
Prospective evaluation of the short access cholangioscopy for stone clearance and evaluation of indeterminate strictures
2017-02-10 08:08:21
Hamburg, Germany
Prospective evaluation of the short access cholangioscopy for stone clearance and evaluation of indeterminate strictures
Athanasios D Sioulas, Muhammad A El-Masry, Stefan Groth, Guido Schachschal, Mario Anders, Thomas R?sch and Ulrike Denzer
Hamburg, Germany
BACKGROUND: Peroral cholangioscopy facilitates diagnosis and therapy of biliary disorders. This study prospectively evaluated a new short access cholangioscopy.
METHODS: Consecutive patients were included as follows: diffcult stones (group 1) underwent cholangioscopy with electrohydraulic lithotripsy and indeterminate biliary strictures (group 2) were evaluated with macroscopic assessment and cholangioscopy guided biopsy sampling. We evaluated the complete stone clearance rate (group 1) and diagnostic accuracy (group 2). Follow-up was performed over a median of 13 and 16 months, respectively.
RESULTS: Group 1 (n=21): complete stone clearance defned as lack of stones in cholangiography and stone removal during cholangioscopy was achieved in 15 (71.4%) patients. Clinical stone clearance defned as lack of symptoms, laboratory abnormalities and hospital visits during follow-up, irrespective of stone clearance was evident in 17 (81.0%) patients. One serious adverse event occurred (bile duct perforation). Group 2 (n=28): malignancy was confrmed in 15 patients. Sensitivity, specifcity and diagnostic accuracy of cholangioscopy were 85.7%, 75.0% and 80.7%, respectively. Sensitivity, specifcity and diagnostic accuracy of biopsies were 54.5%, 100.0% and 72.2%, respectively. No serious adverse events occurred, and one patient was lost to follow-up.
CONCLUSIONS: The novel system enabled complex stone treatment and biliary stricture diagnosis. Cholangioscopy outperformed direct biopsy regarding characterization of indeterminate strictures.
(Hepatobiliary Pancreat Dis Int 2017;16:96-103)
biliary tract diseases;
novel cholangioscopy;
feasibility
Introduction
During endoscopic retrograde cholangiopancreatography (ERCP), cholangioscopy enables removal of complex biliary stones following fragmentation by means of electrohydraulic (EHL) or laser lithotripsy as well as macroscopic and histologic assessment of indeterminate biliary strictures.[1]
Since the frst peroral cholangioscopy in the early 1970s, continued technological improvements have resulted in the development of miniature endoscopes and catheters that permit biliary tract inspection. Currently, cholangioscopy can be carried out as either two- or single-endoscopist technique. Endoscopic equipment for the former procedures involves mother-baby systems with the baby scope being inserted through the accessory channel of the mother one. Single-endoscopist cholangioscopy is performed with a catheter-based system or using an ultraslim gastroscope (USG). Nevertheless, both techniques have several limitations including restricted maneuverability, limited image quality, very small working channels and associated accessories and scopes fragility.[2,3]
To overcome part of the aforementioned disadvantages, a novel short access cholangioscopy (SAC) system was recently developed (Karl Storz GmbH, Tuttlingen, Germany).[4]
This innovative mother-baby system comprises of a dedicated duodenoscope with an extra side port for the entrance of a shortened baby cholangioscope. Apart from its improved fexibility, SAC provides a wider working channel of 1.4 mm allowing the insertion of larger accessories.
The current prospective feasibility study aimed to evaluate practical aspects of this novel mother-baby cholangioscopy system and its effcacy in terms of diffcult bile duct stones treatment and indeterminate biliary stricture diagnosis. Furthermore, several technical and procedural parameters were also assessed and discussed.
Methods
This single-center prospective study was conducted in the Department of Interdisciplinary Endoscopy of the University Hospital Hamburg-Eppendorf in Germany from November 2011 until June 2015. The study protocol was approved by the Institutional Clinical Research Ethics Committee (PV3526) and was registered in Clinicaltrials.gov (NCT01683240). All enrolled patients provided written informed consent before the procedures.
Patients
A total of 49 patients, older than 18 years, were included in the study. Based on the inclusion criteria they were separated in two groups: a) 21 patients with “diffcult” biliary tract stones, namely those not cleared by means of conventional ERCP (group 1) and b) 28 patients with indeterminate biliary duct strictures, defned as not defnitely diagnosed by conventional ERCP with brush cytology and/or biopsy (group 2). Exclusion criteria were as following: 1) very diffcult or impossible access to the papilla, 2) inappropriate biliary tract anatomy (e.g. multiple strictures or duct diameter smaller than scope diameter preventing intubation), 3) magnetic resonance cholangiopancreatography (MRCP)-proven primary sclerosing cholangitis, 4) not corrected coagulopathy (quick time <50% or PLTs <50 000/mm3) or ongoing therapeutic anticoagulant/dual antiplatelet medication and 5) poor performance status (Eastern Cooperative Oncology Group-ECOG IV).
Data collection
For each eligible patient the following data were recorded: basic characteristics [age, gender, ECOG status, body mass index (BMI)], indication for cholangioscopy, pertinent medical history, previous hepatopanceaticobiliary (HPB) surgery, laboratory data [complete blood count (CBC), liver function tests (LFTs), international normalized ratio (INR), carcinoembryonic antigen (CEA), CA19-9] and results of available imaging studies. In group 2 patients the pre-test probability with respect to the diagnosis of malignancy was determined on the basis of history (pain, jaundice, weight loss, recent HPB surgery), clinical, laboratory (CBC, LFTs, tumor markers) and imaging [ultrasound (US), computed tomography (CT), magnetic resonance imaging (MRI)/MRCP] data.
Regarding the endoscopic procedures the following parameters were recorded: type of sedation (propofol administration or endotracheal intubation), durations (time needed for cholangioscope introduction into the bile ducts, cholangioscopy and total duration of examination), subjective scope maneuverability (rating from 1 to 6), percentage of stone clearance in a single procedure, diagnostic accuracy for indeterminate strictures (including macroscopic, histological and cytological evaluation) and adverse events within 24 hours after the intervention.
