
Outpatient prevention counseling for malaria in northwest Nigeria: A single-centre descriptive cross-sectional study
2020-05-15 08:58:18GodpowerChineduMichaelBukarAlhajiGremaIbrahimAliyuMuhammadBabaUsmanZainabAbdulazeezUmar
Godpower Chinedu Michael, Bukar Alhaji Grema, Ibrahim Aliyu, Muhammad Baba Usman, Zainab Abdulazeez Umar
1Department of Family Medicine, Aminu Kano Teaching Hospital, Kano Nigeria
2Department of Paediatrics, Bayero University Kano/ Aminu Kano Teaching Hospital, Kano, Nigeria
3Department of Paediatrics, Aminu Kano Teaching Hospital, Kano, Nigeria
ABSTRACT
Objective: To assess the proportion of caregivers of children and patients who received malaria prevention counseling from their healthcare provider at the time of outpatient malaria treatment.
Methods: This was a descriptive cross-sectional study involving 353 randomly selected adult patients and caregivers of children attending the general and paediatric outpatient clinics of a Nigerian hospital.An interviewer-administered questionnaire was used to collect data on participants’ sociodemographics and last malaria-episode characteristics. Chi square test and logistic regression analysis were used to determine factors associated with and predictors of receiving malaria-prevention counseling, respectively.
Results: The mean age of the respondents was (33.6±9.6) years;they were predominantly females (257, 72.8%). Most had at least secondary-level education (304, 86.1%); the family size was mostly 1-6 persons in 202 (57.2%) respondents. They were treated mostly by doctors 256 (72.5%), but only 132 (37.4%) received malaria prevention counseling. Educational-level (χ2=5.42, P=0.02), family size (Fisher’s exact, P=0.01), place of treatment (Fisher’s exact,P=0.0002), pretreatment malaria test (χ2=9.48, P=0.002), who prescribed treatment (Fisher’s exact P=0.001), consultation time (χ2=22.09, P<0.001), and previous demand for malaria prevention counseling (χ2=36.59, P<0.001) were associated with receiving malaria prevention counseling. However, consultation time [Odd ratio (OR)=2.38, 95% confidence interval (CI): 1.28, 4.40, P=0.006]and previous demand for malaria prevention counseling (OR=3.62,95% CI: 2.15, 6.10, P<0.001) were independent predictors of receiving counseling.
Conclusions: The proportion of respondents that received malaria prevention counseling was surprisingly low. This offers opportunity for policy review towards improving the quality of outpatient malaria care through alternative strategies for giving malaria prevention information, especially in busy clinics where consultation time is constrained.
KEYWORDS: Counseling; Healthcare provider; Malaria;Outpatients; Prevention
1. Introduction
Forty percent of the world’s population is at risk of malaria, which is a preventable, life-threatening infectious disease[1]. Although malaria is caused by five different Plasmodium species, Plasmodium (P.)falciparum transmitted by infected female anopheline mosquito is responsible for the most severe symptoms and deaths associated with malaria. Globally, malaria control efforts have led to reduction of malaria morbidity and mortality between 2000 and 2015[2,3].However, in 2017 this progressive decline in malaria cases stalled;there were 219 million malaria cases and 435 thousand malaria deaths worldwide in 2017 whereas 216 million cases and 445 thousand deaths were recorded in 2016[2,4]. This increase of about 3 million malaria cases in 2017 suggests that malaria control efforts have weakened. Furthermore, the African region still contributed 90% and 93% of global malaria cases and deaths, respectively in 2017; Nigeria alone accounted for 25% of malaria deaths worldwide[2]. Malaria, therefore, remains a disease of public health importance in Nigeria.
