
Survey and analysis of patient safety culture in a county hospital
2018-01-08 09:25:13XingxingZhaoWeiweiLiuYuanyuanWangLiZhang
Xingxing Zhao, Weiwei Liu, Yuanyuan Wang, Li Zhang
1. The Second Outpatient Department, Peking University Third Hospital, Beijing 100096, China
2. Peking University Third Hospital Yanqing Hospital, Beijing 102100, China
Survey and analysis of patient safety culture in a county hospital
Xingxing Zhao1, Weiwei Liu1, Yuanyuan Wang1, Li Zhang2
1. The Second Outpatient Department, Peking University Third Hospital, Beijing 100096, China
2. Peking University Third Hospital Yanqing Hospital, Beijing 102100, China
Objective:This study aimed to survey patient safety culture in a county hospital and to provide evidence for strategies to improve patient safety culture.Methods:Nine hundred and thirty-two medical staff in a county hospital were surveyed with use of the Hospital Survey on Patient Safety Culture. Information was analyzed by one-way ANOVA and multiple linear regression analysis.Results:Nine hundred and thirty-two questionnaires were distributed, of which 661 of those returned were valid. The subscale-level results showed that the positive response rate for “teamwork across units” was higher than 75.0%, indicating it was an area of strength. Five areas — “nonpunitive response to error,” “staffing,” “communication openness,” “overall perceptions of patient safety,” and “frequency of event reporting” — had potential for improvement, with a positive responsive rate lower than 50%. Twenty-nine percent of respondents gave their work area a patient safety grade of “excellent” or “very good.” Further, 60.1% of respondents had reported no event in the previous 12 months. Multiple linear regression analysis indicated that position and number of years working in this hospital were the factors influencing patient safety culture.Conclusion:Patient safety culture in the county hospital has potential for improvement,especially in the areas of “nonpunitive response to error,” “staffing,” “overall perceptions of patient safety,” “communication openness,” and “frequency of event reporting.”Statement of Significance:It has been recognized for almost 20 years that safety culture is important in ensuring high-quality and safe care. This article describes the results of a patient safety culture survey undertaken in one Chinese county hospital, which distributed the Hospital Survey on Patient Safety Culture to 932 health care staff. It reaffirms that there is still a long way to go until hospitals have successfully established positive safety cultures. In terms of relevance, we believe the findings will be most useful to the hospital where the study was undertaken. Many of the recommendations in the discussion should be useful for the hospital.
Patient safety; safety culture; primary health care
Introduction
Patient safety is a serious global public health issue and one of the most important parts of health care. According to the World Health Organization, one in ten patients may be harmed when receiving hospital care, and about half of these injuries are thought to be preventable[1], and 14 in every 100 patients admitted have been affected by hospital infections [2].The reportTo Err Is Humanpublished by the Institute of Medicine [3] in 1999 highlighted the role of developing the patient safety culture of hospitals in building a safer health system. Patient safety culture was first determined by Singer et al. [4]; it refers to “the product of individual and group values, attitudes, competencies and patterns of behavior that determine the commitment to, and the style and proficiency of, an organization’s health and safety programs.” Related research showed that positive patient safety culture can improve patient outcomes,such as readmission rate reduction and hospital infection rate decrease [5, 6]. Patient safety culture is a strategy for improving patient safety.
Many studies on patient safety culture have been conducted since then, with focuses on developing assessment tools, patient safety culture assessment, and influential factors.The Hospital Survey on Patient Safety Culture (HSOPSC)developed by the Agency for Healthcare Research and Quality(AHRQ) in 2004 has been widely used around the world [7],as have the Safety Attitudes Questionnaire developed by the University of Texas in 2000 [8], the Patient Safety Climate in Healthcare Organizations developed by Singer et al. [9]in 2003, and the Manchester Patient Safety Framework [10].Interventions such as executive walk rounds or interdisciplinary rounds, multicomponent unit-based interventions, team training, and communication initiatives have been confirmed as positive for patient safety culture improvement [11, 12].
Studies on patient safety culture started late in China,but their number has been growing fast recently [12, 13].However, little attention has been devoted to patient safety culture of the primary health care system, and most studies on patient safety culture were conducted in large hospitals [13].According toThe Rural Health Service System Construction and Development Planningpublished by China’s Ministry of Health, a second-class comprehensive hospital, such as the county hospital — the head of the primary health care system in China — is responsible for training and technical guidance in primary health care. The primary health care system has also been emphasized in health care reform in the 13th Five-Year Plan of the Chinese government [14]. Studies showed that patient safety was a weak point in primary health institutions,which is also an impediment for improvement of the capabilities of primary health care services [15]. The main objective of this study was to use the HSOPSC to survey patient safety culture in one county hospital in Beijing, from which the strengths and weaknesses of patient safety culture in this hospital could be determined.
Methods
Participants and data collection
The data in this study were obtained from the survey conducted in a county hospital in Beijing from July to December 2014. The survey encompassed all health care workers(physicians, nurses, and allied health professionals) in the county hospital. Questionnaires were distributed by the Department of Science and Education of the hospital. To protect the privacy of respondents, the survey was strictly anonymous. Health care workers who completed and submitted the questionnaires were considered to agree to participate in the survey. Nine hundred thirty-two questionnaires were administered, of which 680 were answered, the response rate being 73.0%. From these, questionnaires with data missing(missing value ≥20%), filled out incorrectly, or not submitted in the effective period were excluded, and the final sample consisted of 661 participants.
The questionnaire
The HSOPSC instrument developed by the AHRQ was used in this study [7]. The HSOPSC has been widely used to assess patient safety culture in a number of countries [16].It was translated into Chinese by one translator with a background in safety research and reviewed by a task group. T he HSOPSC has been used in many hospitals in China, and the reliability expressed as Cronbach’s α for a study in Taiwan ranged from 0.51 to 0.84 [17], whereas Cronbach’s α was 0.889 for a study on the Chinese mainland. It includes 42 items that measure 12 subdimensions of patient safety culture, two items that measure patient safety culture outcome,and seven items that survey demographic characteristics of the participants.
