
Liver transplantation as an alternative for the treatment ofintrahepatic cholangiocarcinoma: Past,present,and future directions
2024-05-03 09:15:30SudhaKodaliAshtonConnorSouhailThabtElizabthBromboszMarkGhobrial
Sudha Kodali ,Ashton A Connor ,Souhail Thabt ,Elizabth W Brombosz ,R Mark Ghobrial a,b,d,,*
a Sherrie and Alan Conover Center for Liver Disease and Transplantation, Houston Methodist Hospital, Houston, TX 77030, USA
b JC Walter Jr Transplant Center, Houston Methodist Hospital, Houston, TX 77030, USA
c Department of Medicine, Weill Cornell Medical College, New York, NY, USA
d Department of Surgery, Houston Methodist Hospital, Houston, TX 77030, USA
e Department of Surgery, Weill Cornell Medical College, New York, NY, USA
f School of Medicine, New Giza University, Giza, Egypt
Keywords: Liver transplantation Cholangiocarcinoma Hepatectomy Transplant oncology Liver neoplasm
ABSTRACT Intrahepatic cholangiocarcinoma (iCCA) is a rare biliary tract cancer with high mortality rate.Complete resection of the iCCA lesion is the first choice of treatment,with good prognosis after margin-negative resection.Unfortunately,only 12%-40% of patients are eligible for resection at presentation due to cirrhosis,portal hypertension,or large tumor size.Liver transplantation (LT) offers margin-negative iCCA extirpation for patients with unresectable tumors.Initially,iCCA was a contraindication for LT until size-based selection criteria were introduced to identify patients with satisfied post-LT outcomes.Recent studies have shown that tumor biology-based selection can yield high post-LT survival in patients with locally advanced iCCA.Another selection criterion is the tumor response to neoadjuvant therapy.Patients with response to neoadjuvant therapy have better outcomes after LT compared with those without tumor response to neoadjuvant therapy.Another index that helps predict the treatment outcome is the biomarker.Improved survival outcomes have also opened the door for living donor LT for iCCA.Patients undergoing LT for iCCA now have statistically similar survival rates as patients undergoing resection.The combination of surgery and locoregional and systemic therapies improves the prognosis of iCCA patients.
Introduction
Cholangiocarcinoma (CCA) is a malignancy arising from the bile duct epithelial cells or nearby hepatic progenitor cells [1].Approximately 90000 people globally are diagnosed with CCA each year [2],80%-93% of whom die within 5 years of diagnosis [3].Most patients present with an advanced stage of disease,leading to poor overall survival (OS) rates [3].Thus,although the incidence is lower than other cancers,the mortality from CCA is higher [4].
There are two main types of CCA based on anatomic location:intrahepatic (iCCA) and extrahepatic.The iCCA subtype forms in second-order or higher bile ducts within the liver parenchyma,whereas extrahepatic CCA involves bile ducts in the liver hilum or outside the liver.Extrahepatic tumors are further subclassified anatomically into perihilar and distal CCA (dCCA) (Fig.1).Perihilar CCA (pCCA,also called Klatskin tumor) occurs in the region of the first-order right and left bile ducts and the common hepatic duct.dCCA occurs in the common bile duct region.iCCA patients comprise around 20% of CCA cases,with pCCA and dCCA encompassing around 55% and 25% of cases,respectively [5].Reports suggest that the incidence of iCCA is increasing,while the incidence of pCCA and dCCA are decreasing [5,6].
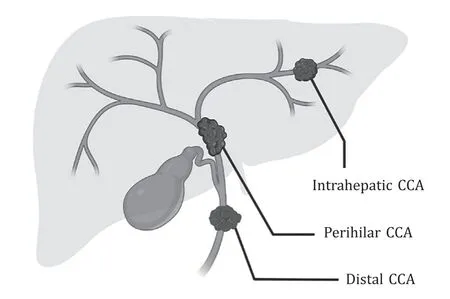
Fig.1. Diagram of the main subtypes of cholangiocarcinoma (CCA),categorized by anatomical location.
