
Acupuncture at the Taixi (KI3) acupoint activates cerebral neurons in elderly patients with mild cognitive impairment
2014-03-27 01:17:46ShangjieChenMaoshengXuHongLiJiupingLiangLiangYinXiaLiuXinyanJiaFenZhuDanWangXueminShiLihuaZhao
中國神經(jīng)再生研究(英文版) 2014年11期
Shangjie Chen, Maosheng Xu, Hong Li, Jiuping Liang, Liang Yin, Xia Liu, Xinyan Jia Fen Zhu Dan Wang Xuemin Shi, Lihua Zhao
1 Department of Rehabilitation, Baoan Hospital, Southern Medical University, Shenzhen, Guangdong Province, China
2 Department of Acupuncture and Moxibustion, First Af fi liated Hospital of Tianjin University of Traditional Chinese Medicine, Tianjin, China
3 Department of Imaging, Baoan Hospital, Southern Medical University, Shenzhen, Guangdong Province, China
4 School of Chinese Medicine, Hong Kong Baptist University, Hong Kong Special Administrative Region, China
5 College of Acupuncture and Moxibustion, Guangxi University of Traditional Chinese Medicine, Nanning, Guangxi Zhuang Autonomous Region, China
Acupuncture at the Taixi (KI3) acupoint activates cerebral neurons in elderly patients with mild cognitive impairment
Shangjie Chen1,2, Maosheng Xu3, Hong Li4, Jiuping Liang2, Liang Yin3, Xia Liu2, Xinyan Jia1, Fen Zhu1, Dan Wang1, Xuemin Shi2, Lihua Zhao5
1 Department of Rehabilitation, Baoan Hospital, Southern Medical University, Shenzhen, Guangdong Province, China
2 Department of Acupuncture and Moxibustion, First Af fi liated Hospital of Tianjin University of Traditional Chinese Medicine, Tianjin, China
3 Department of Imaging, Baoan Hospital, Southern Medical University, Shenzhen, Guangdong Province, China
4 School of Chinese Medicine, Hong Kong Baptist University, Hong Kong Special Administrative Region, China
5 College of Acupuncture and Moxibustion, Guangxi University of Traditional Chinese Medicine, Nanning, Guangxi Zhuang Autonomous Region, China
Our previous fi ndings have demonstrated that acupuncture at the Taixi (KI3) acupoint in healthy youths can activate neurons in cognitive-related cerebral cortex. Here, we investigated whether acupuncture at this acupoint in elderly patients with mild cognitive impairment can also activate neurons in these regions. Resting state and task-related functional magnetic resonance imaging showed that the pinprick senstation of acupuncture at the Taixi acupoint differed signi fi cantly between elderly patients with mild cognitive impairment and healthy elderly controls. Results showed that 20 brain regions were activated in both groups of participants, including the bilateral anterior cingulate gyrus (Brodmann areas [BA] 32, 24), left medial frontal cortex (BA 9, 10, 11), left cuneus (BA 19), left middle frontal gyrus (BA 11), left lingual gyrus (BA 18), right medial frontal gyrus (BA 11), bilateral inferior frontal gyrus (BA 47), left superior frontal gyrus (BA11), right cuneus (BA 19, 18), right superior temporal gyrus (BA 38), left subcallosal gyrus (BA 47), bilateral precuneus (BA 19), right medial frontal gyrus (BA 10), right superior frontal (BA 11), left cingulate gyrus (BA 32), left precentral gyrus (BA 6), and right fusiform gyrus (BA 19). These results suggest that acupuncture at the Taixi acupoint in elderly patients with mild cognitive impairment can also activate some brain regions.
nerve regeneration; acupuncture; acupoint; Taixi (KI3); acupoint specificity; mild cognitive impairment; functional MRI; resting state; cognitive function; brain function; NSFC; neural regeneration
Funding: This study was supported by the National Natural Science Foundation of China, No. 81173354; the Natural Science Foundation of Guangdong Province, No. 10451810101005862; a grant from Guangdong Administration of Traditional Chinese Medicine, No. 20111032, 20132019; the Science and Technology Plan Project of Baoan District, Shenzhen City, No. 200902159.
