
Integration of community pharmacies in an Italian colorectal cancer screening program: insights from the Local Health Authority of Bologna
2024-05-14 12:41:00AngelaChiereghinLorenzoPizziTizianaSannaLorenaSquillaceCarmenBazzaniLorenzoRotiFrancescaMezzetti
Angela Chiereghin, Lorenzo Pizzi, Tiziana Sanna, Lorena Squillace, Carmen Bazzani,Lorenzo Roti, Francesca Mezzetti
1Governance of Screening Programs Unit, Health Management Staff, Local Health Authority of Bologna, Bologna 40124, Italy.
2Screening Center, Department of Public Health, Local Health Authority of Bologna, Bologna 40124, Italy.
3Health Management, Local Health Authority of Bologna, Bologna 40124, Italy.
Abstract In Italy, a nationwide population-based colorectal cancer (CRC) screening initiative has been in place since 2006.In recent years, there has been a growing interest in involving community pharmacies in this activity.This commentary provides an insightful analysis of the integration between the screening program of the Local Health Authority (LHA) of Bologna (Northern Italy) and community pharmacies.A horizontal integration at the micro level with service and clinical integrations supported by meso-level policy (regional authority) was applied.Four types of integration such as normative, informational, financial and functional serving as enablers were implemented.A high level of depth of consensus, connectivity, communication, and trust was pursued.The program achieved large participation from community pharmacies, with 91.1% (n = 234) of pharmacies in the LHA territory actively participating.On average, each pharmacy served 1,228 (range, 1,021-1,519) target citizens.Between 2021 (the first full year under the community pharmacy model) and 2022, pharmacies delivered an annual mean of 68,295 kits(range, 12-840).In 2021, there was a remarkably high level of screening completion, with 93.7% of fecal immunochemical tests being returned to pharmacies.This percentage increased by 3.3% in 2022.In our setting,pharmacy involvement improved service quality by introducing complete traceability of kits and specimen flow, as well as temperature control.It also led to a 4.6% increase in attendance rates compared to the previous organizational model (61.6% vs.57%; P < 0.001).Finally, additional European experiences involving community pharmacies in organized CRC screening programs, resembling the Bologna setting, are reported.
Keywords: Population-based colorectal cancer screening program, community pharmacy, integration,organizational choices, service quality
INTRODUCTION
Context
The present comprehension of the pathogenesis and natural history of colorectal cancer (CRC) lends support to the concept that this is an ideal target for screening[1].Furthermore, effective screening methods,such as stool-based tests for occult blood (i.e., guaiac-based fecal occult blood test [gFOBT] or fecal immunochemical test [FIT]) and endoscopic methods (i.e., sigmoidoscopy and colonoscopy) are available[2].Over the last three decades, there have been significant advancements in genomics and molecular pathology related to cancer biomarkers, enabling a more personalized approach to therapy that positively influences survival outcomes[3].For instance, among the major genetic mutations in CRC, several studies support the notion that RAS mutations play a role in the development and progression of colorectal cancer and carry significant clinical implications[4].In particular, it has been reported that among patients with metastatic CRC, up to approximately 43% have RAS mutations and Kirsten RAS mutations are associated with poor response to anti-epidermal growth factor receptor therapy[3,5].Similarly, in recent years,both peripheral and local markers of cancer-related inflammation, such as lymphocyte-to-monocyte ratio,neutrophil-to-lymphocyte ratio, or platelet-to-lymphocyte ratio and tumor-infiltrating lymphocytes have been extensively investigated and deemed highly prognostic[6].The clinical value of microRNA panels in CRC patients is also now being explored[7].Finally, in patients with CRC, testing the DNA mismatch repair(MMR) status allows for prognostic stratification and/or the identification of patients at high risk for Lynch syndrome.MMR defective (dMMR) function leads to microsatellite instability (MSI) that occurs in about 15% of CRC cases.MSI occurs in the early stages of cancer and represents an important carcinogenic pathway.MSI is an important marker for identifying Lynch syndrome, with 90%-95% of cases showing high-frequency MSI (MSI-H)[8].Beyond Lynch syndrome screening, MSI-H has clear clinical significance for prognostic assessment and prediction drug efficacy, e.g., programmed cell death ligand 1 antibody is effective in the treatment of advanced dMMR or MSI-H tumors.Clinically, immunochemistry (IHC)staining is a primary screening method for patients with dMMR/MSI cancer[8].However, acknowledging limitations to IHC[9,10], recent guidelines suggest a combined approach.For metastatic cancer, it is suggested to perform both ICH and molecular tests, such as PCR with capillary electrophoresis, to direct therapy.In non-metastatic cancer cases, in the presence of equivocal IHC results, it is recommended to subsequently perform molecular testing[10].
