
Retrograde intrarenal surgery:An expanding role in treatment of urolithiasis
2018-12-25 02:22:18MarRodrguezMonsalveHerreroSteeveDoiziEtienneXavierKellerVincentDeConinckOlivierTraxer
Asian Journal of Urology 2018年4期
María Rodríguez-Monsalve Herrero,Steeve Doizi,Etienne Xavier Keller,Vincent De Coninck,Olivier Traxer
Department of Urology,Tenon Hospital,Assistance-Publique H?pitaux de Paris,Paris,France
KEYWORDS Ureteroscopy;Retrograde intrarenal surgery;Endourology;Urolithiasis
Abstract During the past 3 decades,the surgical management of kidney stones has undergone many technological advances and one is the development of the flexible ureteroscopy.The development of this instrument as well as ancillary equipment such as baskets,graspers,and others,and improvements in lithotripsy with Holmium:YAG laser have led to expand its indications with diagnostic and therapeutic management of medical issues of the upper urinary tract such as urolithiasis and urothelial tumors.The objective of this review is to describe its indications and results in the different scenarios for the treatment of urinary stones.
1.Introduction
The historical evolution of flexible ureteroscopy(fURS)has been closely related to several technological advances.Firstly described by Marshall in 1964[1],it was not until 1971 that Takayasu et al.[2]reported the first successful fURS in humans,but the technique did not gain popularity at that time.In 1987 Bagley[3]finally described the technique and its indications,and lately Fuchs and Fuchs[4]systematized the procedure in the way as it is known nowadays.Since thisfirst description,many improvements have been made on the endoscopes as well as ancillary equipment leading to an incredible increase in its use and applications.The development made since the 1990s include the miniaturization of the outer diameter,at least 270°deflexion in both upward and downward directions and the presence of working channels of 3.6 Fr facilitating surgery with an adequate irrigation and the use of accessory instruments.In 2004,digital fURS have been introduced to the market improving the quality of image compared to the fiberoptic fURS.The last innovation is the introduction of single use digital scopes in 2015 with competitive technical characteristics with the reusable ones[5-7].Along with these developments,ancillary equipment benefited from advancements such as baskets,graspers,and others improvements in lithotripsy including the introduction of laser lithotripsy with Holmium:YAG.This led to an increased level of success achieved with this technique and expanding its indications.
The use of this technique can achieve successful results in ureteral and renal stones,and we aimed to review its indications and results in the different scenarios.
2.Historical evolution of stone management
The prevalence ofkidney stone disease has increased overthe past 3 decades and reaches a lifetime rate of approximately 14%[8].This increase is reported to affect most of the developed countries[9-17].In addition,stone disease appears to be related with multiple factors such as socioeconomic conditions,lifestyle changes,environmental factors and has been found to be strongly associated with some comorbidities as obesity,diabetes and metabolic syndrome whose prevalence raised in the same period of time.It is also of importance to note that the widespread use of imaging modalities may explain partly the increase of prevalence of urolithiasis due to incidental stones[18].Simultaneously,the treatment of urolithiasis benefited from the development of minimally invasive surgical techniques such as shock wave lithotripsy(SWL),ureteroscopy(URS)and percutaneous nephrolithotomy(PCNL).Due to technologicaladvances and a comprehensive evaluation of these techniques,trends in surgical management of urolithiasis changed in clinical practice overthe last decades.Recent studies reported the trends in the surgical management of urolithiasis;most of them showed a significant increase in the use of URS compared to SWL,URS becoming the main modality oftreatment since late 2000s.Although PCNL also benefited from technological advances,this technique remained stable over the time and represents approximately 5%of stone treatments[19-21].
3.Technical considerations in retrograde intrarenal surgery(RIRS)
3.1.Access to the upper urinary tract and ureteral access sheath(UAS)placement
Whether it is semi-rigid or fURS,the procedure begins with a rigid cystoscopy to visualize the bladder and to identify location of the ureteric orifices.At this point,a guidewire can be placed into the renal cavities under fluoroscopic guidance.Although not mandatory,the use of a safety guidewire is highly advised as it ensures access to the collecting system and facilitates the insertion of a stent in case of ureteric or collecting system injury such as ureteral perforation or excessive bleeding[22-24].
