
Defining metabolic activity of nephrolithiasis-Appropriate evaluation and follow-up of stone formers
2018-12-25 02:22:16DnilWollinAmKplnGlnnPrmingrPitroMnulFrrroAntonioNouvnnAnrTsEmnulCroppiGiovnniGmroItHilrg
Asian Journal of Urology 2018年4期
Dnil A.Wollin *,Am G.Kpln Glnn M.Prmingr Pitro Mnul Frrro ,Antonio Nouvnn ,Anr Ts ,Emnul Croppi,Giovnni Gmro ,It P.Hilrg
a Duke Comprehensive Kidney Stone Center,Division of Urologic Surgery,Duke University Medical Center,Durham,NC,USA
b Columbus-Gemelli University Hospital,Division of Nephrology,Department of Medical Sciences,Rome,Italy
c University of Parma,Department of Clinical and Experimental Medicine,Parma,Italy
d S.Bortolo Hospital,Department of Urology,Vicenza,Italy
e Universidade Federal de Sa?o Paulo,Nephrology Division,Sa?o Paulo,Brazil
KEYWORDS Follow-up;Medical management;Metabolic evaluation;Urolithiasis
Abstract Considering the variation in metabolic evaluation and medical management of kidney stone disease,this consensus review was created to discuss the metabolic activity of nephrolithiasis,define the difference between single and recurrent stone formers,and develop a schema for metabolic and radiologic follow-up.A systematic review of the literature was performed to identify studies of metabolic evaluation and follow-up of patients with nephrolithiasis.Both single and recurrent stone formers share many similarities in metabolic profiles.The study group determined that based on an assessment of risk for stone recurrence and metabolic activity,single and recurrent stone formers should be evaluated comprehensively,including two 24 h urine studies on a random diet.Targeted medication and dietary recommendations are effective for many patients in reducing the risk of stone recurrence.Follow-up of those with stone disease should be obtained depending on the level of metabolic activity of the patient,the risk of chronic kidney disease and the risk of osteoporosis/osteopenia.A standard scheme includes a baseline metabolic profile,a repeat study 3-6 months after initiation of treatment,and then yearly when stable,with abdominal imaging obtained every 1-2 years.
1.Introduction
The metabolic evaluation and medical management of kidney stone disease varies widely,based on several patient-and practitioner-related factors.The purpose of this consensus document is to provide a guideline for appropriate evaluation and follow-up of stone formers based on metabolic stone activity.A systematic review of the literature was performed to identify studies of metabolic evaluation and follow-up of patients with nephrolithiasis.As limited prospective trials were available, wellperformed retrospective series were also included in our document.The authors then evaluated the evidence and developed consensus recommendations.
2.Methods
A systematic search was performed on PubMed of relevant studies related to the questions:How do we define the metabolic activity of nephrolithiasis?Is there a difference between single or recurrent stone formers and how are they defined?How should kidney stone patients be followed metabolically and radiographically?
The search was performed using specified research strings and captured manuscripts in English published before March 2015.Two of the study members were responsible for identifying eligible research that was addressed by the entire study group.For each included study,relevant data on study design,patient characteristics and outcomes(positive and negative)were extracted and critically appraised for reliability of results.After the consensus conference,data were reviewed up through the conclusion of 2017 to ensure no new recommendations could be made based on current data.
2.1.Single vs.recurrent stone formers
A single stone former is a patient who seeks advice for a single,solitary kidney stone episode or single kidney stone.A recurrent stone former is simply a patient with multiple kidney stones.Stones can occur synchronously or at different times;additionally they do not necessarily need to be associated with symptoms.Patients who form stones at an interval greater than 5 years apart fall into a gray zone coined by some authors as occasional or episodic stone formers[1].
This distinction between single,recurrent and occasionally recurrent stone formers would be an important one if these definitions somehow related to the patients’underlying metabolic derangements or need for medical treatment.Two retrospective studies from the early 1980s,and other more recent data,have suggested that metabolic abnormalities were as common in first time,single stone formers as they were in patients with recurrent nephrolithiasis[2-4].Additionally,making a distinction between single and recurrent stone formers is nearly impossible as there are no metabolic markers that can predict recurrence,aside from lower urine volumes and the amount of calcium in the urine[5].
