
Clinical features and outcomes of diffuse large B-cell lymphoma based on nodal or extranodal primary sites of origin: Analysis of 1,085 WHO classified cases in a single institution in China
2019-03-16 03:24:20YuankaiShiYingHanJianliangYangPengLiuXiaohuiHeChanggongZhangShengyuZhouLiqiangZhouYanQinYongwenSongYuepingLiuShulianWangJingJinLinGuiYanSun
Yuankai Shi, Ying Han, Jianliang Yang, Peng Liu, Xiaohui He, Changgong Zhang, Shengyu Zhou,Liqiang Zhou, Yan Qin, Yongwen Song, Yueping Liu, Shulian Wang, Jing Jin, Lin Gui, Yan Sun
1Department of Medical Oncology, Beijing Key Laboratory of Clinical Study on Anticancer Molecular Targeted Drugs, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College,Beijing 100021, China; 2Departement of Radiation Oncology, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing 100021, China
Correspondence to: Yuankai Shi. Department of Medical Oncology, Beijing Key Laboratory of Clinical Study on Anticancer Molecular Targeted Drugs, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, No. 17 Panjiayuan Nanli, Chaoyang District, Beijing 100021, China. Email: syuankai@cicams.ac.cn.
Abstract Objective: To explore the clinicobiologic features and outcomes of diffuse large B-cell lymphoma (DLBCL)patients in China according to the primary site.Methods: A total of 1,085 patients diagnosed with DLBCL in National Cancer Center/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College during a 6-year period were enrolled. Their clinical characteristics and outcomes were analyzed according to the primary site.Results: In the 1,085 patients, 679 (62.6%) cases were nodal DLBCL (N-DLBCL) and 406 cases (37.4%) were extranodal DLBCL (EN-DLBCL). The most common sites of N-DLBCL were lymphonodus (64.8%), Waldeyer's ring (19.7%), mediastinum (12.8%) and spleen (2.7%), while in EN-DLBCL, stomach (22.4%), intestine (16.0%),nose and sinuses (8.9%), testis (8.4%), skin (7.9%), thyroid (6.9%), central nervous system (CNS) (6.4%), breast(5.7%), bone (3.4%), and salivary gland (2.7%) were most common. N-DLBCL patients tend to present B symptoms, bulky disease, and elevated LDH more often, while age >60 years, extranodal sites >1, Ann Arbor stage I or II, bone marrow involvement, and Ki-67 index >90% were usually seen in EN-DLBCL. The 5-year overall survival (OS) rate and progression-free survival (PFS) rate for all patients were 62.5% and 54.2%. The 5-year OS rate for patients with N-DLBCL and EN-DLBCL were 65.5% and 56.9% (P=0.008), and the 5-year PFS were 57.0% and 49.0% (P=0.020). Waldeyer's ring originated DLBCL possessed the highest 5-year OS rate (83.6%) and PFS rate (76.9%) in N-DLBCL. The top five EN-DLBCL subtypes with favorable prognosis were stomach,breast, nose and sinuses, lung, salivary gland, with 5-year OS rate: 70.3%, 69.6%, 69.4%, 66.7% and 63.6%,respectively. While CNS, testis, oral cavity and kidney originated EN-DLBCL faced miserable prognosis, with 5-year OS rate of 26.9%, 38.2%, and 42.9%.Conclusions: In our study, primary sites were associated with clinical characteristics and outcomes. Compared with EN-DLBCL, N-DLBCL had better prognosis.
Keywords: Diffuse large B-cell lymphoma (DLBCL); distribution; nodal; extranodal
Introduction
Based on studies published by the Surveillance,Epidemiology, and End Results (SEER) Program, the National Program of Cancer Registries, and the North American Association of Central Cancer Registries, non-Hodgkin lymphoma (NHL) is the seventh most commonly diagnosed malignancy worldwide (1). Geographically,NHL is more commonly diagnosed in developed areas,with the highest incidence rates in North America,Australia, and Europe, and the lowest rates in Asia and the Caribbean (2). With advances in biological and genetic research, as well as the availability of new diagnostic methods and therapies, the survival of NHL patients has recently increased. While the nationwide cancer incidence and mortality in 2014 collected by the National Central Cancer Registry of China (NCCRC) showed that lymphoma was not among the 10 most common cancers in China, lymphoma still ranked tenth among causes of death,with an estimated mortality rate of 3.47/100,000.Furthermore, lymphoma ranked as the ninth leading cause of cancer deaths in males (3).
NHL mostly arises in the lymph nodes and in other lymphoid tissues such as Waldeyer's ring, the thymus, and spleen, which are termed nodal NHLs (N-NHLs).However, approximately 25%-40% of NHLs arise in tissues other than the lymph node, and therefore are termed extranodal NHLs (EN-NHLs) (4,5). During the last two decades, the incidence of lymphomas has increased, with EN-NHLs increasing more rapidly compared to N-NHLs (2,6).
Diffuse large B-cell lymphoma (DLBCL) is the most common lymphoid neoplasm in adults, representing 30%to 40% of all diagnosed lymphoid neoplasm cases (1,2).While DLBCL is regarded as a disease of older adults, with a median presentation in the seventh decade of life,DLBCL can be diagnosed at any age (7). The median age of DLBCL Chinese patients is approximately 10 years younger than Japanese and American patients (8,9).Although DLBCL incidence increases with age, gender and race do not influence DLBCL diagnosis. Furthermore,DLBCL can manifest in nearly any organ. The diversity in the clinical features, morphology, and genetic and molecular presentations of DLBCL suggests that it is a heterogeneous group of aggressive B-cell lymphomas rather than a single clinicopathologic entity (10).
