
Position and complications of pedicle screw insertion with or without image-navigation techniques in the thoracolumbar spine: a meta-analysis of comparative studies
2014-04-18 13:18:49JinshanTangZiqiangZhuTaoSuiDechaoKongXiaojianCao
Jinshan Tang,Ziqiang Zhu,Tao Sui,Dechao Kong,Xiaojian Cao
Department of Orthopedics,the First Affiliated Hospital of Nanjing Medical University,Nanjing,Jiangsu 210029,China.
Position and complications of pedicle screw insertion with or without image-navigation techniques in the thoracolumbar spine: a meta-analysis of comparative studies
Jinshan Tang,Ziqiang Zhu,Tao Sui,Dechao Kong,Xiaojian Cao?
Department of Orthopedics,the First Affiliated Hospital of Nanjing Medical University,Nanjing,Jiangsu 210029,China.
Computer-navigated pedicle screw insertion is applied to the thoracic and lumbar spine to attain high insertion accuracy and a low rate of screw-related complications.However,some in vivo and in vitro studies have shown that no advantages are gained with the use of navigation techniques compared to conventional techniques.Additionally, inconsistent conclusions have been drawn in various studies due to different population characteristics and methods used to assess the accuracy of screw placement.Moreover,it is not clear whether pedicle screw insertion with navigation techniques decreases the incidence of screw-related complications.Therefore,this study was sought to perform a meta-analysis of all available prospective evidence regarding pedicle screw insertion with or without navigation techniques in human thoracic and lumbar spine.We considered in vivo comparative studies that assessed the results of pedicle screw placement with or without navigation techniques.PubMed,Ovid MEDLINE and EMBASE databases were searched.Three published randomized controlled trials(RCTs)and nine retrospective comparative studies met the inclusion criteria.These studies included a total of 732 patients in whom 4,953 screws were inserted.In conclusion,accuracy of the position of grade I,II,III and IV screws and complication rate related to pedicle screw placement were significantly increased when navigation techniques were used in comparison to conventional techniques.Future research in this area should include RCTs with well-planned methodology to limit bias and report on validated,patient-based outcome measures.
meta-analysis,position,pedicle screw insertion,navigation,complication
INTRODUCTION
Pedicle screws,which perforate the pedicle cortex, increase the risk of dural tearing,neural damage and vascular or visceral complications,especially in the thoracic spine due to its complex anatomy and decreased pedicle dimensions[36,49].Moreover,pedicle screw misplacement results in a loss of fixation,especially at the lower end of a construct,such as lumbar spine.Ideal pedicle screw should have a maximum diameter and length that do not breach the cortical layer of the pedicle or the vertebral body and should be converged[7].The development of methods that improves the accuracy of pedicle screw insertion is an active area of research.
Pedicle screws are often inserted using conventional techniques that are based on anatomical landmarks of the vertebrae or assisted with any intraoperative imaging fluoroscopy,which is called fluoroscopic guided technique to localize the pedicle and evaluate the position of the pedicle screw[2,4,6,15,16,20,21,29,35,36,41,42,44,45,50,53].With development of computer technology,imagenavigated techniques now include computed tomography(CT)-based navigation and fluoroscopy-based navigation.Both provide 2-or 3-dimensional(2D or 3D)intraoperative imaging to assist screw insertion and have been applied extensively.Many studies reported that image-navigated techniques lead to a significant reduction in the rate of screw misplacement[1,3,9,17,24-26,28,31,37,39,42,43,51,55,56].However,in vivo and in vitro studies found no advantages to using navigation techniques compared to conventional techniques, especially in the thoracic spine[18,28].Additionally,it has been shown that experienced spine surgeons insert screws in the thoracolumbar region with a low incidence of screw misplacement using conventional techniques[22].Furthermore,limitations of navigation systems relate to a lengthy learning curve,calibration errors,bending of instruments,occasional blocking of the surgical field with camera,inadvertently touching or hitting reference frames,and non-rigid connection between reference base and actual surgical site[8,12]. Although a few studies[17,24,44,57]reported that the accuracy of fluoroscopy-assisted pedicle screw insertion is comparable to that of CT navigation,differences in population characteristics and methods of assessing placement accuracy between studies have resulted in inconsistent conclusions.
The accuracy of pedicle screw insertion is determined according to the method performed to insert the pedicle and the tools(such as photography,CT, or magnetic resonance imaging(MRI))performed to assess the position of the pedicle screw and the adoption of standard definitions of correct pedicle screw insertion.According to the relationship between the pedicle and screws,most surgeons consider pedicle violation as a safe zone of pedicle perforation smaller than 2 mm[11,22].The grade of pedicle screw violation based on this definition is classified into four groups: screws fully contained within the pedicle;perforated screws with up to 2 mm of displacement(Grade A); perforated screws with 2-4 mm of displacement (Grade B);perforated screws with greater than 4 mm of displacement(Grade C)[15,33].This classification has been used in the majority of studies.In addition, medial pedicle perforation greater than 4 mm may endanger the neural elements and result in neurological deficit[11,22].However,no studies have compared all types of screw positions.The increased safety of inserting pedicle screws may be related to more accurate screw positioning and the fact that less violation of the lateral cortex is unlikely to cause neurological complications[14].Although serious complications such as neurological,visceral,or vascular complications are very rare[30,34,52],the overall incidence of complications related to screw malposition is 0%-42%[19,32].Moreover,it remains unclear that whether pedicle screw insertion using navigation techniques decreases the incidence of screw-related complications.
In this study,we performed a meta-analysis to compare the positioning of pedicle screws in the human thoracic and lumbar spine,and the screw-related complications with or without the assistance of navigation techniques.
MATERIALS AND METHODS
Inclusion criteria
Studies fulfilling the following criteria were eligible for inclusion.First,the report needed to be a comparative study and included randomized controlled trials (RCTs)or prospective or retrospective comparative studies,and the methods used to insert the pedicle screws were conventional techniques or image-navigated techniques.Second,the study was performed in vivo;cadaveric and animal studies as well as studies that used spine models and morphologic articles were excluded. Third,the study was published in English.Fourth,as fixing the cervical spine using the lateral mass and not the pedicle was the main technique used for the cervical spine because of its complicated anatomy,we excluded studies on pedicle screw insertion in the cervical spine. However,we accepted studies that included pedicle screws inserted into the S1 vertebrae,and we also accepted studies where the cervical spine was involved along with the thoracic and/or lumbar spine if separate results for the thoracolumbar spine were available. Fifth,the postoperative screw position must was assessed using CT or MRI.