Effective use of insecticide treated nets (ITN) has been central in the prevention of malaria (indoor) in sub-Saharan Africa (Nigeria inclusive), especially in combination with indoor residual spraying and environmental management[1,3]. However, this has not yielded the desired results probably because of challenges with achieving universal coverage for ITN (availability of one net for every two individuals per household)[3], and its inappropriate use (including incorrect hanging and inconsistent use)[5-8]. Strategies to increase ownership and use of ITNs had involved health education campaigns by multidisciplinary teams, social marketing, developing a net culture through promotion and publicity, increased availability (including local production of high-quality ITNs), free ITN distribution campaigns and cost reduction (e.g. reduced taxes imposed on ITNs[9]. Furthermore, in the post-2015 period (2016-2030), strategies such as ensuring universal access to malaria prevention, diagnosis and treatment, accelerating efforts towards attainment of malaria-free status and transforming malaria surveillance to a core intervention have been advocated[10]. These programmes require multi-sectoral approach and community ownership of campaigns to achieve the desired objectives.
Unfortunately, there is poor documentation of the efforts of healthcare providers who are influential agents of health promotion with regards to their patients and the community. Studies have not only shown that opportunities exist in the primary care setting for disease prevention counseling but also that this intervention can result in behaviour change towards disease prevention[11-13].Besides, healthcare providers who treat malaria are often involved in counseling of malaria patients or their caregivers on measures of malaria prevention or reinforce their knowledge of effective preventive measures that they previously obtained from other sources.
Hence, this study was undertaken to assess the proportion of outpatients with suspected or confirmed malaria who received counseling on malaria prevention from their healthcare providers.We also assessed the characteristics of their last episode of malaria and factors associated with receiving malaria prevention counseling.It is hoped that the study can serve as a baseline for future studies in outpatient malaria care. It may also help strengthen advocacy for increased involvement of healthcare providers in malaria preventive efforts especially in outpatient settings.
2. Patients and methods
2.1. Study design and setting
A descriptive cross-sectional study was carried out at the general and paediatric outpatient clinics of Aminu Kano Teaching Hospital(AKTH) Kano in August 2018. Kano is known for its commercial activities. It is the capital of Kano State in northwest Nigeria. It lies in the Sahel savanna, with a hot, semiarid climate and an average rainfall of about 690 mm (27.2 inches) annually, most of which occurs from June to September. Malaria is endemic in Nigeria with moderate-to-high transmission in all states[14]. AKTH is a 550-bed capacity federal government-owned tertiary hospital, offering health care services to people of the state and neighbouring states of Nigeria. A majority of the patients are from the Hausa/Fulani ethnic group; however, the Yoruba and Igbo ethnic groups also constitute a substantial proportion of patients. The General Outpatient Clinic (GOPC) and Pediatric Outpatient Clinic (POPC) are run by consultants, residents and general duty doctors from Family Medicine and Pediatrics Departments of the hospital, respectively.Adult patients and caregivers of children attended the GOPC and POPC, respectively.
2.2. Eligibility criteria
All patients (≥18 years of age) attending the GOPC who recalled having a malaria episode in the preceding 12 months were included.Similarly, all caregivers of children (≥18 years of age) attending the POPC with their child/dependent who recalled that their child/dependent had a malaria episode in the preceding 12 months were also included in this study. However, patients with emergent conditions, neuropsychiatric disorder, the elderly (≥65 years), and those that declined to sign the written consent were excluded. A caregiver of children was defined as an adult (≥18 years of age)who had biological (e.g. parent), adoptive, legal or social relationship with the child and from whom the child derived physical, nutritional and psychosocial support[15].
2.3. Sample size estimation
A sample size of 385 was estimated using the formula [n=(Zα)2pq/d2][16]; where n=minimum sample size, Zα=standard normal deviation corresponding to a 5% level of significance (1.96),P=50% (empirical proportion of participants who received malaria prevention advice from their healthcare providers), q=1-p (50%)and d=level of precision (set at 5%). Clinic records showed that the average weekly turnover of patients at the GOPC and POPC were 1 250 and 650, respectively; making a total 7 600 patients in both clinics over the four-week study period. Therefore, with a population of <10 000, the formula[n/(1+n/N)][16] was used to estimate the sample size; where N is the sampling frame (7 600). The sample size of 350 was therefore, obtained. This was rounded off to 380.
2.4. Sampling method
At registration, a trained research assistant identified all adults(patients/caregivers) who had completed registration for possible recruitment. A systematic random sampling technique was then used to proportionately select every 20th (obtained from the quotient of the sampling frame by the estimated sample size, 7 600/380=20)eligible caregiver or patient attending the POPC and GOPC,respectively, after the first had been selected by balloting until the sample size of 130 (POPC) and 250 (GOPC) was obtained. The flow chart of participant selection is shown in supplementary Figure 1.