The subdimensions of patient safety culture consisted of (1)communication openness, (2) feedback and communication about errors, (3) frequency of event reporting, (4) hospital handoffs and transitions, (5) hospital management support for patient safety, (6) nonpunitive response to error, (7) organizational learning — continuous improvement, (8) overall perceptions of safety, (9) staffing, (10) supervisor/manager expectations and actions promoting safety, (11) teamwork across hospital units,and (12) teamwork within hospital units. Each subscale consists of three or four questions. Each item uses a Likert scale of five-point response options to represent the degree of agreement(1 for strongly disagree to 5 for strongly agree) or frequency(1 for never to 5 for always), and negatively worded items were reversely scored. For each subdimension the proportion of positive responses (percent positive score) was calculated for every participant on the basis of the AHRQ instructions, and it ranged from 0 to 1. The patient safety strength of the hospital is defined as those dimensions with more than 75.0% of respondents answering “strongly agree”/“agree” or “always”/“most of the time.” Areas needing improvement were identified as those dimensions for which 50.0% of respondents or fewer did not answer positively. A composite score was calculated for each respondent, relative to each of the 12 safety culture dimensions,and it ranged from 1.0 to 5.0. Higher scores indicate a more positive patient safety culture.
Questions related to the patient safety culture outcome measures included a question on patient safety grade that asked participants to provide an overall grade on patient safety in their respective departments (“excellent,” “very good,”“acceptable,” “fair,” and “failing”) and a question on the number of events that asked participants to provide the number of events they had reported during the previous 12 months (1 for no events to 5 for 21 or more events).
The demographic characteristics included age, sex, profession, educational background, direct interaction with patients,number of years in the hospital, and number of hours of work per week.
Data processing
This study used Epidata 3.0 for data entry, and SPSS for Windows version 16.0 to perform the statistical analysis. We obtained descriptive statistics on the demographic characteristics of participants, and the percentage of positive responses for HSOPSC dimensions. The percentage of respondents who gave their work area/unit a patient safety grade and the number of error reports generated during the previous 12 months were also summarized.
The relationship between demographic factors and patient safety culture outcome measures (including a patient safety grade and the number of events reported during the previous 12 months) was examined by one-way ANOVA.