Search strategy
The electronic databases of PubMed,Ovid MEDLINE (1950 to February,2013),and EMBASE(1980 to February,2013)were searched with the following search terms:‘‘pedicle screw with navigation’’or‘‘navigated’’;‘‘computer assisted/assistance/aided’’;and‘‘image guided/guidance’’.
Screening and assessment of eligibility
Two of the authors(JT and ZZ)independently screened the titles and abstracts of the studies from the electronic search to identify all citations potentially containing the comparison of interest.They independently evaluated and identified these studies by searching references and abstracts from meetings to determine the final set of included articles.Disagreements were resolved by discussion and by further discussion with an independent colleague if necessary.
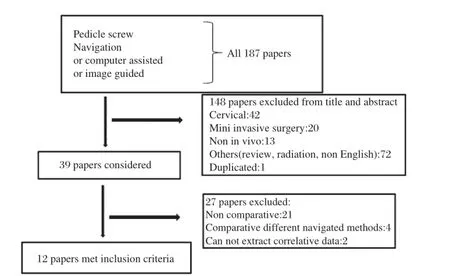
Fig.1Study selection process.
Some definitions and standardizations
Most surgeons consider a pedicle violation of less than 2 mm as a safe zone of pedicle perforation[24,38]. Although there is no strong evidence to support postoperative assessment,this was considered a criterion for inclusion in this meta-analysis[15,37].The grade of pedicle screw violation was categorized into four groups (grade I,II,III and IV)based on published criteria. Grade I screws were those located inside the pedicle, which were defined as the‘‘perfect’’position for the screw;grade II screws were defined as‘‘safe’’zone screws;grade III screws were those in a‘‘potentially hazardous’’zone;and grade IV screws were defined as screws in a zone that was‘‘absolutely hazardous’’. The screw-related complications included nerve root or spinal cord injury,vascular injury,cerebrospinal fluid leak,visceral injury and pedicle fracture[13].
Data extraction
For each eligible study,two of the authors(JT and ZZ extracted the relevant data independently for both the intervention and control groups.These data included demographic data(age and sex)and other types of data. The variables collected including type of study(RCT, prospective comparative study,or retrospective comparative study),anatomic level,number of patients, indications,method of insertion,method of screw position assessment,accuracy of screw placement and criteria,pedicle screw position grades(I,II,III and IV) and screw-related complications.
Statistical analysis