2.5. Data collection
A designed, pretested, interviewer-administered, semi-structured questionnaire was used to obtain participants’ sociodemographics(age, gender, ethnicity, religion, marital status, family size,educational level and employment status) in section one and their last malaria episode characteristics (number of weeks from last malaria episode, where malaria drug was prescribed, whether malaria blood test was done, which health care provider prescribed treatment, how long participant spent with healthcare provider,whether they received malaria prevention counseling, a list of the preventive measures they were asked to use, whether they have ever asked their health care provider about malaria prevention and if regular counseling from their healthcare provider would help them stick to preventive measures) in section two. The questionnaire,originally in English language was translated into Hausa (the common local language) by a family physician and a linguistic professional experienced in health surveys and back translated into English to check for consistency and semantic validity. The internal validity of the questionnaire was determined using Cronbach’s alpha and a value of 0.82 was obtained. Two trained research assistants(general duty doctors) along with three researchers (GCM, MBU,ZAU) administered the questionnaires while participants were receiving care in designated consulting rooms. Regular supervision of the research assistants and review of completed questionnaires was carried out daily by the principal investigator (GCM). The primary outcome measure was “receipt of malaria prevention counseling” during their last malaria episode. This was assessed using the question “Did your healthcare provider talk to you about how to prevent malaria illness? The responses were “No”, “Yes”,“Not applicable”, and “I can’t remember” (“Not applicable” was the option for respondents who self-diagnosed and treated malaria at home); “Received no counseling” was defined by responses of“No”, or Not applicable” (no respondent had the response of “I can’t remember”); whereas a response of “Yes” was defined as “Received counseling”.
2.6. Ethical considerations
Ethical approval was obtained from the Research Ethics Committee of Aminu Kano Teaching Hospital (No. NHREC/21/08/2008/AKTH/EC/2225). Written informed consent was obtained from each participant after explaining study objectives. Confidentiality of obtained data was maintained.
2.7. Statistical analysis
Data were entered and analyzed using Epi Info Version 7.1.1.14,(Centre for Disease Control, Atlanta, GA). It was summarized using frequency tables, means and standard deviations. Chi square test was used to assess relationship between variables and receiving malaria prevention counseling. Independent predictors of receiving malaria prevention counseling were determined by multivariate analysis(using logistic regression) of variables associated with malaria prevention counseling. P value of less than 0.05 was considered statistically significant.
3. Results
3.1. Sociodemographic characteristics of respondents
A total of 353 questionnaires (representing 92.9% response rate)were completed during the study period and were analyzed. The respondents were predominantly females (257, 72.8%) and the mean age was (33.6±9.6) years (range 18-63) (Table 1). They were predominantly of the Hausa tribe (248, 70.3%) and Muslims (318,90.1%). A majority were married (296, 83.9%), had 1-6 persons per household (202, 57.2%), with a median family size (head count of all individuals per household) of 6.0 [interquartile range (IQR): 4.5-8.5]. Most of them had at least secondary school education (304,86.1%) and were gainfully employed (189, 53.5%).
3.2. Characteristics of respondents’ last malaria episode
Table 2 shows that most of the respondents had their last malaria episode in the preceding 13 weeks (276, 78.2%). Most reported having received treatment in a clinic or hospital (258, 73.1%).However, only 190 (53.8%) had malaria blood test before drug treatment. Most respondents (256, 72.5%) reported that anti-malarial drug was prescribed by a doctor. Most respondents spent at least 10 minutes with their healthcare provider (196, 55.5%), while 19(5.4%) had no contact with healthcare provider. However, only 132(37.4%) respondents received malaria prevention counseling from their healthcare provider. One hundred and twenty-nine (36.5%)respondents or 97.2% (129) of those who reported receiving malaria prevention counseling mentioned at least sleeping under ITN as a preventive measure they were advised to use. Most (260, 73.7%) had never sought malaria prevention counseling from their healthcare provider, but a majority 343 (97.2%) believed that regular counseling from their health care provider will help them stick to malaria preventive measures.