The relationship between demographic factors and patient safety culture (total score and 12 dimension scores)was examined by one-way ANOVA and multiple linear regression analysis. The multivariate regression analysis adopted a stepwise approach using entrance/exit tolerance of 0.05/0.10.
Ethical concerns
The survey was approved by the Health Science Ethic Committee of Peking University Third Hospital.
Results
Respondent characteristics
Among the 661 questionnaires, 32.2% of the respondents were physicians, 46.0% were nurses, and the remainder were other health care workers. Most of the respondents (72.5%)were female, and more than half were younger than 35 years(53.4%). Most of the respondents (86.5%) had direct interaction with patients. Only 19.2% of the respondents had worked in the hospital for more than 10 years, while 30.3% had worked there for less than 5 years. About 90% of the respondents worked more than 40 h per week.
Overall safety culture and influencing factors
The percentage of positive responses to all dimensions ranged from 15.7% to 79.2% (see Table 1). The highest positive response rate was for “teamwork across hospital units”(79.2%), which was also the only strength area of this hospital (positive response rate >75.0%). The five lowest positive response rates were for “overall perceptions of safety”(45.0%), “frequency of event reporting” (43.0%), “communication openness” (27.4%), “staffing” (25.9%), and “nonpunitive response to error” (15.7%), all of which were areas needing improvement.
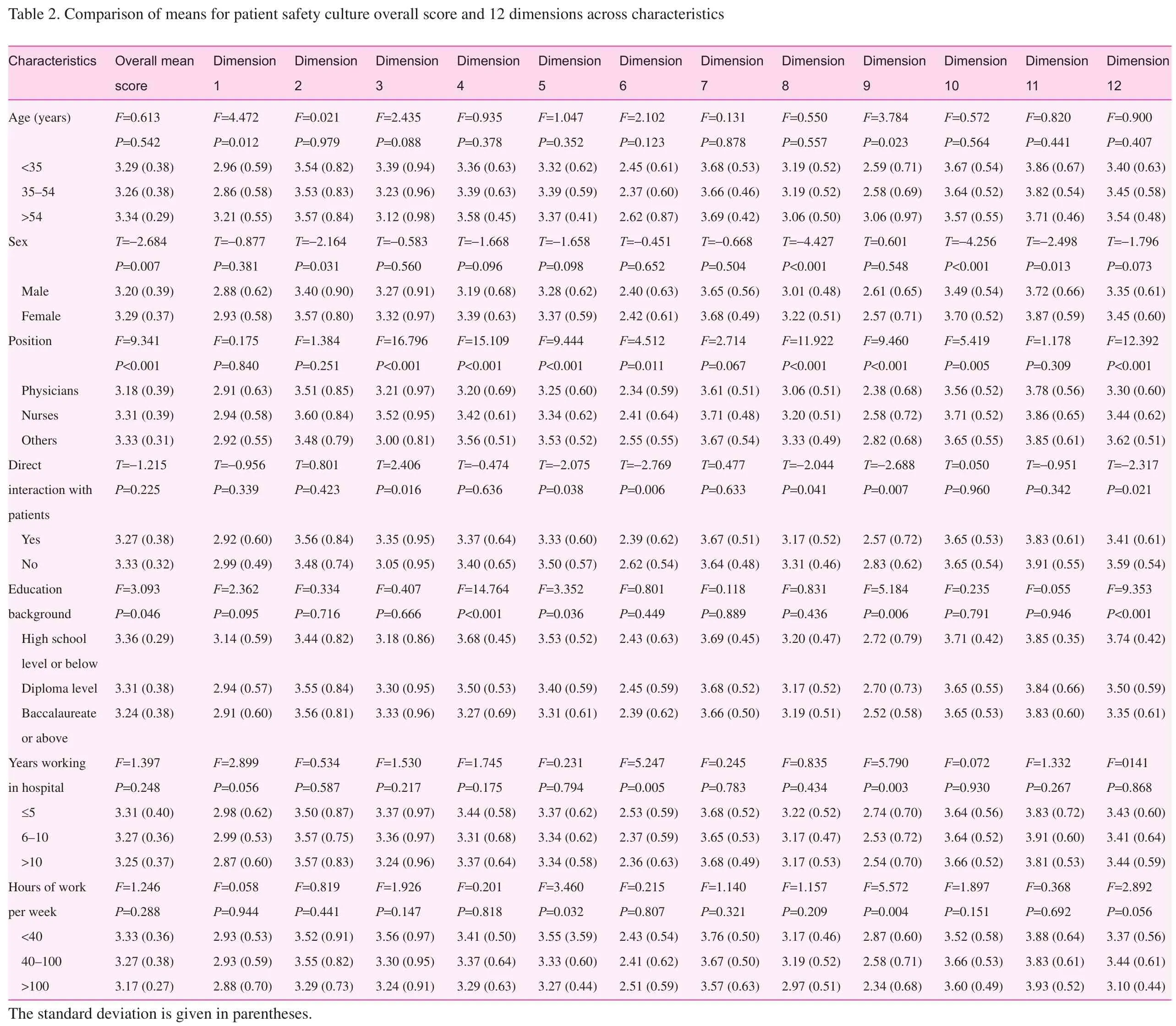
ANOVA indicated that the overall mean score of patient safety culture varied for different positions, educational background, and sex (P<0.05). There was also a significant difference in profession, educational background, and direct interaction with patients across multiple dimensions (see Table 2).

Table 1. Distribution of patient safety culture dimension positive responses
In the multivariate regression analysis, the dependent variables were the mean scores for each of the HSOPSC dimensions and the overall mean score. Demographic factors were tested as independent variables. Sex and direct interaction with patients were entered as a dichotomous variable, with male and direct interaction with patients, respectively, as reference categories. Profession was entered as a dummy variable, with other positions (other than physicians and nurses) as reference categories. Age, sex, number of years in the hospital, and number of hours of work per week were entered as classification variables (see assignment in Table 3). The 12 dimensions were entered in the model as continuous variables. The results of multivariate regression analysis are shown in Table 4. Multivariate regression analysis indicated position was the influencing factor for the patient safety culture overall mean score, and physicians were associated with a lower patient safety culture overall mean score than nurses and other health care workers. For “communication openness,” a greater number of years working in the hospital was associated with a