In an opinion article addressing this very question,Gambaro et al.[6]proposed to consider first-episode stone formers as a distinct clinical entity for both healthcare and research purposes.The article suggests focusing research more on this population rather than those with recurrent nephrolithiasis,since the solitary stone former with occasional relapses uses 80%of healthcare resources.This article urges practitioners to focus on the heterogeneity of the stone formation process,especially when comparing single and recurrent stone formers.
More recently,Rule et al.[7]evaluated 2 239 first-time adult kidney stone formers and observed that the rate of recurrence(observed in 707 individuals)after 2,5,10 and 15 years were 11%,20%,31%and 39%,respectively.The authors identified through their medical records the following risk factors for recurrence:younger age,male sex,white race,family history of stones,prior asymptomatic or non-obstructing stones on imaging,symptomatic renal pelvic or lower pole stone on imaging,gross hematuria and uric acid stone composition.A recurrence of kidney stone nomogram was developed for the prediction of a second symptomatic stone episode,aiming to help identifying patients who may benefit from medical interventions.Instead of using the commonly cited 50%risk of recurrence at 10 years,which is based on high-risk patients in urology clinics,physicians can use the nomogram to individualize risk of symptomatic recurrence.It is important to note,though,that this nomogram has not been validated using external datasets beyond the development sample.At 10 years,stone recurrence rates ranged from 12%in the lowest-risk quintile to no more than 56%in the highest-risk quintile.However,the authors did not include 24 h urine collections as possible variables to predict risk because these data were not available.
Aside from recurrence,another option is to distinguish between stone formers who are metabolically active versus those who are metabolically inactive.The metabolically active stone former has new stone formation or stone growth on serial imaging whereas the metabolically inactive stone former has no apparent stone activity on follow-up imaging.With this categorization,the clinician can determine whether metabolic therapy is required to prevent further stone formation or stone growth.Targeted therapy in the metabolically active stone former has been demonstrated to significantly decrease stone formation risk[8,9].
At this time,the data do not currently support treating recurrent and first-time stone formers as separate clinical entities,although as personalized medicine improves,differing means of pathogenesis may be elucidated,thereby providing differing targets of treatment.
2.2.Indications for metabolic evaluation and medical management
There is a group of experts who believe that both recurrent and first-time stone formers should be evaluated metabolically and offered follow-up and metabolically-targeted treatment at specialized centers[10].Others suggest that the need for metabolic evaluation should be based on the patient’s risk factors for recurrent stone formation or other comorbidities.These risk factors include,but are not limited to:Uric acid and cystine stone formers,patients with recurrent or multiple stones,those with a family history of stone formation,children with calcium stones,stone formation in a solitary kidney,patients with concurrent medical conditions,individuals with nephrocalcinosis,chronic kidney disease(CKD)or bone diseases,and those with a history of bowel disease or bowel surgery[13].Other relative indications for a complete metabolic evaluation include:those patients whose job requires they be without stones(i.e.pilots,frequent business travelers),patients with stones difficult to treat(e.g.urinary tract abnormalities/reconstruction), and individuals who are immunocompromised.
We would recommend,in concordance with the American Urological Association(AUA)guideline regarding medical management of stones,that recurrent stone formers and high-risk(those with risk factors listed above)or interested first-time stone formers should be offered a metabolic evaluation[13].
2.3.Performing the metabolic evaluation
According to a previous and careful review of available randomized controlled trials(RCTs)by the Agency for Healthcare Research and Quality(AHRQ),limited evidence suggested that baseline urinary calcium,oxalate and citrate did not appear to predict efficacy of diet and pharmacologic interventions on stone recurrence.There has also been insufficient evidence to determine a role(if any)for urinary magnesium,phosphate,potassium,pH,calcium oxalate,calcium phosphate or uric acid supersaturation in predicting treatment efficacy or stone recurrence[11].
From a clinical practice perspective,considering the relative lack of evidence-based criteria for metabolic evaluation,many centers will nonetheless customize each patient’s evaluation to their individual risk factors and comorbidities[12].The recent guidelines on medical stone management from the AUA recommend that all patients with nephrolithiasis receive a screening evaluation which includes a medical and dietary history,serum chemistries,a urinalysis and an intact parathyroid hormone(PTH)level if primary hyperparathyroidism(HPT)is suspected[13].On the other hand,given that hypercalcemia can be intermittent,one may consider the measurement of PTH on a routine basis obtained at the same day ionized calcium is determined.This determination would rule out primary HPT and should distinguish it from secondary forms of HPT[14].