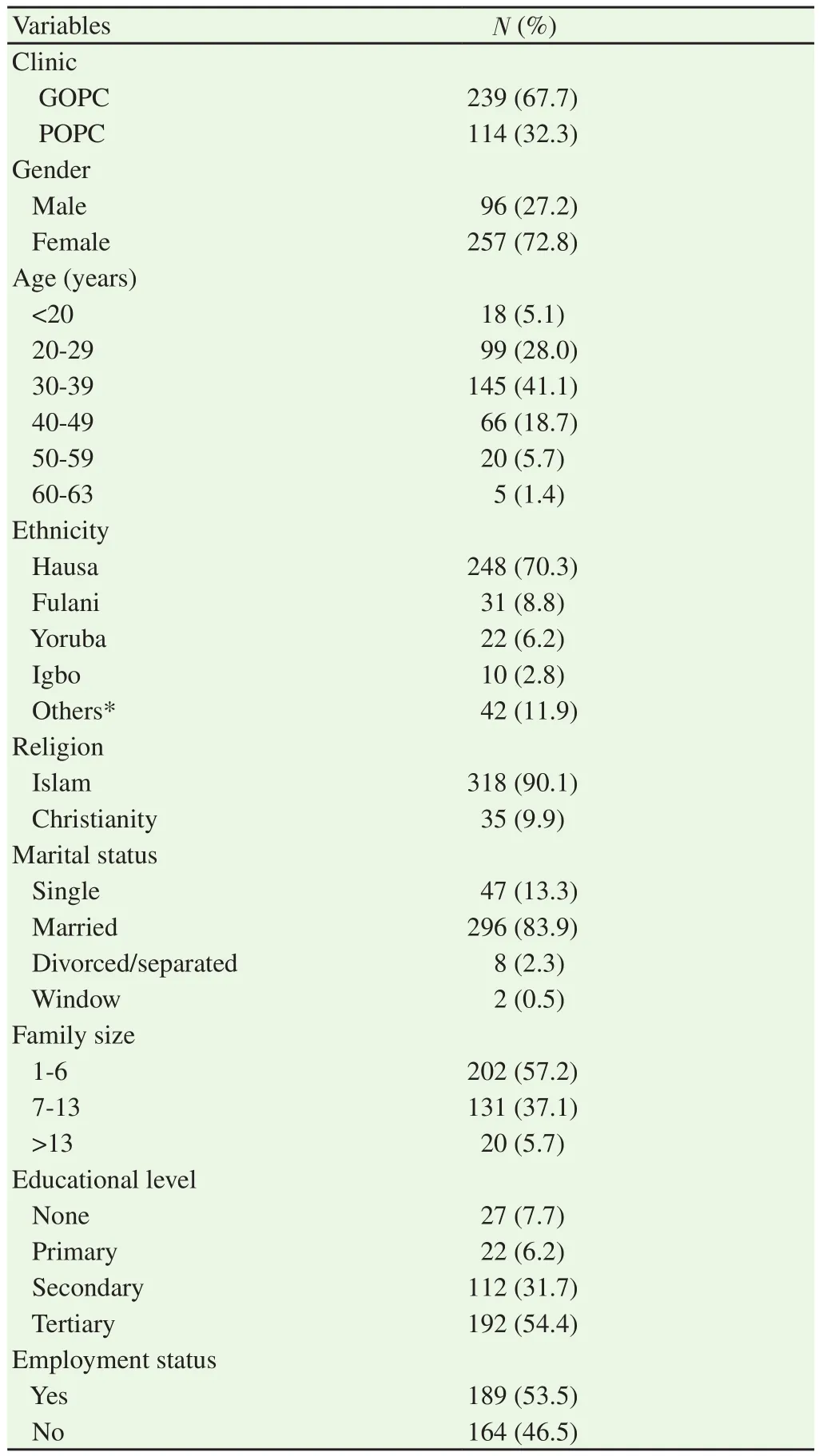
Table 1. Sociodemographic characteristics of respondents.