low score. For “frequency of event reporting,” position and sex were influencing factors. Men had a higher score than women,and physicians and nurses had higher scores than other health care workers. More years working in the hospital and being a physician or a nurse were associated with a lower score for“nonpunitive response to error.” For “overall perceptions of safety,” position and sex were influencing factors. Women had a higher score than men, and physicians and nurses had a lower score than other health care workers. Older age, more years working in the hospital, more hours of work per week,and being a physician or a nurse were associated with a lower“staffing” score.
Patient safety grade and influencing factors
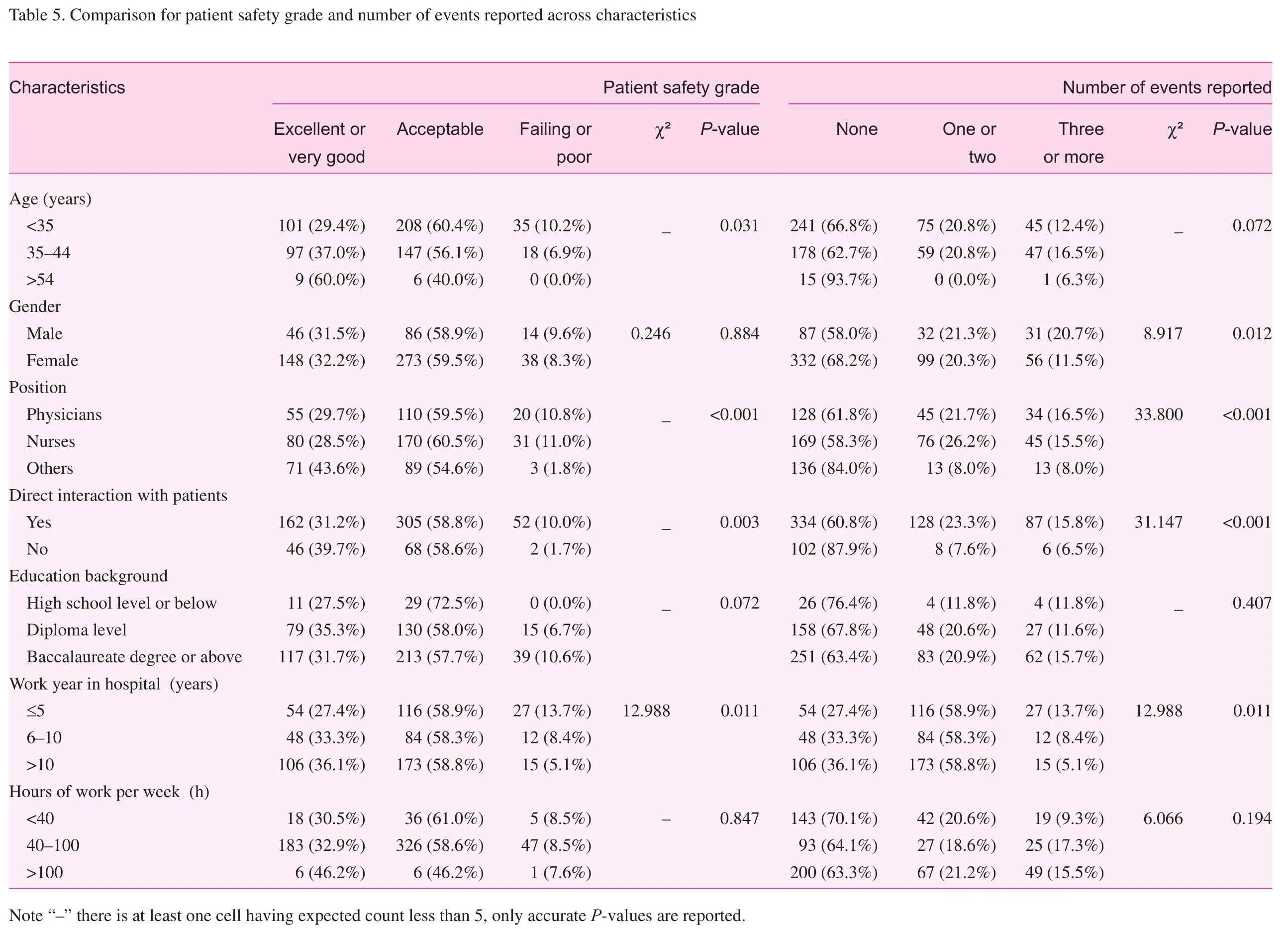
Six hundred staff (90.1%) assessed the overall patient safety.Twenty-nine percent of the respondents assessed patient safety as excellent or very good, 53.4% as acceptable, and 8.3% as failing or poor. Further analysis was conducted with the χ2test and Fisher exact test to indicate possible influencing factors.Statistical analysis showed that there was a significant difference in ages, positions, years worked in hospital and whether there had been direct contact with patients (P<0.05) (see Table 5).
Number of events reported and influencing factors
Six hundred twenty-seven health care workers (94.9%)answered this item: 60.1% of the respondents had not reported at least one adverse event or near-miss event during the previous 12 months, 20.6% of the respondents had reported one or two events, whereas only 2.7% of the respondents had reported more than ten events. χ2test and Fisher exact test showed that the number of events reported during the previous 12 months differed for different positions, gender, years worked in hospital and whether there had been direct contact with patients(P<0.05) (see Table 5).
?
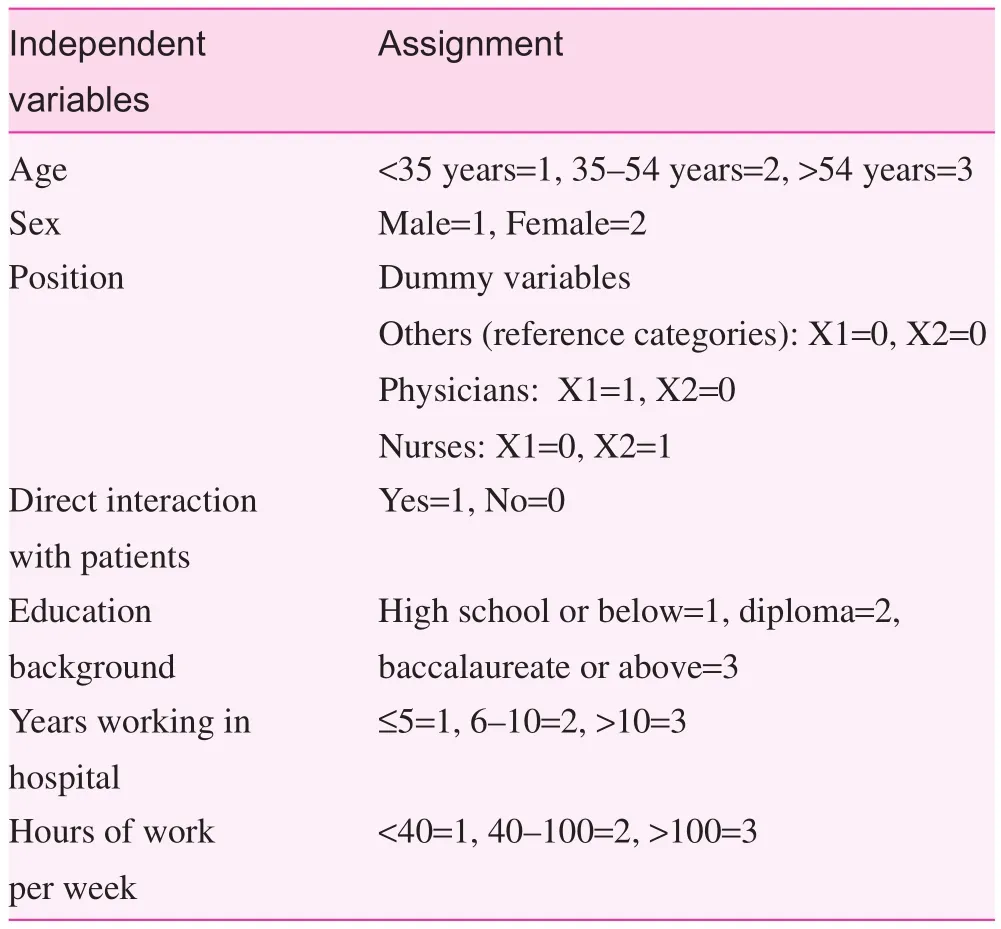
Table 3. Multiple linear regression assignment
Discussion
Patient safety and patient safety culture in a county hospital in China need to be improved
Twenty-nine percent of the respondents were assessed as“good” or “excellent” in this study, meanwhile, 54.4% of the health care workers assessed patient safety as “good” or“excellent” in a survey performed in six public second-class comprehensive hospitals in Hangzhou in 2015 by Zhang [18].Seventy-one percent of the health care workers in third-class comprehensive hospitals in Beijing assessed patient safety as“good” or “excellent” in a survey performed by Liang [19] in 2014. Among health care workers in Anhui province, 66.2% of whom assessed patient safety as “good” or “excellent” in a survey performed by Lu et al. [20]. In addition, a study performed by Tabrizchi and Sedaghat [21] in 2012 regarding Iranian primary health centers showed that 67% of the respondents graded patient safety as “good” or “excellent,” while the rate was 70.8% in the United States and 44.6% in Japan [22].
