
Ductal carcinoma in situ within a fibroadenoma: A case report and review of literature
2024-05-09 03:05:58YazminOlivaresAntnezYesikaJanettvilaZablahJosRazquezvilaGabrielaSofmezMacasMarTeresaMirelesAguilarMargaritaLiliaGarzaMontemayor
World Journal of Radiology 2024年3期
Yazmin Olivares-Antúnez,Yesika Janett Dávila-Zablah,José Raúl Vázquez-ávila,Gabriela Sofía Gómez-Macías,María Teresa Mireles-Aguilar,Margarita Lilia Garza-Montemayor
Abstract BACKGROUND Fibroadenoma (FA) is the most common tumor found in young women,although it can occur in any age group.Ductal carcinoma in situ (DCIS) that is confined in a FA is rare;it is most frequently reported as an incidental finding.CASE SUMMARY We report a case of DCIS within a FA in a 46-year-old female without cancerrelated personal and family histories.The patient was diagnosed with a breast conglomerate of nodules and was followed for 1 year.In the current control image study,we found suspicious microcalcification,as a new finding,within one of the nodules.Consequently,a core biopsy of the tumor,which appeared hypoechoic,oval,and circumscribed,was performed.The pathological diagnosis was ductal carcinoma in situ within a fibroepithelial lesion.The patient underwent breastconserving surgery and received radiotherapy as well as endocrine therapy (tamoxifen).CONCLUSION We recommend a multidisciplinary approach for adequate treatment and followup.
Key Words: Carcinoma in situ;Fibroadenoma;Mammography;Ultrasound;Magnetic resonance imaging;Radiology;Case report
lNTRODUCTlON
Ductal carcinoma in situ (DCIS) arising within a fibroadenoma (FA) is rarely encountered,although pure FA is the most common tumor found.Its incidence ranges from 0.02% to 0.125%,and it is incidentally found.We present a case of breast DCIS arising within a FA and discuss the imaging findings.
CASE PRESENTATlON
Chief complaints
The 46-year-old female was diagnosed with a conglomerate of breast nodules which is stable for a period of 1 year.She came to our department for routine mammography and follow-up nodules by ultrasound (US).