However, despite the implementation of CRC screening programs in various countries and the improvement of target therapeutics, the screening participation rate remains disappointingly low, posing a constraint on their effectiveness[11,12].
Colorectal cancer screening in Italy and the Emilia-Romagna region
In Italy, in accordance with national law[13], the essential levels of assistance have included organized CRC screening for both males and females aged 50-69 since 2006, with no cost to the individuals being screened.According to the most recently available data, the national participation rate in the organized screening for the biennium 2021-2022 was 36.8%.When accounting for opportunistic screening as well, the overall screening coverage reached 44.9%[14].The administration of Italian screening programs is a collaborative effort between regions and Local Health Authorities (LHAs).Regions are responsible for planning,evaluating, and supervising the screening programs in their territories, while LHAs are responsible for practical implementation[15].The participation rate in the organized CRC screening programs varies significantly across the different Italian regions, ranging from 7.9% to 67.0% in South and North Italy,respectively[14].In the Emilia-Romagna region, a total of 11 screening programs are active, inviting male and female citizens of target age to undergo a biennial FIT (screening round).The positive effect of the FIT screening program on CRC incidence rates, in terms of decreasing the pathology, was recently reported by Bucchiet al.[16].The regional attendance screening in the biennium 2021-2022 was 62%, which is higher than the national average.For these programs, the screening pathway concerning first and second-level examinations overlaps.On the contrary, there is no consistency in the invitation strategy adopted in terms of the delivery of FIT kits, and this also applies to the collection of stool samples[12].The FIT kit may be delivered by mail, at General Practitioners’ offices or outpatient clinics, at pharmacies, or in other community facilities, and in some cases, with the support of volunteers[17].
The model of community pharmacy in Italy with a focus on the Emilia-Romagna region
In the past few years, the traditional model of community pharmacy (defined as a pharmacy situated not in a hospital, clinic, or online but within the community and accessible to all) has undergone changes[18,19].Citizens now have access to a variety of services beyond the traditional role of dispensing and supplying medicines, including those in health promotion and prevention settings[18-20].
In Italy, the involvement of local pharmacies in CRC screening activities varies, including agreements between pharmacies and screening programs that show significant differences in terms of formally regulated process phases, responsibilities assigned to pharmacists, and payment for pharmacy services including fees and timing (i.e., payment upon kit delivery, sample return, or sample arrival at the laboratory).At the national level, a unique model is lacking[21].As of 2019, the Emilia-Romagna region is actively working on the implementation and development of the “Pharmacy of Services” (Farmacia dei Servizi).In July 2023, a new memorandum of understanding between the region and pharmacy associations was signed.This document, aligned with the guidelines of the National Health Commission regarding the experimentation of new services, has a two-year duration and defines various areas of activity.These areas include cognitive services, front office services for the Electronic Health Record, telemedicine services, and the administration of severe acute respiratory syndrome coronavirus-2 and influenza vaccines.Furthermore, it reinforces the role of pharmacies as places to implement initiatives supporting prevention,health promotion, and territorial access to care.A communication campaign by the regional health service,to be carried out in the coming months, will explain the key innovations to citizens.