The full metabolic evaluation for a baseline metabolic profile should be obtained at least 3-4 weeks after the last stone passage or treatment.Patients undergoing metabolic evaluation should have an unobstructed urinary tract,eating their regular diet and without urinary tract infection.Debate amongst experts continues on the appropriate application of a 24 h urine study,how many 24 h urine studies should be obtained and when these metabolic tests should be performed.
2.3.1.Simplified metabolic evaluation
A simplified evaluation would be appropriate for the metabolically inactive patient with a single stone who is at lower risk for recurrence.The first-time adult calcium stone former without a family history of stones or any obvious metabolic abnormality may be the patient who can avoid a comprehensive metabolic workup.In many cases,these individuals may remain metabolically inactive if managed by fluid therapy alone[1].
The evaluation should include a detailed history and physical examination to assess for stone-forming risk factors including a detailed review of fluid intake,diet and medications.Laboratory evaluation should be performed to help determine the cause of stone disease,the existence of comorbidities(i.e.CKD)and dictate medical therapy.These studies should include:serum ionized calcium and phosphate to evaluate for primary HPT;serum creatinine to evaluate renal function;serum electrolytes and bicarbonate as well as 12 h fasting urinary pH to evaluate for distal renal tubular acidosis;serum uric acid to evaluate for gout;and 24 h urinary pH for hyperuricosuric calcium oxalate urolithiasis.A urinalysis should be performed to examine for stone crystals that could indicate stone type,assess urine pH and for signs of infection.A thorough review of imaging studies,particularly abdominal X-ray examination,can determine stone burden and may reveal stone type(e.g.nephrocalcinosis may portend renal tubular acidosis,radiolucent stones may be constituted of uric acid or cystine,while staghorn stones often are composed of struvite and associated with infection).
Stone analysis has a limited but potentially significant role in the simplified evaluation of the low-risk stone former.Kourambas et al.[15]evaluated 100 consecutive patients who underwent stone analysis and comprehensive metabolic evaluation.Patients with non-calcium stones had a metabolic diagnosis reflecting their specific metabolic disorder.Patients with calcium stones,however,had heterogeneous metabolic disorders.The exception in this study was the calcium-phosphate stone former,who had a significant likelihood of having renal tubular acidosis or primary HPT.The authors concluded that stone analysis alone may provide guidance for therapeutic treatment and obviate the need for a formal metabolic evaluation,especially in those with non-calcium oxalate stones.
2.3.2.Comprehensive metabolic evaluation
The comprehensive metabolic evaluation we recommend consists of the simplified evaluation in addition to 24 h urine collections that allow for targeted therapy.A recent study confirms that comprehensive metabolic evaluation is widely underutilized,and is offered to less than 8%of high-risk stone formers[16].Contrary to this,there is evidence to suggest that patients at low risk of stone recurrence are more interested in complete metabolic workups and targeted therapy than most clinicians would believe[17].As such,a low-risk-but interested-patient should also be offered a comprehensive metabolic evaluation with the understanding that this evaluation and treatment may relegate the patient to life-long medical therapy.Chandoke[18]evaluated the cost-effectiveness of medical management of stone disease as compared to surgical treatment,and determined that medical management of a first stone episode may not be cost-effective for some patients.For this reason,comprehensive evaluation should not be undertaken in all stone forming patients.
Calcium stone formers,especially the ones with idiopathic hypercalciuria,may present with decreased bone mineral density(BMD)[19];bone histomorphometry may further characterize their bone disease,which is often seen as increased bone resorption,low bone formation and abnormal mineralization[20,21].There has also been epidemiological evidence of increased risk for bone fractures in this population[22,23].Therefore,a bone densitometry should be considered in hypercalciuric patients as treatment can be focused on bone abnormalities,if found.
Targeted therapy based on the results of a metabolic evaluation is effective and supported by several observational studies[24,25]Fine et al.[24]showed a significant decrease in stone formation after shock wave lithotripsy for patients put on targeting medical therapy,including urinary alkalinizing agents(e.g.potassium citrate),thiazide diuretics,or other disease-specific medications.The stone formation rate decreased from 0.67 to 0.0 stones per patient per year(p<0.001)in patients who were stone-free after the procedure and decreased from 2.47 to 0.0 stones per patient per year(p<0.001)for the patients with residual stone fragments.A similar study of patients who had undergone percutaneous stone removal,with and without residual stone fragments,demonstrated a significant decrease in the stone formation rate with medical therapy based on comprehensive metabolic evaluation(0.67 vs.0.02,p<0.0001)[25].
