
A newly designed silicone tube for the treatment of canalicular laceration
2019-01-05 01:42:26
國際眼科雜志 2019年1期
Department of Ophthalmology, The Second People’s Hospital of Jinan City, Jinan 250001, Shandong Province, China
Abstract
?AIM: To evaluate the clinical efficacy of a newly designed silicone tube for the repair of canalicular lacerations.
?METHODS: This was a prospective clinical study. Data were analyzed from 47 eyes of 47 patients presenting with traumatic canalicular laceration in our hospital from January 2013 to October 2015. The newly designed silicone tubes were inserted through the lacrimal punctum and left in the bicanaliculi for 3mo. Data of the lacrimal duct patency, epiphora, and eyelid shape were recorded.
?RESULTS: Surgery was performed successfully in all cases. No complications associated with the silicone tubes occurred. In total, 41 patients (87.23%) achieved complete success, 4 patients (8.51%) achieved partial success, and 2 patients (4.26%) had surgical failure.
?CONCLUSION: The newly designed silicone tube is an effective and atraumatic tool for the management of canalicular lacerations. The operation process is simple, and is easy to grasp for the surgeon.
?KEYWORDS: canalicular laceration; silicone tube; bicanalicular intubation
INTRODUCTION
Canalicular laceration is a common type of trauma occurring in the lacrimal drainage system. If not treated in a timely manner, patients can develop epiphora that subsequently affects their activities of daily living as well as their physical and mental health. Lacrimal mucosal anastomosis and placement of a well-tolerated stent is a basic method for treatment of canalicular lacerations[1-2]. An epidural anesthetic tube is widely used in China because it is inexpensive and easy to obtain. However, it is hard and not easy to bend, and has other disadvantages including cosmetic problems, canalicular slitting, and ectropion of the eyelid. Accordingly, less invasive silicone tubes have been recently proposed as an alternative treatment. At present, there are various types of silicone tubes, but some implantation methods are cumbersome. Therefore, we have selected a novel silicone tube with easy use for the treatment of canalicular lacerations.
The aim of this study was to evaluate the effectiveness of a new type of silicone tube for the treatment of canalicular lacerations.
SUBJECTS AND METHODS
PatientsForty-seven eyes of 47 patients with canalicular laceration were included in this prospective clinical trial from January 2013 to October 2015 at a Hospital in Jinan City (Jinan, China). Diagnosis of the canalicular laceration was based on an ophthalmological examination and lacrimal irrigation.
All patients were informed about the purpose of the study, and provided their informed written consent before surgery in accordance with the Declaration of Helsinki. In addition, institutional review board approval (2013002) was obtained from the Medical Ethics Committee of the hospital.
SurgicalProceduresThe newly designed silicone stent (Jinan Chensheng Medical Silicone Rubber Product Co., Ltd) consisted of a silicone tube and a malleable stainless steel stylet (Figure 1).
The stylet was inserted into the lumen of the tube to increase its rigidity and the diameter of the stylet is 0.42 mm outer diameter. The diameter of both ends of the tube is 1.1 mm outer diameter and 0.6 mm inner diameter and the diameter of the middle part is 0.5 mm. The blue dot in the middle indicated the position of insertion into the lacrimal system.
The same surgeon completed surgery in all patients. All surgeries were performed under general anesthesia or local anesthesia (2% lidocaine with 1∶100 000 epinephrine), depending on the patient’s age and general condition.
The first step involved in surgical reconstruction is identification of the lacerated edges of the canaliculus. The nasal ends of the injured canaliculi were identified under an operating microscope. Saline was injected using a Healon needle to confirm the finding under local anesthesia. In three cases, it was difficult to locate the nasal end of the laceration, and saline was injected through the intact opposite punctum by using a Healon needle. In one case in which the above two methods had failed and we could not detect where the broken ends were, a pigtail probe was used.
The second step involved is implantation of the silicone tube. Both ends of the silicone tube were applied evenly using Tobramycin Dexamethasone Ophthalmic Ointment. The lacrimal punctum was dilated using a punctal dilator. One end of the silicone tube was inserted into the inferior aspect of the lacrimal system and the blue dot was placed near the lacrimal punctum. The stylet was then removed. After this, the other end was inserted into the superior aspect of the lacrimal system and the stylet was also removed. For the injured canaliculae, the end was inserted into the lacrimal punctum and pushed into the canaliculus until it came out, and was then inserted into the nasal end of the injured canaliculus, until it passed to the lacrimalsac and nasolacrimal duct.