3.3. Factors associated with receiving malaria prevention counseling among respondents
Table 3 shows that there were statistically significant associations between respondents educational level (χ2=5.42, P=0.02), family size(Fishers exact, P=0.01), place of treatment (Fisher’s exact, P=0.0002),pre-treatment malaria blood test (χ2=9.48, P=0.002), healthcare provider (Fisher’s exact, P=0.001), time spent with healthcare provider(χ2=22.09, df (degree of freedom)=2, P<0.001), previous demand for malarsia prevention counseling (χ2=36.59, P<0.001) and receiving malaria prevention counseling. However, there were no significant associations between reported receipt of malaria prevention counseling and respondents’ clinic, age, gender, or interval from their last malaria treatment.
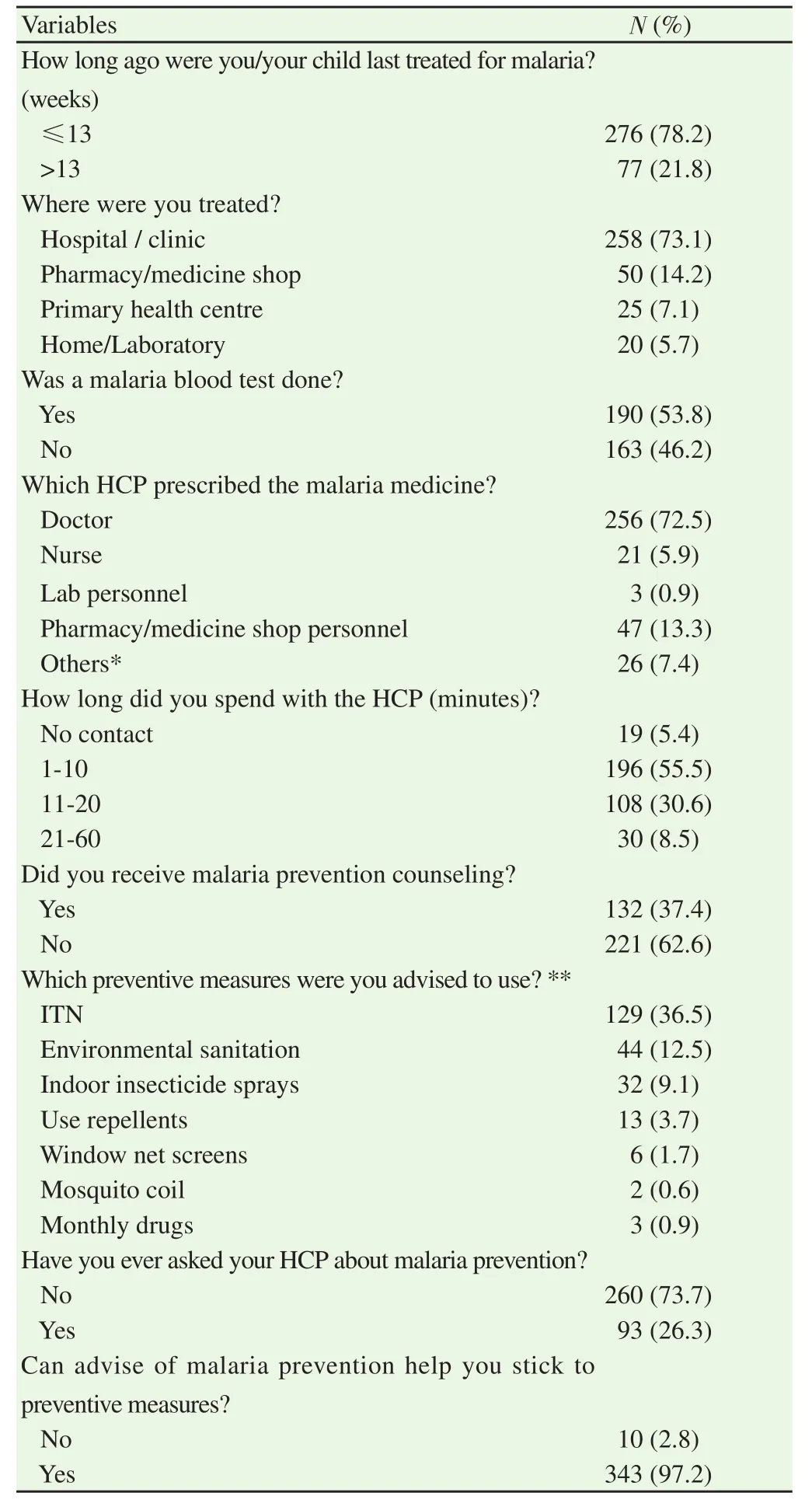
Table 2. Characteristics of respondents’ last malaria episode.