History of present illness
She is asymptomatic.
Personal and family history
Family history: Cervical cancer (her mother was diagnosed at age 81 and her sister was diagnosed at age 50).Gastric cancer (her grandmother diagnosed at age 80).
Personal history: The patient had a history of augmentation mammoplasty.
Physical examination
Right breast without palpable mass.Right and left axillary lymph nodes clinically negative.
Imaging examinations
By mammography,the tissue breast is extremely dense (category “D” of the American College of Radiology,2013).In the right breast,a conglomerate of nodules with obscured margins is seen at the posterior third of the union of lower quadrants.In both axillary regions,no lymph nodes are shown (Figure 1).
Craniocaudal and Mediolateral Oblique projections with magnification of right breast reveal two confluence nodules,which are isodense,oval with obscured margins and microcalcifications associated.The findings are localized 2 cm from skin adjacent to the mastoplasty surgical scar indicated by the linear tissue marker (Figure 2).
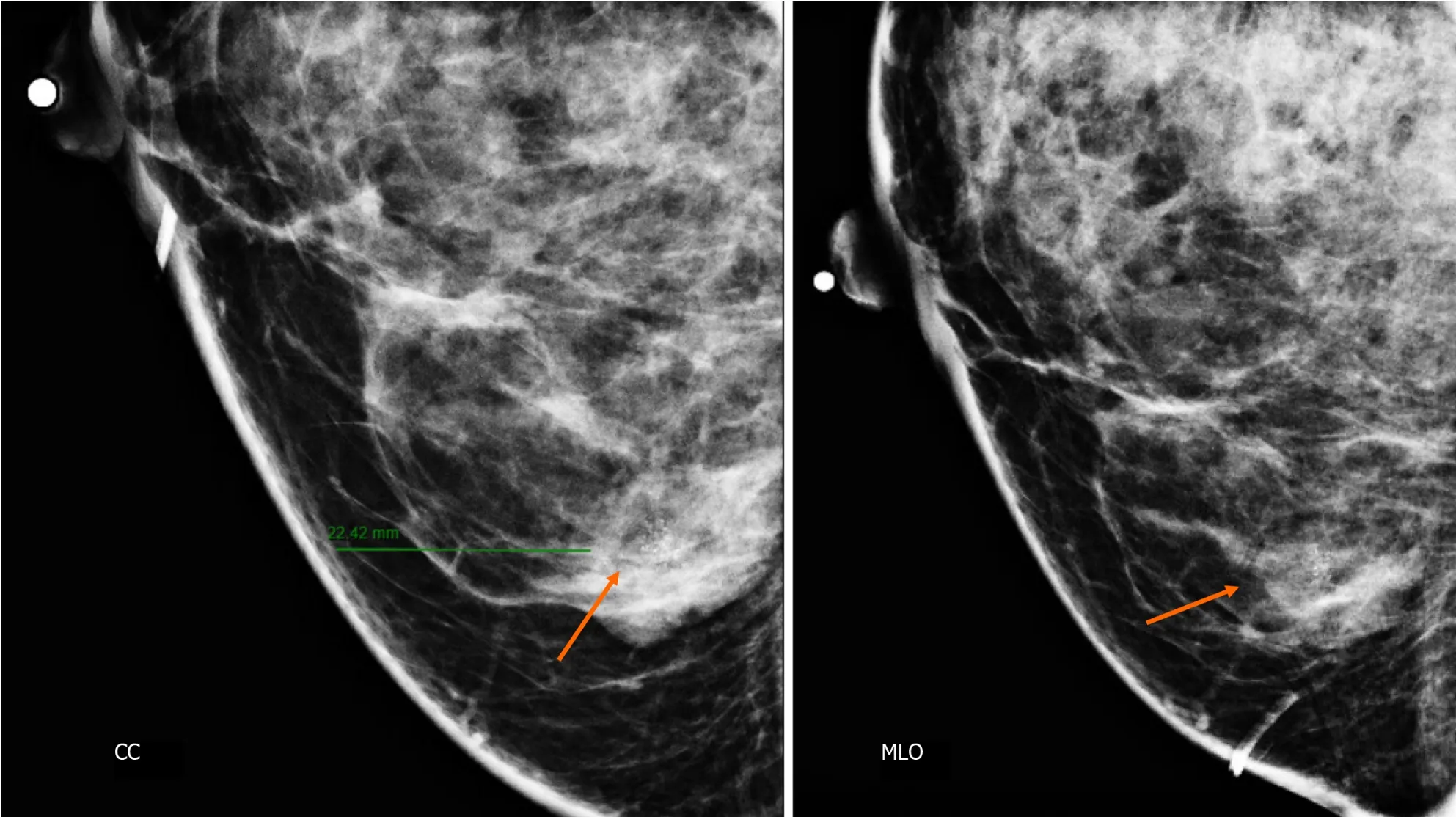
Figure 2 Craniocaudal and mediolateral oblique projections with magnification of right breast. The two confluence nodules are associated with suspicious microcalcifications (arrow).The findings are localized 2 cm from skin and are adjacent to mastoplasty surgical scar indicated by the linear tissue marker as it is seen in the mediolateral oblique projection.CC: Craniocaudal;MLO: Mediolateral oblique.
In addition,the magnification views in orthogonal projections reveal that one of the nodules is associated with fine and linear pleomorphic microcalcifications that extended in an area of 8 mm (Figure 3).
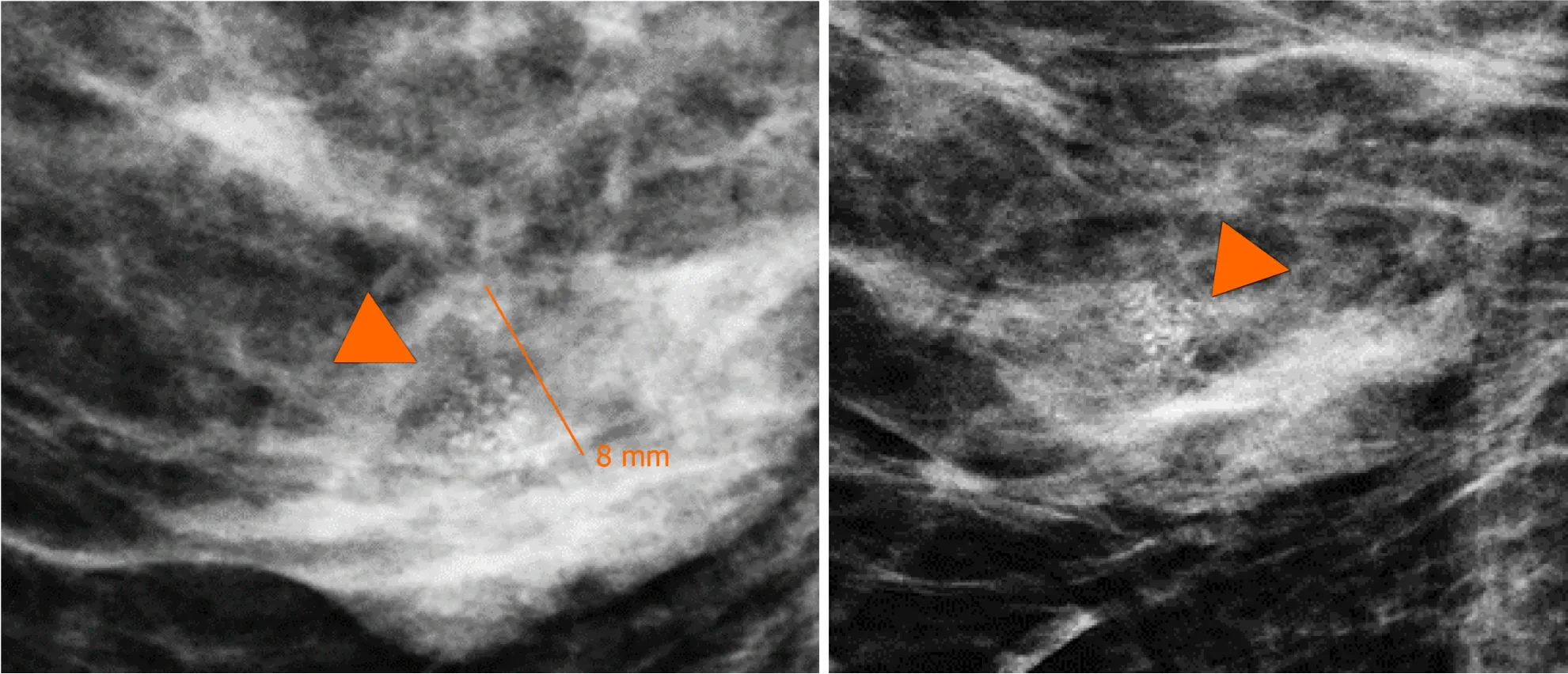
Figure 3 Magnification views in orthogonal projections. One of the nodules is associated with fine and linear pleomorphic microcalcifications (head arrow) that extended in an area of 8 mm.
