
Progression of liver disease and associated risk of hepatocellular carcinoma
2024-05-13 07:41:42EdoardoPoliEleonoraDeMartin
Hepatoma Research 2024年3期
Edoardo Poli, Eleonora De Martin
1AP-HP, H?pital Paul-Brousse, Centre Hépato- Biliaire, FHU Hepatinov, INSERM Unit 1193, Villejuif 91400, France.
2Department of internal Medicine, Division of Gastroenterology and hepatology, Groupe Hospitalier Nord Essonne, Longjumeau 91160, France.
Abstract Hepatocellular carcinoma (HCC) is the primary liver cancer type, often seen in individuals with chronic liver disease.Once the patient progresses to the cirrhotic stage, the annual incidence of HCC is approximately 2%-4%.As it exceeds the minimum threshold of 1.0%-1.5% per year, HCC screening every 6 months through abdominal ultrasound is indicated in the cirrhotic population.While the incidence of viral hepatitis-associated HCC is decreasing, there is a notable rise of HCC associated with metabolic dysfunction-related steatotic liver disease and alcohol-related liver disease, particularly in high-income countries.The most effective approach for oncological prevention remains addressing the cause of liver disease.The indications for HCC screening in patients without cirrhosis depend on the etiology of liver disease and the stage of fibrosis, assessed by liver biopsy or noninvasive tests such as FIB-4 or transient elastography.However, clear recommendations for HCC screening in patients without cirrhosis and for the different etiologies are currently unavailable.Research efforts should focus on identifying markers, or combinations thereof, to provide a more accurate estimate of HCC occurrence.Such advancements would enable the effective targeting of populations at the highest risk of HCC and the establishment of the correct timing to start the screening.
Keywords: HCC, chronic liver disease, cirrhosis, HCC screening
INTRODUCTION
Liver cancer is the second most prevalent cause of cancer-related deaths globally.According to the latest report from the World Health Organization published in 2020, liver cancer accounts for 4.7% of all cancers.It is estimated that about 1.3 million people will die from liver cancer by the year 2040[1].Hepatocellular carcinoma (HCC) is the most common type of hepatic cancer and it represents the first indication for liver transplantation in cirrhotic patients[2].Its incidence is 2 to 3 times higher in men than in women,particularly in certain European countries.In addition to the different distribution of modifiable risk factors such as alcohol consumption among genders, a range of non-modifiable risk factors for HCC associated with individual genetic predispositions and variances between male and female sexes has been documented[3].Hepatocarcinogenesis is a multistep process involving the transformation of hepatocytes,which undergo malignant genomic and epigenomic changes.It is characterized by high clinical and molecular heterogeneity[4,5].Although the exact molecular mechanisms triggering the onset and progression of HCC are far from being completely elucidated, the number of mutated genes and dysregulated signaling pathways associated with HCC are going to be progressively revealed, offering novel prospects for treatment[6,7].Within this context, the fibrogenic process appears not to be the primary trigger; instead,chronic non-resolving inflammation seems to play a pivotal role, by chronically producing cytokines such as IL-6, growth factors, chemokines, and proangiogenic factors.The onset of this environment favoring immune escape has been shown to be critical for the transformation of hepatic progenitor cells into a cancerous phenotype, alongside promoting the activation of anti-apoptotic pathway and inhibiting immune surveillance[8,9].
Once the patient progresses to cirrhosis, the annual incidence of HCC is about 2%-4%[10-13].Consequently,screening is recommended in the cirrhotic population as it is exceeding the minimum threshold of 1.0%-1.5% per year[14,15].
The worldwide disparity in HCC incidence is due to variations in the prevalence of viral hepatitis, which is more prevalent in low-income countries, and environmental factors, predominant in high-income countries.The underlying etiology of liver disease often represents an independent risk factor for HCC occurrence, posing a significant oncologic risk also in the early stages of liver disease[12,13].Indeed, different etiologies of liver disease bring with them a different degree and pattern of chronic inflammation, which may or may not increase HCC risk even in pre-cirrhotic stages of compensated advanced chronic liver disease.Consequently, identifying the risk of developing HCC for each patient group is crucial for defining the appropriate screening and follow-up strategies.