Gold standard criteria for common bile duct clearance assessment included cholangioscopic image and contrast cholangiography with occlusion balloon technique. Gold standard criteria for diagnosis of biliary strictures were regarded the following: defnite histology and/or cytology, surgical resection and/or clinical follow-up exceeding 12 months. For the purpose of analysis, both carcinomas and precancerous lesions (e.g. those exhibiting intraepithelial neoplasia, either low- or high-grade) were considered neoplastic/malignant lesions. Follow-up was performed by telephone interview, hospital visits and chart reviews until patient's death or termination of the study. Inquiries included symptoms, laboratory and/or imaging tests and subsequent interventions, namely endoscopic procedures, interventional radiology procedures and surgery.
Procedures
All procedures were performed by two experienced endoscopists, assisted by a gastroenterology fellow and one or two endoscopy nurses. An anesthesiologist was also involved in case endotracheal intubation was indicated. Histological and cytological specimens were interpreted by an experienced pathologist and cytopathologist, respectively.
All patients underwent ERCP including endoscopic sphincterotomy (EST), if this had not already been performed. Cholangiography revealed either stones or strictures in the biliary tree. Initially, stone removal by at least 2 conventional endoscopic retrograde cholangiography (ERC) attempts (including extension of a pre-existing EST, several attempts using basket and extraction balloon as well as mechanical lithotripsy) was performed.
Patients with persisting stones or biliary stricturesproceeded to cholangioscopy. Using the SAC motherbaby system, a second endoscopist introduced the novel cholangioscope into the bile ducts and by gentle steering attempted to reach the lesion (stone or stricture). Sterile saline solution was continuously fushed to facilitate visualization. Patients were then further managed according to the underlying pathology:
a) Patients with identifed stones were treated by EHL under visual guidance by means of an EHL fber that was introduced through the working channel of the cholangioscope and was advanced until its tip got in direct contact with the stone(s). If fragmented, the stone particles were fushed out or removed with a basket and/ or balloon.
b) Patients with strictures underwent macroscopic evaluation followed by visually guided forceps biopsy sampling and subsequently ERCP-mediated brush cytology sampling (at least 3 passes each) for comparison. Of note, cholangioscopic criteria for malignancy[5,6]included at least one of the following: pathological (abnormally dilated and tortuous) blood vessels, irregular mucosal surface and presence of ulcerative or infltrative lesions.
The SAC system
The SAC mother-baby system involves a dedicated duodenoscope (Frimberger duodenoscope 13883PKS) and a cholangioscope (13700CKS) both manufactured by Karl Storz GmbH in Tuttlingen, Germany. The duodenoscope has an additional side port 70 cm distally on the scope shaft that facilitates the introduction of a shortened to 95 cm cholangioscope. Its reduced length promises better maneuverability and less fragility, while its enlarged working channel (1.4 mm) facilitates advancement of accessories (i.e. biopsy forceps, EHL fber). Moreover, this cholangioscope has a 3.4 mm shaft diameter, enables a 2-way (up and down) steering of its tip and provides a 20 000 pixel glass-fber imaging. As with most other mother-baby systems, procedures with the SAC system require 2 close-coordinating endoscopists with 1 operating the duodenoscope and the other the cholangioscope.
Study outcome parameters
Main outcome parameters of the study, depending on the two different patient groups, were: a) the rate of complete stone clearance, as assessed by contrast ERC and cholangioscopy, and b) the rates of correctly positive and negative results (sensitivity and specifcity) of both macroscopic assessment as well as tissue diagnosis (combined assessment of histology and cytology).
Secondary outcome parameters were:
(1) endoscopist's subjective rating of maneuverability of the system (scale from 1 to 6, 1 indicating excellent and 6 poor, respectively),
(2) incidence of adverse events,
(3) time required for the procedure.
In stone patients:
(4) percentage (%) of stone extraction per procedure,
(5) stone clearance within one session,
(6) clinical stone clearance, defned as lack of associated symptoms, laboratory abnormalities and hospital visits during follow-up, irrespective of cholangioscopically assessed complete or partial stone clearance.
In stricture patients:
(7) technical success, defned as successful advancement of the scope into the pre-determined strictured segment, regardless of whether its passage was eventually achieved or not; patients in whom a pre-diagnosed stricture was ruled out were also included in this defnition,
(8) assessment of quantity and quality of biopsy specimens,
(9) correlation between fnal diagnosis and endoscopic appearance, histology and cytology fndings and pre-test probability of malignancy.
Statistical analysis
Descriptive statistics for continuous variables are presented as means or medians with standard deviations (SD) or interquartile range (IQR), respectively. Categorical variables were reported as absolute values and percentages. Sensitivity, specifcity, diagnostic accuracy, positive and negative predictive values were calculated according to their defnitions.
Results
During the study period 2998 ERCP procedures were performed in our department, 1018 of them for biliary stones treatment. Out of a total of 71 cholangioscopies in 64 patients, included in the study were 56 procedures in 49 patients (26 males, 23 females; mean age: 60.2 years, range 35-88). Indications were either management of complex biliary stones (group 1) or further evaluation of indeterminate biliary strictures (group 2). Excluded from analysis were 15 cholangioscopies, 7 in established primary sclerosing cholangitis patients, 6 due to the presence of multiple biliary strictures and 2 due to abnormal coagulation parameters (Fig. 1). Baseline patient characteristics are summarized in Table 1.
Group 1: stones (Table 2)
The 21 included patients had already undergone a median of 1 (IQR: 1) ERCP procedures, while median maximum size of target stones was 10 mm (IQR: 3).Twenty-four examinations were carried out uneventfully. One examination resulted in serious adverse event. The patient with impacted right sided intrahepatic stones showed a bile duct perforation at the hepatic hilum during the ERC contrast flling after cholangioscopy with EHL and stone removal. Interestingly, this complication was unnoticed during the pre-cholangioscopy ERC with stone removal attempts, as well as during the subsequent cholangioscopy and associated therapeutic interventions. Perforation was closed surgically at the same day and atypical resection of the liver segments with intrahepatic stones was undertaken in a second operation later on. One procedure was prematurely stopped due to technical reasons (instrument defect i.e. loss of cholangioscopic image) and stone extraction was completed using mechanical lithotripsy.