The last step of the procedure involved suturing. Using 6-0 absorbable suture, the peritubular tissue around the broken ends of the ruptured canaliculus was sutured using the horizontal mattress technique. The muscle was then sutured followed by the skin, with interrupted sutures while maintaining the eyelid contour (Figure 2). The length between the upper and lower punctum was adjusted.
Postoperatively, all patients were treated with topical antibiotics and lubricants to prevent infection and they were asked not to rub their eyelid to prevent premature protrusion of the tube.
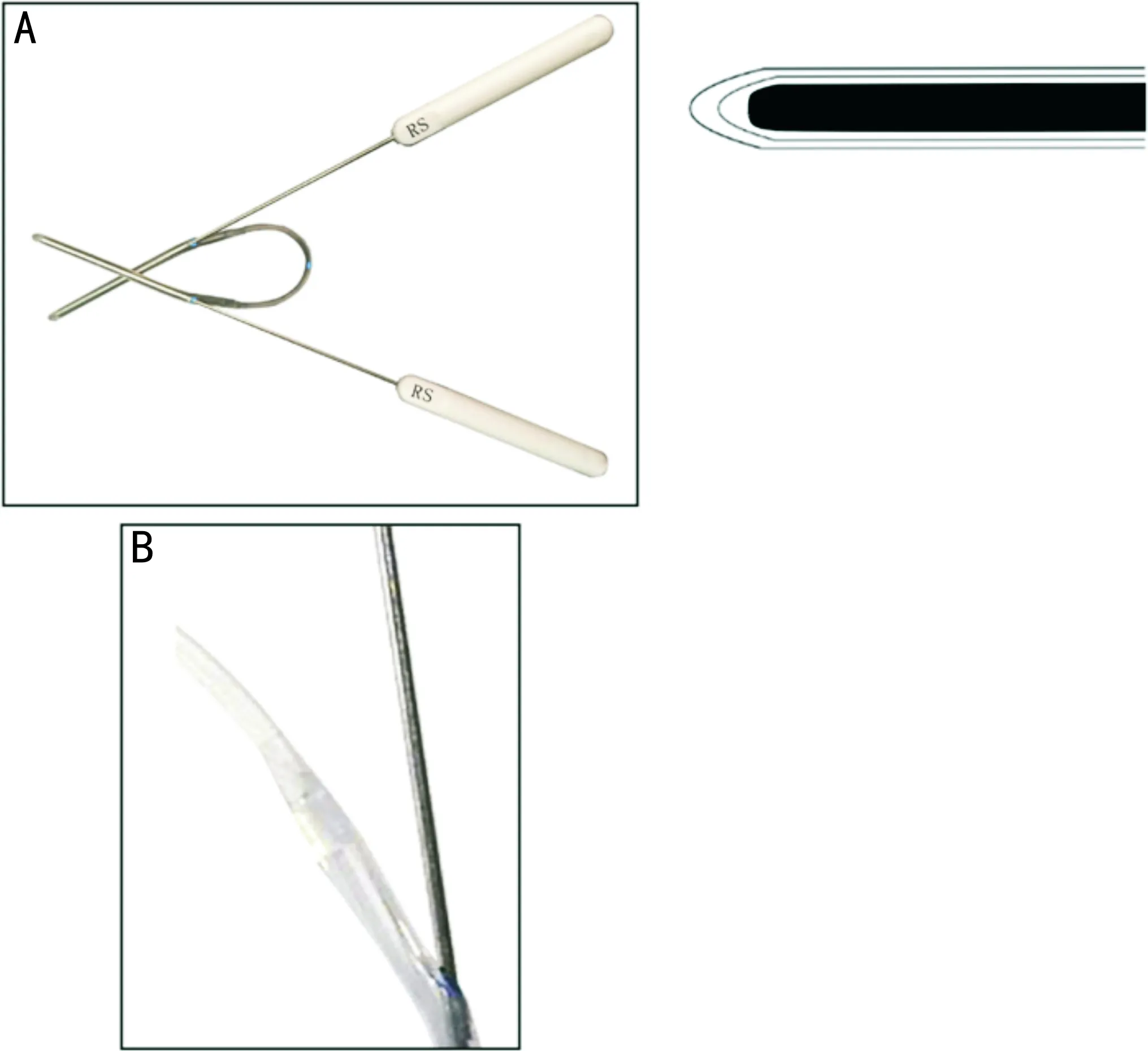
Figure1ThedisposablelacrimaldrainagetubeA:The newly designed silicone stent consists of a silicone tube and a malleable stainless steel stylet. The stylet was inserted into the lumen of the tube to increase its rigidity. The blue dot in the middle indicates the position of insertion into the lacrimal system; B: Local details of the tube. Smooth transition of the coarse and the fine. The front ends of the tube are in an arc shape.