The primary site of DLBCL is important in determining the clinical features, treatment options, and outcomes of NHLs. The primary site of lymphoma, either the lymph node or different extranodal territories, has been suggested as a criterion that might separate two different groups of DLBCL, nodal and extranodal, with particular clinicobiological characteristics and different natural histories (4,5). Many studies on lymphoma incidence patterns or distributions have been reported worldwide.However, research on the clinicopathologic features and outcomes according to the anatomic distribution of DLBCL in Mainland China is still limited, and case numbers are also small. In the current study, we reviewed and analyzed 1,085 consecutive patients diagnosed with DLBCL according to World Health Organization (WHO)classification during an approximate 5-year period. The aims of this study were to evaluate the anatomic distribution, major clinical features, and outcomes of DLBCL patients according to the primary lymphoma sites and to compare our data with that reported in the literature.
Materials and metho ds
Patients and data collection
A total of 1,742 DLBCL patients were referred for an interdisciplinary evaluation, and their data were included in the institutional database of National Cancer Center/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College between June 2006 and December 2012. Patients who did not have complete clinical information or immunohistochemistry data, or who were lost to follow-up immediately after treatment were excluded from this study. After application of the exclusion criteria, 1,085 patients who were diagnosed with DLBCL according to the typical histological and immunophenotypic features based on the WHO classification of Tumors of Haematopoietic and Lymphoid Tissue (2008)were finally enrolled in our study (6). According to the 7th edition of the American Joint Committee on Cancer(AJCC) cancer stage manual, lymph nodes, Waldeyer's ring, thymus, and spleen are considered nodal or lymphatic sites; extranodal or extralymphatic sites include the bone marrow, gastrointestinal tract, skin, bone, central nervous system (CNS), lung, gonads, ocular adnexa (conjunctiva,lacrimal gland, and orbital soft tissue), liver, kidneys, and uterus (11). This study was approved by the Institutional Review Board of the National Cancer Center/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College.
Evaluation and treatment
Pretreatment evaluations included a careful physical examination, routine blood tests, and chemistry profile, the latter of which included lactate dehydrogenase (LDH)levels and serum β2-microglobulin, computed tomography(CT) scans of the neck, chest, abdomen, and pelvis or positron emission tomography (PET) scans, and bone marrow examination. All patients were staged according to the Ann Arbor staging system, immunohistochemically classified into germinal center B-cell-like (GCB) and non-GCB according to the Hans algorithm (12), and stratified according to the original international prognostic index(IPI) (13).
The entire group of patients received initial chemotherapy with radiotherapy (n=492, 45.3%) or chemotherapy alone (n=536, 49.4%), and 38 (3.5%)patients received surgery ± chemotherapy ± radiotherapy.Patients with N-DLBCL (n=679, 62.6%) received initial chemotherapy with radiotherapy (n=347, 51.1%) or chemotherapy alone (n=314, 46.2%). Patients with ENDLBCL (n=406, 37.4%) received initial chemotherapy with radiotherapy (n=145, 35.7%) or chemotherapy alone(n=222, 54.7%). Of the 617 (56.9%) patients who received chemotherapy with radiotherapy as first-line therapy.
Criteria for treatment outcomes
Primary endpoints of this study were overall survival (OS)and progression-free survival (PFS). OS was calculated from the start of the initial treatment until the time of death of any cause, or until the last follow-up time point.PFS was defined from the first day of treatment to the time of disease progression, recurrence, or death due to any cause.
Statistical analysis
The Student's t-test and Chi-square test were used to compare the clinicopathological characteristics of patients between two groups. Survival curves were estimated using the Kaplan-Meier method and compared with a log-rank test stratified according to the primary sites from which DLBCL arose. Unless otherwise stated, P<0.05 was considered statistically significant. The IBM SPSS Statistics(Version 19.0; IBM Corp., New York, USA) was used for data analysis.
Results
Patient characteristics
The demographic and baseline clinical characteristics of DLBCL patients are listed in Table 1. The median age of all patients was 57 (range, 7-85) years. DLBCL was most frequently diagnosed among people 55-64 years of age(Figure 1). A total of 679 (62.6%) patients with N-DLBCL and 406 (37.4%) patients with EN-DLBCL were compared in this study. The incidence of N-DLBCL was higher compared to EN-DLBCL. The median ages of patients with N-DLBCL and EN-DLBCL were 50 and 56 years,respectively. There were more men than women in this cohort, with a male-female (M/F) ratio of 1.27. Except for gender, Eastern Cooperative Oncology Group (ECOG)performance status (PS), pathological classification and IPI score, other clinical features were not comparable between N-DLBCL and EN-DLBCL patients. More N-DLBCL patients had B-cell symptoms, bulky disease, and elevated LDH levels compared to EN-DLBCL patients, while age>60 years, involvement of two or more extranodal sites,Ann Arbor stage I or II, bone marrow involvement, and Ki-67 index >90% were more common in EN-DLBCL patients compared to N-DLBCL patients.
Primary site distribution of DLBCL
In this study, EN-DLBCL was defined as DLBCL arising primarily from sites other than the lymphonodus,Waldeyer's ring, spleen, or mediastinum (lymphonodus and thymus). Approximately 62.6% of all DLBCL were detected in nodal sites at diagnosis. Figure 2A shows the anatomical sites involving N-DLBCL. The most common primary site of N-DLBCL was the lymphonodus (440,64.8%), followed by Waldeyer's ring (134, 19.7%),mediastinum (87, 12.8%) and spleen (18, 2.7%). Primary sites of EN-DLBCL are shown in Figure 2B; the top ten primary sites were as follows: stomach (91, 22.4%),intestine (65, 16.0%), nose and sinuses (included nasal cavity and paranasal sinuses) (36, 8.9%), testis (34, 8.4%),skin (32, 7.9%), thyroid (28, 6.9%), CNS (26, 6.4%), breast(23, 5.7%), bone (14, 3.4%), salivary gland (11, 2.7%), and ovary and cervix (11, 2.7%).