Colorectal cancer screening program at the Local Health Authority of Bologna in the Emilia-Romagna region
At the LHA of Bologna, the capital of the Emilia-Romagna region in Northern Italy, approximately 120,000 citizens are invited every year to undergo a biennial FIT as part of the screening program.The target population receives a letter from the Screening Center containing the invitation to participate in the I level screening test; appointment scheduling for follow-up examinations is also managed by the Screening Center.
In July 2020, a major intra-organizational intervention commenced for the three population-based oncological screening programs active at the LHA of Bologna (i.e., breast and cervical cancer in addition to colorectal cancer).The current organization resulted from this intervention.Briefly, the Screening Center of the LHA of Bologna currently consists of two different structures, i.e., the Assistance Unit Screening Center and the Governance Screening Program Unit, which work in strict collaboration.In particular, the Assistance Unit Screening is staffed by both healthcare and administrative personnel, coordinated by a Medical Assistant.The Governance Screening Program Unit consists of two physicians, a biologist and a statistician, all working under the direction of a physician who serves as the Director.These two structures have organizational tasks.In the same month, following one sentinel event and two near misses, a reorganization of the CRC screening pathway aiming to ensure the governability of the first level of screening was also launched.This organizational change provided for an extension of the involvement of local pharmacies, which were not only used as FIT kit delivery points but also as stool sample collection and sending points to the laboratory[22].
Among the 257 pharmacies in the territory of the LHA of Bologna, almost all (n= 234) adhere to the screening program, representing 91.1% of total pharmacies.This network of both private and public local pharmacies was planned with the aim of providing a widespread screening service to citizens; each pharmacy serves a mean number of 1,228 target citizens, ranging from 1,021 to 1,519 citizens per residence district [Figure 1].
COMMENTARY TOPIC
This commentary provides an insightful analysis of the integration between the Screening Center of the LHA of Bologna and community pharmacies.It also reports additional experiences of CRC screening programs based on the community pharmacy model.
DEFINITIONS, INDICATORS AND STATISTICAL ANALYSIS
The concept and terms of integration adopted here are those described by Urionagüenaet al.in a narrative review summarizing and analyzing different types of integration reported in the health literature[23].Briefly,in agreement with the authors, the integration model is composed of four components: breadth, enablers,intensity, and types of integration classified by the levels of health care system[23].The breadth of integration is represented by vertical and horizontal integration, requiring coordination with and without mechanisms of organizational hierarchy, respectively.Enablers act to facilitate integration, and intensity refers to the degree of integration.Finally, three levels classify types of integrations such as macro level (focusing on the highest level of a national health care system), meso level (focusing on organizational aspects at a regional level), and micro level (focusing on individual experiences that take place in and around clinical encounters)[23].
To evaluate the impact of integrating community pharmacies into the Bologna LHA’s CRC screening program, the “participation rate in the first-level screening test” indicator was considered.The “invitation rate in the first-level screening test” indicator was also taken into account.These indicators were calculated according to the Emilia-Romagna region survey form (Rilevazione Puntuale), which considers the screening round.
Univariate analysis was performed using Chi-squared test for all categorical variables, and Student’st-test for independent samples to compare all continuous variables.Tests were considered significant forP-values < 0.05.The statistical analysis was performed using Stata (Version 18).
DESCRIPTION OF THE INTEGRATION OF THE COMMUNITY PHARMACIES IN THE COLORECTAL CANCER SCREENING PROGRAM OF THE LOCAL HEALTH AUTHORITY OF BOLOGNA
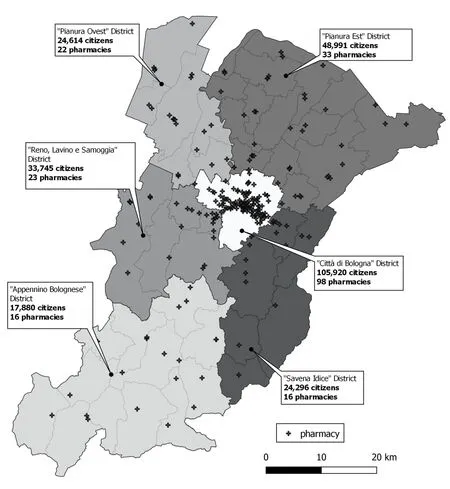
Figure 1.Distribution and number of the local pharmacies participating in the colorectal screening program for each district of residence within the jurisdiction of the Local Health Authority of Bologna, along with the size of target population per residence district.