Once the wire in place,the surgeon may insert a UAS.This choice dependson stone burden,upperurinary tractanatomy,and surgeon’spreference.The goalsofthe UASare:to facilitate multiple passages for stone fragments removal and most importantly to provide irrigation with better fluid outflow,thereby decreasing the intrarenal pressure and potentially reducing operatory time[25-27].The choice ofthe UAS,itssize and diameterdepend on patient’sanatomy and the endoscope utilized[28,29].When a UAS is placed,it is imperative to not force asureteraldamage may asa resultofforced maneouvers.If any resistance is encountered during UAS placement,the endoscope can be introduced to explore the ureter.If not possible,itis saferto place a ureteralstentforpassive ureteral dilation,making a secondary fURS procedure much easier to perform at a later date[30].
3.2.Advances in lithotripsy technology
Currently,laser lithotripsy using Holmium:YAG laser has become the standard for stone lithotripsy during fURS due to its efficacy and safety[31].The holmium laser is effective for any composition of stones.Stones are ablated via a photothermal effect,the laser radiation being absorbed by residual water in the stone,creating a vapour pressure that breaks the stone[32-34].
The current generation of laser lithotripters allows three parameters to set:Pulse energy(J),pulse frequency(Hz)and pulse duration.According to the effect produced,two options for stone laser lithotripsy have been described:Fragmentation,based on the production of fragments that needs to be removed subsequently with a basket,and“dusting” where energy is used to reduce the stone to fine dust and fragments smaller than 2 mm in diameter,that are supposed to pass spontaneously[35].A third setting called“popcorn effect” may be used after fragmentation in order to produce smaller pieces[36,37].
Laser settings for these techniques are:
-Fragmentation:High energy(1-2 J),low frequency(3-5 Hz)and if needed short pulse duration;
-Dusting:most importantly it is required to use a low energy(0.2-0.5 J),high frequency(10-20 Hz)and if needed long pulse duration;
- “Popcorn effect”:High energy(1 J),high frequency(10-20 Hz)and if needed long pulse duration.
Selecting the most appropriate technique depends on stone size,surgeon’s preference,intrarenal anatomy and stone composition and location.Furthermore,those techniques can also be combined during the same procedure to achieve better results.
3.3.Role of preoperative and postoperative stenting nowadays
Prestenting is not necessary before URS,however if dif ficulties are encountered to access the ureter,a ureteric stent can be placed for passive ureteral dilation to facilitate access at a latter procedure[38].
Postoperative stenting must be considered in patients at increased risk of complications such as ureteral trauma or perforation,residual fragments,pregnancy,urinary tract infection and bleeding.To prevent the incidence of postoperative ureteric obstruction and renal colic secondary to ureteral edema,a ureteral stent may be placed[39,40].This practice is debated but according to the last American Urological Association(AUA)guidelines,ureteral stenting is recommended among patients with ureteric injury during URS,those with evidence of ureteral stricture or other anatomical impediments to stone fragment clearance,such as ureteral wall edema,a large stone burden(>15 mm),those who have an anatomically or functionally solitary kidney or renal functional impairment,and those in whom another ipsilateral URS is planned[41,42].
In European Association of Urology(EAU)guidelines it is postulated that,if uncomplicated URS,stent does not need to be placed[43].
4.Ureter stones
Stones located in the ureter are related with the highest morbidity because they can cause renal obstruction that can lead to renal colic,renal failure and sepsis.Thus,ureteral stones frequently lead to the need of urgent assistance and treatment.Therapeutic options for ureteral stones are wide and include observation,medical expulsive therapy,SWL,and surgery(fURS or semi-rigid URS).
4.1.EAU/AUA guidelines
In 2016,the AUA and Endourology Society Guideline published clinical guidelines on surgical management of stones[41,42].The EAU updated their guidelines in 2018[43].
According to the guidelines,conservative management is feasible in uncomplicated and small size ureteral stones with a cut-off size of 6 mm and 10 mm in EAU and AUA guidelines,respectively.
According to EAU guidelines,alpha blockers can be used as medicalexpulsive therapy to treatdistalureteralstones>5 mm and should only be used if active removal is not indicated.
EAU guidelines propose active removal of ureteral stones in case of low likelihood of spontaneous passage,persistent pain despite adequate analgesic medication,persistent obstruction and renal insufficiency(renal failure,bilateral obstruction or single kidney)[33].