As reported by the Global Burden of Disease study in 2019, hepatitis B virus (HBV) accounted for 41.0% of HCC cases, hepatitis C virus (HCV) for 28.5%, alcohol-related liver disease (ALD) for 18.4%, metabolic dysfunction-associated steatotic liver disease (MASLD) for 6.8%, and other etiologies for 5.3%[13].
Early diagnosis of HCC poses a significant challenge, and the availability of noninvasive biomarkers is crucial.Currently, serum alpha-fetoprotein (AFP) serves as the primary serum biomarker for HCC, yet AFP-based diagnostic approaches remain less than satisfactory.While serum AFP alone lacks satisfactory sensitivity and specificity to serve as a standalone screening test, its combination with abdominal ultrasound significantly enhances sensitivity in detecting early-stage HCC (within the Milan criteria)[16].Several biomarkers have been identified and retrospectively studied as diagnostic tools, but few have undergone external validation and biomarkers validated across different populations are yet to be identified and included in HCC clinical guidelines[17].The challenge in finding appropriate biomarkers may also be attributed to the different etiologies of underlying cirrhosis.Nonetheless, with proper validation, the shift from using ultrasound-based methods to a biomarker-based screening approach for HCC appears viable in the near future, offering the potential for a substantial decrease in the incidence of HCC among high-risk populations[18].The introduction of biomarker-based screening will facilitate the implementation of screening programs in low-income countries, where, at the moment, the majority of HCC cases are diagnosed at an advanced stage[12].
HCC RISK ACCORDING TO LIVER DISEASE ETIOLOGY
HCC and HBV +/- HDV infection
HBV infection remains the main risk factor for HCC worldwide, particularly in Asian countries, where more than half of the global HCC population resides[11,13,19].HBV may increase the risk of HCC by 5-100 fold[12].In endemic areas, HBV is etiologically implicated in up to 80% of all HCC cases, while in Western countries, it accounts for about 20% of HCC cases[19].
Beyond its role in causing cirrhosis, HBV itself plays a critical role in the development of HCC, initiating the activation of oncogenic pathways by integrating into host DNA[20-22].As a matter of fact, chronic HBV non-cirrhotic carriers can develop liver cancer and the incidence of HCC in these patients is reported to be around 0.2/100 person-years[12,19].In patients with chronic hepatitis B without cirrhosis, the most significant factor associated with HCC occurrence is HBV viral load: patients receiving NUCs with incomplete suppression, even with low levels of viremia, showed a higher risk of HCC compared to patients with undetectable HBV-DNA[23,24].When cirrhosis occurs, independently from viral load, the incidence of HCC rises to 3.7 per 100 person-years, signifying a 31-fold increased risk of HCC and 44-fold increased mortality[11,12].
In the context of HBV-HDV co-infection, a significant increase in the global risk of HCC development is reported compared to HBV mono-infection.The cumulative incidence of HCC was 2.3%, 5.4%, and 7.5% at 1, 3, and 5 years, respectively, in non-cirrhotic patients, rising to 5.4%, 15.9%, and 23.1% at 1, 3, and 5 years,respectively, in cirrhotic patients[25].Major risk factors are liver cirrhosis, high HDV-RNA serum level, age >50 years, male gender, obesity, and lower platelet count.
Moreover, a significant six-fold increase in the risk of HCC was observed in patients with triple infection of HIV, HBV, and HDV, compared to those with HIV/HBV co-infection[26].
Several noninvasive HCC risk scores have been published worldwide in HBV patients with or without antiviral treatment[27].Even with their high negative predictive values for HCC occurrence spanning a 3- to 10-year period, there is no universally appliable score.
Paiket al.evaluated the effectiveness of two noninvasive serum biomarkers, the aspartate aminotransferase to platelet ratio index (APRI, threshold of 0.5), and the Fibrosis 4 score (FIB-4, threshold of 1.45), in stratifying the risk of HCC among chronic HBV-infected patients (both cirrhotic and non-cirrhotic) with low-level viremia (HBV DNA < 2,000 IU/mL).The authors showed that in the entire cohort, the 5-year cumulative incidence rates of HCC were 13.9%, 1.4%, and 1.2% for those with both high, any high, and both low, respectively.Among non-cirrhotic patients (n= 867,P< 0.001), the rates were 11.4%, 1.5%, and 0.4%,respectively[28].Additionally, the PAGE-B and modified-PAGE-B models[29,30]have been validated for predicting HCC risk in HBV patients undergoing NUC treatment.