There are multiple risk factors for pathogenesis of iCCA,including cholelithiasis,viral hepatitis,primary sclerosing cholangitis,alcoholic and nonalcoholic steatohepatitis,Caroli’s disease,and liver fluke infection [3,6,7].Lifestyle factors like alcohol overuse and smoking are also risk factors of iCCA [3,7].These factors initiate carcinogenesis of iCCA through chronic bile duct epithelium inflammation and/or cholestasis,as well as epigenetic and genetic alterations [8,9].However,a majority of CCA patients do not have a history of these risk factors [6].
Treatment for iCCA may include locoregional therapy,systemic therapy,and/or surgery [10].Many iCCA patients receive a combination of therapies,for example,systemic therapy combined with local resection.In this review,we focused on a comparison of the two surgical treatments for iCCA: resection and liver transplantation (LT).Consensus guidelines only identify resection with negative margins as potentially curative [11].However,LT also offers the potential of margin-negative removal of iCCA and can hence be potentially curative.LT is a particularly important option for patients whose iCCA is deemed unresectable.
Resection for iCCA
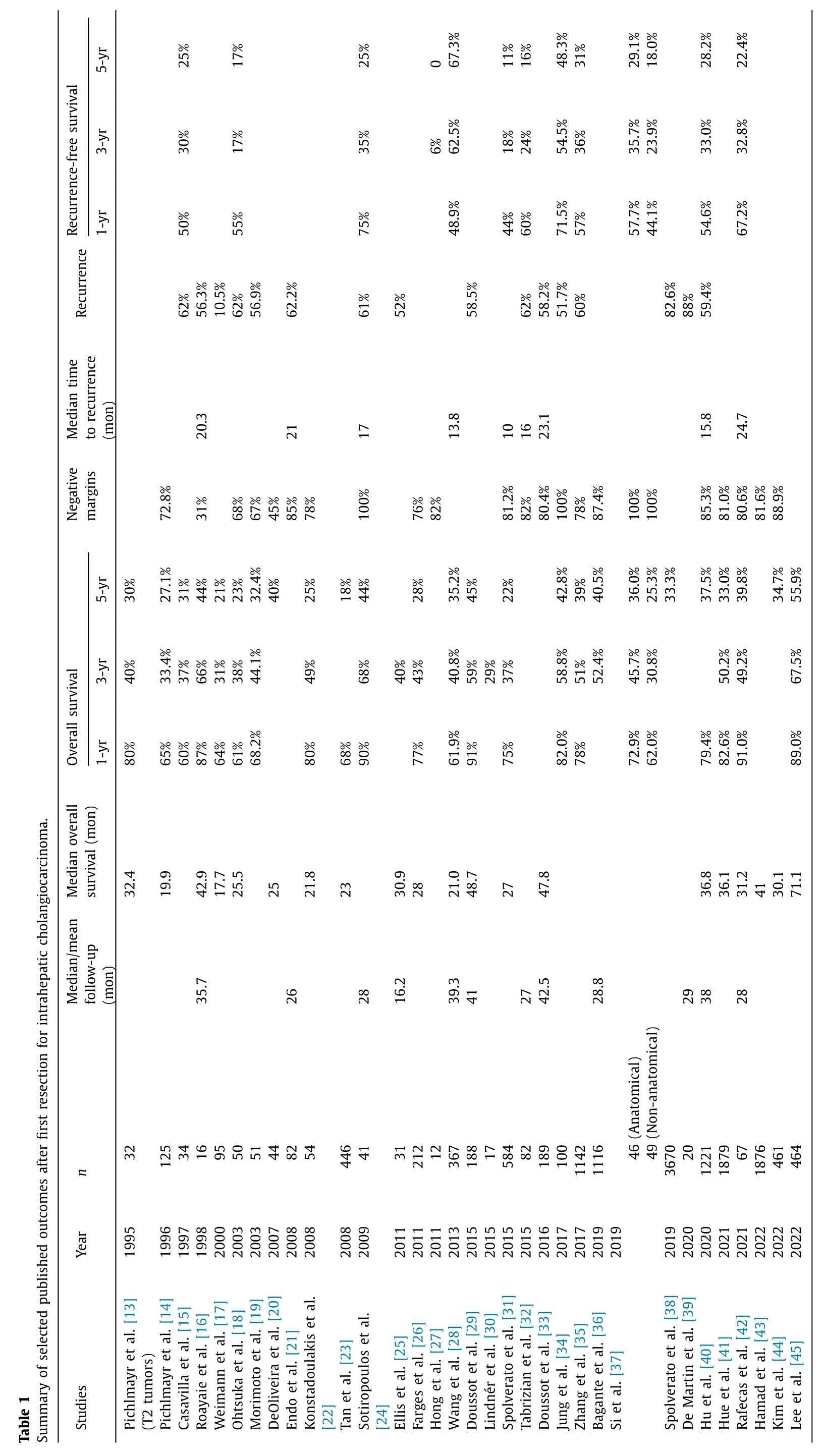
Surgical resection is the first choice for iCCA treatment if anatomically and physiologically amenable [12].Removal of the tumor with negative (R0) margins yields good long-term recurrencefree survival (RFS) and OS (Table 1) [13-45].When R0 resection of liver-limited disease is achieved,resection is considered a potentially curative therapy.Unfortunately,resection with negative margins is not technically feasible for most patients.Additionally,only a minority of patients-an estimated 12%-40%-are candidates for resection at presentation [46].Even though resection provides a survival advantage,recurrence rates are high without R0 margins,and resection is often limited by the size of the predicted future liver remnant (FLR) [47].A recent phase II clinical trial has demonstrated the potential for iCCA downstaging to resectability in 9 of 41 patients with locally advanced tumor burden using a combination of systemic therapy (gemcitabine and cisplatin) with locoregional transarterial radioembolization [48].
Patient selection for resection
Several factors are taken into consideration while determining candidacy for resection,and one of the most important factors is FLR size (Fig.2).Inadequate FLR increases the patient’s risk of liver failure postoperatively [46].Resections that would prohibitively interfere with major vascular or biliary structures of the liver are also generally contraindicated.