Data concerning each grade of screw and screwrelated complications from the included studies were pooled according to whether pedicle screw insertion was performed using conventional or navigation techniques.Dichotomous variables were pooled across studies.The rate of pedicle violation and incidence of complications were summarized using odds ratios (OR)and 95%confidence intervals(CIs).P<0.05 was considered statistical significant.Heterogeneity was evaluated by using the x2test and I2-statistics.P<0.1 and I2>50%were considered to be significant for heterogeneity.Fixed-effect models were used unless statistical heterogeneity was significant,in which case a random-effects model or sub-group analysis was used. Publication bias was assessed by visually examining the funnel plots based on each grade of pedicle screw and screw-related complications.All analyses were carried out in Review Manager 5.1 software(Cochrane IMS).
RESULTS
Search results
Fig.1shows the process for identifying eligible studies.There were 187 potentially relevant papers; after screening the title as well as reading the abstract and the entire article,we identified three published RCTs[17,25,37]and nine retrospective comparative studies[1,3,9,24,26,31,39,42,43]that met all of the inclusion criteria (Fig.1).
Extraction of data
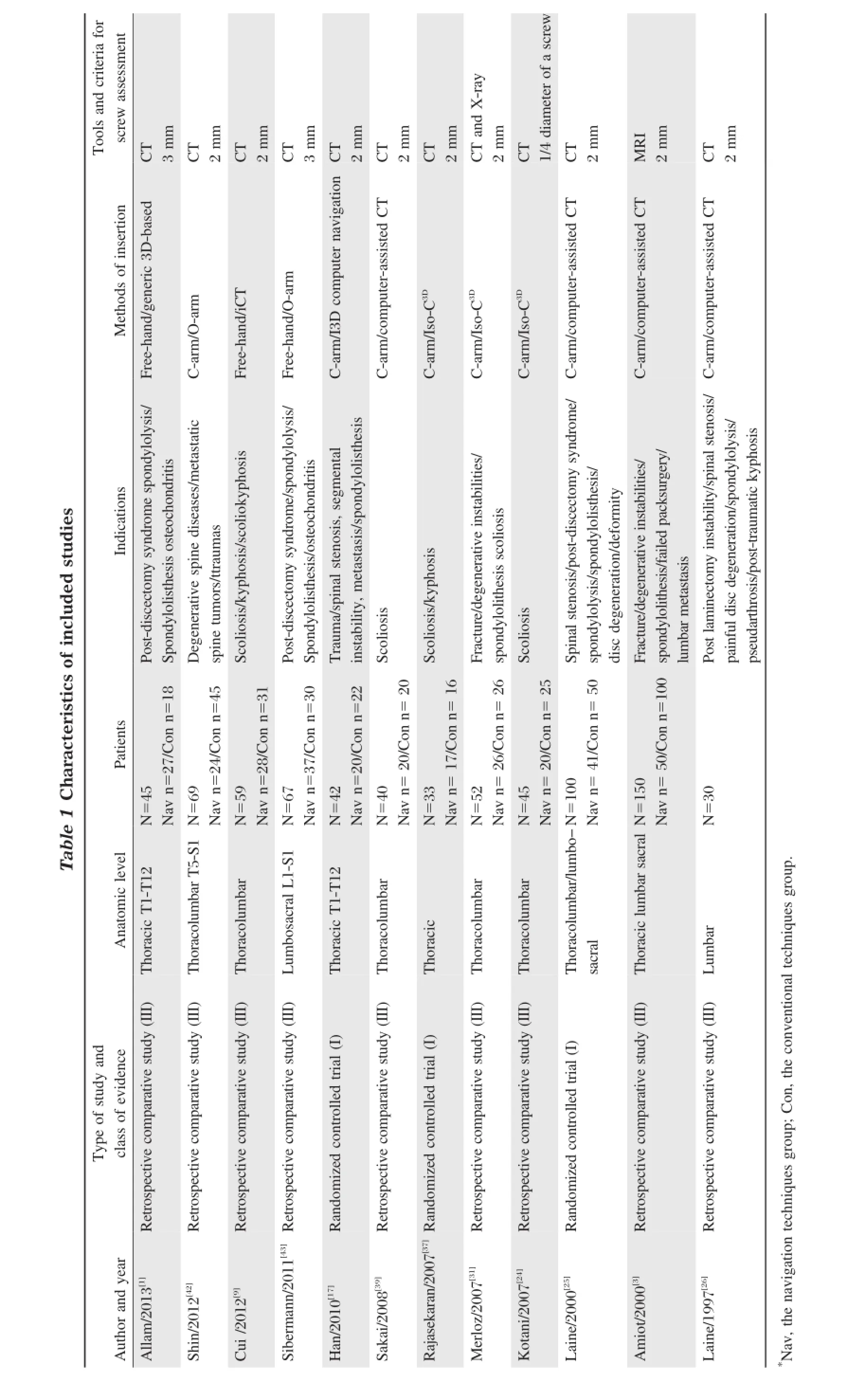
A total of 732 patients and 4,953 screws were included in the 12 studies.There were 2,323 pedicle screws inserted using navigation techniques and 2,630 pedicle screws inserted using conventional techniques.Table 1shows a summary of these studies. CT[3,9,25,26,39]and 3D[1,17,24,31,37]imaging modalities were used to insert pedicle screws in five studies.An O-arm was used in two studies[42,43].Eight[1,3,25,31,37,39,42,43]papers defined the number of screws in grade I,II,and III, and two papers[9,17]described cases of grade I and II. One[26]study defined only grade I screws,and another[24]study published only grade II screws(Table 2).Eight papers[3,9,17,25,31,37,39,42]used 2 mm as the criterion for pedicle screw violation,whereas two papers[1,43]used 3 mm and one[24]used 1/4 of the diameter of the screw as this criterion.With these different criteria,we pooled and analyzed the data according to sub-groups.One[3]study assessed the position of the pedicle screw using MRI, and the others used CT.Tohtz et al.[48]studied postoperative screw position using MRI or CT,and con-cluded that artifact-reduced MRI should be considered an alternative to the gold standard of CT for postoperative imaging after spinal fusion surgery.Therefore,we accepted data that were assessed using MRI.
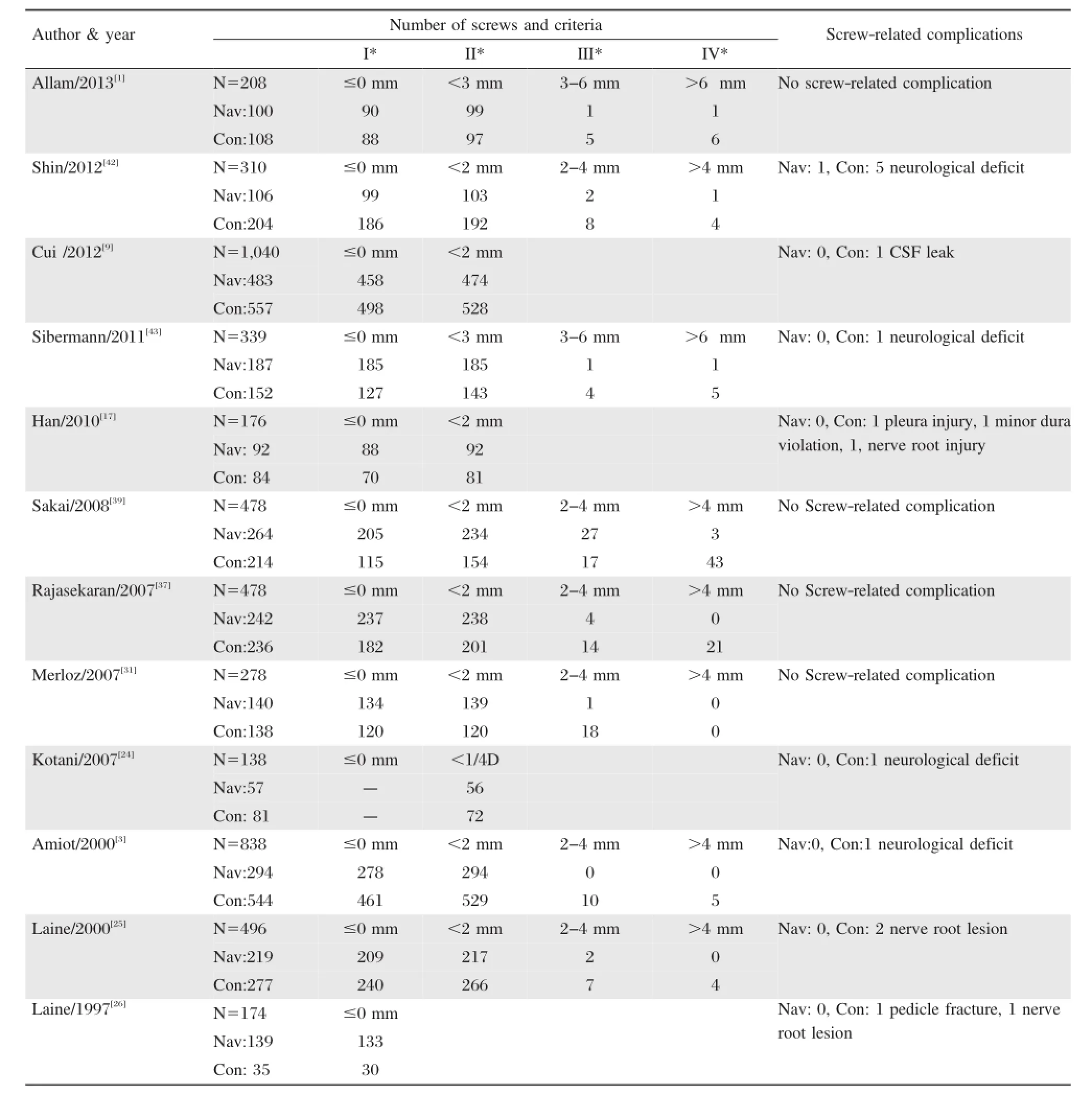
Table 2Grade of screw and screw-related complications of included studies
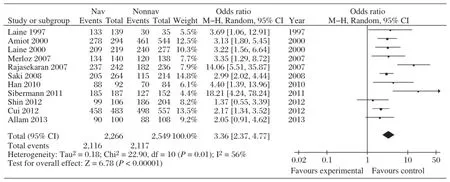
Fig.2Forest plot comparing‘‘perfect’’screws(≤0 mm)between insertions performed with and without navigation.