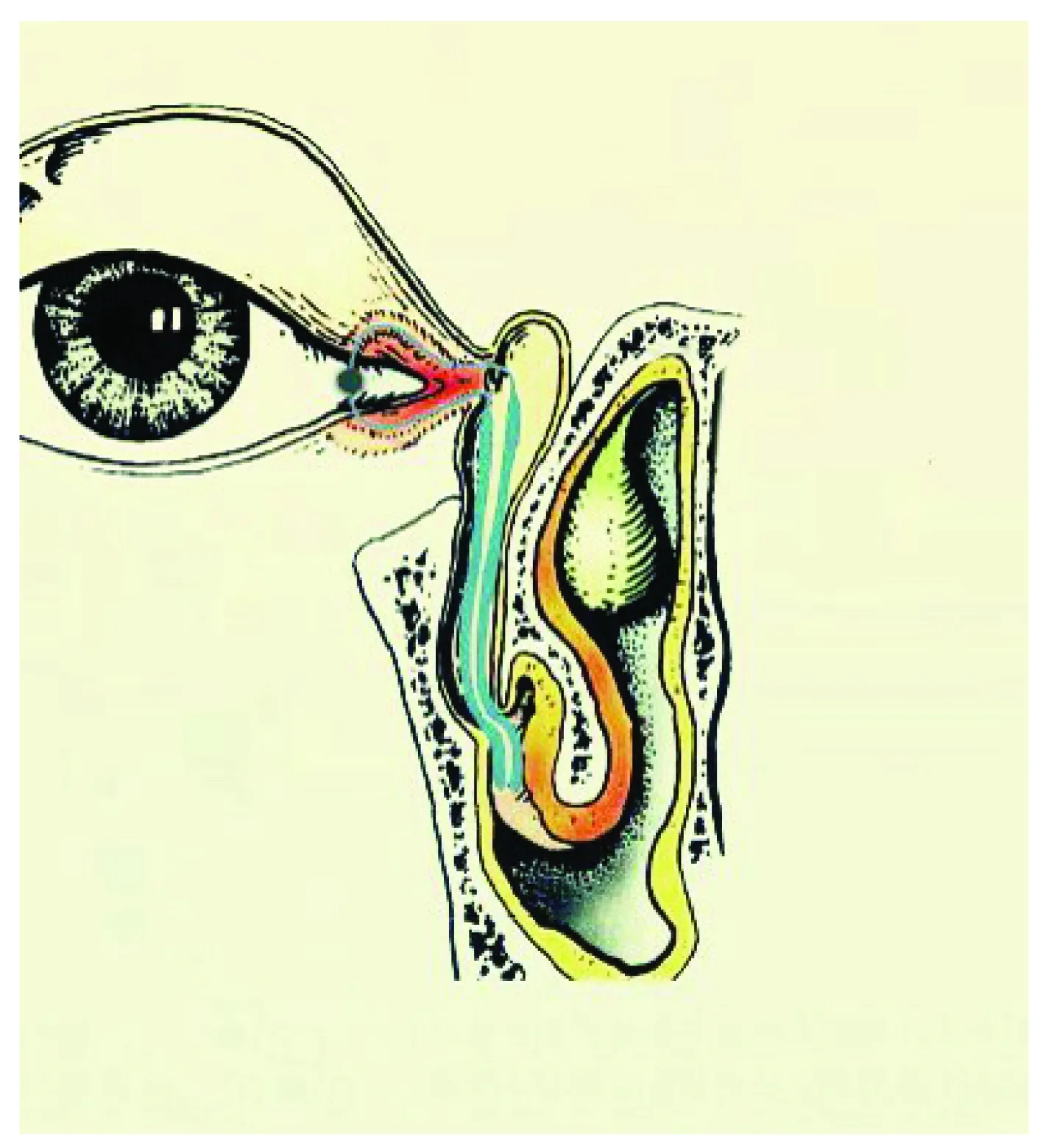
Figure2Schematicdiagramofthesiliconetubeimplantedinlacrimalsystem.