By digital breast tomosynthesis,we corroborate the morphology of microcalcifications (Figure 4).
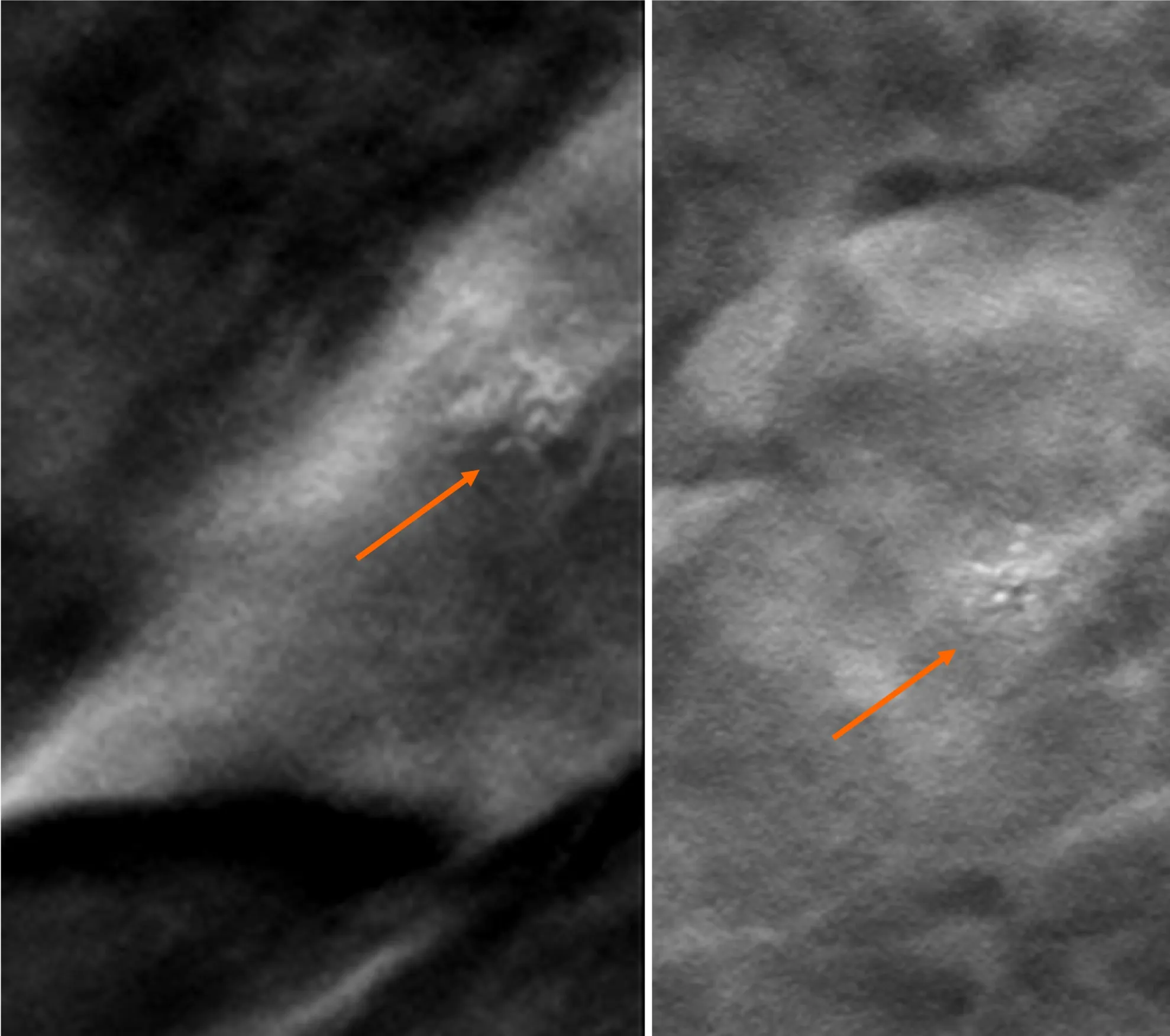
Figure 4 Digital breast tomosynthesis with magnification of craniocaudal and mediolateral oblique projections. The morphology of microcalcifications is corroborated as fine and linear pleomorphic appearance (arrow).
Subsequently,a bilateral breast US was performed.In the right breast is seen a conglomerate of two solid nodules that are hypoechoic,oval,circumscribed,avascular and non-palpable,located at the 6 o'clock position,4 cm from the nipple in the right breast (Figure 5).One of the nodules shows microcalcifications seen in mammography.The bilateral axillary region demonstrates lymph nodes with morphology and fat hilum conservation (Figure 6).These findings correspond to the category of breast imaging-reporting and data system (BI-RADS) 4B.
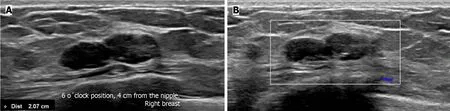
Figure 5 Gray-scale ultrasound and Doppler color images. A: In the right breast is seen a conglomerate of two solid nodules that are hypoechoic,oval,circumscribed and non-palpable with lateral acoustic shadowing,located at the 6 o'clock position,4 cm from the nipple in the right breast.In one of the nodules,internal hyperechoic foci are seen,corresponding to microcalcifications shown in mammography;B: The nodules have neither internal nor peripherical vascularity.