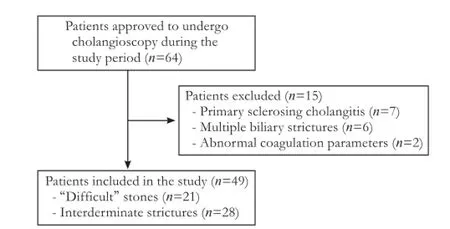
Fig. 1. Study fowchart showing numbers of included and excluded patients.
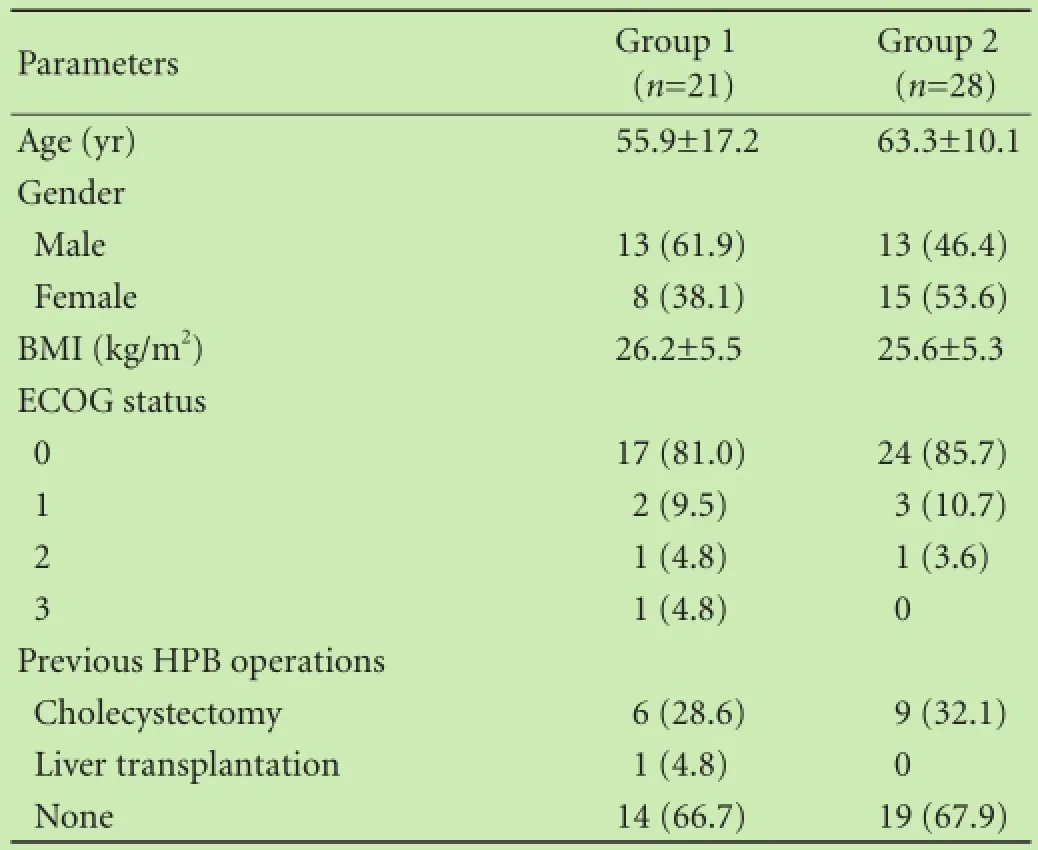
Table 1. Baseline patient characteristics (n, %)
In the intention-to-treat analysis, complete (100.0%) stone removal during cholangioscopy was achieved in 15 patients (12 after 1 procedure, 2 after 2 procedures and 1 after 3 procedures), so the complete clearance rate in one session was 57.1%. Three patients achieved a 50%-80% stone removal in the frst intervention and subsequently, 2 of them underwent ERCP with complete stone clearance and the third one proceeded to hemihepatectomy due to intrahepatic stone localization. The same reason led to surgery an individual who initially achieved less than 50% clearance but was eventually complicated by bile duct perforation. Finally, one patient suffering from dementia was offered nearly complete (>80%) stone removal following 2 examinations and eventually underwent bile duct stent placement, since no further treatment was accepted by caregivers. Clinical stone clearance was achieved in 17/21 (81.0%, intention-to-treat analysis) patients. Detailed procedural data are summarized in Table 2.
Group 2: strictures (Tables 3 and 4)
A total of 28 patients was included and 2 of them underwent 2 examinations each. One patient was lost to follow-up, thus the number of evaluable individuals is 27. The patient was jaundiced in 12/30 procedures. Regarding previous imaging tests, all patients had undergone an upper abdominal US, 7 a multiphasic contrast-enhanced multidetector-row CT, 13 a contrast-enhanced MRI/ MRCP scan and 3 all three modalities. By defnition, all patients had undergone conventional ERCP with inconclusive brush cytology and/or biopsy results, while pre-cholangioscopy bile ducts stenting was evident in 17/30 patients.