If active stone removal is indicated URS is the treatment of choice in both guidelines for distal ureteral stones greater than 10 mm.For distal ureteral stones<10 mm,SWL can be used as option as well as URS in EAU guidelines.In AUA guidelines,URS remains the only first option.
For proximal ureteral stones,URS is recommended asfirst option in stones>10 mm in EAU guidelines and as an equally valid technique with SWL in stones<10 mm.In AUA guidelines URS is treatment of choice for all proximal ureteral stones regardless of the size.
Comparison between indications of the two guidelines are summarized in Table 1.
In conclusion,the role of URS is universally accepted as an excellent choice for treatment of ureteral stones that can be performed in all patients without any specific contraindications apart from general problems such as urinary tract infections or contraindication for general anesthesia.
It is also important to mention that URS is the preferred modality if stone removal is essential and antithrombotic therapy cannot be discontinued since it is associated with less morbidity[41-43].
In case of severe obesity URS should be offered as thefirst-line therapy[44].
4.2.Outcomes
4.2.1.Comparison of URS vs.SWL
The outcomes of URS and SWL for the treatment of ureteral stones are similar in terms of stone free rates,but URS has a higher rate of stone free status after a single procedure.In a systematic review comparing URS to SWL for the treatment of ureteralstones,URS wasassociated with a significantly greaterstone free rate at 4 weeks after surgery but when results were compared at 3 months the difference was not significant[45].Also,URSwasassociated with fewerretreatmentrates,ranging from 0%to 18%for URS and 3.0%-61.1%for SWL.
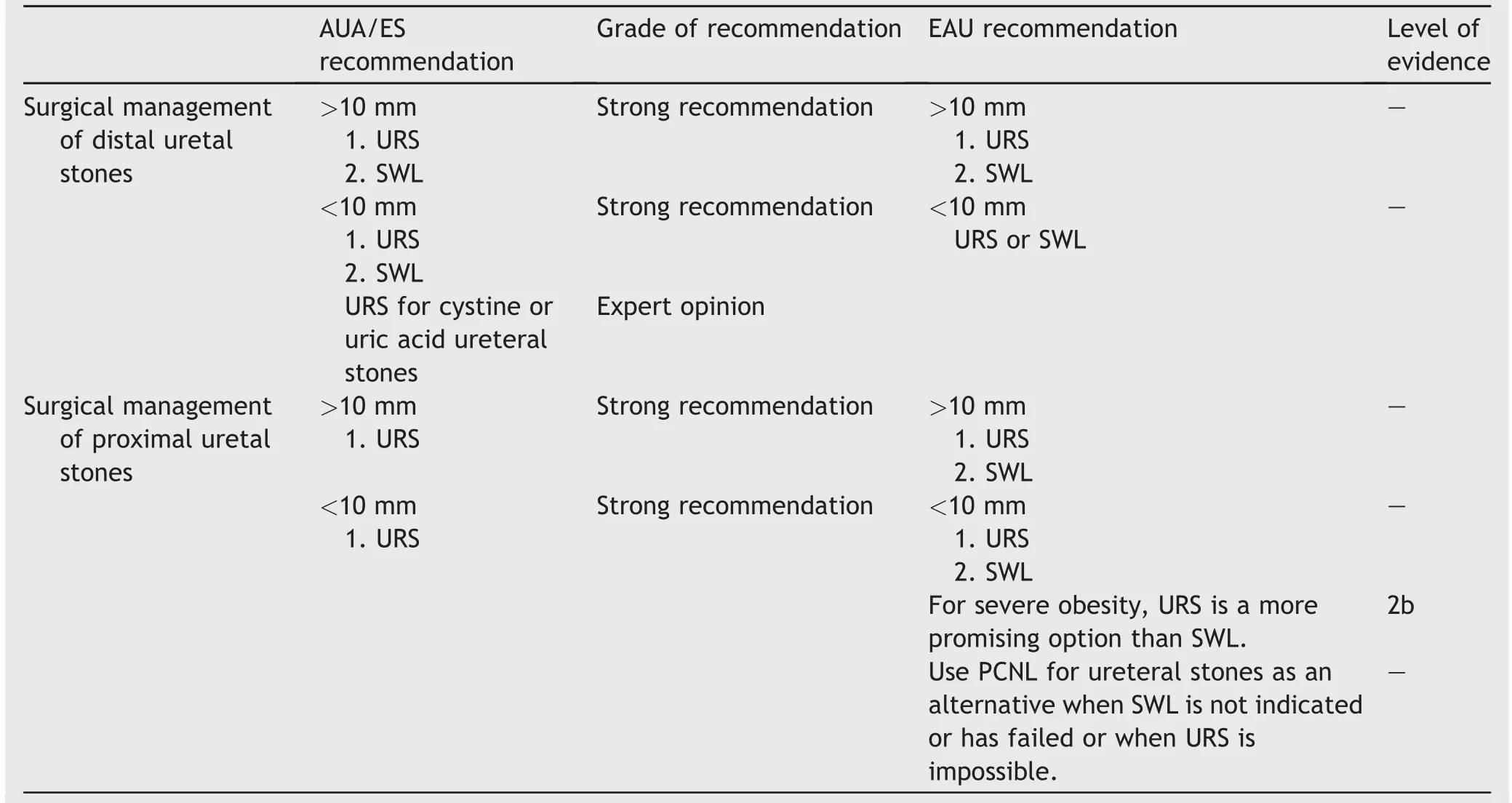
Table 1 AUA and EAU guidelines on ureteral stones.