With regard to areas of strength and areas needing improvement, our study identified one area of strength (“teamwork across hospital units”) and five areas needing improvement in this county hospital, while a study on public second-class comprehensive hospitals in Hangzhou defied two areas of strength and four areas in need of improvement [18], and Chen and Li [23] identified three areas of strength and three areas needing improvement in 42 teaching hospitals in Taiwan.In other countries or regions around the world, the study by Tabrizchi and Sedaghat [21] showed that an Iranian primary health center had two areas of strength areas and three needing improvement [21]. According to an investigation by Danielsson et al. [24] involving all Swedish hospitals, there was no area of strength area of patient safety in Swedish hospitals, while there was only one area needing improvement.
From the preceding discussion, a conclusion can be reached that patient safety and patient safety culture in the county hospital investigated need to be improved overall, especially in comparison with other second-class and third-class comprehensive hospitals in China and hospitals around the world. It should not be ignored that such a comparison has to be made with caution, and a better comparison would be achieved with the same hospital over a longer time.
Areas of strength
Our results show that “teamwork across hospital units” was the only area of strength of patient safety culture in this county hospital, whereas previous studies found that the positive response rate for this dimension was not higher than 75.0%[20], even needing improvement in a third-class comprehensive hospital [25]. This may be related to the size of this county hospital, which may be advantageous in unit management. At the same time, in this hospital, staff members across units are urged to develop and maintain friendly relationships and teamwork.
Areas needing improvement
Four of five areas needing improvement (overall perceptions of safety, frequency of event reporting, communication openness, staffing, and nonpunitive response to error) are the same as those in most previous studies around the world [20, 22,26—28]. The area needing the least improvement is “overall perceptions of safety” (positive response rate of 45.0%), which indicates that patient safety culture perceptions of health care workers in this county hospital need to be improved. This result is similar to that in the study performed by Hao [29] in a county hospital in Beijing in 2013, but different from thoseof most other studies performed in third-class comprehensive hospitals in China, where it was an area of strength [20].Only clinicians and allied health professionals with good perceptions of patient safety can be aware of the importance of patient safety culture improvement, and then promote patient safety and quality.
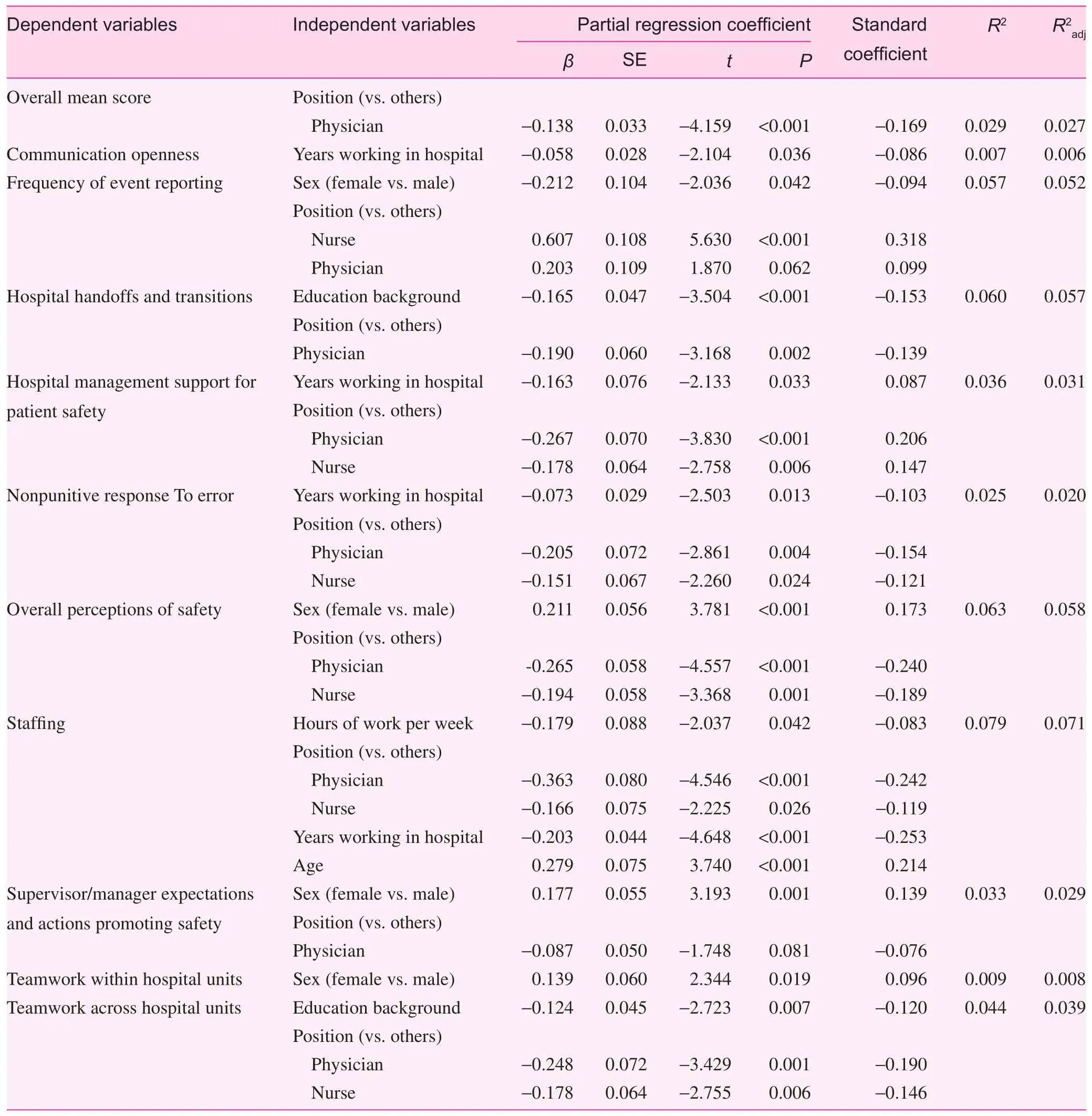
Table 4. Multiple linear regression results for patient safety culture
Patient safety culture education is considered to be an important intervention in improving patient safety and patient safety culture perceptions of health care workers. The importance of this intervention is also acknowledged by the World Health Organization, which developed thePatient Safety Curriculum Guideto guide and support educators to implement educational programs in patient safety [30]. Moreover, to improve culture and safety, Pronovost et al. [31] developed the six-step Comprehensive Unit-Based Safety Program in which safety culture is the first step and education is the second [31].According to a study performed by Chai and Wang [32] in 2014, nursing students’ safety culture knowledge and awareness of adverse events increased after they had received safety culture education. Safety culture training was implemented for nursing managers from ten second-class comprehensive hospitals for 1 month by Xie [33]. The results showed that safety culture training was effective in enhancing perceptions of patient safety culture among nursing managers of the second-class comprehensive hospitals and reducing the incidence of adverse events. Therefore patient safety culture education and training should be implemented regularly for health care workers in county hospitals. According to previous studies, a program that is unit-based, case-based, and a combination of theory and clinical practice would have a better effect [34]. Meanwhile,use of the HSOPSC to measure safety culture before and after intervention and collection of feedback are also indispensable.
Need to build a nonpunitive culture, and perfect the event reporting system