Meta-analysis of each grade of pedicle screw
Eleven papers reported the number of perfect screws. The comparison of outcomes between placement with or without navigation is shown inFig.2.Meta-analysis revealed a significant difference between image-guided and non-image-guided placement(OR:3.36,95%CI: 2.37,4.77,I2=56%,P<0.00001).
Eleven papers provided the number of‘‘safe zone’’screws.As the different criteria used for perforation of the pedicle screw,such as 2 mm,3 mm and 1/4 D, sub-group analysis was used.The comparison of outcomes with or without navigation is shown inFig.3. Based on meta-analysis,there was a significant difference favoring procedures performed using navigation compared to those performed without navigation(OR: 4.72,95%CI:3.25-6.86,I2=9%,P<0.0001).
Seven papers provided the number of‘‘potentially hazardous’’screws.As different criteria were used for the perforation of the pedicle screws,including 2 mm and 3 mm,sub-group analysis was performed. The comparative outcomes for procedures performed with and without navigation are shown inFig.4. Meta-analysis favored procedures performed with navigation compared to procedures performed without navigation(OR:0.27,95%CI:0.10-0.77,I2=69%, P=0.01.)
Six papers provided the number of‘‘absolutely hazardous’’screws.As the different criteria were used for the perforation of the pedicle screw,including 2 mm and 3 mm,sub-group analysis was used.The comparison of absolutely hazardous screws between procedures with and without navigation is shown inFig.5.Meta-analysis favored procedures performed with navigation compared to those without navigation for absolutely hazardous screws(OR:0.09,95%CI: 0.03-0.26,I2=40%,P<0.00001).
Meta-analysis of screw-related complications
All papers included in the analysis provided rates of screw-related complications.Four papers reported no complications in two groups.The total incidence of complications was 0.22%,but only one complication occurred in the navigation group.There were 17 complications overall,including 13 neurological deficits, one cerebrospinal fluid leak,one pleural injury,one minor dura violation,and one pedicle fracture.Metaanalysis of these complications showed a significant difference favoring navigation compared to the conventional method(OR:0.25,95%CI:0.09-0.70,I2= 0%,P=0.008)(Fig.6).
Publication bias
The funnel plot was based on each grade of pedicle screw and screw-related complications(Fig.7).The graphical funnel plots based on screw-related complications of included studies appeared to be symmetrical, which suggested no publication bias,but the funnel plots based on each grade of pedicle screw of included studies appeared to be asymmetric,which suggested the presence of publication bias.
DISCUSSION
This meta-analysis has shown that for screws in the‘‘perfect,’’‘‘safe,’’‘‘potentially hazardous’’,and‘‘absolutely hazardous’’zones,the accuracy of pedicle screwinsertion was significantly improved with the aid of image-guided navigation.Based on the outcomes, screws inserted in the thoracic and lumbar spine with the use of navigation techniques exhibited a higher accuracy in pedicle screw placement than those placed with conventional techniques.The results is consistent with the report by Gelalis[14],who conducted a review to compare the free-hand,fluoroscopic-guided and navigation techniques,and found that the accuracy of screw positioning was improved when navigation assistance was used.However,this previous report used descriptive statistics to explain the findings.There have been four meta-analyses[23,46,47,52]published in the field of pedicle screw accuracy,and all of these reports included studies that performed retrospective analyses of screw placement and also included the cervical spine,which has a more complicated anatomy than other spinal segments.These studies also showed that insertion with navigation techniques improves the accuracy of pedicle screw insertion.Tian et al.[46]also compared pedicle screw insertion accuracy with different navigation methods and found that CT and 2D and 3D navigation techniques presented few differences.However,these studies only compared the accuracy of‘‘safe zone’’screws with or without the use of navigation techniques, whereas the present study compared all of the different screw zones in the thoracic and lumbar spine,which suggests that the current report may provide more accurate evidence.
As pedicle screws were inserted in vivo,the assessment of pedicle screw positioning post operation must be performed using plain radiography,CT,or MRI,as opposed to dissection,which may influence the accuracy of pedicle screw assessment.This is one possible reason why the accuracy of pedicle screw insertion in vitro is superior to that in vivo[23].Assessment by plain radiography was not included in the present study due to its lower accuracy[5,54],whereas CT scans have been considered the‘‘gold standard’’for the assessment of pedicle screw placement[5,6,10,38].The CT technique can reduce metal artifact significantly and provide 3D images that display all aspects of the position ofthe pedicle screw.However,CT images cannot display the soft tissues clearly,especially the nerve root.In contrast,MRI provides excellent evaluation of the soft tissues,including the nerve root,although due to metal artifacts,MRI cannot display metal screws clearly. Recently,one study[48]has shown that artifact-reducedMRI could be considered an alternative to the gold standard for postoperative imaging to assess the accuracy of pedicle screw insertion,as this technique can reveal the relationship of the pedicle screw to the nerve root after spinal fusion surgery.Thus,MRI will likely become a standard method to assess the position of pedicle screws in the future.
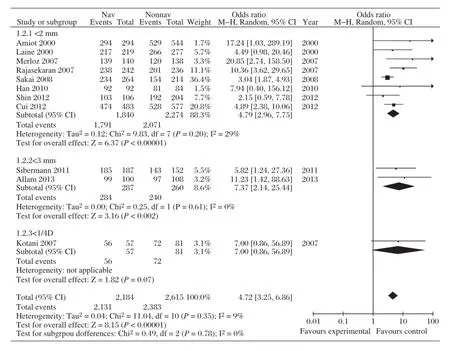
Fig.3Forest plot of the comparison between‘‘safe zone’’screw procedures performed with and without navigation.
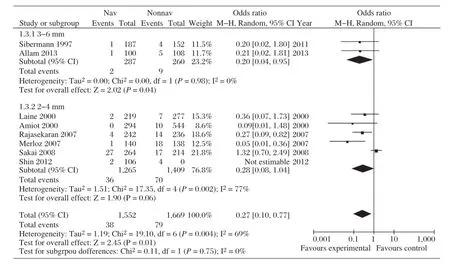
Fig.4Forest plot of the outcomes for‘‘potentially hazardous’’screws compared between procedures performed with and without navigation.