Clinical outcomes
The median follow-up time was 57 (range, 1-146) months in this study. The 5-year OS and PFS rates for the entiregroup were 62.5% and 54.2%, respectively. The 5-year OS rates for patients with N-DLBCL and EN-DLBCL were 65.5% and 56.9%, respectively (P=0.008) (Figure 3A), and the 5-year PFS were 57.0% and 49.0%, respectively(P=0.020) (Figure 3B).
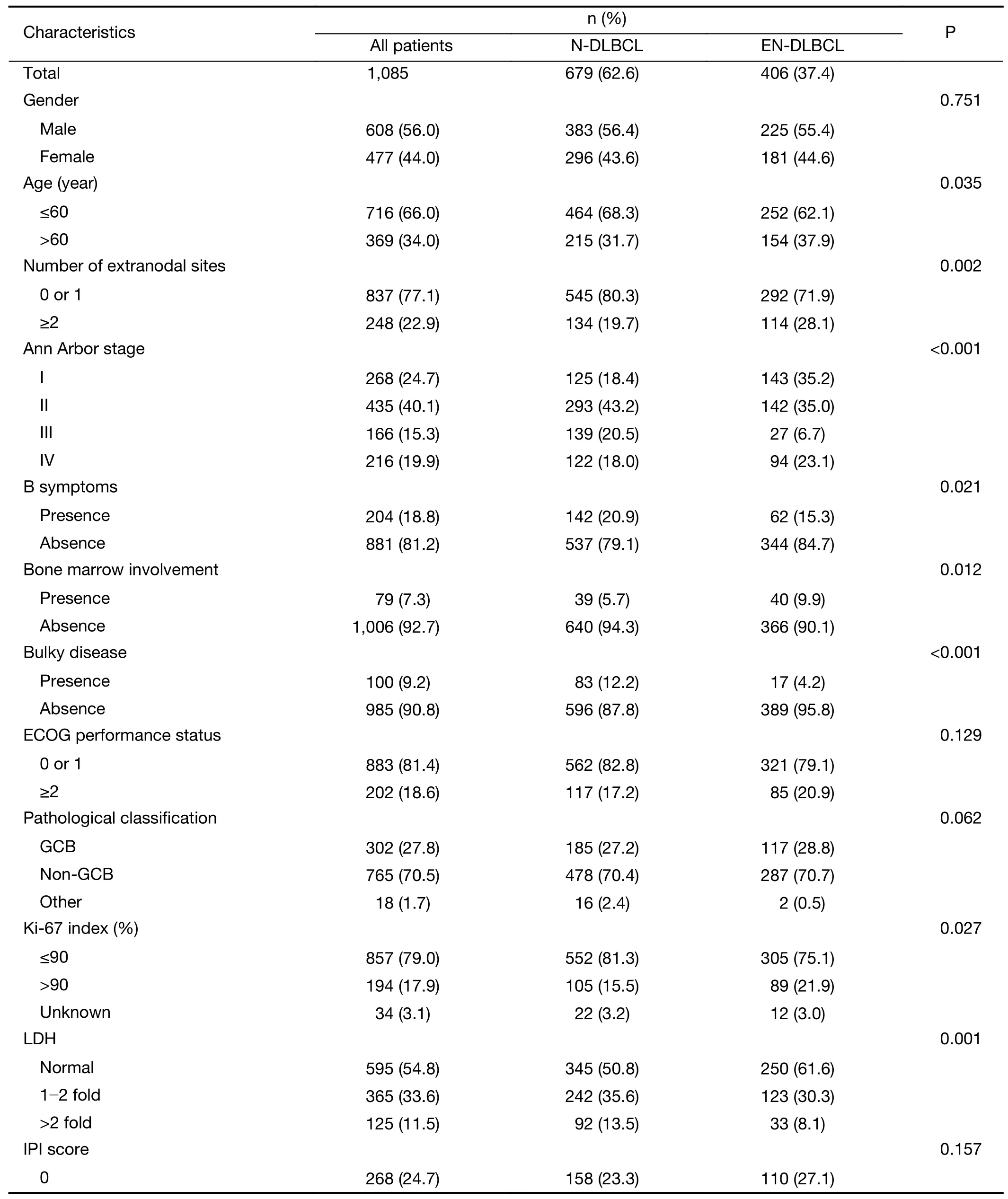
Table 1 Demographic and baseline clinical characteristics of patients with N-DLBCL and EN-DLBCL

Table 1 (continued)
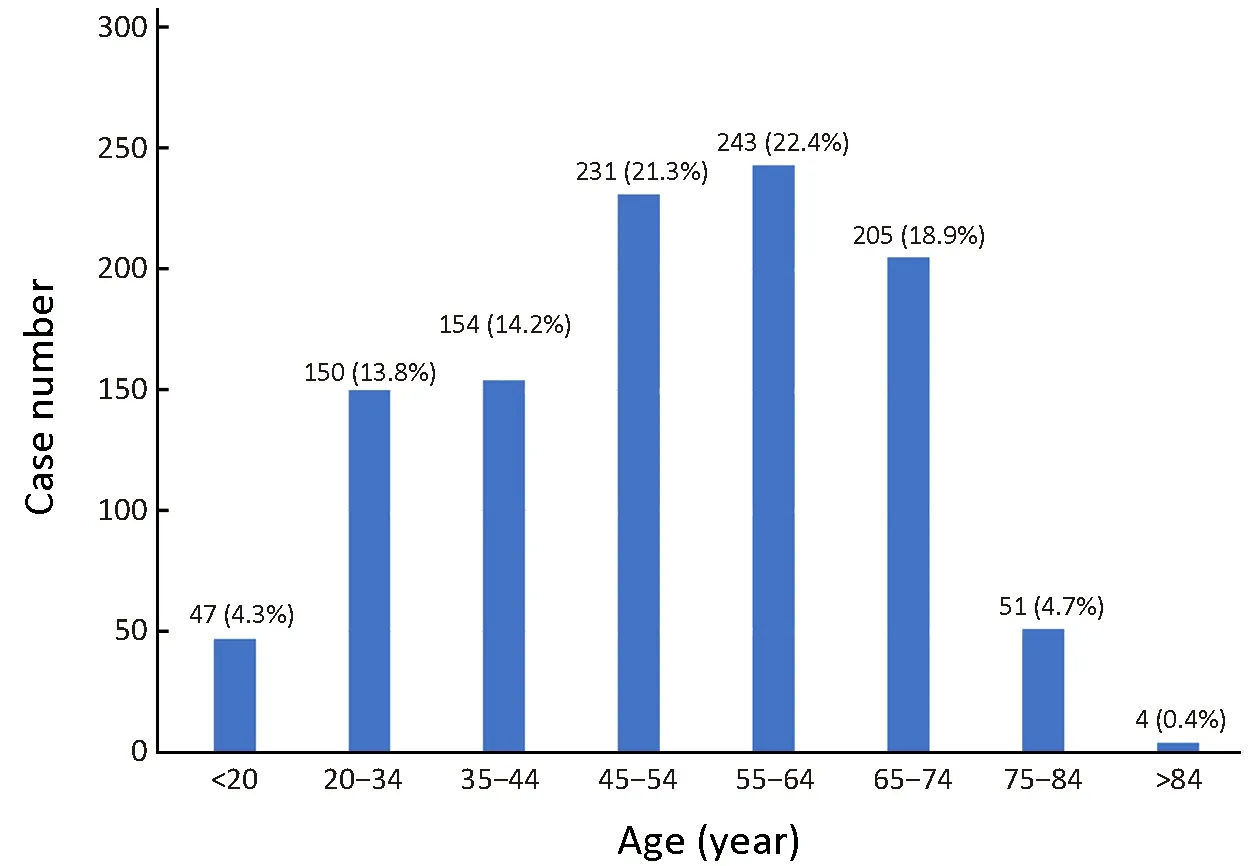
Figure 1 Proportion of diffuse large B-cell lymphoma by age.
An exploratory analysis was conducted to evaluate the impact of anatomic sites on OS and PFS in DLBCL. For N-DLBCL patients, DLBCL originating in Waldeyer's ring resulted in higher 5-year OS rates (83.6% vs. 72.2%,65.5% and 59.8%, P<0.001) (Figure 4A) and PFS rates(76.9% vs. 61.1%, 60.9% and 50.0%, P<0.001) compared to the spleen, mediastinum, and lymphonodus (Figure 4B).For EN-DLBCL patients, there were significant differences in OS (P=0.025) and PFS (P=0.030) in the different anatomic sites (Figure 5). The top five anatomic sites that had a good 5-year OS were: stomach (70.3%),breast (69.6%), nose and sinuses (69.4%), lung (66.7%),and salivary gland (63.6%). The top five anatomic sites that had a good 5-year PFS were: stomach (64.8%), salivary gland (63.6%), nose and sinuses (58.3%), thyroid (53.6%),and breast (52.2%). The top three anatomic sites that had a poor 5-year OS were: CNS (26.9%), testis (38.2%), oral cavity (42.9%) and kidney (42.9%). The top three anatomic sites that had a poor 5-year PFS were: CNS (15.4%), lung(33.3%), and testis (35.3%). All data are shown in Table 2.
Discussion
To the best of our knowledge, this retrospective study is the largest comprehensive descriptive research analysis of clinical outcomes based on the anatomic distribution of DLBCL according to the WHO classification of Tumors of Haematopoietic and Lymphoid Tissue (2008) conduced in a single institution in China.

Figure 2 Distribution of primary sites in nodal diffuse large B-cell lymphoma (N-DLBCL) (A) and extranodal diffuse large B-cell lymphoma (EN-DLBCL) (B). CNS, central nervous system.