The area of adverse event reporting performed poorly in most of the previous studies on patient safety culture in China [19,28]. The positive response rate for the frequency of event reporting in this study was 43.0%, and 60.6% of the respondents had not reported at least one adverse event or near-miss event in the previous 12 months, while the proportions in Japan were 68.0% and 36.0% respectively [22]. The following reasons may explain the unreported events. Firstly, with poor perceptions of patient safety and patient safety culture(positive response rate for overall perceptions of safety of 45.0%), health care workers in this hospital were not sensitive to adverse events, which would lead them to be unconscious of the importance and necessity of adverse event reporting.
Secondly, absence of a nonpunitive culture in this hospital should also contribute to unreported events. The positive response rate for nonpunitive response to error in this study was the lowest of the 12 dimensions (15.7%), and this means that this county hospital pays more attention to punishing health care workers than the error itself when an error happens. According to the culture of the hospital, we conjectured that adverse events were considered as a result of incompetent performance of the health care workers involved. So, because of concern about performance appraisal, health care workers would not report adverse events proactively, especially an error that was caught and corrected before affecting the patient, and that has no potential to harm the patient, and that could harm the patient but does not. A penalty culture and a blaming culture are popular in the health care system. Surprisingly, some researchers have even thought that punishment should be intensified to warn physicians to make no errors [35]. By using the Safety Attitudes Questionnaire, Li et al. [36] surveyed 54 public hospitals in the central and western regions of China. The scores for “fear of blame and punishment” and “fear of shame”were among the lowest scores [37]. A survey performed by Hao [29] in a county hospital in Beijing also indicated the area “nonpunitive response to error” as needing improvement.Similar results were obtained in Japan, the United States, and Iran. In 1999 the Institute of Medicine pointed out that a significant percentage of errors in health care are caused by the system rather than individuals [3]. Studies had already confirmed that after removal of the punishment mechanism, a significant increase in the rate of errors in health care was reported [38].In conclusion, forming a nonpunitive culture in a hospital is essential to promote event reporting and safety culture.
Thirdly, the medical adverse event reporting system of this county hospital needs to be improved. The county hospital had set up a medical/accident reporting system and a management system for nursing adverse events, and the medical service is responsible for implementing the systems. Medical disputes refer to disputes arising from medical treatment,between medical institutions and patients or close relatives,and resulting from different perceptions of treatment plans and outcomes. “Major medical accident” and “critical medical negligence” are defined by the National Health and Family Planning Commission of the People’s Republic of China as an event that happened when a health care worker was in violation of medical and health management laws or rules, and caused injury to patient. These rules resulted in errors that did not cause patients to be dissatisfied or that were not defined as fatal errors in health care being ignored. Measures to encourage physicians to report errors proactively were also missed. In addition, the manager of the medical service may not be fully aware of learning from errors, so adequate feedback of errors was also missed, needless to say collected and systematically analyzed errors, which could be used to identify hidden hazards for improving patient safety. A possible explanation for the high rates of adverse events or near-miss events is that all Japanese hospitals established an in-house, legally binding event reporting system in 2002 [22]. Britain and the United States have also established a nationwide adverse event reporting system and root cause analysis of adverse events [39].
Hence building a universal, unobstructed, nonpunitive,complete reported adverse events analysis and feedback system, where health care workers report errors without fear of punishment and can learn from errors, is highly recommended and essential.
It is important to note that although an incident reporting system and root cause analysis are promising approaches to improve patient safety, there are limitations with them, such as lack of proper taxonomy and two-way engagement in the incident reporting system, questionable quality, and unsatisfactory production of risk controls in root cause analysis. So more professional investigation, learning, and sharing within and across organizations should also be taken into account in the process of establishing an incident reporting system and root cause analysis [40, 41]. In addition, some researchers have suggested that we should learn from everyday clinical work instead of learning from incidents only, while the former can motivate staff to contribute to improving patient safety [42, 43].