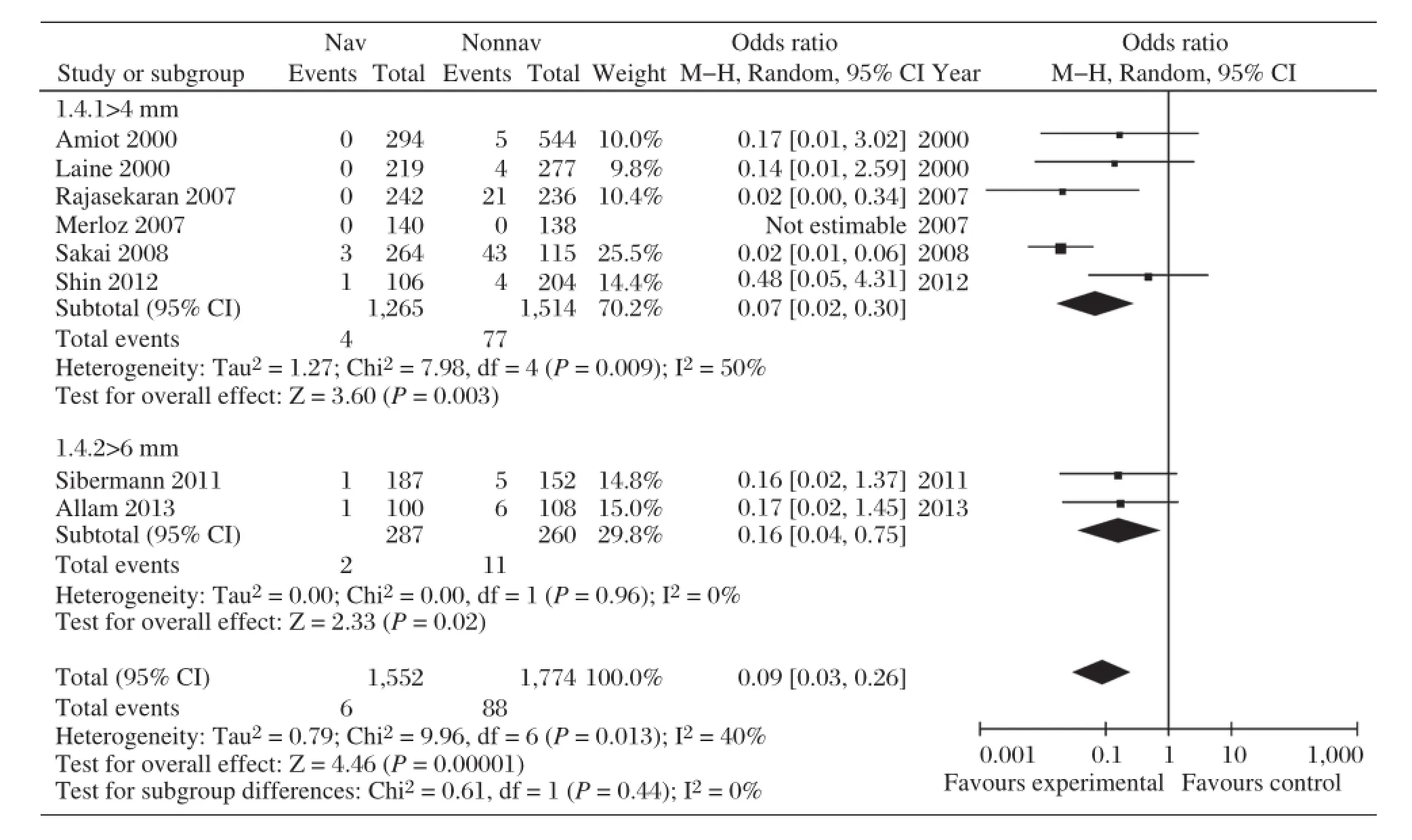
Fig.5Forest plot comparing‘‘absolutely hazardous’’screws between procedures performed with and without navigation.
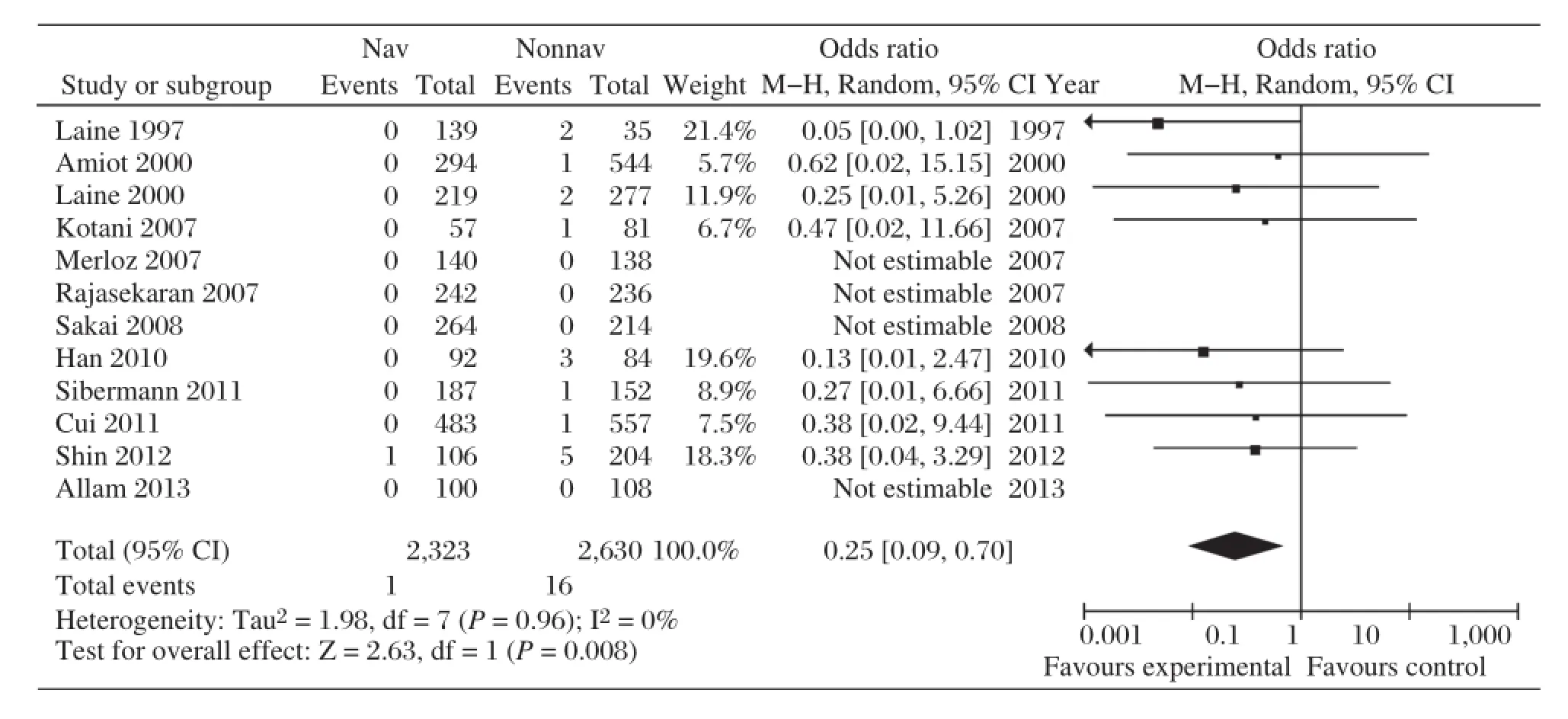
Fig.6Forest plot comparing complications between procedures performed with and without navigation.