Randomized clinical trials assessing the efficacy of empiric and directed dietary and medical treatment show efficacy of both treatment schemes[11].Kocvara et al.[26]demonstrated,in a prospective randomized study,that specific dietary therapy,adjusted according to a comprehensive metabolic evaluation,is more effective than general dietary recommendations in preventing formation of a second stone.
2.3.3.One vs.two 24 h urine collections
The validity of a single 24 h urine collection is a matter of debate.Several authors have proposed performing a single 24 h study to reduce cost and increase patient compliance,so long as the results are adequate for medical decisionmaking.Castle et al.[27]retrospectively examined 777 patients with two 24 h urine studies.The study showed that there was no significant difference in all 12 different parameters of two 24 h urine studies collected within 3 days of each other,concluding that a single 24 h study is adequate.Pak et al.[28]also demonstrated no significant difference between urine collections of 225 patients on random and restricted diets,with a highly significant positive correlation in the two random samples.
In another retrospective review of 813 patients,there were significant differences between samples collected within 10 days of each other.Depending on the parameter assessed,5.5%-44.9%of patients changed from having no metabolic abnormality to having an abnormality or vice versa.A significant number of patients in this study would have had different medical therapies prescribed if only one urine collection had been obtained[29].Another retrospective review corroborated these results,showing significant differences in all 11 urinary parameters between two separate samples collected on consecutive days[30].Parks et al.[31]found large variations between collections in 459 private practice and 683 university stone research patients,arguing that a single 24 h sample is insufficient and can lead to misdiagnosis of the patient’s underlying metabolic defect.
There is no evidence to suggest performing a 24 h urine collection on a calcium-restricted diet to diagnose absorptive hypercalciuria type 1 versus type 2.The diagnosis of absorptive hypercalciuria type 1 can be made on the basis of high urinary calcium alone.A calcium loading test is also unnecessary and currently does not appear to add any additional, clinically relevant information[24,25].
Based on previous studies,we recommend that two 24 h urine studies on a random diet should be collected on 2 non-consecutive days to complete a comprehensive metabolic evaluation for both recurrent stone formers and single stone formers at high risk of recurrence(positive family history,early age of onset,nephrocalcinosis,associated medical conditions).The presence of a solitary kidney also places the patient at high risk due to the more serious implications of obstruction from a stone.We recognize that multiple 24 h urine studies may not be financially or socially feasible for some patients;in these cases,a single 24 h urine collection should be used for information regarding metabolic abnormalities.
2.4.Follow-up
Follow-up is the mainstay of conservative and active management of nephrolithiasis,to prevent both stone growth and new stone formation.Close surveillance also aids to assess treatment adherence or effectiveness,allows the physician to adjust pharmacological treatment dosing and to determine short or long-term adverse effects of directed medical therapy.The single-stone former at mild to moderate risk of stone recurrence may not require medication but should be offered the following empiric guidelines:maintain high fluid intake(>2 500 mL/day)[32],decrease intake of salt and oxalate rich food[33],avoid purine gluttony,increase citrus fruit intake,while maintaining a normal calcium intake of 800-1 200 mg/day(including dairy and nondairy sources)[34-37].
Follow-up management of patients with stone disease varies widely between practitioners,and no studies have assessed an optimal follow-up schedule as the primary outcome.In fact,the AHRQ statement indicated that no pharmacologic RCTs reported and prospectively compared subsequent stone recurrence outcomes between treatments stratified by follow-up biochemistry or urine supersaturation levels or changes in these measures from pretreatment baseline[11].Accordingly,follow-up regimens are instead decided upon based on the experiences,preferences,beliefs or habits of individual clinicians.