3.4. Predictors of receiving malaria prevention counseling among respondents
Logistic regression of variables associated with receipt of malaria prevention counseling (Table 4) shows that time spent with healthcare provider [Odd ratio (OR)=2.38, 95% confidence interval (CI)=1.28-4.40, P=0.006] and previous demand for malaria prevention counseling (OR=3.62, 95% CI=2.15-6.10, P<0.001)were the predictors of receiving malaria prevention counseling from healthcare providers.
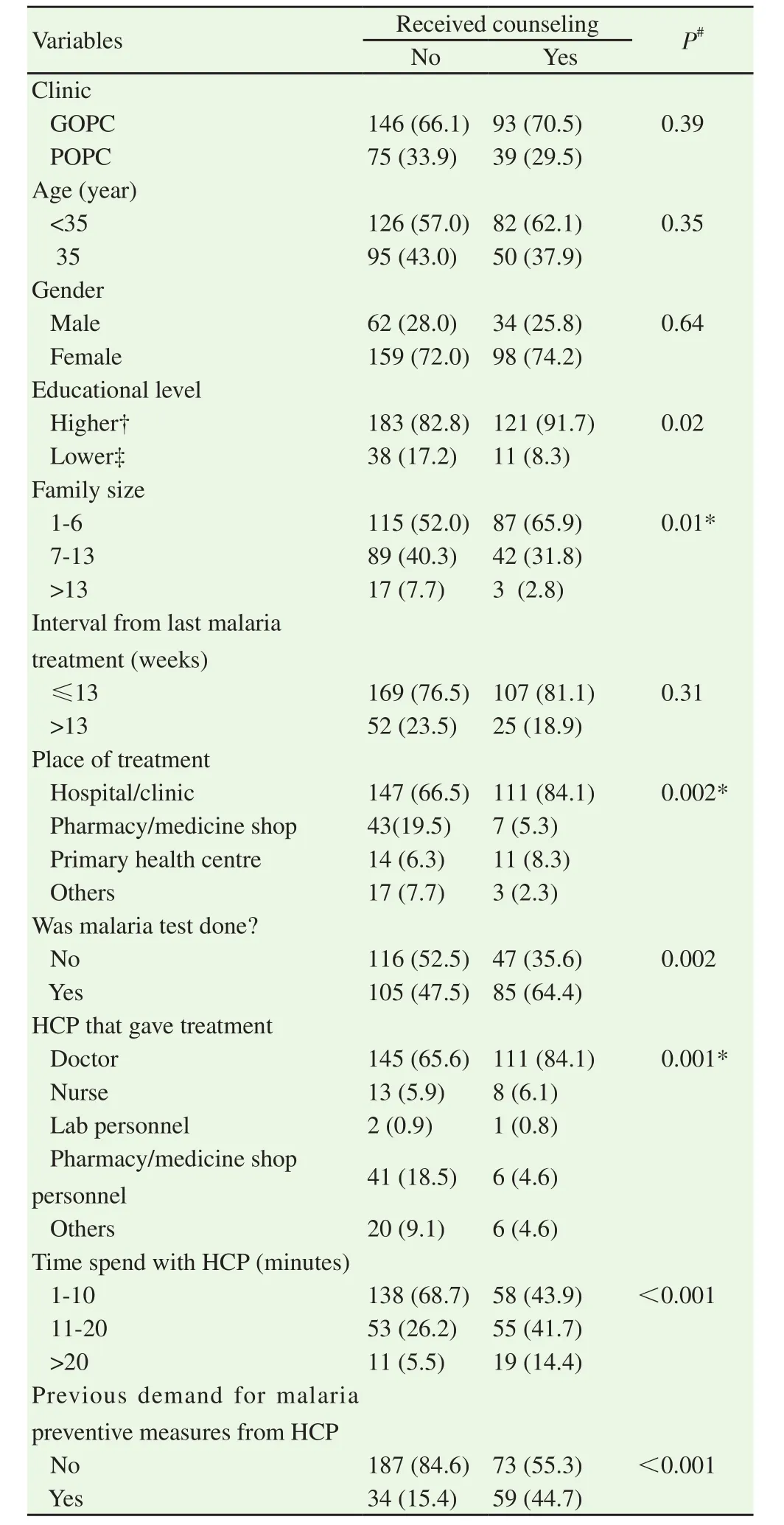
Table 3. Factors associated with receiving malaria prevention counseling among respondents [n (%)].