RemovaloftheSiliconeTubeThree months after the operation, the tube was removed. A drop of topical ophthalmic anesthetic (0.5% proparacaine hydrochloride eye drops, the Second People’s Hospital of Jinan City, China) was instilled into the conjunctival sac. The tube loop was pulled out from the medial canthus. Irrigation (with an antibiotic solution) was administered to the patients immediately after the tube was removed to clear any discharge in the lacrimal passage.
PostoperativeFollow-upThe postoperative follow-up schedule was generally at 1wk and 1, 3, 4, 6, 9mo, and every 3mo thereafter following the operation. We observed the following: epiphora, eyelid shape, lacrimal puncta and any related adverse reactions.
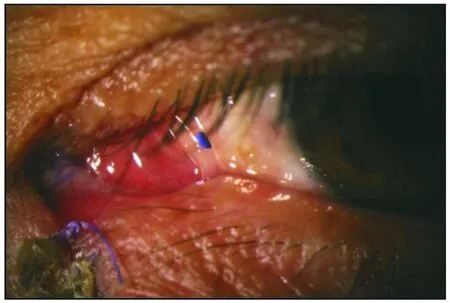
Figure3PostoperativeappearanceofthetubeinthelacrimalsystemSlitlampphotographofapatientaftertheoperationshowingthataloopoftubingisleftvisibleandextendsbetweentheinferiorandsuperiorpuncta.Lacrimalpunctumisinitsnormalpositionandhasgoodcontactwiththelacrimallacus.
RESULTS
Of the 47 patients, 40 were males and 7 were females. The mean age was 41.3±10.7 (range 2-60) years. Among the patients, 39 (82.98%) had isolated lower canalicular lacerations, 5 (10.64%) had isolated upper canalicular lacerations and 3 (6.38%) had bicanalicular lacerations. The causes of injury included: blunt injury (19 cases), traffic accident injury (5 cases) and sharp-object injury (23 cases).
The mean duration from canalicular injury to surgical reconstruction was 8 (range: 2-24)h. All the tubes were successfully implanted in all eyes without any intraoperative complications. All tubes were removed successfully in the outpatient department three months later. Mean duration of follow-up after tube removal was 8.7±2.3 (range 6-12) mo.
Treatment effects were defined at the end of follow-up after the stent was removed. The outcomes were defined at three levels: Cured entirely, meliorated and no effects. Cured entirely was defined as the absence of epiphora, and no canalicular obstruction or stenosis when an irrigation test was performed, and the punctum was in a good position and shape. Meliorated was defined as: mild epiphora or canalicular stenosis when irrigated or there was punctal slitting. The no effects outcome comprised the presence of epiphora, canalicular obstruction on irrigation, and no resetting of the punctum.
Of the 47 patients, 41 patients (87.23%) were cured entirely. Four patients (8.51%) were allocated to the meliorated outcome as they developed mild epiphora in conditions such as wind and cold weather, which irritate the eye. However, they considered the outcome negligible and there was no punctal slitting. Two patients (4.26%) experienced surgical failure.
Eyelid position was satisfactory in all patients. No cases showed ectropion of the eyelid. No complications related to the stent such as eye irritation, inflammation, granuloma formation, or punctum ectropion occurred during the stenting period or during removal. There were no cases of premature stent extrusion. None of the patients complained about the appearance of the stent. The tube has no influence on the daily life of the patients. Sometimes even less attention was paid to the presence of the tube(Figure 3).