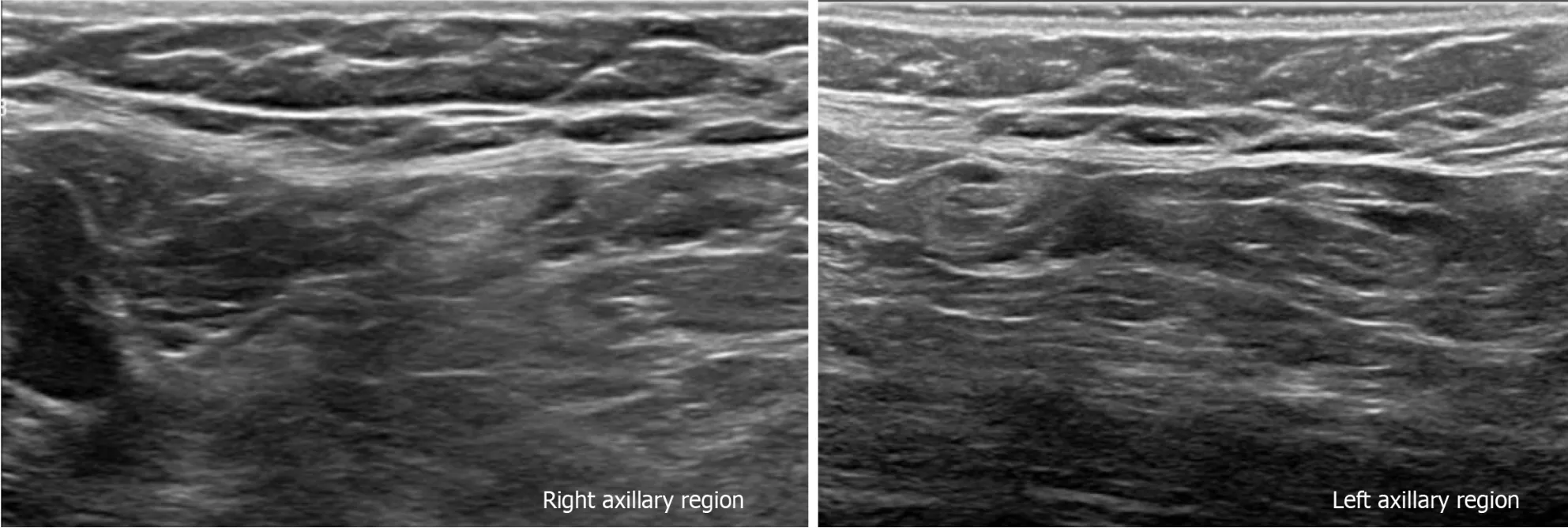
Figure 6 Gray-scale ultrasound images. The bilateral axillary region shows lymph nodes with conservative morphology and fat hilum,with cortex of < 3 mm.
An US-guided core biopsy was indicated.A percutaneous biopsy was performed of the conglomerate solid nodules,using a 12-gauze needle.Six cores were obtained and sent in formalin for pathology analysis.A tissue marker (or clip) is placed in one of the nodules which is associated with macrocalcifications.A projection of mammography is taken to confirm the position of the tissue marker (Figure 7).
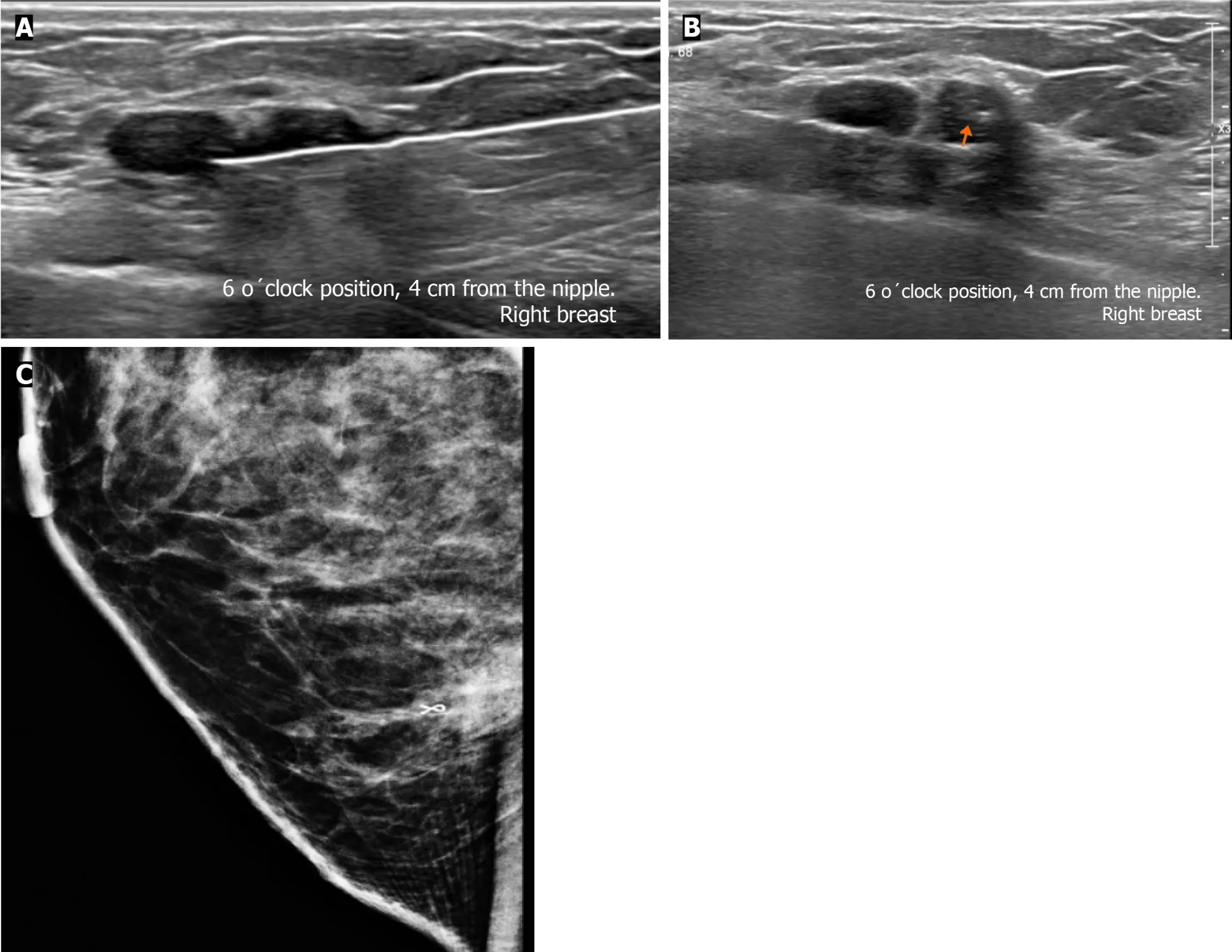
Figure 7 Ultrasound-guided core biopsy images. A: Percutaneous biopsy was performed of the conglomerate solid nodules,using a 12-gauze needle;B: A tissue marker or clip is placed in one of the nodules (arrow) which is associated with microcalcifications;C: Lateral projection of mammography.The tissue marker confirms the position of biopsied microcalcifications.