In our setting, a horizontal integration at the micro level with service and clinical integrations supported by meso-level policy (regional authority) was applied.Four types of integration, such as normative,informational, financial, and functional, serving as enablers were implemented.Finally, aiming to achieve a high degree of intensity of integration, a high level of depth of consensus, connectivity, communication, and trust[23]was pursued.Indeed, subsequent to the design phase conducted at the Screening Center and validation by the LHA’s Healthcare Management, several meetings were held with the four associations representing the pharmacies to present the project proposal.All planned actions underwent collective discussions and their implementation required mandatory consensus between the pharmacies’ associations and the LHA.Strategies to be adopted, including the use of a unique and createdad hocinformation system to manage the screening process, were all shared and mutually agreed upon by both parties with continuous bidirectional communication.The integration was governed by a contractual agreement (referred to as the“Accordo tra Azienda USL di Bologna_Associazioni Farmacie”, dated July 08th, 2020; renewed in 2021 with a validity of 3 years) established among the LHA of Bologna and the pharmacies’ associations (normative integration); the document has set responsibilities and goals.The process phases regulated by the latest agreement were: (i) kit procurement; (ii) provision of tertiary thermal containers; (iii) warehouse management; (iv) data processing consent collection (although it is not required for screening activities [EU Regulation 2016/679, Article 9 GDPR - “Trattamento di categorie particolari di dati personali”], the LHA must appoint pharmacists as data processing controllers); (v) kit delivery; (vi) sample returning; (vii) sample storage in pharmacy (with specified timing and temperature); (viii) sample transportation and storage in pharmacy distributors’ warehouses (with specified timing and temperature); (ix) sending the sample to the laboratory; and (x) sample tracking.The kit orders are managed by the central pharmacy of the Bologna LHA.This structure is part of the Pharmaceutical Department that ensures the fulfillment of the governance functions of the hospital and territorial pharmaceutical care process.Storage and supply of materials to pharmacy distributors, based on pharmacy needs, are handled by a private company partnered with the LHA.The process phases, from kit delivery to sending the sample to the laboratory, are handled by pharmacies and continuously monitored by the Screening Center using the specific informatics tool allowing for tracking the entire process until the visualization of test results (informational integration); any non-conformities are managed by the Screening Center’s health personnel.A remuneration for pharmacy services (i.e., 3.66 Euros/sample VAT included) was agreed upon (financial integration).As per the contractual agreement, payment is expected only for the stool return phase, and a monetary bonus linked to the achievement of specific screening attendance rates was included.An additional acknowledgment of 0.20 Euros/sample and 0.50 Euros/sample fees for screening attendance rates > 65% and > 80%, respectively,were defined.Likewise, a deduction of 0.20 Euros/sample from the base rate has been stipulated in the event of a decrease in screening attendance rate < 50%.Additional activities to be carried out by pharmacists are outlined in the contractual agreement, including informing citizens about the correct timing and method of stool storing, detailing how FIT results will be communicated, and explaining the necessity of specific further investigations in the event of a positive FIT result.Lastly, pharmacists are also tasked with promoting participation among citizens in the target age range for the CRC screening program, advising them on the significance of undergoing FIT.The display and distribution of information material created by the region can aid in this action (functional integration).