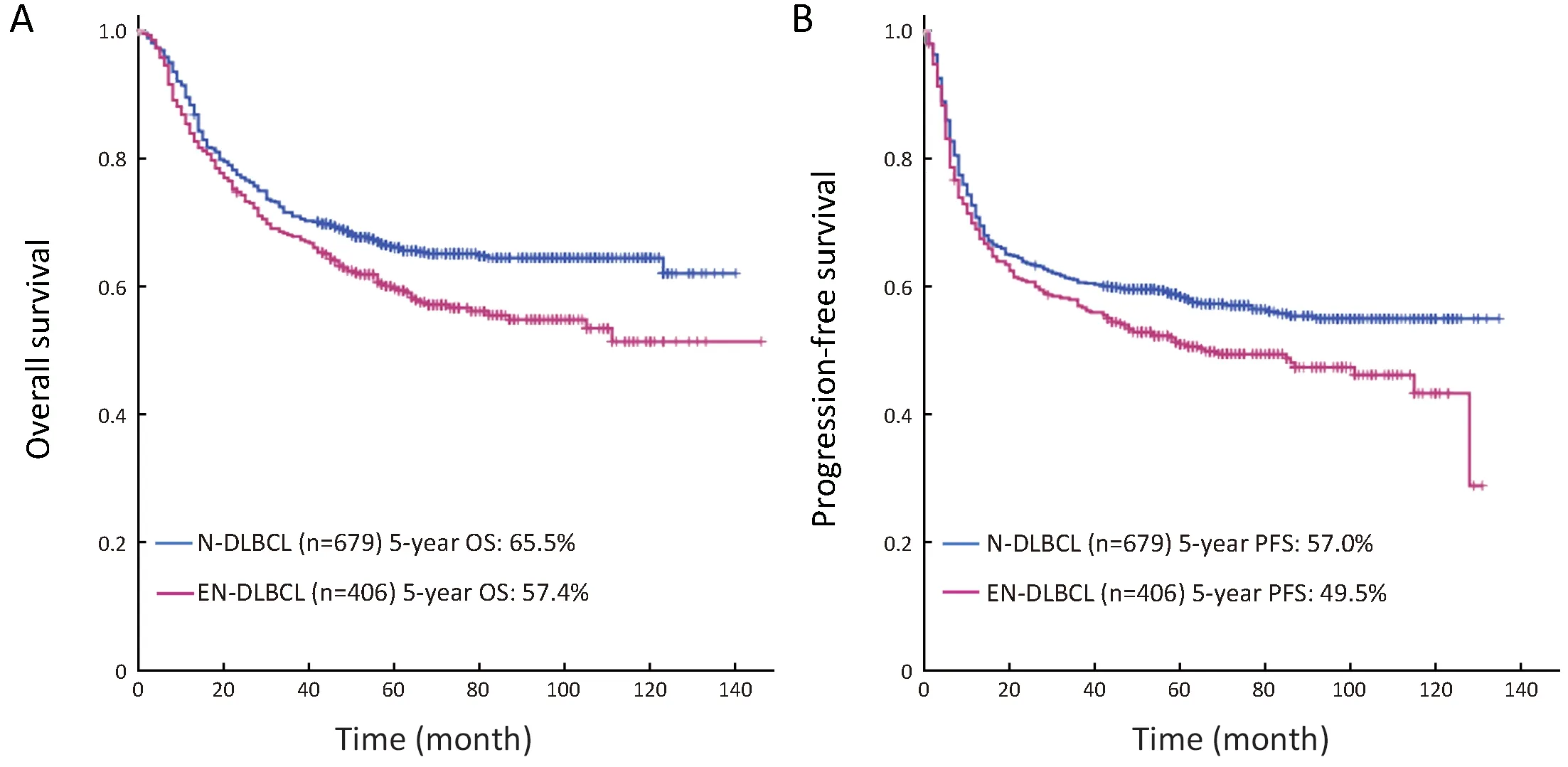
Figure 3 Overall survival (OS) (A) and progression-free survival (PFS) (B) for patients with nodal diffuse large B-cell lymphoma (NDLBCL) and extranodal diffuse large B-cell lymphoma (EN-DLBCL). (A) P=0.008; (B) P=0.020.
DLBCLs have various clinical presentations and responses to therapy, and the site of origin of the lymphoid tissue is an important determinant of lymphocyte migration patterns. In this study, lymphomas arising in nodal and extranodal sites showed different clinical features at diagnosis. Most DLBCL patients in our study were adults,which was in line with that reported in the literature for Chinese studies. For example, a study including 4,638 cases of lymphoid neoplasm in China performed by Sun et al.showed that the mean age was 51.6 years (14). However, we noted that the mean age of Chinese DLBCL patients was much lower than that reported in Japan (8). In the present study, the EN-DLBCL group included more patients who were >60 of age compared to the N-DLBCL group (37.9%vs. 31.7%, P=0.035). In agreement with previous studies(8,9,14), gender distribution in the whole DLBCL cohort in our study showed a male predominance, with an average M/F ratio of 1.27. Also, more patients had stage III-IV disease in the N-DLBCL group compared to the ENDLBCL group (38.5% vs. 29.8%), which could possibly be attributed to the fact that EN-DLBCL patients are likely to present earlier with local symptoms due to noticeable tumor mass in extranodal sites. However, more N-DLBCL patients had a bulky disease compared to EN-DLBCL patients (12.2% vs. 4.2%, P<0.001), which was likely due to the involvement of N-DLBCL in the primary mediastinal(thymic) large B-cell lymphoma, which typically accompanies bulky disease (15). We also found that 48.4%of N-DLBCL patients had serum LDH levels above the normal range before treatment, which were higher compared to the EN-DLBCL group (49.2% vs. 38.4%,P=0.001). With regard to the clinical outcomes, the elevated serum LDH levels were generally associated with unfavorable outcomes, such as poor treatment responses and low survival rates regardless of IPI scores; thus, LDH levels may represent tumor growth and invasive potential in neoplastic diseases (16). In the present study, the finding that the N-DLBCL group had more patients at stage III or IV and/or bulky disease may be related to the high incidence rates of elevated serum LDH levels in this group.

Figure 4 Overall survival (OS) (A) and progression-free survival (PFS) (B) for patients with nodal diffuse large B-cell lymphoma (NDLBCL) according to the primary site of the lymphoma. (A) P<0.001; (B) P<0.001.