Implementing different interventions for different groups
The results of multivariate regression analysis showed that physicians had lower scores in many dimensions (overall perceptions of safety, supervisor/manager expectations and actions promoting safety, hospital handoffs and transitions,hospital management support for patient safety, and nonpunitive response to error) and overall mean score of patient safety culture, which is consistent with several previous studies [44].The possible reasons are as follows: First, nurses had contact with patients more frequently than physicians, which led them to identify patient safety problems more easily, and at the same time they gained more experience. Second, the nursing department manager paid more attention to patient safety education,related regulations, and evaluation of patient safety culture than physicians. Third, a review by Mao et al. [13] showed that more attention to patient safety had been paid in the nursing field than in other medical fields in China in the previous 10 years, including patient safety culture assessment, assessment tool development, and interventions such as education and manager walkaround [13]. All of these indicate that interventions should be implemented with more focus on physicians, especially in safety culture education and management support.
Our findings also show that respondents who worked longer had lower scores in several dimensions (staffing, nonpunitive response to error, and communication openness),which is contrary to the findings of previous studies [45]. A possible reason is that health care workers who work longer are more experienced, with more critical thinking, and have greater awareness of patient safety culture. Taking the opinions of these staff members into account when interventions are being implemented may be a good idea.
Limitation
There are several limitations in our study. First, as quantitative research, a questionnaire survey cannot fully assess safety culture for it is a multicultural, comprehensive concept. More qualitative research is encouraged. Second, 932 staff members in only one county hospital were surveyed, and safety culture needs to be surveyed in more county hospitals. Third, this study is a cross-sectional study, so the influencing factors need to be verified in research on interventions for improvement of patient safety culture.
Conclusion
According to our survey, the overall patient safety and patient safety culture of this county hospital need to be improved,especially in areas of potential for improvement such as“overall perceptions of safety,” “frequency of event reporting,” “communication openness,” “staffing,” and “nonpunitive response to error.” The area of strength is “teamwork across hospital units,” which the hospital should maintain. According to the multivariate regression analysis results, we recommend that a nonpunitive culture should be developed and a smooth,perfect event reporting system should be established. In addition, patient safety and patient safety culture are also important and essential to health care workers in this county hospital,especially to physicians. A further study should be performed on interventions for improving safety culture.
The authors are grateful to the managers and health care workers in the county hospital who participated in the survey.
Conflict of interest
The authors declare no conflict of interest.
Funding
The research was supported by the China-US Center for Medical Professionalism funded by Peking University Health Science (PUHSC-MPC1302).
Author contributions
Xingxing Zhao analyzed the data and drafted the manuscript.
Weiwei Liu led to the design, organization, implementation and data collection of the study.
Yuanyuan Wang guided statistical analysis and article modifications.
Li Zhang carried out the data collection infield.
All authors read and approved the final manuscript.
1. Baker GR, Norton PG, Flintoft V, Blais R, Brown A, Cox J, et al.The canadian adverse events study: the incidence of adverse events among hospital patients in Canada. Can Med Assoc J 2004;170:1678—86.
2. World Health Organization. 10 facts on patient safety. www.who.int /features/factfiles/patient safety/en/index.html. 2014.
3. Institute of Medicine. To err is human: building a safer health system. Washington: National Academics Press; 1999.
4. Singer SJ, Gaba DM, Geppert JJ, Sinaiko AD, Howard SK,Park KC, et al. The culture of safety: results of an organizationwide survey in 15 California hospitals. Qual Saf Health Care 2003;12(2):112—8.
5. Mardon RE, Khanna K, Sorra J, Dyer N, Famolaro T. Exploring relationships between hospital patient safety culture and adverse events. J Patient Saf 2010;6(4):226—32.
6. Hansen LO, Williams MV, Singer SJ. Perceptions of hospital safety climate and incidence of readmission. Health Serv Res 2011;46(2):596—616.
7. Nieva VF, Sorra J. Safety culture assessment: a tool for improving patient safety in healthcare organizations. Qual Saf Health Care 2003;12(Suppl 2):i17—23.
8. Sexton JB, Helmreich RL, Neilands TB, Rowan K, Vella K,Boyden J, et al. The Safety Attitudes Questionnaire: psychometric properties, benchmarking data, and emerging research. BMC Health Serv Res 2006;6:44.
9. Singer S, Meterko M, Baker L, Gaba D, Falwell A, Rosen A.Workforce perceptions of hospital safety culture: development and validation of the patient safety climate in healthcare organizations survey. Health Serv Res 2007;42(5):1999—2021.
10. Ashcroft DM, Morecroft C, Parker D, Noyce PR. Safety culture assessment in community pharmacy: development, face validity, and feasibility of the Manchester Patient Safety Assessment Framework. Qual Saf Health Care 2005;14(6):417—21.
11. Kirkman MA, Sevdalis N, Arora S, Baker P, Vincent C, Ahmed M. The outcomes of recent patient safety education interventions for trainee physicians and medical students: a systematic review.BMJ Open 2015;5(5):e7705.
12. Morello RT, Lowthian JA, Barker AL, McGinnes R, Dunt D,Brand C. Strategies for improving patient safety culture in hospitals: a systematic review. BMJ Qual Saf 2013;22(1):11—8.
13. Mao X, Nie Y, Cui H, Jia P, Zhang M. Literature review regarding patient safety culture. J Evid Based Med 2013;6(1):43—9.
14. The State Council of the People’s Republic of China. Health and hygiene planning of the 13th Five-Year Plan. 2016.
15. Liu LQ. Improving capacities of health services delivery: the key to the sustainable development of grass-roots medical service system. Chin Gen Pract 2017;20(4):379—82.