DISCUSSION
Lacrimal canalicular anastomosis with stenting of the canalicular cut ends is currently the recommended surgical treatment for canalicular lacerations. Identification of the nasal end of the canaliculus is the most important step in surgical repair. In 43 out of 47 cases in this study, the medial cut ends were identified by direct observation under the microscope. Direct observation is the most common method. The medial cut end typically had a rolled white edge and a shiny epithelial lining under the microscope. It is important to expose the operation field with a sterile piece of cotton or suture traction in the nasal skin wound, have the patient’s head tilted towards the injured side, and have sufficient hemostasis. There are other methods for identification such as the injection of air[3]or liquid[4]and use of a pigtail probe[5]. In three cases, the lacerated end was deep and the surrounding soft tissues were crushed, thus the end was found by injecting liquid. In one case, there were no options for detecting the lacerated canalicular end and we used a pigtail probe. Application of a pigtail probe is easy to form a false passage. In addition, it is difficult to control the direction, and the arc of the probe is fixed and can easily damage the lacrimal system. Therefore, we do not recommend the usual use of this method.
Selection of the appropriate stent is important for the success of surgery. In terms of material, there are primarily two types-epidural anesthetic tube and silicone tube. In our study, we chose silicone tube because the silicone tube has the advantage of the epidural anesthetic tube. For use with an epidural anesthetic tube, its end must be fixed on the eyelid using percutaneous sutures. Sometimes, the suture is loose, and a second set of sutures is required, which may be more invasive. If the loose tube cannot be fixed in time, it may be pulled out in advance or it may stimulate the cornea. Secondly, the presence of an external stent is not cosmetically satisfactory, especially for young patients. The exposed part may also affect some daily activities, such as washing the face. Lastly, an epidural catheter is relatively hard and does not bend easily. After implantation is performed, the lacrimal punctum is valgus and does not attach well to the conjunctiva. Consequently, the siphon function of the lacrimal system is damaged and most patients complain of uncontrollable tears. Furthermore, the hard tube may cause a tear in the lacrimal punctum. In addition, the fixed end may stretch the skin and cause a certain amount of pain to the patient. On the contrary, our silicone tube does not have the shortcomings above. Firstly, it does not need to be fixed onto the surface of the skin, reducing the pain for patients. Secondly, after the operation, a loop of tubing is left visible and extends between the inferior and superior puncta and this was cosmetically satisfactory for patients. Last, the silicone tube is soft and flexible, has good tissue compatibility, and does not increase pericanalicular inflammation[6]. After implantation, the lacrimal punctum was in its normal position and had good contact with the lacrimal lacus. The diameter of the middle part of the tube is only 0.5 mm. The lacrimal punctum is not completely blocked; tears are sucked into the lacrimal duct along the gap between the tube and the lacrimal punctum. Therefore, in this study, patients did not experience lacrimation as a side effect. Patients had no other discomfort following the operation.
About silicone tube, there are different designs and implantation at present. As far as the implantation method is concerned, it can be divided into monocanalicular intubation and bicanalicular intubation. The efficacy of a monocanalicular stent was not significantly different than a bicanalicular stent[7]. Abroad, Monostent and Mini-Monoka(MM), which are representative of the monocanalicular intubation, are widely used for canalicular laceration[8-10]. However, these products have not yet entered the Chinese market. They could avoid injury to the intact canaliculus by monocanalicular intubation, but the rate of early extrusion is high. In 22 patients with MM insertion, 29% had premature stent loss and 14% had stent migration, and this was only applied to the rupture of a single lacrimal duct[11]. Masterka is a new monocanalicular silicone tube designed in recent years, but it still has the drawbacks mentioned above[12]. A “Y” shaped silicon tube was reported for the treatment of lower canalicular laceration in China. But most of the implantation process was carried out in the nasal cavity: traction guide was hooked from the nasal cavity and the stent was retrograde retracted from the inferior meatus into the lacrimal duct[13]. Our newly designed tube belongs to bicanalicular intubation. In our study, no extrusion occurred in the three-month postoperative period. The silicone tube is not fixed, and theoretically, there is the possibility that the tube may be extruded. However, due to limited space and mechanical principles, the tube would not likely come out. The diameter of both ends of the tube is 1.1-mm outer diameter. After implantation, the silicone tube diameter from the lacrimal sac to nasolacrimal duct opening was 1.1 mm and with the two sections side by side, the diameter will reach 2.2 mm. However, the diameter of lacrimal canaliculi is only 0.5 mm. Therefore, the silicone tube was placed in a tight space, and not easily removed. We also hypothesize that the orbicularis muscle may have an extrusion effect on the lacrimal canaliculus and this effect may be helpful in preventing prolapse of the tube. Thus, without the need for fixing, the tube essentially cannot fall out and is self-retaining. Also, the newly designed tube is particularly suitable for both superior and inferior canaliculi lacerations in one eye. In our study, 3 (6.38%) had bicanalicular lacerations.