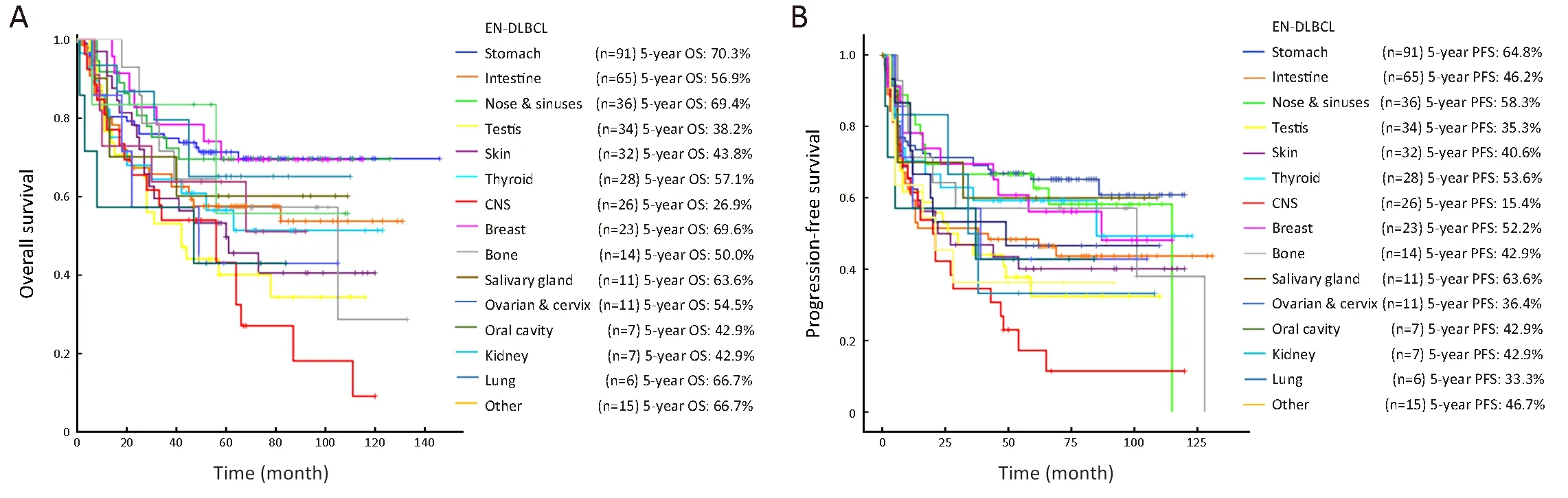
Figure 5 Overall survival (OS) (A) and progression-free survival (PFS) (B) for patients with extranodal diffuse large B-cell lymphoma (ENDLBCL) according to the primary site of the lymphoma. (A) P=0.025; (B) P=0.030. CNS, central nervous system.
Ki-67, a surrogate marker of proliferation, has been investigated in various neoplasms and found to be a powerful prognostic factor for survival outcomes (17). It has been reported that DLBCL patients with high Ki-67 expression received limited survival benefits from RCHOP therapy (18). In our study, more patients with high Ki-67 expression (>90%) were identified in the ENDLBCL group compared to the N-DLBCL group (21.9%vs. 15.5%, P=0.027). Previous literature reported that the majority of primary CNS lymphomas exhibit markedly increased proliferative activity, with more than 90% of cells expressing the Ki-67 antigen (19), and primary testicular lymphoma also had significantly increased proliferative capacity, with Ki-67 expression in the 70% to 90% (20).According to the 7th edition of the AJCC cancer stage manual, EN-DLBCL includes primary CNS DLBLC and primary testicular DLBLC, which may explain the high number of EN-DLBCL patients with elevated Ki-67 expression in our study.
Studies from Western countries have reported theoccurrence of EN-NHL to be 25%-40% of all NHL(4,5,21). In accordance with those reports, our study found a similar rate (37.4%) of EN-DLBCL. The fluctuating frequency of EN-NHL may be caused by genetic and ethnic factors, as well as diverse definition criteria. The consideration of particular territories as nodal or extranodal is a controversial issue, such as Waldeyer's ring. In general,Waldeyer's ring, in which the lymphoid tissue is similar to that of the lymph node, is included in the nodal areas according to the 7th edition of the AJCC cancer staging manual (11). The above issues could explain the disparate results obtained in our study from those of previous studies in China (9,14). The gastrointestinal (GI) tract is one of the most common anatomic sites of EN-NHL involvement,accounting for 30%-50% of all NHL (8,9,22). In the present study, approximately one quarter of patients had stomach involvement. There is compelling evidence that EN-NHLs at some sites have site-specific causes, such as Helicobacter pylori (Hp) in gastric lymphomas (23). The high rate of stomach involvement in our study was likely due to the high prevalence of Hp infections in China. The second most common anatomic site of EN-DLBCL was the intestine (16.0%), and the third was the nasal cavity/sinus (8.9%). This trend was similar to that reported in the literature in China. For example, a study including 6,328 cases of lymphoid neoplasm in China performed by Yang et al. showed the most common anatomic sites in the same order (9).