Chen SJ, Xu MS, Li H, Liang JP, Yin L, Liu X, Jia XY, Zhu F, Wang D, Shi XM, Zhao LH. Acupuncture at the Taixi (KI3) acupoint activates cerebral neurons in elderly patients with mild cognitive impairment. Neural Regen Res. 2014;9(11):1163-1168.
Introduction
At present, functional magnetic resonance imaging (fMRI) is the most important MRI-related technique for studying the mechanisms underlying acupuncture. Most fMRI studies focus on the immediate effect of acupoint acupuncture (Chen et al., 2008, 2011; Zhou and Jia, 2008; Asghar et al., 2010; Bai et al., 2010; Hui et al., 2010; Gopinath et al., 2011; Liu et al., 2011). These studies explain the speci fi city of acupoint from different points of view. Chae et al. (2009) compared verum acupuncture with sham acupuncture at the Xingjian (LR2) acupoint and found that true acupuncture elicited significant activation in motor function-related brain regions. They suggest that acupuncture at the Xingjian acupoint modulated the affective components of the pain matrix and that verum acupuncture-induced brain activation provides a neurobiological basis of acupuncture. Another study has demonstrated that differential activation resulting from verum or sham acupuncture may be attributed to the more varied and stronger sensations evoked by verum acupuncture. It further suggests that acupuncture can activate the resting brain networks, which include anti-nociceptive, memory and affective brain regions (Dhond et al., 2008). However, most of the subjects involved in the above-mentioned studies are healthy. According to traditional Chinese medicine theory, the effect of acupoint acupuncture is best observed in people who are ill or suffering, and it is dif fi cult to evoke the effect in healthy people. Therefore, studying acupoint specificity with regards to a disease is necessary to fi nd the neural targetof the acupoint. The best condition to study is mild brain injury in which patients suffer minimal impairments and are close to a normal condition.

Figure 1 Schematic diagram of acupuncture at the Taixi (KI3) acupoint.
At present, a large number of studies have investigated cognitive-related acupoints using healthy subjects or Alzheimer’s disease patients. For example, a comparison of acupuncture at the Shenmen (HT7, a cognitive-related acupoint) and Yanglao (SI6, a non-related acupoint) in healthy young participants showed that acupuncture at Shenmen can activate corresponding cognitive areas, and was associated with meridian circulation and acupoint speci fi city (Chen et al., 2008). Electric acupuncture directed at the injured brain regions of Alzheimer’s disease patients potentially alleviates some Alzheimer’s disease-related de fi cits (Bai et al., 2009b). These regions include the hippocampus, insula, parietal cortex, temporal cortex, and cerebellum, all of which are closely related to Alzheimer’s disease and underlie the mechanism by which this acupuncture induces its effects. Because Alzheimer’s disease patients often do not cooperate well with physicians, data is often corrupted due to movements during scanning. Patients with mild cognitive impairment (MCI) do not have extensive brain pathologies, and electroencephalographic signals are not greatly different from those of healthy people. Moreover, they cooperate with physicians, making experiments more efficient. To the best of our knowledge, few functional magnetic resonance imaging studies have been reported regarding acupuncture in patients with MCI. Our previous fi ndings demonstrated that acupuncture at the Taixi (KI3) acupoint can activate regions corresponding to cognitive function (Chen et al., 2009). To better re fl ect the effect of acupuncture at cognitive-related acupoints, here, we investigated brain activation after acupuncture at the Taixi in elderly patients with MCI and healthy elderly controls.
Subjects and Methods
Subjects
Twelve elderly patients with MCI and twelve healthy elderly controls were recruited according to inclusion and exclusion criteria. Inclusion criteria for healthy, elderly controls were: (1) education level greater than middle school, (2) mentally healthy as confirmed by body examination in an upper second-class hospital, and (3) a body-mass index between 20 and 24.
Elderly MCI patients were diagnosed with MCI following MCI diagnostic criteria (Petersen, 2004).