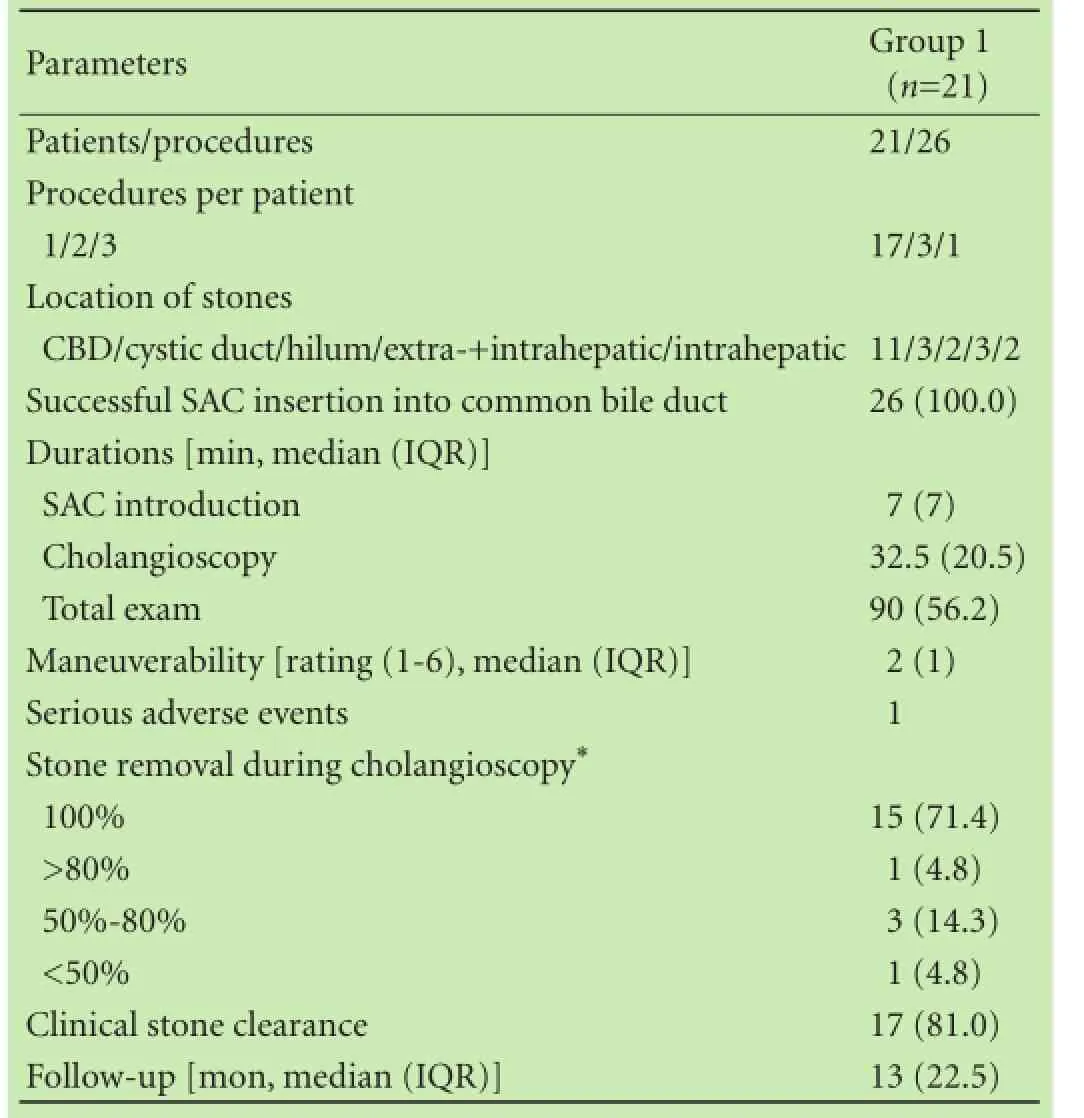
Table 2. Procedure-related details of group 1 (n, %)
In all examinations cannulation of the biliary tract and insertion of the cholangioscope were successful without complications. Only 1 event of transient mild hypoxemia due to sedation that was immediately reversed occurred.
A malignant stricture was confrmed in 15 patients according to the previously mentioned gold standard criteria. Cholangiocarcinoma was the most commondiagnosis (9 patients, 60.0%). Six patients had a stricture of benign nature, presence of a stricture was excluded in 6 patients, while no data are available for 1 patient whose stenosis was macroscopically and histologically benign, but was lost to follow-up.
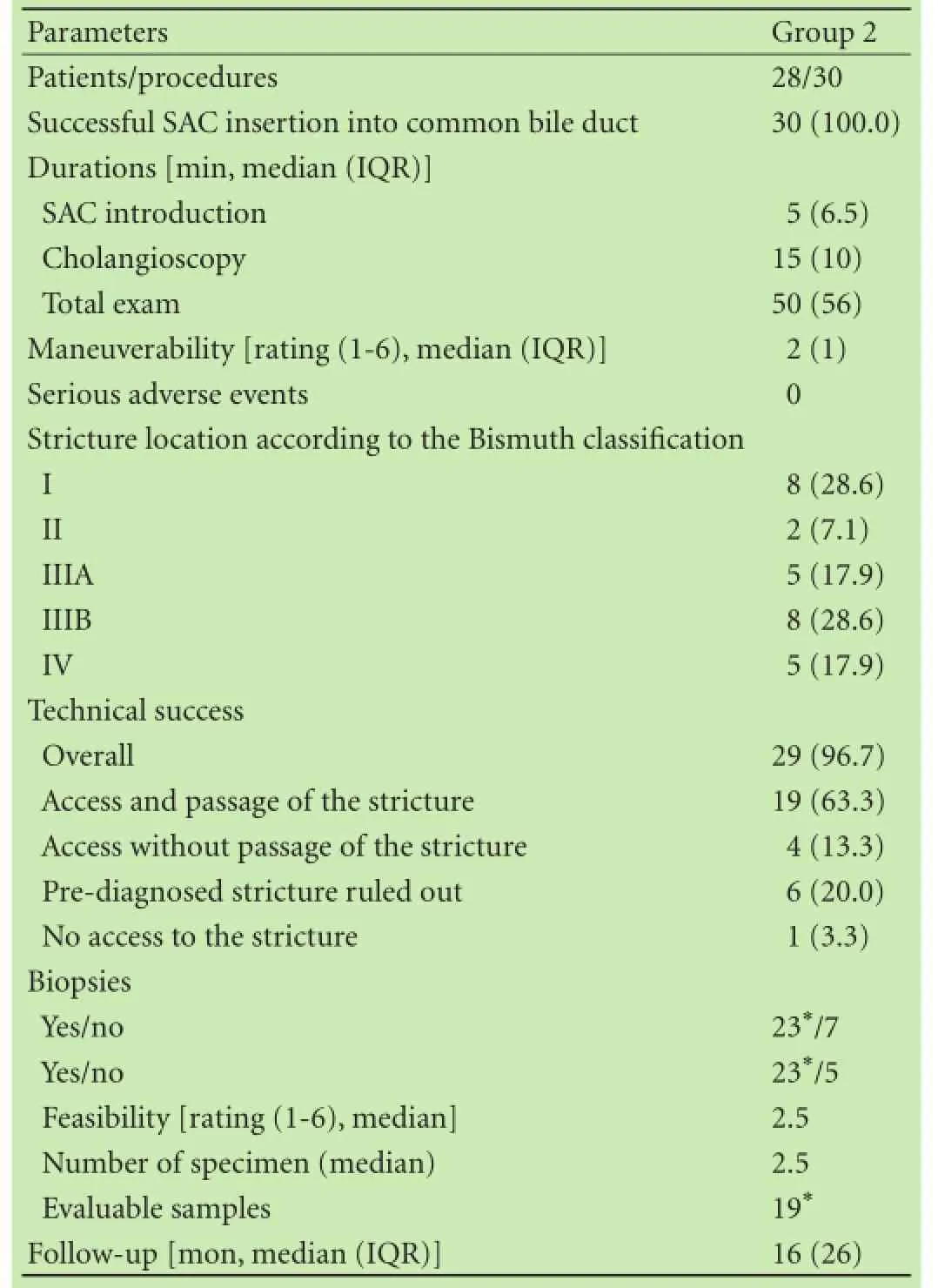
Table 3. Procedure-related details of group 2 (n, %)
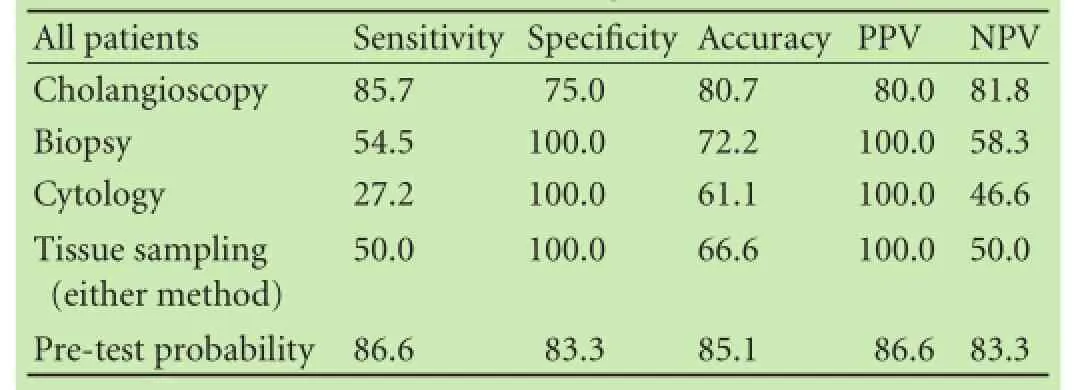
Table 4. Contribution in the diagnosis of strictures (%)