The histopathology report corresponds to 1.5 mm of high-nuclear grade DCIS with comedonecrosis and microcalcifications,which are within a fibroephitelial lesion that corresponds to a FA.Hematoxylin and eosin stain slides revealed pleomorphic neoplastic cells within a FA (Figure 8).
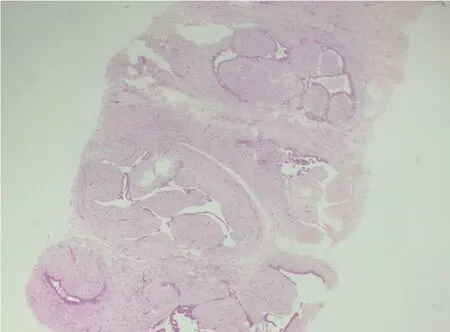
Figure 8 Hematoxylin and eosin stain slide. Pleomorphic neoplastic cells are seen within a fibroadenoma.
TREATMENT
The patient underwent surgery,involving guidewire localization of the non-palpable conglomerate of nodules done under US (Figure 9).The treatment consists of conserving surgery and no sentinel lymph node biopsy was needed.
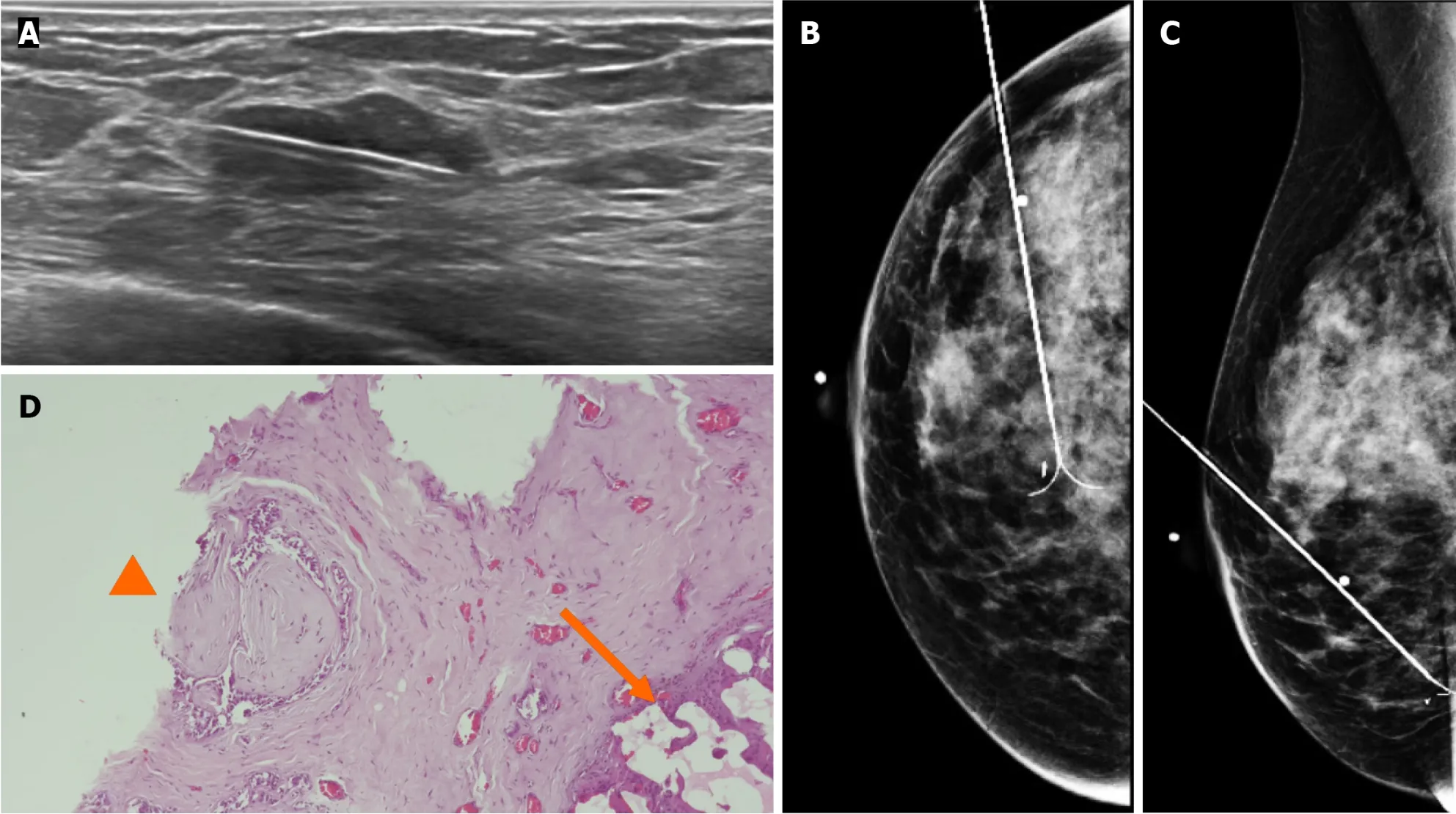
Figure 9 Gray-scale ultrasound images. A: Preoperative guidewire is inserted percutaneously into the breast to localize the non-palpable conglomerate of nodules done under ultrasound;B and C: Craniocaudal and mediolateral oblique projection.The adequate position of the hook wire is confirmed in the target lesion;D: Histological slide of partial mastectomy.The site of the previous biopsy is seen (arrow).Also,fibroadenoma is shown which contains pleomorphic neoplastic cells and nucleolus with pleomorphic appearance (head arrow) that corresponds to ductal carcinoma in situ.