4. Discussion
This was a hospital-based study among outpatients that assessed the proportion of adult patients and caregivers of children who reportedly received malaria prevention counseling when they last treated malaria. In Africa (Nigeria inclusive), the dearth of skilled health care providers has resulted in the use of nurses and other community health workers to deliver effective healthcare interventions[17]. In this study, respondents reported that doctors,nurses, community health extension workers, laboratory, and pharmacy/medicine shop personnel prescribed malaria medicines for suspected or confirmed malaria. This is in line with the community case management of malaria, an established route of distribution of artemisinin-based combination therapy for the treatment of malaria.It is an effective strategy in the control of malaria in rural as well as urban areas[18].
We found that only 37.4% of the respondents reportedly received malaria prevention counseling. This surprisingly low finding may be due to the reported high level of knowledge of malaria in urban Nigerian patients and the consequent neglect of this aspect of care by health care providers[6,19,20]; however, these studies have also reported the disparity between knowledge of malaria and practice[6,19,20]. Secondly, it could also be due to poor healthcare provider knowledge of malaria prevention as was reported in a multi-centre study (Ghana, Laos, Senegal and Tanzania) where only a few healthcare providers correctly answered knowledge questions on ITNs[18]. Moreover, in this study, a greater proportion of malaria prevention counseling was given by doctors, suggesting that knowledge and skill gap of other healthcare providers could partly be responsible for this trend. Thirdly, the national guideline for malaria treatment has not clearly stated the need for counseling on malaria preventive measures at the time of treating an index patient[21].
Furthermore, we observed no significant difference in the proportion of respondents that received malaria prevention counseling from the clinic overseen by family physicians (GOPC)and pediatricians (POPC); suggesting that this deficiency in malaria care is prevalent across disciplines that treat outpatients.
We also found that among the factors associated with receiving malaria prevention counseling (including respondents’ educational level, family size, place of treatment, healthcare provider thatprescribed treatment, having pre-treatment malaria test, time spent with health care provider and previous demand for malaria prevention counseling), time spent with the healthcare provider(contact or consultation time) and previous demand for malaria prevention counseling were the independent predictors of receiving malaria prevention counseling. These findings are remarkable because our hospital’s outpatient charter prescribes a consultation time of 10 to 15 minutes per patient. However, we found that there was over a two-fold increase in the odds of receiving malaria prevention counseling when their reported consultation time exceeded 15 minutes. This suggests that time constraint and probably the dismal health worker to patient ratio existing in many developing nations may be responsible for the small proportion of respondents that received malaria prevention counseling. Similarly, previous demand for malaria prevention counseling predicted receiving malaria prevention counseling, suggesting active patient participation in the control of malaria by some of the respondents. Such patients that seek counseling are important targets for offering health-related counseling as they are more motivated and likely to practice malaria preventive measures.