By means of macroscopic criteria cholangioscopy identifed correctly 12 of 15 malignant strictures, including 1 case of extrinsic compression secondary to infltrative mass. Examples are given in Figs. 2 and 3. Of note, the patient whose lesion (cholangiocarcinoma) could notbe reached by cholangioscopy was excluded from this analysis.
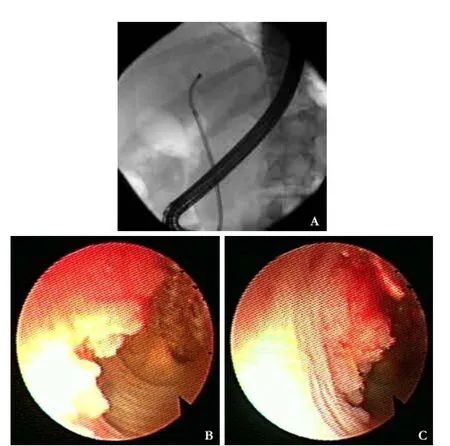
Fig. 2. A 50-year-old male. Clinical presentation with recurrent intrahepatic cholelithiasis in the left hepatic duct. Endoscopic retrograde cholangiography revealed a flling defect suspicious of a mass or stone at the left hepatic duct. Cholangioscopy showed a polypoid adenoma confrmed by biopsy. The patient underwent a left sided hemihepatectomy with biliodigestive anastomosis.
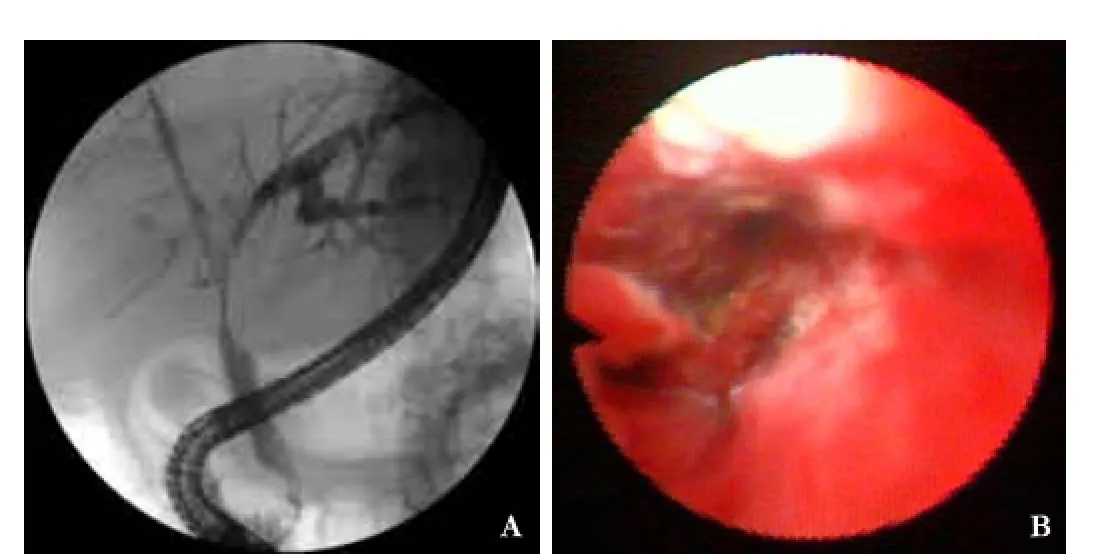
Fig. 3. A 57-year-old male. Suspected cholangiocarcinoma Bismuth type IV. Cholangioscopy reached the proximal part of the stenosis showing an ulcerating tumor with pathological vessels. Biopsy revealed dysplastic bile duct tissue. Due to an underlying liver cirrhosis the lesion was not considered resectable and the patient received palliative chemotherapy.