FlNAL DlAGNOSlS
The pathological report corresponds to residual tumor of 0.5 mm foci which corresponds to a high-nuclear grade DCIS,comedo subtype,central necrosis and microcalcifications associated within a complex FA,that measures 2.5 cm.
Stage 0,cTisN0M0 within a FA,with the following immunochemistry markers: Estrogen receptor (+) 90% and progesterone receptor (+) 70% (Figure 10).

Figure 10 lmmunohistochemical staining. A: Immunohistochemical markers 5 ×,estrogen receptor+(90%) in ductal carcinoma in situ within fibroadenoma;B: Immunohistochemical markers 5 ×,progesterone receptor (+) 70% in ductal carcinoma in situ within fibroadenoma.
Other histological findings: Columnar cell changes and hyperplasia with microcalcifications and 2 peripheral papillomas,one measures 0.7 mm.
OUTCOME AND FOLLOW-UP
The patient subsequently received radiotherapy and endocrine therapy (tamoxifen).According to the final diagnosis the patient has a good prognosis.
DlSCUSSlON
FA is the most common benign fibroepithelial breast tumor in young women and can occur at any age,being most common between 20 years and 40 years of age[1-13].
FA is a biphasic tumor composed of stromal (connective) and epithelial tissue that grows by estrogen and progesterone stimulation and is commonly found in pregnancy and lactation.During menopause,FAs suffer atrophy[3,4,6,9,13].
FAs are divided into simple and complex types.FAs with 1 or more of the following characteristics are considered complex: Epithelial calcifications,apocrine metaplasia,sclerosing adenosis and/or cysts larger than 3 mm[1,4-7,9,11,12,14].
The risk of breast carcinoma in complex FAs is 3.10 times greater than in patients with pure FAs and is associated with the percentage of epithelial proliferation[1,3,5,13].
DCIS within a breast FA is uncommon,with an incidence of 0.02% to 0.125%.Fewer than 130 cases have been reported in the literature[1].
Cancer may arise from the surrounding breast tissue,in the fissures of the FA,or the carcinoma may be completely confined within the FA.The age at presentation of these patients is 42.5 to 46.9 years-old,approximately 20 years later than the maximum age at presentation of patients with pure FA[1,6,10,12].
There are no specific imaging characteristics to distinguish between a pure FA and DCIS within a FA.In most cases,DCIS presents as an incidental finding and is indistinguishable from benign lesions on imaging (Table 1)[1].
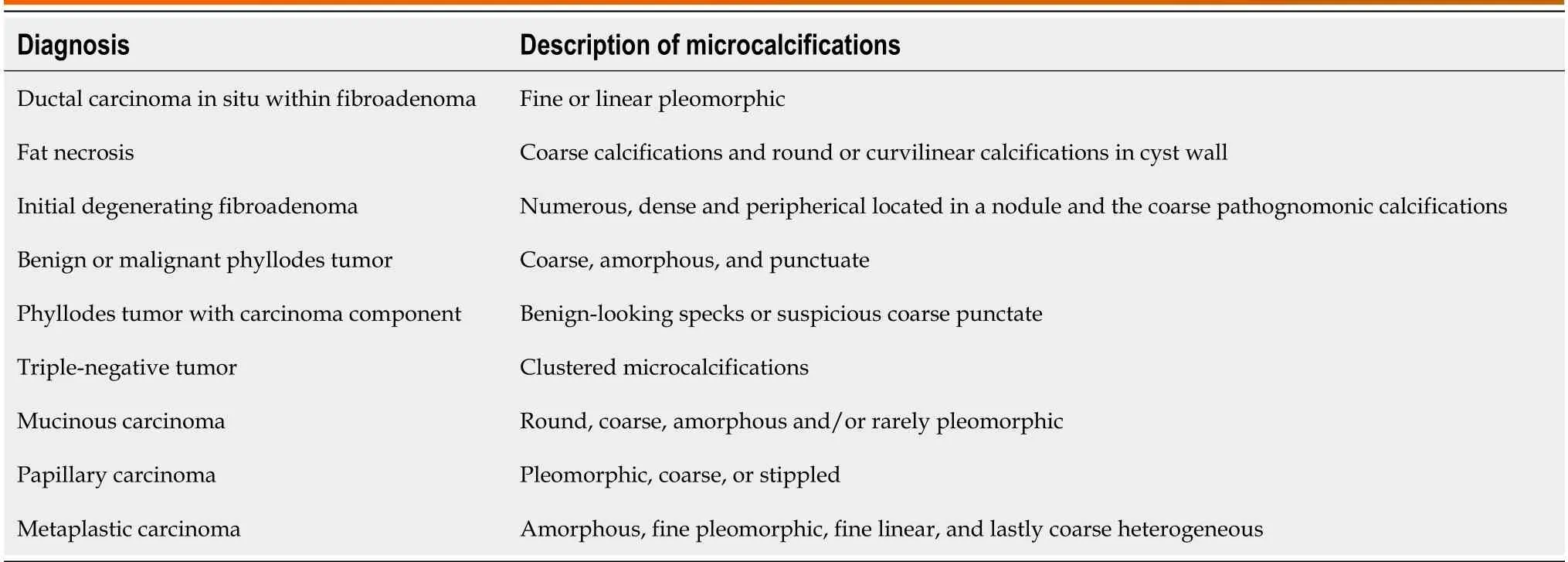
Table 1 Differential diagnosis microcalcifications within a nodule
The suspicious finding of carcinoma in a FA in mammography is a group of fine or linear pleomorphic microcalcifications within a nodule of indistinct margins[1-4,6,7,9,12,14].