Malposition of a pedicle screw leads to many complications,such as dural lesions,nerve root irritation, vascular injury,cerebrospinal fluid leak,visceral injury and pedicle fracture.However,there are few symptomatic complications relative to the high rate of pedicle screw perforations[27,30,34,52].Neurological complications while inserting pedicle screws are rare but serious.In our study,12 papers reported that 94 screws perforated the pedicle by more than 4 mm,but only 17 screwrelated complications were reported,with a mean incidence of 18%.The results of our study show that dural lesions and irritation of nerve roots occurred in a mean of 0.06%and 0.15%of pedicle screws,respectively.In all 12 papers,only one complication was reported in the group using navigation techniques.However, Schulze et al.[40]reported that experienced surgeons could accurately place pedicle screws in 80%of cases with conventional techniques and that neurological symptoms are rarely affected by an inaccurate pedicle screw placement,even if the penetration of the pedicle wall is greater than 6 mm.Gelalis et al.[14]showed in a review that the neurological complication rate was similar between studies using CT navigation,the free-hand technique and fluoroscopy.In our meta-analysis,pedicle screw insertion using navigational techniques led to a significantly lower incidence of screw-related complications compared to conventional methods(P=0.008).
The results of this meta-analysis should be interpreted with caution due to several limitations.First, only three studies were RCTs,and most data included in the present study were reported from nonrandomized,controlled trials.A meta-analysis of such data leads to less powerful results compared to those obtained purely from randomized studies.However, it is difficult to conduct a prospective randomized trial to answer these types of questions due to poor patient compliance,different patient demographic characteristics and different indications for surgery.Second, methods and tools used to assess postoperative screw position vary across studies,and these differences are usually associated with heterogeneity among studies. Furthermore,technical issues,such as differences in surgeons′skills,varying complexity of the surgery, and screw/pedicle dimensions could be responsible for this reported heterogeneity.Other limitationsinclude the heterogeneity of different navigation techniques and the different spine levels instrumented. Although the outcome of the current study indicated a significant difference,the funnel plots based on each grade of screw showed obvious publication bias as authors are more likely to report positive outcomes. We also only included papers written in English.
In conclusion,our study showed that the accuracy and complication rate of pedicle screw insertion using navigation techniques was superior to those obtained using conventional techniques.Furthermore,research in this area should include RCTs with well-planned methodologies to limit bias and report on validated patient-based outcome measures.
The outcome of this meta-analysis found that the accuracy and complication rate of pedicle screw insertion using navigation techniques was superior to those obtained using conventional techniques.More RCTs of high quality are needed to strengthen the quality of evidence.
[1] Allam Y,Silbermann J,Riese F,Greiner-Perth R. Computer tomography assessment of pedicle screw placement in thoracic spine:comparison between free hand and a generic 3D-based navigation techniques.Eur Spine J 2013;22:648-53.
[2] Amato V,Giannachi L,Irace C,Corona C.Accuracy of pedicle screw placement in the lumbosacral spine using conventional technique:computed tomography postoperative assessment in 102 consecutive patients.J Neurosurg Spine 2010;12:306-13.
[3] Amiot LP,Lang K,Putzier M,Zippel H,Labelle H. Comparative results between conventional and computerassisted pedicle screw installation in the thoracic,lumbar, and sacral spine.Spine(Phila Pa 1976)2000;25:606-14.
[4] Belmont PJ,Klemme WR,Robinson M,Polly DJ. Accuracy of thoracic pedicle screws in patients with and without coronal plane spinal deformities.Spine(Phila Pa 1976)2002;27:1558-66.
[5] Berlemann U,Heini P,Muller U,Stoupis C,Schwarzenbach O.Reliability of pedicle screw assessment utilizing plain radiographs versus CT reconstruction.Eur Spine J 6:406-10,1997.
[6] Castro WH,Halm H,Jerosch J,Malms J,Steinbeck J, Blasius S.Accuracy of pedicle screw placement in lumbar vertebrae.Spine(Phila Pa 1976)1996;21:1320-4.
[7] Cho W,Cho SK,Wu C.The biomechanics of pedicle screw-based instrumentation.J Bone Joint Surg Br 2010;92:1061-5.
[8] Choi WW,Green BA,Levi AD.Computer-assisted fluoroscopic targeting system for pedicle screw insertion. Neurosurgery 2000;47:872-8.
[9] Cui G,Wang Y,Kao TH,Zhang Y,Liu Z,Liu B,et al. Application of intraoperative computed tomography with or without navigation system in surgical correction of spinal deformity:a preliminary result of 59 consecutive human cases.Spine(Phila Pa 1976)2012;37:891-900.
[10]Farber GL,Place HM,Mazur RA,Jones DE,Damiano TR.Accuracy of pedicle screw placement in lumbar fusions by plain radiographs and computed tomography. Spine(Phila Pa 1976)1995;20:1494-9.
[11]Fisher CG,Sahajpal V,Keynan O,Boyd M,Graeb D, Bailey C,et al.Accuracy and safety of pedicle screw fixation in thoracic spine trauma.J Neurosurg Spine 2006;5:520-6.
[12]Fu TS,Wong CB,Tsai TT,Liang YC,Chen LH,Chen WJ. Pedicle screw insertion:computed tomography versus fluoroscopic image guidance.Int Orthop 2008;32:517-21.
[13]Gautschi OP,Schatlo B,Schaller K,Tessitore E. Clinically relevant complications related to pedicle screw placement in thoracolumbar surgery and their management:a literature review of 35,630 pedicle screws. Neurosurg Focus 2011;31:E8.