MCI patients were excluded if they met any one of the following: (1) education level greater than middle school, (2) uncomfortable within 1 week after examination, (3) severe visual or hearing disorders, or aphasia, (4) presence of mental within the body, a history of surgery or tattooing, (5) unable to undergo magnetic resonance imaging due to fear or other factors, (6) a disease focus or suspected focus in the brain, (7) suspected pathology based on blood examination or electrocardiogram, (8) a history of mental disease or epilepsy, (9) a history of alcohol or drug abuse, or (10) pre-menopausal women.
The experiment was terminated if any of the following events occurred: (1) the participant felt uncomfortable or an adverse event occurred during the scanning, (2) the participant was unsuitable for MRI scans because of mood of fear and other reasons, (3) the MRI magnetic fi eld was non-homogeneous, (4) a disease focus or suspected focus in the brain, (5) or abnormal activity during scanning.
All participants were right handed and aged between 55 and 70 years. The informed consents were obtained from all the participants. The elderly patients with MCI and healthy elderly controls were subjected to evaluation by the Clinical Dementia Rating scale score and Mini-Mental State Examination score. The experimental protocol was approved by Ethics Committee, Shenzhen Baoan Hospital, Southern Medical University, China.
Methods
Resting state and task-related fMRI signals were recorded (Figure 1). A 9-minute fMRI scan was performed, consisting of a resting state period of 6 minutes (R) and a task period of 3 minutes. The task period included needling, retention (1 minute), and twirling (2 minutes).
Acupuncture
Acupuncture at the Taixi acupoint on the right side was performed in both groups of participants by the same physician who had over 10 years of clinical experience in acupuncture and moxibustion. After routine disinfection, a tip of a 0.35 × 25 mm silver needle (silver content 85%; Huatuo Brand, Suzhou Huatuo Acupuncture Instruments General Factory, China) was perpendicularly pricked into the Taixi acupoint at a depth of 12 mm (Figure 1). One minute later, the needle was twirled at approximately 60° for 2 minutes at a rate of 120 twirls/min (Bian and Zhang, 2003).
fMRI
All scans were performed using a 3.0T MRI scanner (Philips, Amsterdam, the Netherlands). After head fi xation, anatomic and functional imaging was performed. Precisely, axial anatomic imaging was performed using a gradient-echo echo planar imaging sequence. Data were collected at the level parallel to the line anterior commissure-posterior commissure axis, and from the area covering the entire brain. The parameters were: repetition time (TR) = 2 s, echo time (TE) = 30 ms, fi eld of view (FOV) = 22 mm × 22 cm, Flip angle = 77°, matrix = 64 × 64, slice thickness = 4 mm, slice interval = 1 mm, total number 30 slices. For anatomic imaging, T1-weighted gradient-echo sequence was used. Functional images were obtained at the same orientation as the anatomic images. The parameters were: TR = 2.1 seconds, TE = 4.6 ms, matrix= 256 × 256, FOV = 230 mm × 230 cm, fl ip angle = 8°, slice thickness = 1 mm.