EFFECT OF THE INTEGRATION OF THE COMMUNITY PHARMACIES IN THE COLORECTAL CANCER SCREENING PROGRAM OF THE LOCAL HEALTH AUTHORITY OF BOLOGNA
The integration, as expected, overcame fragmentation, improved quality, and strengthened services[23].Indeed, the involvement of local pharmacies allowed the introduction of complete traceability of kits and specimens flow, as well as temperature control.Furthermore, comparing 2022 with 2019 (the base year under the previous organizational model), an increase in screening attendance rate of 4.6% was observed(i.e., 61.6%vs.57%, respectively;P< 0.001)[22].Moreover, in 2021, a notably high level of screening completion was observed, i.e., 93.7% of stool samples were returned to pharmacies; this value increased by 3.3% in 2022, reaching 97%.Of note, the invitation coverage of the target population in the first-level screening test in 2022, as compared to 2019, overlapped; it stood at 98.7% (236,860 invited subjects) in 2022vs.99.6% (255,253 invited subjects) in 2019.The data also showed overlaps in demographic characteristics, district of residence, and screening attendance history of the invited citizens.Specifically,when comparing 2022 to 2019, the proportion of females among the invited population was 51.9%vs.51.8%,with a mean age of 58.1vs.58.4 years, respectively, and the majority (i.e., 40.0%vs.39.2%) resided in Bologna Città District.Finally, in both years, they were mainly historically never attenders/intermittent attenders to the Bologna LHA’s CRC screening program (i.e., 46.4% in 2022vs.46.9% in 2021).
The correct timing of the sample's arrival at the laboratory (i.e., < 14 days between sampling and processing)is informatically overseen by the Screening Center.If this timeline is not adhered to, the citizen is contacted by health personnel to repeat the FIT.In particular, during the period from 2021 to 2022, this occurred in 0.57% (range, 0.25%-1.54%) of cases.A continuous interface between pharmacists and Screening Center healthcare staff occurs to prevent the recurrence of the same errors; during the initial implementation period, closer monitoring and communication were necessary.A total of 34,998 errors, underlying nonconformities in no more than 17% of cases, were observed.In particular, the majority of these were represented by manual mistyping of data such as citizens' fiscal code or kit barcode during data entry(49.5%;n= 17,364) (notably, the information system allows all actions to be carried out automatically),followed by lack of data entry (32.9%;n= 11,513), lack of informatics recording of kit delivery/sample collection phases (14.6%;n= 5,088), and barcode mismatches between the kit assigned at delivery and the one detected at collection (3.0%;n= 1,033).Considering 2021 and 2022, a mean number of 68,295 kits were annually delivered by the pharmacies (min-max values per pharmacy, 12-840).It has been observed that pharmacies handling a lower number of kits and samples (< 410 actions/year) make more errors compared to those with a higher workload (> 626 actions/year), with an average of 19.7 errors per 100 actionsvs.12.6 errors per 100 actions, respectively (P= 0.019).These data suggest that periodic update training should be provided to pharmacies with lower screening activity levels to ensure the same quality level of the screening pathway to the entire target population.
As part of the functional integration, in 2022, pharmacists were tasked with performing active phone call reminders to approximately 2,000 citizens who picked up FIT kit without returning the sample for at least 5 months.The list of citizens, along with their telephone numbers, was provided by the Screening Center staff to the respective pharmacies where the kits were delivered.The attendance rate among these citizens was 29.3%, supporting that active phone calls are an effective method to improve CRC screening uptake[24]and also indicating a good level of confidence in the pharmacy profession and receptivity to healthcare advice[19,25].Furthermore, our data on kit delivery and sample return provide insights into citizen fidelity to the pharmacist.Despite the option for citizens to obtain the kit and return the sample at different pharmacies for convenience, in the first semester of 2023, 91.3% of citizens chose a single pharmacy for screening, consistent with 90.8% in 2022.