Pre-test probability suggested malignancy in 15/30 examinations. Taking into account the fnal diagnosis in the 27 evaluable patients a correct assessment was made in 13/15 patients with malignancy.
Cholangioscopy-directed biopsy and brush cytology was performed in 22 and 18 of 27 evaluable patients, respectively. Combined tissue analysis reached slightly better results; 15 patients eligible for evaluation underwent both biopsy and cytology yielding adequate specimen. Of interest, in only 8 of them both techniques had identical results and these were in agreement with the fnal diagnosis.
The performance of the aforementioned diagnostic tools is presented in Table 4.
Discussion
The primary advantage of direct cholangioscopy is that it offers the ability of visualization of the biliary tract, allowing inspection and targeted biopsies of the suspected lesions, as well as interventional procedures such as lithotripsy for bile duct clearance from complex stones. Despite its promising potential, cholangioscopy has not gained generalized acceptance since its advent in the early 1970s. Reasons for under-utilization are technical and practical obstacles including instrument fragility, diffcult maneuverability of the miniature endoscopes, suboptimal optical resolution, time-consuming procedures with requirement of two endoscopists and highcost equipment.[7]Recently, numerous technological improvements have led to variable improvements regarding the technical features and diagnostic yield of cholangioscopy. In this setting, new modalities are available including catheter-based systems, baby cholangioscopes with optional use of narrow band imaging and specifcallydesigned USG.[8-12]
We conducted the present study in order to evaluate a novel mother-baby cholangioscopy system in terms of feasibility and effcacy in patients with diffcult bile duct stones or indeterminate biliary tract strictures. Our results indicate that the SAC system displays suffcient maneuverability achieving bile duct visualization at least including the hepatic hilum. Moreover, it facilitates complete extrahepatic stone clearance via fragmentation with EHL and enables macroscopic evaluation and, in most cases, direct biopsy sampling of suspected lesions.
With regards to the group of patients with diffcult stones, the main reason for failure was the intrahepatic location of the stones with limited access of the cholangioscope necessitating surgery. Extracorporeal shock wave lithotripsy could possibly serve as an alternative step, although not implemented. Nevertheless, our results are in line with those of other studies assessing the effcacy of cholangioscopy-delivered EHL in the management of diffcult bile duct stones.[12-14]
Indeterminate biliary strictures represent the most challenging indication for cholangioscopy allowing the endoscopist to reach a diagnosis and decide on the appropriate further management. The new shortened baby cholangioscopy was also evaluated in the diagnosis of such strictures by means of both macroscopic criteria and SAC-mediated forceps biopsies. SAC system's sensitivity and specifcity compares well with the results from other prospective studies.[15-19]Similarly, tissue sampling by either cholangioscopy-directed forceps biopsy or ERCP-directed brushing cytology yielded relatively low sensitivity and negative predictive values, which is comparable to literature results including a recent metaanalysis.[20-23]Fukuda et al[16]demonstrated a signifcant improvement in sensitivity, diagnostic accuracy and negative predictive value when cholangioscopy combined with ERCP-mediated tissue sampling (either forceps biopsy specimen or brushing) was performed. Of interest, also in our study, macroscopic assessment of biliary strictures performed better than tissue sampling (by either biopsy or ERCP-mediated brushing cytology) with respect to the correct fnal diagnosis.
Most previous studies did not take pre-test likelihood into account which greatly infuences diagnostic accuracy of imaging since examiners cannot be blinded to clinical results as well as other imaging procedures, especially ERCP. For example, both a young woman with a biliary stricture after cholecystectomy and a 70 year old man with painless jaundice have very high pre-test likelihood, the former for a benign stricture and the latter for malignancy. These facts and other tests such as ERCP showing smooth or irregular strictures and other features greatly infuence the diagnostic capability. In the area of endoscopic ultrasound (EUS) cancer staging, we showed some years ago that knowledge of the endoscopic aspects signifcantly improves EUS staging capability.[24]Tissue confrmation of a clinical suspicion is another issue which is often considered necessary before initiation of far-reaching treatments such as major surgery and/or chemotherapy, and will become more important with individualized therapies depending on tissue characteristics and marker features. Unfortunately, biliary tissue sampling either by ERCP or even by direct cholangioscopy has remained unsatisfactory over the years, and the hope that directed biopsy under visual control may substantially improve results, have not been fulflled.[16,22,25-29]
Storz cholangioscopy system has been also evalu-ated in two studies of different design.[4,30]Prinz et al[4]conducted a prospective pilot study to evaluate the new modality in terms of feasibility in patients with indeterminate strictures and fxed flling defects. According to the results, cholangioscopy performed excellent in the visual diagnosis of strictures (sensitivity, 96.4%; specifcity, 92.6%, diagnostic accuracy, 94.5%), while biopsy tissue sampling reached a sensitivity of 64.3%. Complete stone removal via visually-guided laser lithotripsy was achieved in all 9 patients with complex stones (5 in 1 and 4 in 2 sessions). Cannulation of the biliary tree was in all cases successful and no complications were encountered.[4]A single-center randomized controlled trial compared the performance of the SAC system and direct cholangioscopy with an USG in patients with various cholangiopathies (strictures, intraductal flling defects, adenomas of the papilla with suspected ductal extension and removal of retained stones).[30]The two techniques did not differ in terms of technical success, access to the hilus or strictured segment, time needed to intubate the common bile duct and complication rates. However, SAC system needed signifcantly less total procedural time and gained signifcantly better access to the intrahepatic ducts in cases with no major stenoses. On the other hand, USG showed a better correlation between the endoscopic prediction and histologic fndings as compared to SAC system.[30]It is noteworthy that in this study the cholangioscopic/ histologic evaluation mismatch was much lower as compared to ours. This fnding could possibly explained by the fact that the majority of our stricture cases were located proximally in the biliary tree, although no relative data to compare are presented by Pohl et al.