Hospital stay as well as the need for adjunctive procedures was higher in the URS group(most commonly the insertion of a double J stent).
The predictive factors of failure of SWL are obesity,stone size exceeding 10 mm,mid-ureteral stone and severe hydronephrosis.If these factors are present,initial surgical approach with URS is recommended[46].
4.2.2.Comparison of fURS vs.semi-rigid URS
A study compared the outcomes of semi-rigid versus fURS for the treatment of proximal ureteral stones.Stone free rates at 3 months were 77.7%and 93.4%for semi-rigid and fURS,respectively.There was no significant difference in terms of complication rates[47].
In a study comparing outcomes for ureteral stones at different locations,in which semi-rigid URS was predominantly performed(72%of the patients),stone free rates reached 94.2%for distalureter location,89.4%for midureter location,84.5%for proximal ureter location,and 76.6%for multiple locations.Stone free rate was higher in patients treated with semi-rigid URS(90.2%)compared to fURS(80.9%)for the treatment of midureter stones only[48,49].
It has also been reported that fURS in prestented patients was not associated with a better stone free rate,except in case of ureteral location in univariate analysis.Thus,prestenting seems not to influence the outcomes of fURS[50].
4.2.3.Use of antegrade approach
The antegrade approach has been described as an option in cases of large impacted ureteral calculi with similar efficacy and safety rates[51].The antegrade approach achieves higher stone free rates than those of retrograde URS with Holmium:YAG laser lithotripsy.The drawbacks of the antegrade procedure are longer operative time and hospitalstay.
This approach may be an option in patients with ureterointestinal diversion such as ileal conduit[52].
5.Kidney stones
During the last 3 decades,many changes have been made in the surgical management of kidney stones with the development of minimally invasive techniques such as SWL,semi-rigid and fURS and PCNL.
The use of fURS to treat renal stones has increased in the last few years dramatically in comparison with the other active treatment options:SWL and PCNL[53].This increase in the number of procedures is related to advances in technology(endoscopes and equipment)and the efficiency as well as safety of the URS for the treatment of renal stones.
5.1.EAU/AUA guidelines
Herein,we present the indications presented in AUA and EAU guidelines for clinical and surgical treatment of kidney stones[41-43].
When renal stones are discovered incidentally,it may be questioned whether active stone treatment is necessary.If asymptomatic,such stones may also be controlled expectatively.According to the EAU guidelines,active surveillance can be offered for stones up to 15 mm.
Both EAU and AUA guidelines recommend follow-up imaging as an integer part of active surveillance.
Active treatment can be considered in cases of associated urinary infection,stone growth,and personal/vocational reasons like pilots for example,choice of treatment.It is known that the risk of presenting a symptomatic episode or need for intervention in asymptomatic patients with renal stones is 10%-25%per year[54].
Active treatment is recommended in cases of obstruction or symptomatic stones in both guidelines.
Comparison between indications of the two guidelines are summarized in Table 2.
For stones<20 mm located in the renal pelvis or,upper and middle calyx,SWL and fURS are the treatments of choice.In EAU guidelines PCNL is another option considered in stones from 10 to 20 mm.In cases of stones larger than 20 mm PCNL is the first option for every location.