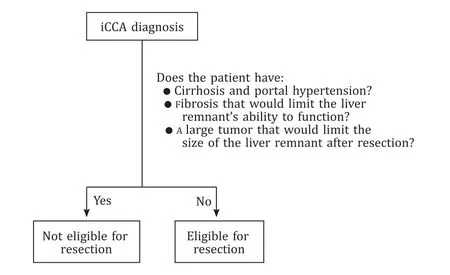
Fig.2. Criteria for patient with intrahepatic cholangiocarcinoma (iCCA) eligibility for liver resection.Patients with unresectable tumors may be considered for liver transplantation.
Resections can be anatomical or non-anatomical.Anatomical resection involves the removal of the entire section of affected liver,including the associated biliary and vascular pedicles.Proponents argue that anatomic resection reduces the risk of metastasis by removing the blood vessels most likely to carry metastatic tumor cells.Non-anatomical resection aims to maximize liver remnant parenchyma.A study by Si et al.in 2019 compared outcomes of propensity-score matched patients undergoing anatomical and non-anatomical resections [37].The authors found that patients receiving anatomical resection had significantly better OS and RFS.In addition,multivariate analysis revealed that non-anatomical resection was independently associated with a higher risk of death and recurrence.
Factors affecting recurrence and survival post-resection
Multiple factors are tied to long-term outcomes after hepatic resection.Surgical margins are one of the strongest predictors of tumor recurrence and patient survival after hepatectomy.Patients undergoing margin-negative resection have 5-year RFS rates of 18%-48.3% and 5-year OS rates of 25.3%-44% (Table 1) [24,34,37].Studies have also identified tumor margin as an independent predictor of OS in multivariable analyses [15,20,26,36].A recent metaanalysis by Dai and coauthors agreed that wide resection margins(>10 mm) improves OS and RFS [49].
Tumor characteristics are also associated with RFS and OS after resection.Measures of tumor burden such as largest tumor diameter and tumor number are significantly associated with OS or RFS [15-17,21,24,28,33,35-37,39].Similarly,higher stage tumors and poorly differentiated tumors also increase the risk of recurrence and death after resection [13,17,33,35,36,40].Tumor vascular invasion was independently associated with OS [28,40,42]and RFS [33,40,32].
Some studies have proposed a link between biomarkers and post-resection outcomes.Wang and colleagues found that serum carcinoembryonic antigen (CEA) and carbohydrate antigen 19-9(CA19-9) predicted OS after resection [28].Similarly,Si and colleagues also reported that CEA and CA19-9 were associated with both RFS and OS [37].