By US,if the shape or margin of the nodule is irregular and has acoustic shadowing,an echogenic halo or distortion of the architecture should be considered suspicious for malignancy[1-4,6,7].
By magnetic resonance imaging (MRI),a typical FA is observed as an oval mass,with circumscribed margins and persistent contrast enhancement.A carcinoma should be suspected when there is contrast enhancement with a rapid uptake curve and washout late phase (type 3)[1,3,6,7].
In adult patients,the American Society of Breast Surgeons recommends against routinely excising biopsy-proven FA that are < 2 cm.The American College of Radiology Appropriateness Criteria for palpable breast masses even states that short term imaging follow-up (such as every 6 months for 2 years) is a reasonable alternative to biopsy for solid masses with probably benign features suggesting FA[15].
A core biopsy should be performed on a nodule that presents rapid growth.The criteria for rapid growth are: (1) Volume growth rate ≥ 16% per month for patients younger than 50 years;(2) volume growth ≥ 13% per month for patients ≥ 50 years;and (3) mean change in dimension over a 6-month interval of > 20,especially in patients over 40 years of age to exclude the possibility of phyllodes tumor or malignancy[15].
The indications for excision include size > 30 mm,considering that pre-operative biopsy is also insufficient to distinguish phyllodes tumor from FA,and there is the possibility of underestimation.Other indications for surgical removal are for growing FA,a nodule with increased BI-RADS classification grade during the follow-up and core needle biopsy suggesting atypical hyperplasia or unusual pathologic features.Persistent discomfort and pain from a FA are a relative indication to consider surgical excision.Another indication for surgical removal is patient′s request or cosmetic concerns[6,16-19].
The differential diagnoses to consider for a nodule with suspicious microcalcifications are fat necrosis,initial degenerating FA,phyllodes tumor,triple-negative,mucinous,papillary,and metaplastic carcinoma (Table 1)[6,20].
Fat necrosis can be seen as a circumscribed soft-tissue mass with or without macro-or microcalcifications.At mammography,fat necrosis may be characterized by lipid cysts,microcalcifications,coarse calcifications near architectural distortion of surgical scar and focal masses[20,21].
The classic degenerating FA contains coarse pathognomonic calcifications.Occasionally,at the initial period of involution,the calcifications are small,numerous and may have a malignant appearance.Mammography helps to distinguish from ductal carcinoma.The microcalcifications in carcinomas are commonly small and asymmetrically located in a small area,whereas those in FAs tend to be denser,and more diffusely spaced or peripherical located in a nodule[20].
The phyllodes tumor is observed as a dense,round,or oval mass with circumscribed or indistinct margins.Libermanet al[22].described 4 cases of benign and malignant phyllodes tumors containing coarse,amorphous,and punctuate microcalcifications.Also,the presence of benign-looking specks or suspicious coarse punctate clusters of microcalcifications is reported in less than a third (29%) of phyllodes tumors with a carcinoma component,which would significantly change the subsequent management plan.By US the phyllodes tumor is round or oval,heterogeneous with cystic areas and posterior acoustic enhancement.By MRI,it is a round,lobulated mass with circumscribed margins.When the tumor presents cystic areas,the mass is hypointense on T1-sequences and hyperintense on T2-sequences.Only 33% of these tumors show enhancement,including the internal septa[6,22,23].
Mucinous carcinoma occurs more frequently in older people,and the average age at presentation is 71 years.It represents 1% to 4% of all breast cancers.On mammography,mucinous carcinoma appears as a circumscribed,round,or oval mass of low density,which may resemble a cyst or FA.Microcalcifications are rare,but when are present,they appear as round,coarse,amorphous and/or rarely pleomorphic.Microcalcifications most commonly occur in those tumors that demonstrate papillary or comedo growth patterns.Psammornatous microcalcifications that are seen with other types of mucin-producing tumors have been found in some cases.US shows a round or oval,circumscribed,and isoechoic mass with posterior acoustic enhancement.MRI demonstrates a circumscribed,oval mass,hyperintense on T2 and with heterogeneous enhancement[6,20,24].