The aforementioned study is the only available comparing cholangioscopy with the SAC system versus cholangioscopy with a USG.[30]The latter represents a single-operator method providing high resolution images similar to standard endoscopy. Additionally, it enables a 4-direction tip movement and advancement of diagnostic and therapeutic accessories through its 2-mm working channel. However, cholangioscopy with a USG faces two important obstacles: frst, its diffculty to cannulate the ampulla of Vater, given its outer diameter (5-6 mm) and second, the acute angle that must be maneuvered from the second duodenal part into the biliary tree. Therefore, several techniques (i.e. guidewire, intraductal balloon, overtube) with various results have been implemented to overcome these problems.[31]The SAC system lacks such drawbacks and, as also shown in our study, can easily gain access inside the bile ducts. Moreover, it demonstrated better accessibility of the intrahepatic ducts as compared to USG. On the contrary, USG offered better correlation between the endoscopic prediction and histologic fndings and shorter procedure times.[30]Further comparative studies are warranted to accurately defne SAC system's position among the available facilities for direct biliary visualization.
Two limitations of the present study should also be discussed. Firstly, the study sample size is rather small, but, on the other hand, results are in line with previous studies. Secondly, it was performed in a single-tertiary university hospital by experienced endoscopists possibly limiting generalization of the results in the everyday clinical practice. However, this defnitely represents a fact of life, since complicated cases should be referred to centers providing well-educated staff and advanced technological equipment.
In summary, the new shortened peroral mother-baby cholangioscopy system provided advanced maneuverability allowing safe and unrestricted access to target sites within the biliary tree. Moreover, its good stability enabled biopsy sampling and successful therapeutic interventions, when indicated. The SAC system allowed for a reasonable macroscopic stricture diagnosis exceeding that obtained by tissue sampling. Undoubtedly, large, multicenter trials as well as randomized comparisons of the novel system with other cholangioscopy modalities are needed to further elucidate its role in biliary tract diseases. One of the major challenges in addition will be improvement of cholangioscopy-directed tissue sampling.
Contributors:SAD searched the literature, drafted and fnally approved the manuscript. DU designed the study, performed the endoscopies, reviewed the draft and fnally approved the manuscript. EMA and AM collected the data, made critical revisions, reviewed the draft and fnally approved the manuscript. GS and SG performed the endoscopies, reviewed the draft and fnally approved the manuscript. RT conceived the idea, critically reviewed the draft and fnally approved the manuscript. DU is the guarantor.
Funding:This study was supported by a grant from Karl Storz GmbH, Tuttlingen, Germany.
Ethical approval:The study protocol was approved by the Institutional Clinical Research Ethics Committee (PV3526) and was registered in Clinicaltrials.gov (NCT01683240).
Competing interest:The author or one or more of the authors have received or will receive benefts for personal or professional use from a commercial party related directly or indirectly to the subject of this article.
1 Moon JH, Terheggen G, Choi HJ, Neuhaus H. Peroral cholangioscopy: diagnostic and therapeutic applications. Gastroenterology 2013;144:276-282.
2 Ross AS, Kozarek RA. Cholangioscopy: where are we now? Curr Opin Gastroenterol 2009;25:245-251.
3 Ghersi S, Fuccio L, Bassi M, Fabbri C, Cennamo V. Current status of peroral cholangioscopy in biliary tract diseases. World JGastrointest Endosc 2015;7:510-517.
4 Prinz C, Weber A, Goecke S, Neu B, Meining A, Frimberger E. A new peroral mother-baby endoscope system for biliary tract disorders. World J Gastrointest Endosc 2014;6:20-26.
5 Seo DW, Lee SK, Yoo KS, Kang GH, Kim MH, Suh DJ, et al. Cholangioscopic fndings in bile duct tumors. Gastrointest Endosc 2000;52:630-634.
6 Kim HJ, Kim MH, Lee SK, Yoo KS, Seo DW, Min YI. Tumor vessel: a valuable cholangioscopic clue of malignant biliary stricture. Gastrointest Endosc 2000;52:635-638.
7 Parsi MA. Peroral cholangioscopy in the new millennium. World J Gastroenterol 2011;17:1-6.
8 Itoi T, Neuhaus H, Chen YK. Diagnostic value of imageenhanced video cholangiopancreatoscopy. Gastrointest Endosc Clin N Am 2009;19:557-566.
9 Larghi A, Waxman I. Endoscopic direct cholangioscopy by using an ultra-slim upper endoscope: a feasibility study. Gastrointest Endosc 2006;63:853-857.
10 Choi HJ, Moon JH, Ko BM, Hong SJ, Koo HC, Cheon YK, et al. Overtube-balloon-assisted direct peroral cholangioscopy by using an ultra-slim upper endoscope (with videos). Gastrointest Endosc 2009;69:935-940.
11 Igarashi Y, Okano N, Ito K, Suzuki T, Mimura T. Effectiveness of peroral cholangioscopy and narrow band imaging for endoscopically diagnosing the bile duct cancer. Dig Endosc 2009;21: S101-102.
12 Chen YK, Pleskow DK. SpyGlass single-operator peroral cholangiopancreatoscopy system for the diagnosis and therapy of bile-duct disorders: a clinical feasibility study (with video). Gastrointest Endosc 2007;65:832-841.
13 Piraka C, Shah RJ, Awadallah NS, Langer DA, Chen YK. Transpapillary cholangioscopy-directed lithotripsy in patients with diffcult bile duct stones. Clin Gastroenterol Hepatol 2007;5:1333-1338.
14 Arya N, Nelles SE, Haber GB, Kim YI, Kortan PK. Electrohydraulic lithotripsy in 111 patients: a safe and effective therapy for diffcult bile duct stones. Am J Gastroenterol 2004;99:2330-2334.