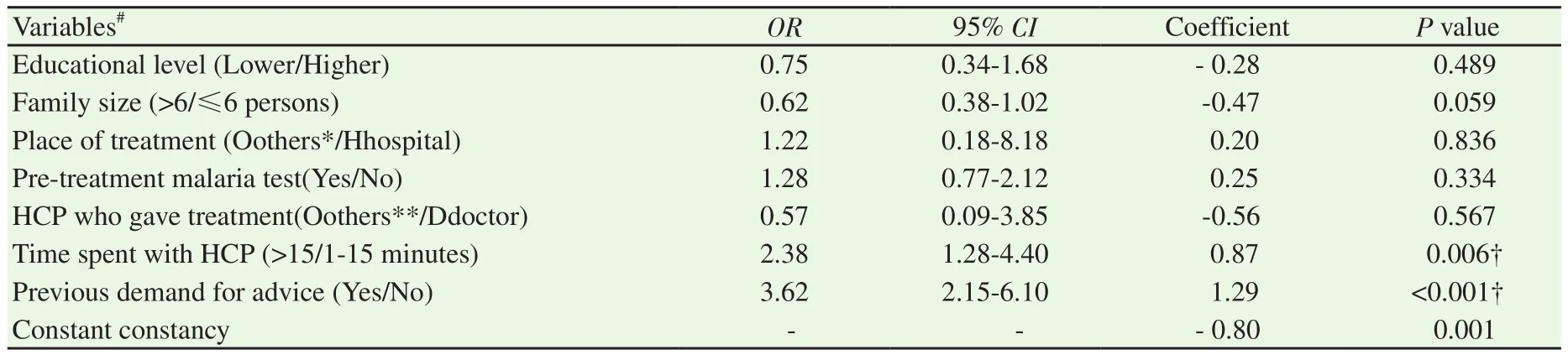
Table 4. Predictors of receiving malaria prevention counseling among respondents.
The reported low proportion of patients that received malaria prevention counseling presents a window of opportunity for offering malaria prevention counseling in the outpatient clinic. The time constraint observed in busy outpatient clinics suggest the need for different strategies to improve outpatient malaria care. This should include the use of social marketing (posters, and prerecorded televised information on malaria prevention) in the waiting area. If possible, trained counsellors could also be used for this aspect of care. Regular training and retraining of healthcare workers (including those who dispense antimalarials in the community) on malaria prevention practices and counseling skills is also required. The national guidelines for malaria treatment in endemic areas may need to clearly state the need for malaria prevention counseling during treatment of malaria (whether uncomplicated or severe forms).
Among the limitations of this study were that we could not eliminate recall bias. The estimation of time spent with healthcare provider by respondents was subjective and could have been spurious in some cases. Similarly, our finding is limited to urban and outpatient settings as there may be important differences in rural and inpatient settings. The absence of studies on this subject also made comparisons difficult. Despite these limitations, this study has highlighted a deficiency in outpatient care of malaria which if addressed can lead to reduction in the current malaria burden. This study also serves as a baseline for future multicenter, appropriately designed studies in this domain.
The proportion of respondents that received malaria prevention counseling was low. This presents an opportunity for reviewing policy towards improving the quality of outpatient malaria care. This may require using alternative strategies in giving malaria prevention information especially in busy clinics where consultation time is constrained. This can be an important step towards reducing malaria burden in this and similar settings.
Conflict of interest statement
The authors have declared that no competing interests exist.
Acknowledgement
The authors are grateful to the research assistants and staff of the Family Medicine and Paediatric departments of Aminu Kano Teaching Hospital, Kano for their contributions and support.
Authors' contributions
G.C.M. is the guarantor and was involved in study conception and design, data collection, analysis and interpretation, manuscript drafting and critical revision, and final approval of version to be published. B.A.G was involved in analysis and interpretation of data, critical revision for intellectual content and final approval of the version to be published. I.A. was involved in study design,manuscript drafting and critical revision, and final approval. M.B.U.was involved in data collection, critical revision and final approval.Z.A.U, was involved in data collection, critical revision and final approval.
 Asian Pacific Journal of Tropical Medicine2020年5期
Asian Pacific Journal of Tropical Medicine2020年5期
- Asian Pacific Journal of Tropical Medicine的其它文章
- Coronavirus disease 2019 (COVID-19) outbreak: Strengthening the treatment component in health care establishments to minimize case fatality
- Public health preparedness towards COVID-19 outbreak in Nigeria
- COVID-19 epidemic control approach in Italy
- Mathematical modelling of COVID-19 in South Africa
- Spatial distribution of cutaneous anthrax in western Iran from 2009 to 2016:Geographic information system mapping for predicting risk of anthrax outbreaks
- Lesson learned: Retrospective analysis of ‘missed out’ dengue NS1 positives among IgM negative population