THE MODEL OF COMMUNITY PHARMACY IN COLORECTAL CANCER SCREENING ACTIVITY IN EUROPE
In Europe, where the approach is to implement population-based cancer screening programs[26], mention should be made of two groups of Spanish authors who have reported their experience involving community pharmacies in screening activity.Specifically, the Colorectal Cancer Early Screening Program of Barcelona was implemented in 2009 and involved community pharmacies in the distribution and collection of screening kits and samples[27].In the study evaluating the main indicators of the first round (2010-2011) of the program, Burónet al.found a 43.6% attendance rate, considering it satisfactory, and suggested that the positive acceptance could, to some extent, also be attributed to the role of pharmacies in terms of availability(high number of hours) and accessibility (very high in the cities)[27].Similarly, in a study analyzing the data on FIT kit distribution and collection in the Metropolitan area of Barcelona during 2017-2018, Viveset al.reported extensive community pharmacies’ involvement (i.e., 82.4%) in the program and a high level of quality in the distribution and collection process (i.e., among citizens who picked up a FIT kit, the compliance with screening completion was 93.5%)[26].For a widespread and successful involvement of community pharmacies, the authors highlight the importance of specific organizational choices similar to those adopted by our Center, such as the central coordination of pharmacies by the Official College of Pharmacists, the availability of a dedicated training program, and compensation for pharmacies’ service.They also pointed out the importance for citizens to receive accurate and adequate instructions from pharmacists[26].Finally, in the UK, the role of community pharmacies in supporting the local population with advice and information on CRC screening is promoted[28].In particular, in 2016, Public Health England established the quality criteria for community pharmacies to be recognized as “Health Living Pharmacy”,with a further definition in the National Institute for Health and Care Excellence guideline “Community pharmacies: promoting health and wellbeing”, published in 2018[29].
CONCLUSION
Despite the different organizational structures of population-based CRC screening programs worldwide,which make it challenging to generalize single experiences, the involvement of community pharmacies appears promising in terms of improving both the quality of services offered and screening attendance.In the near future, understanding the opinions and satisfaction of both professionals and citizens involved in our screening program, through the administration ofad hocsurveys, can allow us to identify eventual vulnerabilities in the pathway and then design and plan improvement interventions.Efforts should be directed towards developing pharmacies as centers for promoting cancer screening awareness, aiding citizens in taking a proactive approach to managing their health.
DECLARATIONS
Acknowledgments
The authors would like to thank the four associations representing the local pharmacies in the territory of the Local Health Authority of Bologna, as well as all the pharmacists who participate in the colorectal cancer screening program, for their collaboration.Additionally, the authors extend their thanks to all the members of the Screening Centre’s staff for their work.
Authors’ Contributions
Interpreted data, drafted the work, and performed its review and editing: Chiereghin A
Acquired, analyzed, and interpreted data: Pizzi L
Contributed to data acquisition and wrote the original draft: Squillace L, Sanna T
Conceived and designed the work, as well as contributing to the critical revision of the manuscript:Bazzani C
Validated the work and contributed to the critical revision of the manuscript: Roti L
Conceived, designed, and supervised the work, as well as contributing to the critical revision of the manuscript: Mezzetti F
All authors have approved the final version of the manuscript.
Availability of Data and Materials
Not applicable.
Financial Support and Sponsorship
None.
Conflict of interest
All authors declared that there are no conflicts of interest.
Ethical Approval and Consent to Participate
Institutional approval was not required for the publication of the organizational model of colorectal cancer screening.The assessments reported here regarding the screening participation of the target population are part of the institutional commitments of the Local Health Authority of Bologna.When citizens are invited to participate in colorectal cancer screening, they are informed that their personal data may be used for various purposes, including administrative, managerial, and financial fulfillment related to the institutional tasks of the LHA.This usage extends to purposes of significant public interest, such as planning,management, monitoring, and evaluation of health care, as well as for epidemiological and statistical activities.The complete text of the “Privacy Policy” document for citizens is available on the Bologna Local Health Authority website at www.ausl.bologna.it.
Consent for Publication
Not applicable.
Copyright
? The Author(s) 2024.
 Journal of Cancer Metastasis and Treatment2024年2期
Journal of Cancer Metastasis and Treatment2024年2期
- Journal of Cancer Metastasis and Treatment的其它文章
- Editorial on “Chinese expert consensus on the clinical practice of non-small cell lung cancer fusion gene detection based on RNA-based NGS” (2023 edition)
- Consideration of liquid biomarkers for surveillance of HPV-related oropharyngeal cancer in veteran populations
- Cancer-associated fibroblasts (CAFs) based model reveals potential for predicting bladder cancer patients’ prognoses and immunotherapy responses