Thus, in patients with chronic HBV infection, the two main risk factors for HCC occurrence are the stage of liver disease and viral load.Besides initiating early HCC screening and antiviral treatment in patients that are already infected, immunization against HBV should always be checked as it is the best prevention strategy.In Taiwan, 30 years after the beginning of universal newborn vaccination, HBV carrier rates have dropped from 10%-17% to 0.7%-1.7%, resulting in an 80% reduction in HCC rates[31].
HCC and HCV infection
Historically, the majority of HCC cases in high-income countries were associated with chronic HCV infection.However, this trend has recently shown a decline due to the advent of new direct antiviral agents(DAA).The risk of HCC occurrence in patients with HCV-related cirrhosis is approximately 2%-6% per year, almost 17-fold higher compared to other cirrhotic patients with compensated disease[19].Typically,HCC development occurs after two or more decades of HCV infection, and the increased risk has traditionally been limited to patients with cirrhosis.Notably, the incidence of HCC in the USA has tripled over the last four decades, likely due to the aging chronic hepatitis C patient pool, alongside a significant increase in MASLD, and the implementation of more accurate screening programs using ultrasounds in cirrhotic patients[32].
In the context of HCV-related cirrhosis, the FIB-4 score has a better prognostic performance for HCC occurrence prediction than APRI.Values > 2.18 were able to predict the occurrence of HCC with high sensitivity and specificity (92.4% and 87.2%, respectively)[33].Degasperiet al.described a significantly increased 3-year risk of HCC in cirrhotic patients with LSM values > 30 kPa or with FIB-4 > 9 at baseline[34].A multicenter French study developed an HCC score [taking into account age > 50 years, past excessive alcohol intake, low platelets count, high gammaGT levels, and absence of sustained virological response(SVR)], which can accurately predict the 1-, 3- and 5-year HCC occurrence[35].The presence of clinically significant portal hypertension, defined as the presence of esophageal varices and/or ascites, was also found to be an independent predictor of HCC occurrence in several studies involving HCV cirrhotic patients treated with DAA[36,37].
Therefore, the prevention of liver disease progression seems to be the most important factor affecting HCC risk in HCV patients.The early achievement of a SVR in HCV-infected patients has led to a substantial decrease in the risk of HCC worldwide, esteemed to be around 50% to 80%[38,39].However, Eradicating HCV reduces, though does not completely eliminate, the risk of HCC in patients with confirmed cirrhosis,necessitating lifelong monitoring[40,41].
Interestingly, it has been demonstrated that machine learning algorithms can enhance HCC risk prediction in HCV patients, and possibly in individuals with other causes of liver disease[42].
HCC and MASLD
The MASLD, now replacing the term non-alcoholic fatty liver disease/steatohepatitis according to the new nomenclature, is rapidly emerging as the most common etiology of chronic liver disease worldwide[12,43]and is the fastest-rising cause of HCC.As the occurrence of HBV-related HCC is expected to decrease thanks to vaccination coverage and viral suppression with antiviral treatments, and HCV-related HCC diminishes with the advent of DAA, the absolute prevalence increase in MASLD is becoming even more significant when assessed in terms of percentages and is destinated to become the most common etiology of liver disease underlying HCC in numerous countries[44].In Western countries, MASLD-related HCC has increased by up to threefold in the last decades[15].The stage of fibrosis is identified as one of the strongest liver-related predictors of overall survival and HCC development in MASLD patients[45].
Nevertheless, around 25% of HCC cases associated with MASLD happen without cirrhosis, showing a 2.61 times higher HCC incidence in non-cirrhotic MASLD livers compared to patients with chronic liver diseases from different causes[46].