2.4.1.Follow-up metabolic evaluation
RCTs that evaluated dietary or pharmacological interventions(e.g.thiazide or citrate)on stone prevention,suggest that 24 h urine samples should be obtained at intervals from 3 to 12 months.However,data from most of the pharmacological and dietary RCTs suggested that follow-up urine calcium values may have limitations as a predictor of treatment efficacy in preventing stone recurrence[11].Since there have been no available data from prospective trials concerning follow-up urine supersaturation levels,it is not established whether changes in urine supersaturation measurements due to treatment can predict reduced risk of recurrent stones.Although 24 h urine collections have not conclusively been shown to offer a superior method of preventing stone recurrence,there are a number of observational and case-control studies demonstrating that changes in the urinary parameters were associated with a reduction in stone activity[9,38,39],and thus,the AUA Nephrolithiasis Guidelines favored the use of repeated urine collections.With 24 h urine collections,the practitioner can prescribe specific,rather than generic,dietary recommendations to individual stone formers and target specific lithogenic risk factors with medication-directed therapy[13,40].Accordingly,a targeted urine screening,depending on the underlying metabolic disturbance,instead of a complete one,can be performed during follow-up,aiming at cost-effectiveness.
Regardless of the lack of evidence-based principles,most centers and clinical practitioners perform a yearly follow-up to review stone activity,symptoms,as well as to potentially modify dietary and medical recommendations.We are in agreement with the AUA Medical Stone Guidelines,suggest that another 24 h urine should be repeated,after an initial clinical evaluation,after 3-4 months on selective medical therapy(and within 6 months from the beginning of treatment),to assess response to dietary and/or medical therapy and monitor for adverse effects.Followup thereafter can be yearly,to assess the effectiveness and adherence of metabolic therapy.Some authors recommend 24 h urine parameters be obtained every 6 months[13].Additionally,repeated stone analysis is justified if a failure of dietary or medical therapy is seen[13].
The periodicity of blood testing for adverse effects assessment must be tailored to the type of pharmacological therapy.From nine RCTs of thiazide treatment for kidney stones with a mean follow-up of 2.6 years,only two studies measured serum glucose and lipid levels and found no significant change,two out of three studies that measured serum potassium observed a significant decline and all three studies in whom serum uric acid levels were determined,a significant increase was identified[41].Given the available data,no specific recommendation can be given for follow-up serum evaluation in a patient stable on directed medical therapy.Still,initial blood testing is useful upon initiation of directed medical therapy.
2.4.2.Follow-up imaging studies
Plain abdominal radiography,computed tomography(CT)imaging,ultrasound and digital tomography are all methods to monitor stone growth or new stone formation.The most common imaging modalities utilized in the included studies were kidney/ureter/bladder(KUB)X-ray,intravenous pyelogram(IVP)or renal ultrasound at intervals of 6-12 months to assess for stone activity,although this was mostly seen in RCTs performed in the 1980s and 1990s.The AUA Medical Stone Guidelines recommendations were fairly loose regarding suggestions for frequency of imaging studies,recommending yearly imaging for stable patients and tailoring the imaging regimen based on stone activity or clinical signs[13].
Renal ultrasonography is the preferred imaging modality for following patients,especially those with radiolucent stones.The advantages of ultrasound include avoiding exposure to ionizing radiation and a lower cost,although renal ultrasonography has an inferior specificity and sensitivity compared to other imaging modalities.Non-contrast CT,while more costly and carrying a higher radiation dose,has the greatest sensitivity and specificity of all the modalities listed[13].Choosing the best imaging procedure for follow-up must take into account specificity and sensitivity,cost,dose of radiation,availability of the service,risks of contrast and,in some cases,the need to assess other nonstone conditions with the same modality.The use of lowdose CT(around 2-4 mSv per study)is a valuable alternative,given the long-term side effects of ionizing radiation.Low-dose CT maintains a sensitivity and specificity of 90%among patients with a body mass index(BMI)<30 kg/m2and should be considered in cases where detailed anatomic information may not be a priority given the lower radiation dosage[42].
Follow-up KUB X-rays examination can be used as an indicator of stone activity identified on either CT scout or an initial KUB or if positioned in the sacroiliac area.Growth of pre-existing calculi on follow-up imaging can be difficult to identify with KUB X-ray alone.Digital tomosynthesis,a new technique which acquires a series of projections during a single sweep of the X-ray tube over a limited angle,may provide enhanced detection of radiopaque stones with much less radiation exposure(0.54 mSv)[43,44].This technique shows promise for the detection and follow-up of renal stones and proximal ureteral calculi.Using non-contrast CT as the standard,the sensitivity of digital tomosynthesis for detecting renal stones was compared to digital KUB.Expert readers had a significantly higher sensitivity using digital tomosynthesis over plain KUB(66%vs.24%),with the largest gain in sensitivity for stones 2-5 mm in size[43].Digital tomosynthesis also showed similar stone detection rates to noncontrast CT,without significant effect from stone size and BMI[44].