As for design, there are three main kinds. One design in a study by Panetal[14]reported that the two ends of the silicone tube required knotting in the nasal cavity, so that patients have foreign body sensation. The knot was easily attached by secretions. When removing the silicone tube, the doctor needed to hook the knot from the nose, which may damage the nasal mucosa. In our clinic, we encountered times when the knot was carelessly pulled into the lacrimal sac. In these cases, there were some difficulties removing the tube. In some patients, the tube could not be removed and there was long-term retention. The Crawford tube also has the shortcomings mentioned above[15]. In the study by Liangetal[16]and Liuetal[17]another design of silicone tube was inserted backwards into the lacrimal system with the guide of a probe. The guidelines for this method were complex and involved tying the tube off three times (end-to-end) with 5-0 silk sutures, which is cumbersome. Another disadvantage of these previous methods was that the operator was required to use a nasal endoscope to identify the end of the stent or create a knot under the inferior turbinate. Without the help of endoscopy, it is easy to damage the nasal mucosa and cause bleeding, and repeated hooking may cause an unnecessary increase in pain to the patient. This method also required doctors to be trained in nasal endoscopy. The third design, the self-retaining stent (SRS, FCI Ophthalmic, Issy-Les Moulineaux, France) has been developed recently[18]. To date, there are no studies investigating its application for canalicular laceration. The head is larger than the lacrimal punctum, and it has no probe for guidance, so we hypothesize that insertion would be difficult. Prior to implantation, the Bowman probes were applied to increase the size of the canaliculi. The probe is relatively hard, and this may damage the normal lacrimal duct. So we used a newly designed silicone tube and modified the method of inserting. Compared to others, our design has many incomparable advantages. First, the insertion process was quick and straightforward. There are no cumbersome steps for insertion, no need to retrieve the stent from the nose, and no need to create knots or sutures. The procedure is very simple and implantation may take only five minutes for a skilled surgeon. The process of implantation is very similar to that of the epidural catheter. The surgeon does not need to carry out special training, and the learning curve is short. Furthermore, they do not need the help of a nasal endoscope. Another advantage of our product is that the front ends of the new silicone tube are in an arc shape that can prevent the damage to the mucosa of the lacrimal duct. Additionally, the front ends of the new silicone tube have a probe feature at the same time. Therefore, the tube was passed through the lacrimal passage once, unlike other designs that require multiple insertions into the lacrimal duct. There is less damage to the lacrimal duct system than that with other designs such as a lacrimal hollow cannula with internal copper wire[14], a segmental epidural catheter[16]and a pigtail probe[5]. No iatrogenic injury occurred in our study as the design minimizes trauma to the healthy canalicular system. There was no canalicular obstruction or stenosis when an irrigation test through the unlacerated canaliculus was performed at each visit. Last, the tube is shorter than other designs with a total length of 88 mm. Patients have no sensation of a foreign body in the nasal cavity.
For the first time, We applied the silicone tube in the treatment of canalicular lacerations in a total of 47 patients. The newly designed silicone tube was found an effective tool with a relatively high success rate, providing complete epiphora relief in 41 (87.23%) patients, partial relief in four (8.51%) patients and only failure in two patients (4.26%). No complications associated with the silicone tubes occurred.
Studies in normal healing suggest that this process should be complete within three months[19]. As the silicone tube is generally very well tolerated, we prefer to leave it in place for three months to ensure that the process of proliferative fibrosis has fully matured before the stent is removed. It is easy to remove the tube, simply by pulling it out between the superior and inferior canaliculi. There is no need for suture removal or use of an extensive nasal endoscopy. When removing it, we should not pull out the upper and lower part of the tube simultaneously, but successively.
In conclusion, the new design of silicone tube used in this study was an effective tool for the treatment of traumatic canalicular lacerations and has many advantages over other designs and methods. The operation process is simple and easy to grasp for the surgeon. It is associated with fewer complications. And the silicone tube is available for both superior and inferior canaliculi lacerations in a single eye.
The main limitation of our study was the absence of a control group. However, we believe that the relatively large number of patients used in this study makes it a better choice for the management of canalicular lacerations.