The intraductal papillary neoplasms of the breast include papilloma,papilloma with atypical ductal hyperplasia (ADH) or DCIS,papillary DCIS (pDCIS),encapsulated papillary carcinoma (EPC),solid papillary carcinoma (SPC) and invasive papillary carcinoma (IPC).Papilloma,papilloma with ADH,DCIS,and pDCIS are associated with microcalcification.Papillary carcinomas with microcalcifications within the tumor are usually pleomorphic but may occasionally be coarse or stippled in appearance.US can reveal a hypoechoic solid mass or a complex cyst with septations or mural-based papilliform nodularity.The most common finding of EPC on mammography is a solitary oval or round mass with microlobulated or circumscribed margins and calcifications are not uncommon and are mainly amorphous or pleomorphic.In SPC concomitant microcalcification on mammography was rarely reported in the literature cases and 33.32% were accompanied by amorphous calcifications.Sonographically has been reported as multiple nodules accompanied by ductal ectasia,well-circumscribed,complex,cystic lesion,and homogeneous solid lesions.Ciureaet al[25].reported IPCs as round or lobulated masses,often associated with mammographic calcification.Micropapillary DCIS is frequently associated with “snake skin-like” microcalcification[25-27].
In Krizmanich-Conniffet al[28] series found that 7% of triple-negative carcinoma appeared as clustered microcalcifications,whilst another 29% manifested as masses with associated microcalcifications.The rapid growth,with no precancerous stage,also explains the low incidence of microcalcifications.Microcalcifications inside a mass or isolated segmental type calcifications were more often associated with a DCIS and a human epidermal growth factor receptor 2+status.On US and MRI images,commonly theses tumors appear as a round or oval mass with irregular,spiculated,or circumscribed margins with rapid early enhancement and a late washout curve[6,28,29].
Metaplastic breast cancer,on mammography,are commonly large masses of 4.2 cm,with high density and smooth,well-defined and spiculated margins.Microcalcifications are very rare within the mass;when this happens,they are more likely to be amorphous,fine pleomorphic,fine linear,and lastly coarse heterogeneous[30,31].
It is important to understand that suspicious microcalcifications within masses can indicate the presence of malignancies such as mucinous carcinoma,metaplastic carcinoma with less incidence than CDIS within FA.In our case,microcalcifications have to be distinguished from fat necrosis because their localization is near surgical scar.Is not frequent to encounter CDIS within a nodule but the radiologist has to be aware of it.A stereotactic biopsy may be used to remove the group of microcalcifications however there were at 2 cm from the skin,which contraindicated this interventional procedure.According to the site of the findings in mammography,we corroborated that the microcalcifications that were seen within one of the nodules were the suspicious group,therefore we were able to make the biopsy by US instead of used stereotactic-guided vacuum-assisted system.After the diagnosis of DCIS was reported by pathologist,to assurance a successful surgery for nonpalpable nodule,wire localization is needed.The limitation of our case is that MRI images of this patient are not available in our Institution,and we cannot detail the findings by this method.
The treatment of choice is conservative surgery,if 2 or fewer suspicious lymph nodes are found on imaging,or 2 or fewer positive lymph nodes are confirmed by needle biopsy,then is recommended sentinel lymph node mapping.Adjuvant therapy includes radiotherapy and endocrine therapy.The majority have good prognosis,with no difference between young and older women.Ten percent of patients present with recurrence or metastasis[1-3,6,9].
CONCLUSlON
FAs are common in imaging studies,but the presence of a DCIS within the nodule is rare and has nonspecific findings on imaging.Faced with a circumscribed nodule within microcalcifications is a diagnostic challenge and by imaging studies can simulate benign and malignant pathologies.The radiologist has to consider in the differential diagnosis DCIS within a FA or other round tumors associated with microcalcifications,and the core biopsy should be performed.We recommend a multidisciplinary approach for adequate treatment and follow-up.
FOOTNOTES
Author contributions:Olivares-Antúnez Y performed searched the literature and wrote the manuscript;Dávila-Zablah YJ performed the research and reviewed the manuscript;Vázquez-ávila JR and Gómez-Macías GS performed the subtraction image processing,discussed the results and contributed to the final manuscript;Mireles-Aguilar MT was the primary surgeon,and provided surgical insights into the case;and Garza-Montemayor ML was the senior author who supervised and made substantial contributions to the conception of the work.
lnformed consent statement:Informed written consent was obtained from the patient for the publication of this report and any accompanying images.
Conflict-of-interest statement:All the authors report no conflicts of interest for this article.
CARE Checklist (2016) statement:The authors have read the CARE Checklist (2016),and the manuscript was prepared and revised according to the CARE Checklist (2016).
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is non-commercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:Mexico
ORClD number:Yazmin Olivares-Antúnez 0000-0002-3588-645X;Yesika Janett Dávila-Zablah 0000-0002-5153-2360;José Raúl Vázquez-ávila 0009-0004-4592-5899;Gabriela Sofía Gómez-Macías 0000-0003-4849-492X.
S-Editor:Luo ML
L-Editor:A
P-Editor:Zhao S
 World Journal of Radiology2024年3期
World Journal of Radiology2024年3期
- World Journal of Radiology的其它文章
- Artificial intelligence for disease diagnostics still has a long way to go
- Evaluating pediatric ureteropelvic junction obstruction: Dynamic magnetic resonance urography vs renal scintigraphy 99mtechnetium mercaptoacetyltriglycine
- Chronic pancreatitis: Pain and computed tomography/magnetic resonance imaging findings