Table 1 Comparison of baseline data between elderly patients with mild cognitive impairment and healthy elderly controls
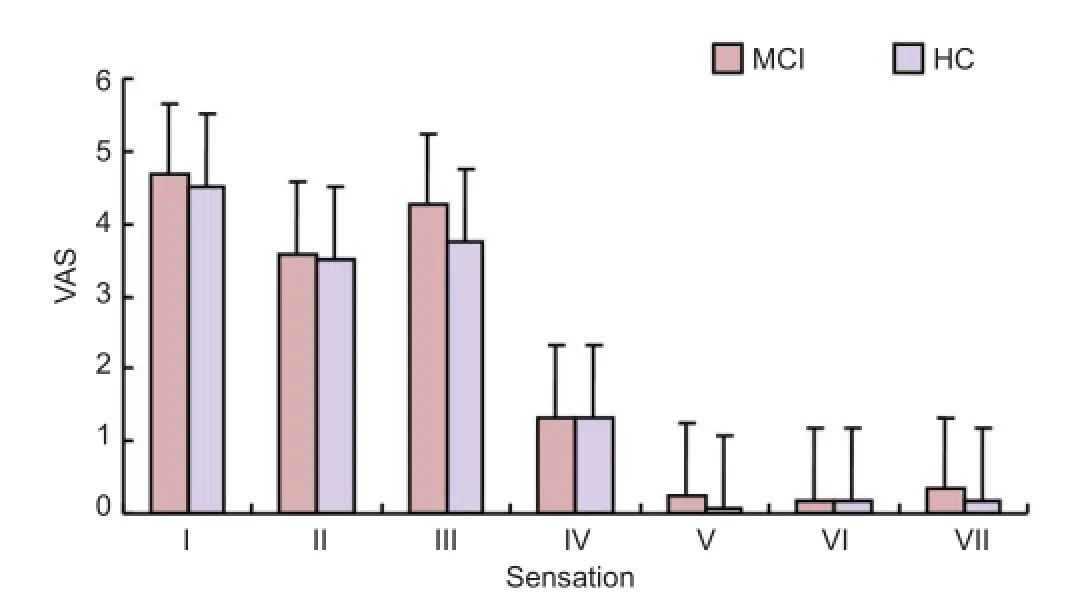
Figure 2 Comparison of pinprick sensation between elderly patients with mild cognitive impairment and healthy elderly controls.
Observation indices
Several indices were used to score the acupuncture. (1) Pinprick sensation indices: after acupuncture, needling sensation was quantified using the Visual Analogue Scale (VAS) (scale: 0 = no feeling, 1-3 = minor, 4-6 medium, 7-8 = strong, 9 = very strong, and 10 = unbearable). The pinprick sensation indices included overall feeling, soreness, numbness, coldness, hotness, sharp pain, blunt pain, heaviness, tingling, itching, continuous pain, extrusion feeling, and present pain intensity (Hui et al., 2010). (2) Activation indices: Comparison of brain regions activated by acupuncture at KI3. (3) Safety index: accidents including broken needles, stuck needles, hematoma, fainting, convulsion during the scanning process, observed by the researchers and whether participants felt subjective discomfort.
Image analysis and data post-processing
Data were analyzed using SPM5 software (http://www.fil. ion.ucl.ac.uk/spm/software/spm5). First, data conversion and pre-processing (slice timing, realignment, normalization and smoothing) were performed, followed by general linear model (GLM) analysis. Image of each subject at rest (0-6 minutes) and during acupuncture (6-9 minutes) were subjected to GLM analysis. The GLM was applied to the whole brain of each subject, and parameter estimates were obtained for all voxels. Different comparison charts in response to stimuli were obtained by comparing brain activity using the acupuncture. The activation caused by acupuncture stimulation was analyzed using a two-sample t-test with a signi fi cant level of P < 0.005 and a cluster-size greater than 10.

Figure 3 Comparison of brain regions activated by acupuncture at the Taixi (KI3) acupoint in mild cognitive impairment patients and healthy controls.
Statistical analysis
Measurement data are expressed as mean ± SD, and numeration data as percentage. SPM5 software was used for data analysis. Two-sample t-test and chi-square test were used for comparison between groups. A level of P < 0.05 was considered statistically signi fi cant.
Results
Quantitative analysis of subjects
All subjects were included in the final analysis, without dropouts.
Baseline data
There were no signi fi cant differences in age, gender, or educational level between MCI patients and the healthy controls (P > 0.05). The Clinical Dementia Rating scale score and Mini-Mental State Examination score for the elderly patients with MCI were signi fi cantly higher than that for the control subjects (P < 0.01;Table 1).
Comparisons of pinprick sensation after acupuncture at theTaixipoint
The pinprick sensation was evaluated by the VAS and pri-marily included soreness, numbness, distension, tepid feeling, and a few sharp pains. There were no significant differences in pinprick sensation between the two groups of participants (P > 0.05;Figure 2).