According to the latest EASL guidelines, HCC surveillance is recommended in patients with MASLD cirrhosis; surveillance is suggested to be considered also in patients with F3 fibrosis (either histologically or via elastography)[47].In cohort studies including MASLD patients without cirrhosis, the incidence of HCC ranges from 0.08/1,000 patient-years to a maximum of 0.62/1,000 patient-years, with a recent meta-analysis reporting an incidence of HCC in non-cirrhotic livers of 0.3/1,000 patient-years[48].These rates are significantly higher compared to the incidence of HCC in chronic liver diseases from other etiologies in the absence of cirrhosis[46,49].In the context of MASLD-related cirrhosis, the incidence of HCC ranges from 2 to 26/1,000 person-years, depending on cohort characteristics[48,50,51].
Concerning the role of noninvasive tests of fibrosis, Kanwalet al.suggested that a FIB-4 score > 3.25 can predict an HCC risk > 1%, thereby recommending HCC surveillance in these patients[50].
HCC and alcohol-related liver disease
The established causal relationship between alcohol intake and HCC occurrence is well-documented[15,52].A recent meta-analysis reported a cumulative risk of HCC at 5 and 10 years in alcohol-related cirrhosis of 3%and 9%, respectively[53].Indeed, in addition to the duration of chronic alcohol consumption, a metanalysis estimated a 16% increase in the risk of HCC among those patients consuming 3 or more alcoholic units/day and a 22% increased risk among those consuming > 6 units/day[54], compared to non-drinking patients.Moreover, alcohol can act synergistically with other liver disease etiologies, exacerbating the progression of liver disease and further elevating the risk for HCC occurrence[55,56].
Regarding the role of noninvasive tests, the cumulative incidence rate of HCC at 3 years was 4.1% in patients with a modified FIB-4 index > 4 and 0.7% in patients with an index < 4.This suggests the need for HCC screening in the former group[57].In the context of ALD, total abstinence from alcoholic beverages stands as the only effective method to reduce HCC-risk occurrence.This recommendation should also be extended to patients with other underlying etiologies of liver disease, as in these patients, the role of alcohol in promoting liver disease progression and increasing oncologic risk tends to be underestimated.
HCC and rare liver diseases
In the context of autoimmune hepatitis (AIH), the occurrence of HCC has historically been considered a rare complication[58].However, a recent retrospective, observational, multicentric study revealed an incidence rate of HCC in patients with AIH of 1.44/1,000 patient-years.After cirrhosis develops, the cumulative incidence of HCC increases to 2.6%, 4.6%, 5.6%, and 6.6% at 5, 10, 15, and 20 years,respectively[59].Obesity, cirrhosis, and AIH/primary sclerosing cholangitis overlap syndrome were independent risk factors for HCC occurrence.These incidences meet the cut-off value of 1.5%, thereby recommending HCC screening as recommended and cost-effective.
Patients with primary biliary cholangitis (PBC) show an incidence of HCC of 2.4%.According to the latest Japanese data, HCC incidence is 5.1% in males and 2.0% in females[60].A recent multicenter international study in Europe reported an HCC incidence of 3.4/1,000 patient-years, with a similar increased incidence in men[61].This increased incidence of HCC in males was irrespective of histological stage, emphasizing the importance of HCC screening for males with PBC from an early stage of the disease.
The exact annual incidence of HCC in HFE-related hereditary hemochromatosis remains undefined, but it appears to be close to 1.5%.The majority of HCC occurs in cirrhotic livers with iron overload, but the occurrence of HCC in non-cirrhotic livers of patients with hemochromatosis has also been described.According to the latest EASL recommendations, HCC screening in patients with hemochromatosis should be proposed if, at the time of diagnosis, the fibrosis stage is at least F3 and should be continued even if iron depletion allows regression of liver fibrosis to a lower stage[62].
In Wilson’s disease, the chance of developing primary liver cancer is said to be low.A European study of 1,186 patients found that only 1.2% had liver cancer, with an incidence rate of 0.28 per 1,000 patient-years.Cirrhosis continues to be the main risk factor for liver cancer in these patients[58].
Table 1 summarizes the actual indications for 6-month interval ultra-sounds HCC screening according to liver disease etiology and stage of liver disease.