15 Shah RJ, Langer DA, Antillon MR, Chen YK. Cholangioscopy and cholangioscopic forceps biopsy in patients with indeterminate pancreaticobiliary pathology. Clin Gastroenterol Hepatol 2006;4:219-225.
16 Fukuda Y, Tsuyuguchi T, Sakai Y, Tsuchiya S, Saisyo H. Diagnostic utility of peroral cholangioscopy for various bile-duct lesions. Gastrointest Endosc 2005;62:374-382.
17 Osanai M, Itoi T, Igarashi Y, Tanaka K, Kida M, Maguchi H, et al. Peroral video cholangioscopy to evaluate indeterminate bile duct lesions and preoperative mucosal cancerous extension: a prospective multicenter study. Endoscopy 2013;45:635-642.
18 Ramchandani M, Reddy DN, Gupta R, Lakhtakia S, Tandan M, Darisetty S, et al. Role of single-operator peroral cholangioscopy in the diagnosis of indeterminate biliary lesions: a singlecenter, prospective study. Gastrointest Endosc 2011;74:511-519.
19 Siddiqui AA, Mehendiratta V, Jackson W, Loren DE, Kowalski TE, Eloubeidi MA. Identifcation of cholangiocarcinoma by using the Spyglass Spyscope system for peroral cholangioscopy and biopsy collection. Clin Gastroenterol Hepatol 2012;10:466-471.
20 Hartman DJ, Slivka A, Giusto DA, Krasinskas AM. Tissue yield and diagnostic effcacy of fuoroscopic and cholangioscopic techniques to assess indeterminate biliary strictures. Clin Gastroenterol Hepatol 2012;10:1042-1046.
21 Pugliese V, Conio M, Nicolò G, Saccomanno S, Gatteschi B. Endoscopic retrograde forceps biopsy and brush cytology of biliary strictures: a prospective study. Gastrointest Endosc 1995;42:520-526.
22 Draganov PV, Chauhan S, Wagh MS, Gupte AR, Lin T, Hou W, et al. Diagnostic accuracy of conventional and cholangioscopyguided sampling of indeterminate biliary lesions at the time of ERCP: a prospective, long-term follow-up study. Gastrointest Endosc 2012;75:347-353.
23 Navaneethan U, Njei B, Lourdusamy V, Konjeti R, Vargo JJ, Parsi MA. Comparative effectiveness of biliary brush cytology and intraductal biopsy for detection of malignant biliary strictures: a systematic review and meta-analysis. Gastrointest Endosc 2015;81:168-176.
24 Meining A, Dittler HJ, Wolf A, Lorenz R, Schusdziarra V, Siewert JR, et al. You get what you expect? A critical appraisal of imaging methodology in endosonographic cancer staging. Gut 2002;50:599-603.
25 de Bellis M, Fogel EL, Sherman S, Watkins JL, Chappo J, Younger C, et al. Infuence of stricture dilation and repeat brushing on the cancer detection rate of brush cytology in the evaluation of malignant biliary obstruction. Gastrointest Endosc 2003;58:176-182.
26 Jailwala J, Fogel EL, Sherman S, Gottlieb K, Flueckiger J, Bucksot LG, et al. Triple-tissue sampling at ERCP in malignant biliary obstruction. Gastrointest Endosc 2000;51:383-390.
27 Weber A, von Weyhern C, Fend F, Schneider J, Neu B, Meining A, et al. Endoscopic transpapillary brush cytology and forceps biopsy in patients with hilar cholangiocarcinoma. World J Gastroenterol 2008;14:1097-1101.
28 Chen YK, Parsi MA, Binmoeller KF, Hawes RH, Pleskow DK, Slivka A, et al. Single-operator cholangioscopy in patients requiring evaluation of bile duct disease or therapy of biliary stones (with videos). Gastrointest Endosc 2011;74:805-814.
29 Itoi T, Osanai M, Igarashi Y, Tanaka K, Kida M, Maguchi H, et al. Diagnostic peroral video cholangioscopy is an accurate diagnostic tool for patients with bile duct lesions. Clin Gastroenterol Hepatol 2010;8:934-938.
30 Pohl J, Meves VC, Mayer G, Behrens A, Frimberger E, Ell C. Prospective randomized comparison of short-access motherbaby cholangioscopy versus direct cholangioscopy with ultraslim gastroscopes. Gastrointest Endosc 2013;78:609-616.
31 Neuhaus H. New techniques for direct biliary visualization: do we need them and what can be achieved? Gastrointest Endosc 2011;74:317-320.
Received May 3, 2016
Accepted after revision August 26, 2016
Author Affliations: Department of Interdisciplinary Endoscopy, University Hospital Hamburg-Eppendorf, Martinistra?e 52, 20246, Hamburg, Germany (Sioulas AD, Groth S, Schachschal G, Anders M, R?sch T and Denzer U); Division of Gastroenterology, Department of Internal Medicine, Assiut University Hospital, Al Walideyah Al Qebleyah, Qesm Than Asyut, Assiut Governorate, Egypt (El-Masry MA)
Ulrike Denzer, MD, Department of Interdisciplinary Endoscopy, University Hospital Hamburg-Eppendorf, Martinistra?e 52, 20246, Hamburg, Germany (Tel: +49-407410-0; Fax: +49-407410-44420; Email: u.denzer@uke.de)
? 2017, Hepatobiliary Pancreat Dis Int. All rights reserved.
10.1016/S1499-3872(16)60170-4
Published online January 5, 2017.
 Hepatobiliary & Pancreatic Diseases International2017年1期
Hepatobiliary & Pancreatic Diseases International2017年1期
- Hepatobiliary & Pancreatic Diseases International的其它文章
- Meetings and Courses
- Limitations of current liver transplant immunosuppressive regimens: renal considerations
- Editors
- Information for Readers
- The relationship between SPARC expression in primary tumor and metastatic lymph node of resected pancreatic cancer patients and patients' survival
- Quercetin protects liver injury induced by bile duct ligation via attenuation of Rac1 and NADPH oxidase1 expression in rats