Table 2 Brain regions activated by acupuncture at the Taixi acupoint (data from both participant groups are combined)
Brain regions activated by acupuncture at theTaixiacupoint in elderly MCI patients and healthy elderly controls
Acupuncture at the Taixi acupoint activated the same 20 regions in both groups of participants (Table 2,Figure 3).
Safety evaluation
During acupuncture, no needles were broken or stuck, and no hematoma, fainting, or other adverse reactions were observed.
Discussion
All pinprick sensations that occur during needle retaining result in brain activation. Multi-group design, found in many previous fMRI studies regarding acupuncture have considered the period of needle retaining to be the resting state (Zhou and Jia, 2008; Chae et al., 2009; Hui et al., 2010). This is contradictory to clinical evidence, theory, and the underlying mechanism of acupuncture and moxibustion. The clinical practice of acupuncture and moxibustion has demonstrated that the resting state during needle retaining is not a pure resting state, but rather, is associated with a marked effect. Several studies have demonstrated that the effect of acupuncture continues even after needle manipulation is complete, and should be taken into consideration during study design and data analysis (Bai et al., 2009a; Chen et al., 2012). More attention should be paid to the effects of acupuncture at each stage of the procedure when selecting baseline data. The conventional multi-group design-based linear analysis produces biased results, underestimates brain activity, and leads to artifacts, all of which are not suitable for fMRI studies. Recently, although a large number of studies have considered the brain activation caused by needle retaining, the resting state after needle insertion is still considered a pure resting state. However, clinical practice and related experimental fi ndings have shown that brain activation after needle insertion can still in fl uence the fi nal results (Zhang et al., 2009). fMRI studies of the resting-state during acupuncture have increased in recent years (Xue et al., 2011; Feng et al., 2012; Zhong et al., 2012). However, resting-state data only re fl ect post-acupuncture effects, not the activation during acupuncture, and are therefore unsuitable for detecting the immediate effects of acupuncture in the brain. For this reason, here we chose the period before acupuncture as the resting state baseline in order to avoid the in fl uence of needle insertion and the lasting effects that occur after acupuncture. This method can be used to effectively evaluate brain activation during acupuncture.
Traditional Chinese medicine theory holds that acupoint acupuncture has wide therapeutic effects. For example, acupuncture at the Taixi acupoint can be used to treat a number of disorders, including deafness, tinnitus, insomnia, nocturnal emission, impotence, renal disease, headache, toothache, and cognitive disorder. The precise effect of acupoint acupuncture should be exerted under some pathological condition because the effect in normal persons is sporadic. Acupuncture and moxibustion can maintain homeostasis and improve the pathological state in patients (Plummer, 1981; Kaptchuk, 2002). However, most acupuncture-related fMRI studies use healthy individuals, which leads to abnormal results. In this study, the brain activation induced byacupuncture at a cognitive-related acupoint was investigated under the pathological conditions, which better reflect the speci fi city of the acupoint.
People suffer from many types of cognitive disorders, but those with MCI were the most suitable subjects for this study. Early intervention in MCI is a key to prevention and treatment of Alzheimer’s disease, thus studying potential intervention methods is extremely important. Dementia is a mental state that leads to disability (25.1%) and stroke (11.4%) in elderly Chinese and other developing countries (Sabat, 2009). In that study, the reported survival of dementia was 478 days, which is equivalent to the death rate of advanced cancer. Biomedical interventions for treating and preventing dementia are lacking (Sabat, 2009). Once Alzheimer’s disease manifests, it likely cannot be reversed. Therefore, prevention and treatment should be started before the presence of initial symptoms, and a long time period of treatment with bearable adverse events is required (Mucke, 2009). The 5-year conversion rate of MCI to dementia is 10-15%, with a cumulative conversion rate of 31.4% (Mitchell and Shiri-Feshki, 2008). Therefore, treatment should focus on people with MCI, who are at higher risk of developing Alzheimer’s disease than the general population. At present, most drugs for MCI were previously used to treat dementia, and their ef fi cacies are uncertain and can produce unwanted effects. For example, anti-inflammatory agents previously used for treating dementia can actually increase the risk of developing dementia (Breitner et al., 2009). The safety of drugs used to treat MCI needs to be evaluated (Chen et al., 2008). There are no drugs that reliably postpone progression of Alzheimer’s disease or the development of dementia for long time periods (Farlow, 2009). Acupuncture and moxibustion have low incidences of side effects and few adverse reactions (Cheng et al., 2008; Wang et al., 2012). Therefore, acupuncture, should be considered more seriously as treatment for MCI. MCI is a disease suitable for explaining the brain function speci fi city of acupuncture at cognitive-related acupoints.