16. Bodur S, Filiz E. Validity and reliability of Turkish version of“Hospital Survey on Patient Safety Culture” and perception of patient safety in public hospitals in Turkey. BMC Health Serv Res 2010;10:28.
17. Li L, Liu X. Analysis of nurses’ assessment of the patient safety culture in hospital. Chin J Nurs 2009;44(4):304—7.
18. Zhang X. An analysis of perception and impacting factors of patient safety culture in medical staffs among public medi-cal institutions in Hangzhou. Hangzhou: Hangzhou Normal University; 2016.
19. Liang S. Hospital Survey on patient safety culture in tertiary general hospitals in Beijing. Beijing: Peking Union Medical College;2014.
20. Lu C, Ji F, Wang Z, Wang Y, Zhang W. Study on patients’ safety culture cognition of medical staff in 3A hospital, Anhui. Chin Health Serv Manage 2016;(10):739—42.
21. Tabrizchi N, Sedaghat M. The first study of patient safety culture in Iranian primary health centers. Acta Med Iran 2012;50(7):505—10.
22. Fujita S, Seto K, Ito S, Wu Y, Huang CC, Hasegawa T. The characteristics of patient safety culture in Japan, Taiwan and the United States. BMC Health Serv Res 2013;13:20.
23. Chen IC, Li HH. Measuring patient safety culture in Taiwan using the Hospital Survey on Patient Safety Culture (HSOPSC).BMC Health Serv Res 2010;10:152.
24. Danielsson M, Nilsen P, Rutberg H, Arestedt K. A national study of patient safety culture in hospitals in Sweden. J Patient Saf 2017. doi:10.1097/PTS.0000000000000369.
25. Zhang Q, Zhang J, Liu L, Wei X. Evaluation and analysis of the patient’s safety culture status by staffs in a hospital. Nurs J Chin PLA 2015;32(14):49—52.
26. Deng X, Xi X, Cui Y, Zhang J, Feng J. Comparison of patient safety culture among departments. Chin Health Serv Manage 2016;(2):99—102.
27. Verbakel NJ, Van Melle M, Langelaan M, Verheij TJ, Wagner C,Zwart DL. Exploring patient safety culture in primary care. Int J Qual Health Care 2014;26(6):585—91.
28. Liu C, Liu W, Wang Y, Zhang Z, Wang P. Patient safety culture in China: a case study in an outpatient setting in Beijing. BMJ Qual Saf 2014;23(7):556—64.
29. Hao J. An analysis of perception of patient safety culture in medical staffs in primary hospitals. Cap Med 2013;(16):31—2.
30. World Health Organization. Patient safety curriculum guide:multi-professional edition. Geneva, Switzerland: World Health Organization; 2011.
31. Pronovost PJ, King J, Holzmueller CG, Sawyer M, Bivens S,Michael M, et al. A web-based tool for the Comprehensive Unit-Based Safety Program (CUSP). Jt Comm J Qual Patient Saf 2006;32(3):119—29.
32. Chai X, Wang L. The practice and effects of safety culture education among nursing students in clinical practice. Chin J Nurs Educ 2014;12:927—30.
33. Xie J. Study on effect of safety culture training on enhancing perceptions of patient safety culture among nursing managers of the 2nd Hospital. Changsha: Central South University; 2014.
34. Halligan M, Zecevic A. Safety culture in healthcare: a review of concepts, dimensions, measures and progress. BMJ Qual Saf 2011;20(4):338—43.
35. Gu Z, Wu W. The application of ticket in control medical documents error. Hosp Manage Forum 2010;7(6):28—31.
36. Li M, Tang H, Wei X, Zhou P, Xue D. Status of patient safety in public hospitals in China. Chin Hosp Manage 2017;37(1):11—3.
37. Xu W. The application of root cause analysis in nursing safety management. J Nurs Train 2008;23(5):414—6.
38. Vincent CA. Analysis of clinical incidents: a window on the system not a search for root causes. Qual Saf Health Care 2004;13(4):242—3.
39. Macrae C. The problem with incident reporting. BMJ Qual Saf 2016;25(2):71—5.
40. Peerally MF, Carr S, Waring J, Dixon-Woods M. The problem with root cause analysis. BMJ Qual Saf 2017;26(5):417—22.
41. Sujan M. An organisation without a memory: a qualitative study of hospital staff perceptions on reporting and organisational learning for patient safety. Reliab Eng Syst Saf 2015;144:45—52.
42. Sujan MA, Huang H, Braithwaite J. Learning from incidents in health care: critique from a safety-II perspective. Saf Sci 2016.doi:10.1016/j.ssci.2016.08.005.
43. Peng L, Fu L. Survey and analysis on cognition on patients’safety culture of medical staff from primary level general hospital. Nurs Rehabil J 2015;14(2):114—8.
44. Song Z. Study on nurses’ intention of reporting adverse events and its related factors analysis and intervention in tertiary hospital in Liuzhou. Nanning: Guangxi Medical University; 2014.
45. Feng X, Bobay K, Krejci JW, McCormick BL. Factors associated with nurses’ perceptions of patient safety culture in China: a cross-sectional survey study. J Evid Based Med 2012;5(2):50—6.
Xingxing Zhao
The Second Outpatient Department, Peking University Third Hospital, Beijing 100096, China E-mail: zhaoxx_2014@163.com
25 April 2017;Accepted 11 July 2017
 Family Medicine and Community Health2017年4期
Family Medicine and Community Health2017年4期
- Family Medicine and Community Health的其它文章
- An automated management system for the community health service in China
- Additive manufacturing techniques and their biomedical applications
- A case of probable sporadic Creutzfeldt–Jakob disease
- Seguin Form Board as an intelligence tool for young children in an Indian urban slum
- Assessment of family physicians’ knowledge of childhood autism
- Counseling strategies for nutritional anemia by family physicians in Saudi Arabia, 2016: Implication for training