LT for iCCA
Although resection is the preferred local treatment for CCA,some patients are not resectable due to concurrent acute or chronic liver disease,cirrhosis,portal hypertension,or the anatomic features of the iCCA tumor(s) described above [50,51].These patients may be considered for LT.LT may attain negative oncologic margins and remove intrahepatic micro-metastases [10].
History of LT for hepatic malignancy
Initial attempts to treat primary liver cancer with LT resulted in high recurrence and low OS rates [52,53].However,a 1996 paper by Mazzaferro and colleagues demonstrated that hepatocellular carcinoma (HCC) patients with relatively low tumor burden can have good post-LT survival [54].In HCC,we have since learned that these initial limits of HCC tumor size and number could be somewhat expanded while maintaining good outcomes [55-57].Recent studies indicate that tumor biology is another predictor of posttransplant outcomes: patients with more aggressive HCC have decreased survival [58-60].Carefully selected patients demonstrating radiologic and biologic (e.g.,biomarker) tumor stability or response to neoadjuvant locoregional or chemotherapy can have excellent outcomes,even when tumor burden exceeds traditional cutoffs [58].Combining tumor size with biomarkers such as alphafetoprotein and des-γ-carboxy prothrombin can predict post-LT recurrence and OS more accurately [61,62].
History of LT for CCA
Like HCC,CCA was once a contraindication for LT.As treatments for CCA improved,some centers began to report successful cases with combined neoadjuvant therapy and LT for pCCA [63,64].Following these successes,researchers at the Mayo Clinic set out to identify selection criteria for patients expected to have good outcomes after LT for pCCA [65].Heimbach and colleagues reported on 28 patients receiving neoadjuvant radiotherapy combined with 5-fluorouracil and subsequent LT.The patients had excellent 1-and 5-year post-LT OS rates of 88% and 82%,respectively.Patients with unresectable pCCA ≤3 cm with elevated CA19-9 (>100 U/mL)and/or biopsy proven pCCA are eligible for exception points if they have neither intra-nor extrahepatic metastases nor regional lymph nodes metastases.
History of LT for iCCA
Initial attempts at LT for iCCA also yielded poor results,with dismal 1-year OS rates between 13.9% and 53% prior to 1996 (Table 2) [13-15,17,27,30,34,38,39,41,44,45,52,66-90].Between 1990 and 2010,5-year survival rates ranged between 0 and 40%,with 1 report of 83% survival in a cohort of 10 patients [69].These early studies did not restrict LT based on tumor burden;their selection protocols only excluded patients with resectable tumors.Papers that did report 5-year OS rates over 50% only included patients with incidentally diagnosed iCCA [69].Outcomes published in the early 2010s (2010-2013) included slightly improved 1-year OS rates ranging between 51% and 84.2%,but with low 5-year OS rates between 21.8% and 45% [27,76-78].