The pathological location of MCI is in the brain, but the essential factor lies in the kidney. Strong evidence exists that MCI is closely related to the “kidney” in traditional Chinese medicine. The Taixi acupoint is one of the main acupoints clinically used for treatment of cognitive disorders. Although Taixi is near the Qiuxu (GB40) acupoint, the brain regions activated by the two are greatly different (Chen et al., 2011). Comparing verum and sham acupunctures using verum versus sham acupoints is widely used for investigating the acupoint speci fi city (Chae et al., 2009; Liu et al., 2011). To the best of our knowledge, there are few studies of acupuncture at acupoints with different functions. Results from this study demonstrated that sensations of acupuncture at the Taixi acupoint primarily consist of soreness, numbness, fullness, warmth, and sharp pain. There were no signi fi cant differences in pinprick sensations between elderly patients with MCI and healthy elderly controls in our small sample size.
Brain activation was found in many regions after acupuncture at Taixi in both elderly patients with MCI and healthy elderly controls. The following brain regions were activated: including the bilateral anterior cingulate gyrus (Brodmann areas [BA] 32, 24), left medial frontal gyrus (BA 9, 10, 11), left cuneus (BA 19), left middle frontal gyrus (BA11), left lingual gyrus (BA18), right middle frontal gyrus (BA 11), bilateral inferior frontal gyrus (BA 47), left superior frontal gyrus (BA 11), right cuneus (BA 19, 18), right superior temporal gyrus (BA 38), left subcallosal gyrus (BA 47), bilateral precuneus (BA 19), right medial frontal gyrus (BA 10), right superior frontal (BA 11), left cingulate gyrus (BA 32), left precentral gyrus (BA 6), and right fusiform gyrus (BA 19). BA18 and 19 are visual association cortex. Taixi is an origin acupoint of the kidney meridian. Acupuncture at the Taixi acupoint mainly activated cognitive-related brain areas. The eyes act as the window of the liver, but hepatic yin should be nourished by the “kidney” in traditional Chinese medicine. Therefore, Taixi is related to vision and thereby acupuncture can activate corresponding vision function areas. The limbic system is involved in the regulation learning, memory, emotion, stress, internal organ activities, and endocrine functions. The cingulate gyrus mainly participates in the regulation of internal organs and emotional expression. The limbic lobe, with the cingulate gyrus as its center, regulates the activity of internal organs, and it is also called the third association area of cerebral cortex (the other two being located in prefrontal and occipital-parietal-temporal junctional zone). BAs 32 and 24 are important components of the limbic system and participate in various physiological functions including affective pain. BA 9 is a part of dorsolateral prefrontal cortex, integrates information from many cortical subcortical regions, and is the center for cognitive functions. BA 6 contains premotor and supplementary motor areas. BAs 10, 11, and 47 are frontal regions closely related with cognitive functions. BAs 9, 10, and 11 are association areas of the frontal lobe and are closely related to intelligence and psychomotility. Results from this study demonstrated that compared to healthy elderly controls, acupuncture at the Taixi better activates cognitive-related brain areas in MCI patients. This finding suggests that acupoint acupuncture shows different effects under different cognitive states. Acupuncture at acupoints more obviously exerts effects under the pathological conditions.
Taken together, results from this study demonstrate that the Taixi acupoint is closely related to cognition, which supports the argument that acupuncture at the Taixi acupoint may be good treatment for MCI in the clinic, and lays the foundation for subsequent studies.