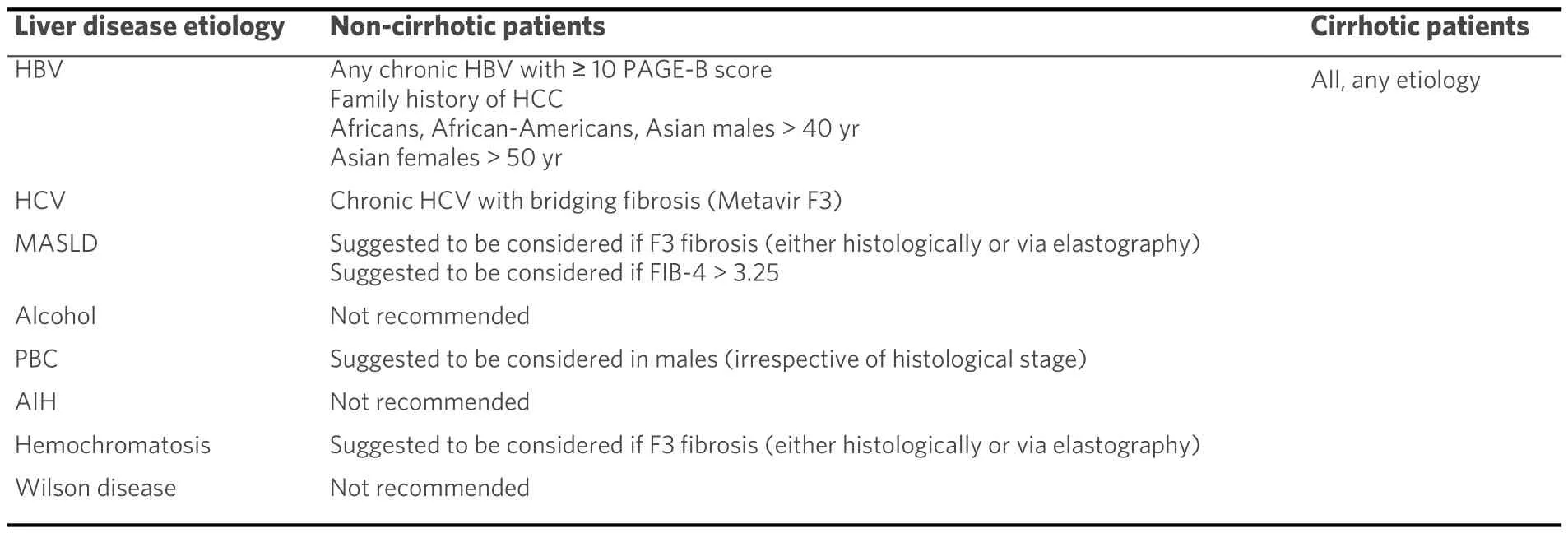
Table 1.Actual indications for 6-month interval ultra-sounds HCC screening according to liver disease etiology and stage of liver disease
CONCLUSION
In conclusion, the risk of HCC is primarily determined by the progression of liver disease, which is strongly influenced by the underlying etiological factor.A 6-month HCC surveillance by abdominal ultrasound and serum AFP is recommended for patients with cirrhosis of any etiology and some selected patients with chronic HBV infection.The etiological treatment of liver disease remains the most effective oncological prevention.Some etiologies demonstrate significant HCC incidence rates even in the non-cirrhotic population; nevertheless, the paucity of data does not allow the formulation of robust guidelines in this regard at present.
DECLARATIONS
Authors’ contributions
Draft manuscript preparation, review of the manuscript, and approval of the final version of the manuscript: Poli E
Review of the manuscript and approval of the final version of the manuscript: De Martin E
Availability of data and materials
Original data from the literature, elaborated by the authors.
Financial support and sponsorship
None.
Conflicts of interest
Both declared that there are no conflicts of interest.
Ethical approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Copyright
? The Author(s) 2024.

- Hepatoma Research的其它文章
- Introduction of Chinese expert consensus on neoadjuvant therapy for primary liver cancer (2023 edition)
- Introduction to 2023 Chinese expert consensus on the whole-course management of hepatocellular carcinoma
- Reflections and perspectives on adjuvant treatment in the setting of resected hepatocellular carcinoma
- Dysmetabolic comorbidities and non-alcoholic fatty liver disease: a stairway to metabolic dysfunctionassociated steatotic liver disease
- Role of temporary portosystemic surgical shunt during liver resection to prevent a post-resection small for size-like syndrome
- The role of percutaneous hepatic perfusion (PHP) in the treatment of cholangiocarcinoma