Finally,asymptomatic stones are commonly seen on various imaging studies,being responsible,at least in part,for epidemiologic estimates of the higher prevalence of nephrolithiasis[45].However,the need for follow-up of these patients,especially if calculi are small and non-obstructing,remains uncertain.Kang et al.[46]performed a retrospective analysis of medical records from 347 patients with asymptomatic renal stones,followed for 6-180 months.Of those patients,24.5%required intervention,29.1%passed their stones spontaneously.By 19 months after diagnosis,50%of the patients became symptomatic from their stone,calling into question the term“asymptomatic stone”.The authors concluded that long-term follow-up of stone formers is necessary and that a periodic evaluation should be recommended in patients with risk factors[41,47].
Although most experts recommend repeat assessment of stone-forming risk factors by performing 24 h urine collections,stone activity (defined as existing stone growth or new stone formation)can only be determined by follow-up imaging studies.We concur with previous investigations that imaging studies should be typically performed every 1-2 years,though the timing and type of imaging can be tailored based on stone activity,clinical signs/symptoms and stone location (renal or ureteral).Aside from kidney stone passage itself,imaging is the most sensitive way to gauge metabolic stone activity.
2.4.3.Compliance
The greatest challenge in following stone formers is the low compliance to conservative or selective medical recommendations,particularly dietary advice.The cost of medications can be highly variable and limiting for many patients.Such challenges are not unique to stone disease,and are also seen in chronic conditions such as hypertension,in which the symptoms are absent or few and far between[48].We suggest that the purpose of follow-up is,not only to assess the efficacy of treatment,but also to encourage patient compliance and ultimately reduce the risk of stone recurrence.In fact,studies have shown that patients who are followed long-term in a stone-focused medical clinic have lower stone recurrence rates and require fewer procedures[49].
3.Conclusion