For stones<10 mm located in the lower pole,fURS or SWL are recommended as primary treatment option.For stones between 10 and 20 mm,both fURS and PCNL are valid options according to both guidelines.In cases of stones larger than 20 mm again PCNL is the first option.
Similar to ureteral stones,same recommendations are made for use of perioperative prophylaxis and antithrombotic therapy in cases of kidney stones[41-43].
Also in cases of severe obesity,RIRS should be considered as first-line therapy for active removal of kidney stones[44].
5.2.Outcomes
When comparing treatment outcomes of renal stones,some considerations must be taken into account.First,most of the studies are limited by their retrospective nature.Second,various definitions of stone free rate are used with different imaging techniques,size cut-off and differing follow-up durations.
Also,we might consider that different instruments,techniques and tools can be used for both procedures,RIRS and PCNL making it very difficult to standardize.
5.2.1.Stones>20 mm
Recent series have evaluated the validity of RIRS as a fistline therapy for stones larger than 2 cm[54,55].In experienced hands,feasibility of this approach could be verifi ed,but the authors pointed at a possible lower stone free rates and a higher retreatment rates.The benefit of using this technique in stones>20 mm is the smaller rate of complications in comparison with PCNL and the shorter hospitalization time.
5.2.1.1.Stone free rate outcomes. Fortreatmentofstones>20 mm,single surgicalprocedure stone free rate wasin favour of PCNL compared to RIRS[56,57].Conversely,a few reports showed comparable stone free rates between RIRS and PCNL when re-treatment rates were not considered[58].Series with more than 50 patients reported mean stone free rates between 88%and 93.5%and mean number of procedures between 1.1 and 1.54[54,59,60].A recent study compared stone free rates between four different stone size categoriesand reported that this latter was 70.5%for stones between 20 and 30 mm,and 55%for stones>30 mm after a single procedure[61].

Table 2 AUA and EAU guidelines on kidney stones.
According to these results,we may assume that both RIRS and PCNL are comparable in terms of stone free rates.
5.2.1.2.Lower pole outcomes. The access to lower pole stones can be challenging,especially when unfavourable anatomic factors such as long infundibulum and a sharp infundibulopelvic angle(<30°)are present[62].Some studies showed similar stone free rates of RIRS in such cases compared to PCNL[60-64].
5.2.1.3.Surgical and hospitalization times. In terms of surgical time many studies reported benefit for RIRS even for treating stones<20 mm.The use of digital scopes has also improved operative time.In the study of Binbay et al.[65],a significant decrease in surgical time has been demonstrated. Also, the hospitalization time was significantly shorter after RIRS in comparison with PCNL.The factor that reduces the hospitalization time after PCNL is a tubeless surgery[66].
5.2.1.4.Complications. Compared to PCNL,RIRS is associated with less severe and rate of complications[60].
5.2.2.Stones<20 mm
Treatment of stones smaller than 20 mm can be performed with SWL,RIRS or PCNL.
Many series reported in recent years the outcomes of comparing results of these techniques[67-71].When comparing the three techniques for stones<20 mm not located in the lower pole,stone free rates of SWL and fURS are inversely related to stone size.PCNL stone free rate is the least affected by stone size.
If the comparison is made between fURS and SWL it seems that fURS has a lower likelihood of needing more subsequent procedures so we could assume stone free will be achieved quicker than with SWL[72].
5.2.2.1.Stone free rate outcomes. SWL for treating renal stones showed good results in stones located outside of lower pole.The stone-free rates at 3 months are 86%-89%(renal pelvis),71%-83%(upper calyx),73%-84%(middle calyx)and 37%-68%(lower calyx)[72].
In a meta-analysis published by De et al.[57],a subanalysis comparing efficacy of RIRS and minimally invasive PCNL showed a significant greater stone free rate in favour of RIRS than mini-or micro-PCNL with an odds ratio (OR) of 1.70 (95% confidence interval (CI)1.07-2.70).For 10-20 mm stones,Sabnis et al.[68]noted stone free rates of 96.88%for RIRS and 100%for mini-PCNL.In a recent study comparing stone free rates between four different stone size categories the stone free rate of fURS was 79.8%for stones between 10 mm and 20 mm,and 90.4%for stones<10 mm after a single procedure[61].