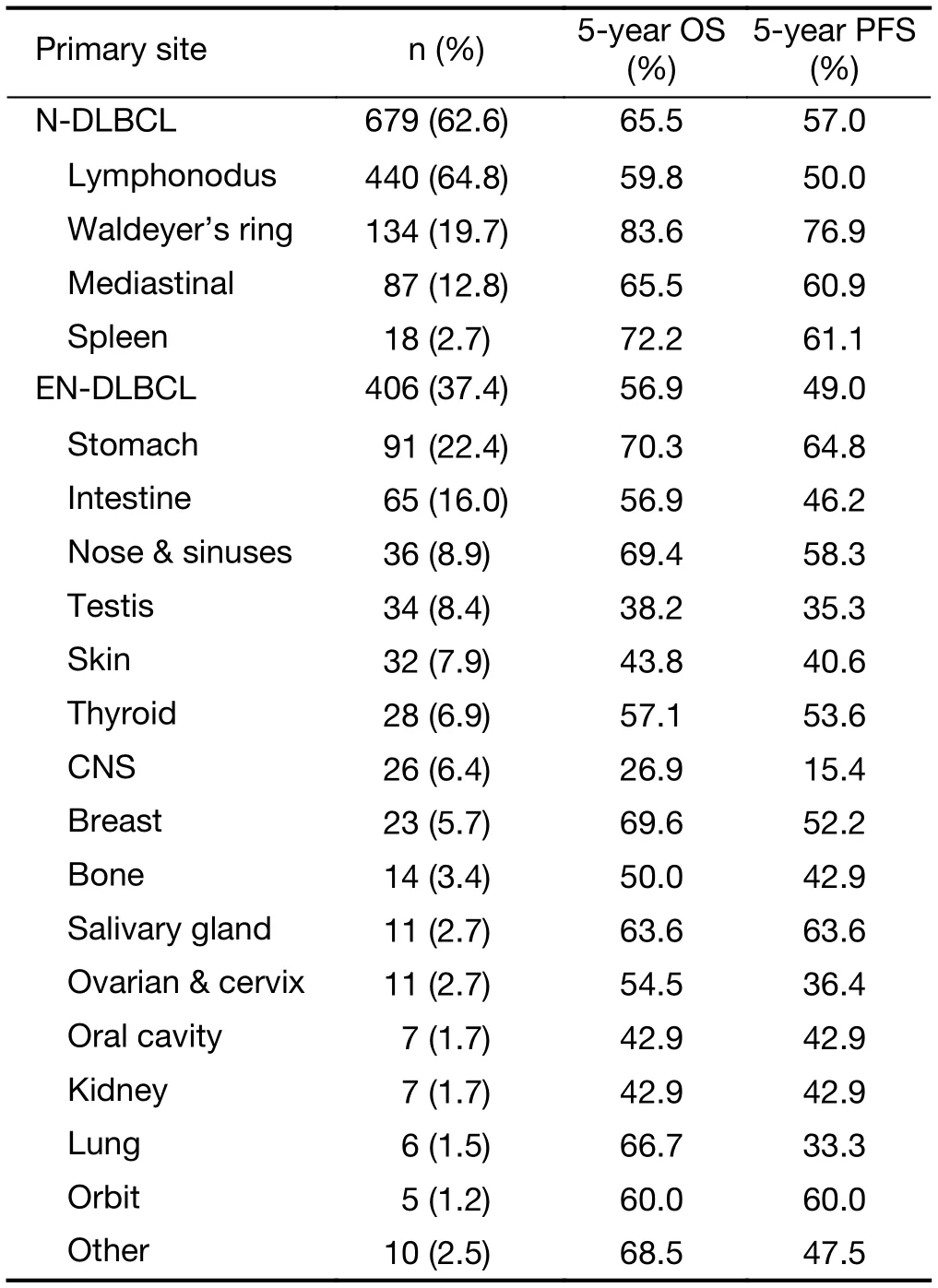
Table 2 OS and PFS of 1,085 patients with DLBCL according to primary sites of lymphoma
In this study, the 5-year OS among all patients was 62.5%, and the 5-year PFS was 54.2%. Since the last review of NHL in the Lancet in 2012 (24), advances in understanding the biology and genetics and the availability of new diagnostic methods and therapies have improved.These findings are comparable to those obtained from the international statistics, the 5-year relative survival rate was reported as 56.1% in EUROCARE west, 47.1% in EUROCARE east, and 56.3% in SEER (25). In agreement with previous studies (25), primary Waldeyer's ring DLBCL showed a notably better outcome than the other anatomic sites in N-DLBCL. The GI tract is one of the most common extranodal sites of lymphoma (9,14,26,27).According to research on GI lymphoma, primary gastric DLBCL (PG-DLBCL) and primary intestinal DLBCL(PI-DLBCL) had different clinical characteristics and treatment outcomes (28-30). In our study, we separated PG-DLBCL from PI-DLBCL for statistical analysis. The PG-DLBCL group showed a remarkably good OS (70.3%)and PFS (64.8%) compared to other extranodal sites, but the PI-DLBCL group did not match these outcomes.Primary CNS lymphoma (PCNSL) is a rare and highly aggressive lymphoma that arises in the intracerebral or intraocular spaces without systemic involvement. In agreement with previous studies (31), we found that PCNSL had a worse prognosis than systemic DLBCL in any setting analyzed.
Conclusions
In the present study, we demonstrated that the primary sites of DLBCL are associated with particular clinicopathologic features and outcomes. N-DLBCL patients have better treatment outcomes compared to ENDLBCL. These results highlight the heterogeneity of DLBCL, and optimal treatment modalities should be selected according to the primary sites.
Acknowledgements
This study was primary funded by grants from the National Science and Technology Support Program (No.2014BAI09B12) and Chinese Academy of Medical Sciences(CAMS) Innovation Fund for Medical Sciences (CIFMS)(No. 2016-I2M-1-001).
Footnote
Conflicts of Interest: The authors have no conflicts of interest to declare.
1.Siegel RL, Miller KD, Jemal A. Cancer statistics,2017. CA Cancer J Clin 2017;67:7-30.
2.Armitage JO, Gascoyne RD, Lunning MA, et al.Non-Hodgkin lymphoma. Lancet 2017;390:298-310.
3.Chen W, Sun K, Zheng R, et al. Cancer incidence and mortality in China, 2014. Chin J Cancer Res 2018;30:1-12.
4.Zucca E, Roggero E, Bertoni F, et al. Primary extranodal non-Hodgkin's lymphomas. Part 1:Gastrointestinal, cutaneous and genitourinary lymphomas. Ann Oncol 1997;8:727-37.
5.Zucca E, Roggero E, Bertoni F, et al. Primary extranodal non-Hodgkin's lymphomas. Part 2: Head and neck, central nervous system and other less common sites. Ann Oncol 1999;10:1023-33.
6.Swerdlow SH, Campo E, Harris NL, et al. WHO Classification of Tumors of Haematopoietic and Lymphoid Tissues (4th edition). Lyon: IARC Press,2008.
7.Rosenwald A, Wright G, Chan WC, et al. The use of molecular profiling to predict survival after chemotherapy for diffuse large-B-cell lymphoma. N Engl J Med 2002;346:1937-47.