Single and recurrent stone formers share many similarities in metabolic profiles.Based on an assessment of risk for stone recurrence and metabolic activity,the single and recurrent stone formers should be evaluated comprehensively,including two 24 h urine studies on a random diet.Targeted medication and dietary advice is effective for many patients in reducing the risk of stone recurrence.Follow-up of those with stone disease should be obtained depending on the level of metabolic activity of the patient,the risk of CKD and the risk of osteoporosis/osteopenia.A standard regimen includes a baseline metabolic profile,a repeat study 3-6 months after initiation of treatment(and then yearly when stable)with abdominal imaging obtained every 1-2 years and BMD in osteoporotic/osteopenic patients(Fig.1).
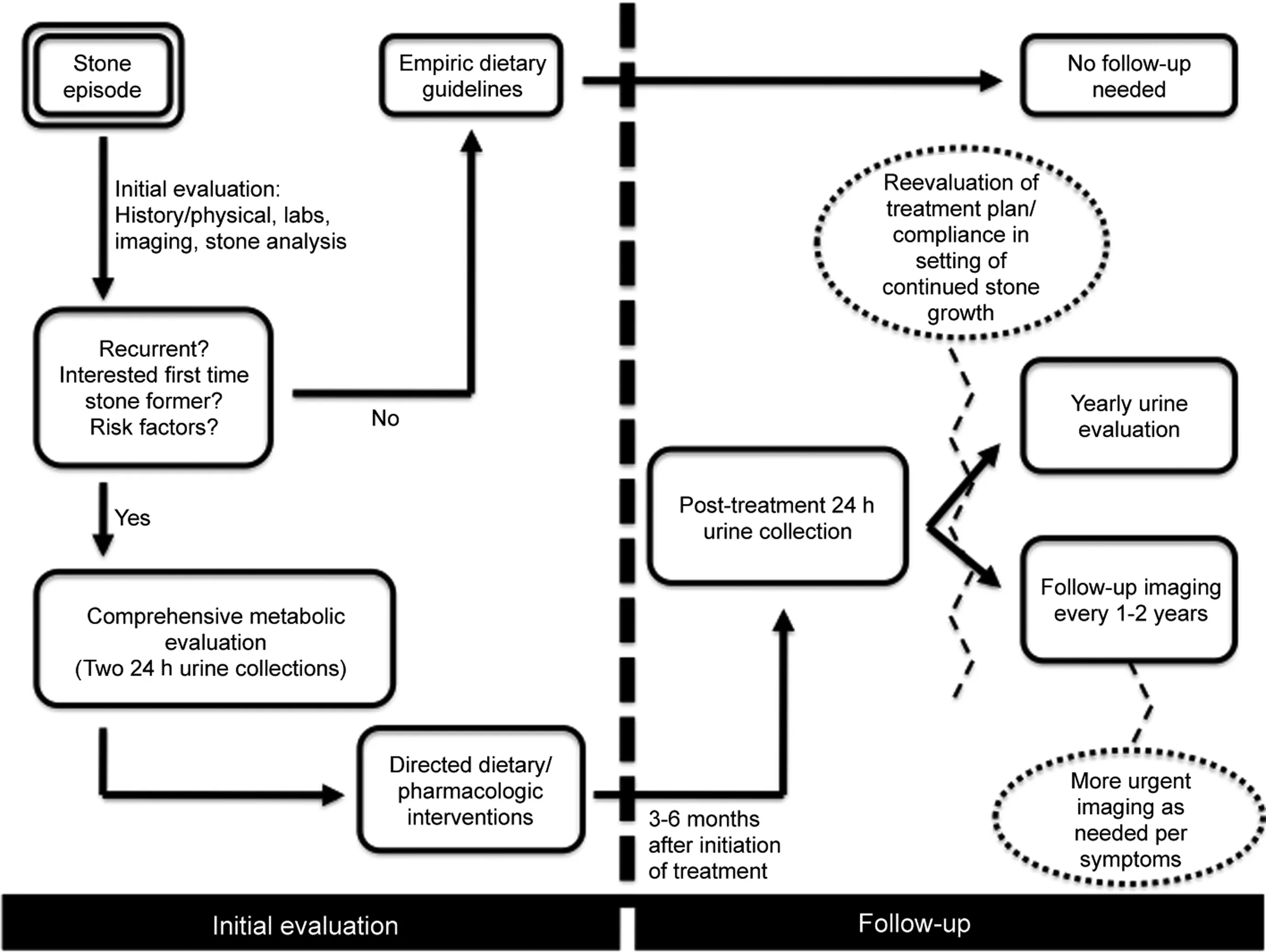
Figure 1 Consensus algorithm for stone evaluation and follow-up.
Author contributions
Study design:Glenn M.Preminger,Pietro Manuel Ferraro,Antonio Nouvenne,Andrea Tasca,Emanuele Croppi,Giovanni Gambaro,Ita P.Heilberg.
Data acquisition:Daniel A.Wollin,Adam G.Kaplan,Glenn M.Preminger,Pietro Manuel Ferraro,Antonio Nouvenne,Andrea Tasca,Emanuele Croppi,Giovanni Gambaro,Ita P.Heilberg.
Data analysis:Daniel A.Wollin,Adam G.Kaplan,Glenn M.Preminger,Pietro Manuel Ferraro,Antonio Nouvenne,Andrea Tasca,Emanuele Croppi,Giovanni Gambaro,Ita P.Heilberg.
Drafting of manuscript:Daniel A.Wollin,Adam G.Kaplan,Glenn M.Preminger.
Critical revision of the manuscript:Daniel A.Wollin,Adam G.Kaplan,Glenn M.Preminger,Pietro Manuel Ferraro,Antonio Nouvenne,Andrea Tasca,Emanuele Croppi,Giovanni Gambaro,Ita P.Heilberg.
Conflicts of interest
This article is based on the results of the“Consensus Conference for the metabolic diagnosis and medical prevention of calcium nephrolithiasis and its systemic manifestations”,Rome on March 26-28,2015 which was generously supported by International Foundation Menarini,Milan,Italy with an unrestricted grant.
 Asian Journal of Urology2018年4期
Asian Journal of Urology2018年4期
- Asian Journal of Urology的其它文章
- Miniaturised percutaneous nephrolithotomy:Its role in the treatment of urolithiasis and our experience
- Present indications and techniques of percutaneous nephrolithotomy:What the future holds?
- Ureteral stents in urolithiasis
- Retrograde intrarenal surgery:An expanding role in treatment of urolithiasis
- Indications and contraindications for shock wave lithotripsy and how to improve outcomes
- Medical therapy for nephrolithiasis:State of the art