5.2.2.2.Lower pole outcomes. Lower pole is the most common location for renal stones.Donalson et al.[73],in a systematic review and meta-analysis,compared the outcomesoflowerpole stones<20 mm treatmentwith SWL,RIRS or PCNL.For>10 mm stones,stone free rates were higher after PCNL(96.3%)and RIRS(91.7%)compared to SWL(54.5%).For<10 mm stones,the magnitude of benefice was less important.Another study found that stone free rates did not differ significantly between lower pole(74.1%)and non-lower pole stones(78%)[74].
5.2.2.3.Surgical and hospitalization times. Regarding surgical time,data are inconclusive but it seems that RIRS has similar operative time compared to other techniques but with less radiation exposure during procedure and shorter hospitalization time[68,70].
5.2.2.4.Complications. The complication rates for PCNL are linked to diameter of the tract.Reducing the tract reduces bleeding and transfusion rates[75].Number of complications are similar when comparing both techniques but with less postoperative pain in the case of RIRS.
5.3.Complications
The overall complication rate after URS is 9%-25%[48,76,77].The intraoperative complication rate in URS according to the recent study published was 4.2%and the postoperative one was 2.6%[78].Few risk factors have been isolated for the appearance of complications but it is demonstrated that previous perforation is an important one.
The most common complications after fURS are:
-Ureteral strictures:One of the most important complication after endoscopic treatment of ureteral stones,especially in the case of impacted stones is the development of ureteral stenosis that can appear up to 7.8%of patients in cases of impacted stones.
-Haematuria:It has been reported as a complication of both SWL and URS.In one study,haematuria rates(assessed according to a visual analogue score)were significantly higher after URS than SWL.In another study,rates of gross haematuria following treatment were significantly higher after SWL than URS,occurring in 20%of patients after SWL,compared with 2.5%of patients treated with URS[45,79].
-Infection/sepsis:The importance of preventing infections is vital in this surgery because this complication is the most life threatening and must be carefully evaluated.A urine culture must be performed before any treatment.In patients with negative urine culture,single dose antibiotic prophylaxis must be offered perioperatively.The incidence of infectious complications after fURS can be rated around 8%-10%.Pyuria,operative duration,and infectious stones are risk factors for infectious complications following fURS[80].
-Steinstrasse:The incidence of this complication increases with the size of the treated stones.
-Pain:In general,reported pain levels were relatively low and,if present,can be managed with oral analgesia.
-Post voiding symptoms:The prevalence of post voiding symptoms is 33.7%after treatment with URS[81].
6.Particular cases
6.1.Horseshoe kidney
This is the most common congenital abnormality with an incidence of 1/400 births.This condition predisposes to stone formation with a rate of 20%[82].Stones in a horseshoe kidney may reasonably be managed with any of the surgical modality according to EAU guidelines,but the guidelines state that SWL may result in poor passage of fragments.AUA only mentions that PCNL should be first-line treatment for lower pole stones>10 mm.
Molimard et al.[84]reported a series of 17 patients with stones in horseshoe kidney treated with fURS and showed a mean of 1.5 procedures per patient.Stone free and complication rates were 88.2%and 11.76%,respectively.We can conclude that,in the few studies focusing on the effectiveness of RIRS in horseshoe kidney,fURS achieved high success rate and minimal morbidity[83-85].
6.2.Pelvic kidney
Pelvic kidney incidence ranges from 1 in 500-3000.It is an embrionary abnormality that results from failure of the kidney to ascend to the normal anatomic location in the renal fossa.It is located in the pelvic fossa,anterior to the bladder and below the aortic bifurcation.The accompanying vasculature and rotation abnormalities complicate treatment modalities in these cases[86].Patients with pelvic kidney are more likely to develop urolithiasis compared with the normal population.A series reported the outcomes of fURS in 26 patients,with mean stone size of 17.0±5.1 mm(10-28 mm),treatment was successful in 84.6%(22 patients).It concluded that this procedure is safe and effective for small-and medium-sized stones[87].
6.3.Urinary diversion
Patients with urinary diversion have higher risk of stone formation favoured by well-studied metabolic factors(hyperoxaluria,hypercalciuria,hypocitraturia)in combination with other mechanical and infectious factors[88,89].A study presenting 20 PCNL and four antegrade URS procedures showed that these techniques were feasible,safe and effective[90].
