ultrasound endoscope, Devièreet al[3]reported a thickened LEMP in individuals with achalasia compared with healthy controls. Conversely, Ponsotet al[31]argued that those results may have been attributable to puckering of the EGJ and found that the LEMP was not thicker in patients with achalasia than in healthy controls. In the 30 years since these studies, the number of studies that use different EUS techniques and include more participants have increased. Our results agree with many of these studies, where most of the individuals in the present study had a thickened LEMP[5-7]. This suggests that LEMP thickness may be of value in achalasia diagnosis. However, because the identification of the differences in LEMP structure between patients with achalasia and healthy individuals is not easy, the use of muscle thickness in diagnosing achalasia is still controversial.
Our study has several limitations. First, it was done retrospectively and without a healthy control group for comparison of LEMP thickness according to age and other patient characteristics. Second, there was no protocol for measuring the esophageal wall thickness and variations in measurements have been noted in previous studies. Third, evaluation of disease severity and recurrence using the Eckardt score can be highly subjective where physicians may tend to report more marked symptom improvement than patients[32]. Fourth, the cross-sectional area (CSA) of the muscularis propria may be a better indicator to estimate the degree of hypertrophy since a disassociation between muscle thickness and the CSA in some individuals with a dilated esophagus was observed. Patients with a dilated and distended esophagus may have a thin LEMP but a high CSA because of distension of the esophageal wall[5]. Fifth, although the normal value of LEMP thickness is unknown, the cutoff of 3mm is higher than that in previous studies[3,23,24]. This suggests that our patient population may not be the best representative of Achalasia patients in general, a fact that might undermine the external validity of the results. However, considering the difference of age and disease duration in patients with different LEMP thicknesses, we believed that the 3mm cutoff in this study is reasonable. In addition, the pathophysiology of achalasia is not fully understood and the role of muscular features in the progression and prognosis of the disease is still undetermined. Therefore, future studies should focus on clarifying the etiology of the disease to explain the mechanisms associated with its pathophysiology.
CONCLUSION
Most patients with achalasia have a thickened muscularis propria determined by EUS measurement. Therefore, it is likely that EUS can help diagnose achalasia. Patients with a thickened muscularis are typically older and had a longer disease course. Younger age and male gender are associated with recurrence in the present study. Patients with a thin muscularis propria may have a higher risk of symptomatic recurrence, but validation through further large-scale studies is needed.
ARTICLE HIGHLIGHTS

ACKNOWLEDGEMENTS
We thank Professor Si-Yu Sun, the co-corresponding author of this article, for his support and guidance to this study, as well as all other doctors who participated in this study.
 World Journal of Gastroenterology2020年38期
World Journal of Gastroenterology2020年38期
- World Journal of Gastroenterology的其它文章
- Role of artificial intelligence in the diagnosis of oesophageal neoplasia: 2020 an endoscopic odyssey
- Molecular mechanisms of viral hepatitis induced hepatocellular carcinoma
- Tacrolimus and mycophenolate mofetil as second-line treatment in autoimmune hepatitis: Is the evidence of sufficient quality to develop recommendations?
- Comparative study between bowel ultrasound and magnetic resonance enterography among Egyptian inflammatory bowel disease patients
- Monitoring hepatitis C virus treatment rates in an Opioid Treatment Program: A longitudinal study
- Longitudinal decrease in platelet counts as a surrogate marker of liver fibrosis