[14]Gelalis ID,Paschos NK,Pakos EE,Politis AN, Arnaoutoglou CM,Karageorgos AC,et al.Accuracy of pedicle screw placement:a systematic review of prospective in vivo studies comparing free hand,fluoroscopy guidance and navigation techniques.Eur Spine J 2012;21: 247-55.
[15]Gertzbein SD,Robbins SE.Accuracy of pedicular screw placement in vivo.Spine(Phila Pa 1976)1990;15:11-4.
[16]Guzey FK,Emel E,Hakan SM,Serdar BN,Ozkan N,Sel B,et al.Accuracy of pedicle screw placement for upper and middle thoracic pathologies without coronal plane spinal deformity using conventional methods.J Spinal Disord Tech 2006;19:436-41.
[17]Han W,Gao ZL,Wang JC,Li YP,Peng X,Rui J,et al. Pedicle screw placement in the thoracic spine:a comparison study of computer-assisted navigation and conventional techniques.Orthopedics 2010;33:doi:10.3928/ 01477447-20100625-14.
[18]Hart RA,Hansen BL,Shea M,Hsu F,Anderson GJ. Pedicle screw placement in the thoracic spine:a comparison of image-guided and manual techniques in cadavers. Spine(Phila Pa 1976).2005;30:E326-31.
[19]Hicks JM,Singla A,Shen FH,Arlet V.Complications of pedicle screw fixation in scoliosis surgery:a systematic review.Spine(Phila Pa 1976)2010;35:E465-70.
[20]Ishikawa Y,Kanemura T,Yoshida G,Ito Z,Muramoto A, Ohno S.Clinical accuracy of three-dimensional fluoroscopy-based computer-assisted cervical pedicle screw placement:a retrospective comparative study of conventional versus computer-assisted cervical pedicle screw placement.J Neurosurg Spine 2010;13:606-11.
[21]Kim HS,Heller JG,Hudgins PA,Fountain JA.The accuracy of computed tomography in assessing cervical pedicle screw placement.Spine(Phila Pa 1976)2003;28:2441-6
[22]Kim YJ,Lenke LG,Bridwell KH,Cho YS,Riew KD. Free hand pedicle screw placement in the thoracic spine: is it safe?Spine(Phila Pa 1976)2004;29:333-42;discussion 342.
[23]Kosmopoulos V,Schizas C.Pedicle screw placement accuracy:a meta-analysis.Spine(Phila Pa 1976) 2007;32:E111-20.
[24]Kotani Y,Abumi K,Ito M,Takahata M,Sudo H, Ohshima S,et al.Accuracy analysis of pedicle screw placement in posterior scoliosis surgery:comparison between conventional fluoroscopic and computer-assisted technique.Spine(Phila Pa 1976)2007;32:1543-50.
[25]Laine T,Lund T,Ylikoski M,Lohikoski J,Schlenzka D. Accuracy of pedicle screw insertion with and without computer assistance:a randomised controlled clinical study in 100 consecutive patients.Eur Spine J 2000;9: 235-40.
[26]Laine T,Schlenzka D,Makitalo K,Tallroth K,Nolte LP, Visarius H.Improved accuracy of pedicle screw insertion with computer-assisted surgery.A prospective clinical trial of 30 patients.Spine(Phila Pa 1976)1997;22: 1254-8.
[27]Li G,Lv G,Passias P,Kozanek M,Metkar US,Liu Z,et al. Complications associated with thoracic pedicle screws in spinal deformity.Eur Spine J 2010;19:1576-84.
[28]Li SG,Sheng L,Zhao H,Zhang JG,Zhai JL,Zhu Y. Clinical applications of computer-assisted navigation technique in spinal pedicle screw internal fixation. Zhong hua Yi Xue Za Zhi 2009;89:736-9.
[29]Lim MR,Girardi FP,Yoon SC,Huang RC,Cammisa FJ. Accuracy of computerized frameless stereotactic imageguided pedicle screw placement into previously fused lumbar spines.Spine(Phila Pa 1976)2005;30: 1793-8.
[30]Lonstein JE,Denis F,Perra JH,Pinto MR,Smith MD, Winter RB.Complications associated with pedicle screws.J Bone Joint Surg Am 1999;81:1519-28.
[31]Merloz P,Troccaz J,Vouaillat H,Vasile C,Tonetti J,Eid A,et al.:Fluoroscopy-based navigation system in spine surgery.Proc Inst Mech Eng H 2007;221:813-20.
[32]Merloz P,Tonetti J,Pittet L,Coulomb M,Lavallee S, Sautot P.Pedicle screw placement using image guided techniques.Clin Orthop Relat Res 1998;39-48.
[33]Mirza SK,Wiggins GC,Kuntz CT,York JE,Bellabarba C,Knonodi MA,et al.Accuracy of thoracic vertebral body screw placement using standard fluoroscopy, fluoroscopic image guidance,and computed tomographic image guidance:a cadaver study.Spine(Phila Pa 1976) 2003;28:402-13.
[34]Nottmeier EW,Seemer W,Young PM.Placement of thoracolumbar pedicle screws using three-dimensional image guidance:experience in a large patient cohort.J Neurosurg Spine 2009;10:33-9.
[35]Odgers CT,Vaccaro AR,Pollack ME,Cotler JM. Accuracy of pedicle screw placement with the assistance of lateral plain radiography.J Spinal Disord 1996;9: 334-8.
[36]Panjabi MM,Takata K,Goel V,Federico D,Oxland T, Duranceau J,et al.Thoracic human vertebrae.Quantitative three-dimensional anatomy.Spine(Phila Pa 1976) 1991;16:888-901.
[37]Rajasekaran S,Vidyadhara S,Ramesh P,Shetty AP. Randomized clinical study to compare the accuracy of navigated and non-navigated thoracic pedicle screws in deformity correction surgeries.Spine(Phila Pa 1976) 2007;32:E56-64.
[38]Rao G,Brodke DS,Rondina M,Bacchus K,Dailey AT. Inter-and intraobserver reliability of computed tomography in assessment of thoracic pedicle screw placement. Spine(Phila Pa 1976)2003;28:2527-30.
[39]Sakai Y,Matsuyama Y,Nakamura H,Katayama Y, Imagama S,Ito Z,et al.Segmental pedicle screwing for idiopathic scoliosis using computer-assisted surgery.J Spinal Disord Tech 2008;21:181-6.
[40]Schulze CJ,Munzinger E,Weber U.Clinical relevance of accuracy of pedicle screw placement.A computed tomographic-supported analysis.Spine(Phila Pa 1976) 1998;23:2215-20;discussion 2220-1.