Author contributions:Xu MS, Liang JP, Yin L, and Liu X were responsible for data collection, integration, and analysis. Chen SJ was in charge of study conception and design, fundraising, and wrote the manuscript. Zhao LH, Li H, and Wang D provided suggestions on technique application and material collection, and translated the manuscript. Jia XY and Zhu F participated in experiments. Shi XM guided the study. All authors approved the final version of this paper.
Con fl icts of interest:None declared.
Asghar AU, Green G, Lythgoe MF, Lewith G, MacPherson H (2010) Acupuncture needling sensation: the neural correlates of deqi using fMRI. Brain Res 1315:111-118.
Bai LJ, Qin W, Tian J, Liu P, Li LL, Chen P, Dai JP, Craggs JG, von Deneen KM, Liu YJ (2009a) Time-varied characteristics of acupuncture effects in fMRI studies. Hum Brain Mapp 30:3445-3460.
Bai LJ, Qin W, Tian J, Dong MH, Pan XH, Chen P, Dai JP, Yang WH, Liu YJ (2009b) Acupuncture modulates spontaneous activities in the anticorrelated resting brain networks. Brain Res 1279:37-49.
Bai LJ, Tian J, Zhong CG, Xue T, You YB, Liu ZY, Chen P, Gong QY, Ai L, Qin W (2010) Acupuncture modulates temporal neural responses in wide brain networks: evidence from fMRI study. Mol Pain 6:73.
Bian J, Zhang C (2003) Conception and core of academician Shi Xuemin’s acupuncture manipulation quantitative arts. Zhongguo Zhen Jiu 5:287-289.
Breitner J, Haneuse S, Walker R, Dublin S, Crane P, Gray S, Larson E (2009) Risk of dementia and AD with prior exposure to NSAIDs in an elderly community-based cohort. Neurology 72:1899-1905.
Chae YY, Lee HJ, Kim HJ, Sohn HJ, Park JH, Park HJ (2009) The neural substrates of verum acupuncture compared to non-penetrating placebo needle: an fMRI study. Neurosci Lett 450:80-84.
Chen SJ, Liu B, Fu W, Wu S, Chen J, Ran P (2008) A fMRI observation on different cererbral regions activated by acupuncture of Shenmen (HT 7) and Yanglao (SI 6). Zhen Ci Yan Jiu 33:267-271.
Chen SJ, Zhu F, Liu B, Wu SS, Ran PC, Chen J, Shi XM (2009) fMRI studies of healthy young people by stimulating KI3 point and sham acupoint. Zhongguo Kangfu 24:308-309.
Chen SJ, Cheng HJ, Wu SS, Chen J, Ran PC, Shi XM (2011) Activation of various brain areas during acupuncture at Taixin (KI 3) and Qiuxu (GB 40) acupoints. Neural Regen Res 6:925-928.
Chen SJ, Meng L, Yan H, Bai L, Wang F, Huang Y, Li J, Peng X, Shi X (2012) Functional organization of complex brain networks modulated by acupuncture at different acupoints belonging to the same anatomic segment. Chin Med J (Engl) 125:2694-2700.
Cheng HY, Yu JC, Jiang ZG, Zhang XZ, Liu CZ, Peng YM, Chen FY, Qu Y, Jia YJ, Tian QF (2008) Acupuncture improves cognitive de fi cits and regulates the brain cell proliferation of SAMP8 mice. Neurosci Lett 432:111-116.
Dhond RP, Yeh C, Park K, Kettner N, Napadow V (2008) Acupuncture modulates resting state connectivity in default and sensorimotor brain networks. Pain 136:407-418.
Farlow M (2009) Treatment of mild cognitive impairment (MCI). Curr Alzheimer Res 6:362-367.
Feng YY, Bai LJ, Ren YS, Chen SJ, Wang H, Zhang WS, Tian J (2012) FMRI connectivity analysis of acupuncture effects on the whole brain network in mild cognitive impairment patients. J Magn Reson Imaging 30:672-682.