The use of antegrade fURS in these patients has been reported with a stone free rate of 80%after the first procedure[52].Due to the higher risk of recurrence of stone disease in these patients,regular follow-up after treatment is recommended for early detection and treatment of stone recurrence.
6.4.Caliceal diverticulum
Caliceal diverticulum has a reported incidence of 0.6%.There are genital outpouchings from the renal calyx or pelvis into the renal cortex.These diverticula are lined with transitional cell epithelium and have no secretory function.Urine usually enters in the diverticulum by passive filling through the usually narrow caliceal neck,leading to stone formation in 10%-50%of cases[91].Indications for treatment in these cases include pain,recurrent infection,increased stone growth,haematuria,or damage of surrounding parenchyma.Chen et al.[92]retrospectively reviewed the records of 43 patients with symptomatic caliceal diverticulum stones treated with fURS and reported a success rate of 81.4%(35 patients),the remaining eight patients (16.6%) had significant residual fragments(>3 mm),five of them became completely stone free after the second procedure,and other three patients were symptom free and underwent a routine follow-up.The final treatment success rate was 93.0%.
For the management of caliceal diverticulum,EAU proposes any of the approaches,whereas AUA recommend endoscopic procedures over SWL.
Bas et al.[93]compared the outcomes of 54 patients that have been treated with fURS or PCNL for stone-bearing caliceal diverticula and concluded that the location of the stone and diverticula is an important factor for the selection of the procedure.
6.5.Pediatric cases
Nowadays more than 1%-2%of all urinary stones are diagnosed in children with an increasing rate in developed countries and remains an endemic disease in some areas[94,95].Several factors must be considered in children.First,larger fragments may pass without repercussion.Second,the need of adapting the instruments to a smaller caliber of urinary organs.In guidelines,SWL remains the first-line option for ureteral stones and renal stones up to 20 mm.If stones are bigger than 20 mm PCNL and URS must be considered[96].
Azili el al[97].retrospectively analysed 80 ureterorenoscopic procedures performed in 58 renal units of 47 children,after a single procedure stone free rate was 50.9%but after a second session the stone clearance rate reached to 85.1%.
In the latest years with the development of smaller size fURS,RIRS has become an efficient treatment for pediatric patients and is associated with less radiation exposure and lower complications rates than PCNL[97,98].
7.Conclusion
The use of fURS has become widely accepted for the treatment of ureteral and renal stones.The continuous improvement in URS and its equipment has ameliorated the outcomes of this technique expanding the role in stone treatment.The high efficacy and lower rate of complications have positioned this technique as the treatment of choice for renal stones up to 20 mm and it must also be considered as an option for treating bigger stones.
Author contributions
Study design:María Rodr?′guez-Monsalve Herrero,Steeve Doizi,Olivier Traxer.
Data acquisition:María Rodr?′guez-Monsalve Herrero,Steeve Doizi,Etienne Xavier Keller,Vincent De Coninck.
Data analysis:María Rodr?′guez-Monsalve Herrero,Steeve Doizi,Olivier Traxer.
Drafting of the manuscript:María Rodr?′guez-Monsalve Herrero,Steeve Doizi.
Critical revision of the manuscript:Steeve Doizi,Etienne Xavier Keller,Vincent De Coninck,Olivier Traxer.
Supervision:María Rodr?′guez-Monsalve Herrero,Steeve Doizi,Olivier Traxer.
Conflicts of interest
The authors declare no confilict of interest.
Acknowledgments
Etienne Xavier Keller is supported by a Travel Grant from the University Hospital Zurich and a grant from the Kurt and Senta Herrmann Foundation.Vincent De Coninck is supported by a EUSP scholarship from the EAU and a grant from the Belgische Vereniging voor Urologie(BVU).
 Asian Journal of Urology2018年4期
Asian Journal of Urology2018年4期
- Asian Journal of Urology的其它文章
- Miniaturised percutaneous nephrolithotomy:Its role in the treatment of urolithiasis and our experience
- Present indications and techniques of percutaneous nephrolithotomy:What the future holds?
- Ureteral stents in urolithiasis
- Indications and contraindications for shock wave lithotripsy and how to improve outcomes
- Medical therapy for nephrolithiasis:State of the art
- Defining metabolic activity of nephrolithiasis-Appropriate evaluation and follow-up of stone formers