[41]Schwarzenbach O,Berlemann U,Jost B,Visarius H,Arm E,Langlotz F,et al.Accuracy of computer-assisted pedicle screw placement.An in vivo computed tomography analysis.Spine(Phila Pa 1976)1997;22:452-8.
[42]Shin MH,Ryu KS,Park CK.Accuracy and Safety in Pedicle Screw Placement in the Thoracic and Lumbar Spines:Comparison Study between Conventional CArm Fluoroscopy and Navigation Coupled with OArm(R)Guided Methods.J Korean Neurosurg Soc 2012;52:204-9
[43]Silbermann J,Riese F,Allam Y,Reichert T,Koeppert H, Gutberlet M.Computer tomography assessment of pedicle screw placement in lumbar and sacral spine:comparison between free-hand and O-arm based navigation techniques.Eur Spine J 2011;20:875-81.
[44]Smorgick Y,Millgram MA,Anekstein Y,Floman Y, Mirovsky Y.Accuracy and safety of thoracic pedicle screw placement in spinal deformities.J Spinal Disord Tech 2005;18:522-6.
[45]Suk SI,Lee CK,Kim WJ,Chung YJ,Park YB.Segmental pedicle screw fixation in the treatment of thoracic idiopathic scoliosis.Spine(Phila Pa 1976)1995;20:1399-405.
[46]Tian NF,Huang QS,Zhou P,Zhou Y,Wu RK,Lou Y, et al.Pedicle screw insertion accuracy with different assisted methods:a systematic review and meta-analysis of comparative studies.Eur Spine J 2011;20:846-59.
[47]Tian NF,Xu HZ.Image-guided pedicle screw insertion accuracy:a meta-analysis.Int Orthop 2009;33:895-903.
[48]Tohtz SW,Rogalla P,Taupitz M,Perka C,Winkler T, Putzier M.Inter-and intraobserver variability in the postoperative evaluation of transpedicular stabilization:computed tomography versus magnetic resonance imaging. Spine J 2010;10:285-90.
[49]Vaccaro AR,Rizzolo SJ,Balderston RA,Allardyce TJ, Garfin SR,Dolinskas C,et al.Placement of pedicle screws in the thoracic spine.Part II:An anatomical and radiographic assessment.J Bone Joint Surg Am 1995;77:1200-6.
[50]Vaccaro AR,Rizzolo SJ,Allardyce TJ,Ramsey M,Salvo J,Balderston RA,et al.Placement of pedicle screws in the thoracic spine.Part I:Morphometric analysis of the thoracic vertebrae.J Bone Joint Surg Am 1995;77:1193-9.
[51]Van de Kelft E,Costa F,Van der Planken D,Schils F. A prospective multicenter registry on the accuracy of pedicle screw placement in the thoracic,lumbar,and sacral levels with the use of the O-arm imaging system and StealthStation Navigation.Spine(Phila Pa 1976) 2012;37:E1580-7.
[52]Verma R,Krishan S,Haendlmayer K,Mohsen A. Functional outcome of computer-assisted spinal pedicle screw placement:a systematic review and meta-analysis of 23 studies including 5,992 pedicle screws.Eur Spine J 2010;19:370-5.
[53]Wang B,Lu G,Chen R,Kang Y,Li J,Chen F,et al. Accuracy of free-hand thoracic pedicle screw placement in severe idiopathic scoliosis via CT scan.Zhong Nan Da Xue Xue Bao Yi Xue Ban 2009;34:226-9.
[54]Weinstein JN,Spratt KF,Spengler D,Brick C,Reid S. Spinal pedicle fixation:reliability and validity of roentgenogram-based assessment and surgical factors on successful screw placement.Spine(Phila Pa 1976)1988;13:1012-8.
[55]Wu H,Gao ZL,Wang JC,Li YP,Xia P,Jiang R.Pedicle screw placement in the thoracic spine:a randomized comparison study of computer-assisted navigation and conventional techniques.Chin J Traumatol 2010;13:201-5.
[56]Yu X,Xu L,Bi LY.Spinal navigation with intraoperative 3D-imaging modality in lumbar pedicle screw fixation.Zhong hua Yi Xue Za Zhi 2008;88: 1905-8.
[57]Zausinger S,Scheder B,Uhl E,Heigl T,Morhard D, Tonn JC.Intraoperative computed tomography with integrated navigation system in spinal stabilizations.Spine 2009;(Phila Pa 1976)34:2919-26.
Retraction:Physical and degradation properties of PLGA scaffolds fabricated by salt fusion technique.
The paper entitled‘‘Physical and degradation properties of PLGA scaffolds fabricated by salt fusion technique.J Biomed Res 27(4),318-325(DOI:10.7555/JBR.27.20130001)’’has been retracted.The paper is withdrawn at the request of the editor as it contains plagiarized materials from Murphy,William L.,et al.‘‘Salt fusion:an approach to improve pore interconnectivity within tissue engineering scaffolds.’’Tissue engineering 8.1(2002):43-52.The Publisher apologizes for any inconvenience this may cause.
Received 14 October 2013,Revised 20 January 2014,Accepted 16 March 2014,Epub 12 April 2014
?Corresponding author:Xiaojian Cao,Department of Orthopedics,the First Affiliated Hospital of Nanjing Medical University,Nanjing,Jiangsu 210029,China.Tel/Fax:+86013002505801/+86-025-83724440,
E-mail:xiaojiancao@gmail.com.
The authors reported no conflict of interests.
?2014 by the Journal of Biomedical Research.All rights reserved.
10.7555/JBR.28.20130159
 THE JOURNAL OF BIOMEDICAL RESEARCH2014年3期
THE JOURNAL OF BIOMEDICAL RESEARCH2014年3期
- THE JOURNAL OF BIOMEDICAL RESEARCH的其它文章
- Analytical characteristics of a qPCR-based molecular diagnostic assay-conceptual considerations for laboratory personnel
- Drainage vs.non-drainage after cholecystectomy for acute cholecystitis:a retrospective study
- Correlation of obstructive sleep apnea hypopnea syndrome with metabolic syndrome in snorers
- Class A scavenger receptor activation inhibits endoplasmic reticulum stress-induced autophagy in macrophage
- Expression of human hepatic lipase negatively impacts apolipoprotein A-I production in primary hepatocytes from Lipc-null mice
- A genetic variant in pseudogene E2F3P1contributes to prognosis of hepatocellular carcinoma