Gopinath K, Ringe W, Goyal A, Carter K, Dinse HR, Haley R, Briggs R (2011) Striatal functional connectivity networks are modulated by fMRI resting state conditions. Neuroimage 54:380-388.
Hui KK, Marina O, Liu J, Rosen BR, Kwong KK (2010) Acupuncture, the limbic system, and the anticorrelated networks of the brain. Auto Neurosci 157:81-90.
Kaptchuk TJ (2002) Acupuncture: theory, efficacy, and practice. Ann Intern Med 136:374-383.
Liu JX, Qin W, Guo Q, Sun JB, Yuan K, Dong MH, Liu P, Zhang Y, von Deneen KM, Liu YJ (2011) Divergent neural processes specific to the acute and sustained phases of verum and SHAM acupuncture. J Magn Reson Imaging 33:33-40.
Mitchell A, Shiri-Feshki M (2008) Temporal trends in the long term risk of progression of mild cognitive impairment: a pooled analysis. J Neurol Neurosurg Psychiatry 79:1386-1391.
Mucke L (2009) Neuroscience: Alzheimer’s disease. Nature 461:895-897.
Petersen RC (2004) Mild cognitive impairment as a diagnostic entity. J Intern Med 256:183-194.
Plummer J (1981) Acupuncture and homeostasis: physiological, physical (postural) and psychological. Am J Chin Med 9:1-14.
Sabat SR (2009) Dementia in developing countries: a tidal wave on the horizon. Lancet 374:1805-1806.
Wang ZQ, Nie BB, Li DH, Zhao ZL, Han Y, Song HQ, Xu JY, Shan BC, Lu J, Li KC (2012) Effect of acupuncture in mild cognitive impairment and Alzheimer disease: a functional MRI study. PLoS One 7:e42730.
Xue T, Bai LJ, Chen SJ, Zhong CG, Feng YY, Wang H, Liu ZY, You YB, Cui FY, Ren YS (2011) Neural speci fi city of acupuncture stimulation from support vector machine classi fi cation analysis. J Magn Reson Imaging 29:943-950.
Zhang Y, Qin W, Liu P, Tian J, Liang JM, von Deneen KM, Liu YJ (2009) An fMRI study of acupuncture using independent component analysis. Neurosci Lett 449:6-9.
Zhong CG, Bai LJ, Dai RW, Xue T, Wang H, Feng YY, Liu ZY, You YB, Chen SJ, Tian J (2012) Modulatory effects of acupuncture on resting-state networks: a functional MRI study combining independent component analysis and multivariate Granger causality analysis. J Magn Reson Imaging 35:572-581.
Zhou Y, Jia J (2008) Effect of acupuncture given at the HT 7, ST 36, ST 40 and KI3 acupoints on various parts of the brains of Alzheimer’s disease patients. Acupuncture Electro 33:1-2.
Copyedited by Guo Y, Chang XR, Philips A, Robens J, Wang J, Li CH, Song LP
10.4103/1673-5374.135319
Lihua Zhao, M.D., College of Acupuncture and Moxibustion, Guangxi University of Traditional Chinese Medicine, Nanning, Guangxi Zhuang Autonomous Region,
China, zhaolh67@163.com.
http://www.nrronline.org/
Accepted: 2014-05-09
- 中國神經(jīng)再生研究(英文版)的其它文章
- High matrix metalloproteinase-9 expression induces angiogenesis and basement membrane degradation in stroke-prone spontaneously hypertensive rats after cerebral infarction
- A viral vector expressing hypoxia-inducible factor 1 alpha inhibits hippocampal neuronal apoptosis
- Somatosensory stimulation suppresses the excitability of pyramidal cells in the hippocampal CA1 region in rats
- Heavy ion and X-ray irradiation alter the cytoskeleton and cytomechanics of cortical neurons
- Potential targets for protecting against hippocampal cell apoptosis after transient cerebral ischemiareperfusion injury in aged rats
- Neuroprotective effect of ischemic preconditioning in focal cerebral infarction: relationship with upregulation of vascular endothelial growth factor