8.Aoki R, Karube K, Sugita Y, et al. Distribution of malignant lymphoma in Japan: analysis of 2260 cases,2001-2006. Pathol Int 2008;58:174-82.
9.Yang QP, Zhang WY, Yu JB, et al. Subtype distribution of lymphoma in Southwest China:analysis of 6,382 cases using WHO classification in a single institution. Diagn Pathol 2011;6:77.
10.Schmitz R, Wright GW, Huang DW, et al. Genetics and pathogenesis of diffuse large b-cell lymphoma. N
ReferencesEngl J Med 2018;378:1396-407.
11.Edge SB, Byrd DR, Compton CC, et al. AJCC Cancer Staging Manual. 7th Edition. New York:Springer, 2010.
12.Hans CP, Weisenburger DD, Greiner TC, et al.Confirmation of the molecular classification of diffuse large B-cell lymphoma by immunohistochemistry of diffuse using a tissue microarray. Blood 2004;103:275-82.
13.International Non-Hodgkin's Lymphoma Prognostic Factors Project. A predictive model for aggressive non-Hodgkin's lymphoma. N Engl J Med 1993;329:987-94.
14.Sun J, Yang Q, Lu Z, et al. Distribution of lymphoid neoplasms in China: analysis of 4,638 cases according to the World Health Organization classification. Am J Clin Pathol 2012;138:429-34.
15.Swerdlow SH, Campo E, Pileri SA, et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood 2016;127:2375-90.
16.Yao S, Li J, Yao Z, et al. Extranodal involvement in young patients with diffuse large B-cell lymphoma:distribution, prognostic value and treatment options.Chin J Cancer Res 2017;29:57-65.
17.Urruticoechea A, Smith IE, Dowsett M. Proliferation marker Ki-67 in early breat cancer. J Clin Oncol 2005;23:7212-20.
18.Li ZM, Huang JJ, Xia Y, et al. High Ki-67 expression in diffuse large B-cell lymphoma patients with nongerminal center subtype indicates limited survival benefit from R-CHOP therapy. Eur J Haematol 2012;88:510-7.
19.Abrey LE, Batchelor TT, Ferreri AJ, et al. Report of an international workshop to standardize baseline evaluation and response criteria for primary CNS lymphoma. J Clin Oncol 2005;23:5034-43.
20.AI-Abbadi MA, Hattab EM, Tarawneh MS, et al.Primary testicular diffuse large B-cell lymphoma belongs to the nongerminal center B-cell-like subgroup: A study of 18 cases. Mod Pathol 2006;19:1521-7.
21.Krol AD, le Cessie S, Snijder S, et al. Primary extranodal non-Hodgkin's lymphoma (NHL): the impact of alternative definitions tested in the Comprehensive Cancer Centre West population-based NHL registry. Ann Oncol 2003;14:131-9.
22.Warrick J, Luo J, Robirds D, et al. Gastrointestinal lymphomas in a North American population:clinicopathologic features from one major Central-Midwestern United States tertiary care medical center. Diagn Pathol 2012;7:76.
23.Govi S, Patti C, Raderer M, et al. Final results of a multicenter phase II trial assessing the activity and efficacy of Helicobacter pylori-eradicating antibiotic therapy as exclusive treatment for patients with stage I-III diffuse large B-cell lymphoma of the stomach(the HGL-1 trial). Blood 2011;118:958.
24.Shankland KR, Armitage JO, Hancock BW. Non-Hodgkin lymphoma. Lancet 2012;380:848-75.
25.Sant M, Allemani C, De Angelis R, et al. Influence of morphology on survival for non-Hodgkin's lymphoma in Europe and the United States. Eur J Cancer 2008;44:579-87.
26.Warrick J, Luo J, Robirds D, et al. Gastrointestinal lymphomas in a North American population:clinicopathologic features from one major Central-Midwestern United States tertiary care medical center. Diagn Pathol 2012;7:76.
27.Ghimire P, Wu GY, Zhu L. Primary gastrointestinal lymphoma. World J Gastroenterol 2011;17:697-707.
28.Li X, Xia B, Guo S, et al. A retrospective analysis of primary gastric diffuse large B-cell lymphoma with or without concomitant mucosa-associated lymphoid tissue (MALT) lymphoma components. Ann Hematol 2013;92:807-15.
29.Wu YX, Liu B, Chen L, et al. Prognostic factors of primary gastric diffuse large B-cell lymphoma:a retrospective study of 75 cases in China. Ann Hematol 2013;92:861-2.
30.Kim SJ, Kang HJ, Kim JS, et al. Comparison of treatment strategies for patients with intestinal diffuse large B-cell lymphoma: surgical resection followed by chemotherapy versus chemotherapy alone. Blood 2011;117:1958-65.
31.Yamanaka R, Homma J, Sano M, et al. Immunochemotherapy with a combination of rituximab,methotrexate, pirarubicin and procarbazine for patients with primary CNS lymphoma -a preliminary report. Leuk lymphoma 2007;48:1019-22.
 Chinese Journal of Cancer Research2019年1期
Chinese Journal of Cancer Research2019年1期
- Chinese Journal of Cancer Research的其它文章
- STIM1 expression is associated with osteosarcoma cell survival
- Prognostic implications of epidermal growth factor receptor variant III expression and nuclear translocation in Chinese human gliomas
- Risk-stratification model to select conversion surgery for advanced gastric cancer patients
- Metastatic patterns and surgical methods for lymph nodes No. 5 and No. 6 in proximal gastric cancer
- Prognostic value of 18F-fluorodeoxyglucose positron emission tomography using Deauville criteria in diffuse large B cell lymphoma treated with autologous hematopoietic stem cell transplantation
- Incidence and mortality of thyroid cancer in China, 2008-2012