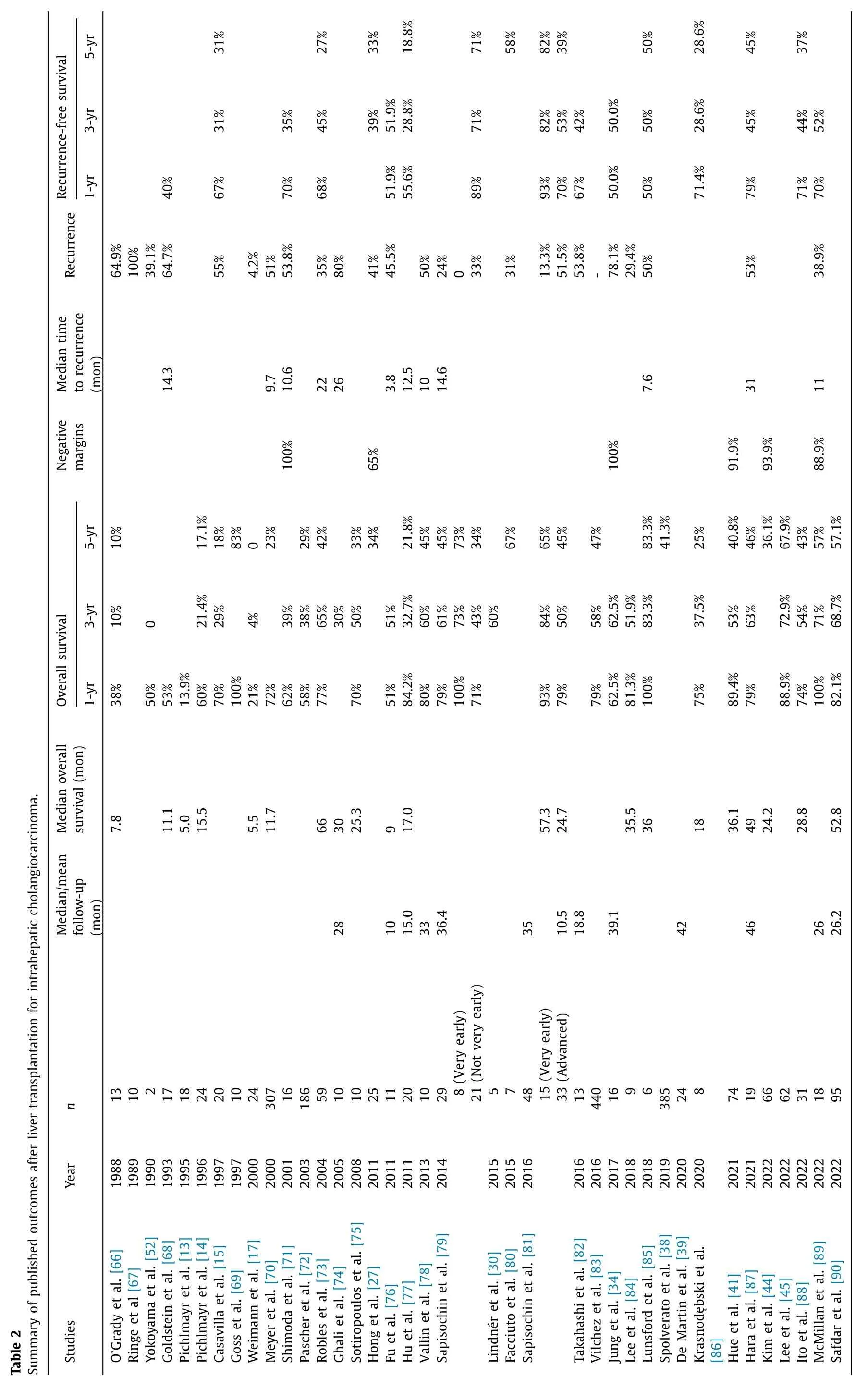
LT gained greater acceptance after the suggestion of sizebased selection criteria for iCCA,as with HCC and pCCA.In 2014,Sapisochin and colleagues published a retrospective study examining the outcomes of patients undergoing LT for iCCA [79].They identified a subgroup of patients with “very early” iCCA,defined as a single iCCA tumor ≤ 2 cm in diameter.Post-LT OS rates for “very early” patients were 100%,73%,and 73% at 1,3,and 5 years,respectively.A subsequent multicenter study reported 1-,3-,and 5-year OS rates of 93%,84%,and 65% for similarly stratified patients [81].LT recipients with “advanced” iCCA,defined as multiple tumors or a single tumor>2 cm in diameter,had OS rates of 79% at 1 year,50% at 3 years,and 45% at 5 years post-LT [81].Importantly,the authors noted that tumor size was not a significant predictor of RFS in their multivariate analysis,suggesting that size did not fully reflect biological aggressiveness in their cohort.
In addition to size-based selection,evidence of the benefits of neoadjuvant therapy and LT for iCCA continued to grow.Hong and colleagues reported higher post-LT recurrence rates in iCCA patients who did not receive neoadjuvant therapy [91].Similarly,a study by Hu et al.found that receiving neoadjuvant therapy reduced the risk of death [risk ratio (RR)=0.050;P=0.005]and recurrence (RR=0.233;P=0.042) in univariate analysis [77].
The effects of combined LT and neoadjuvant therapy led some centers to consider response to therapy when selecting LT candidates.Authors from Houston Methodist Hospital have shown that patients with locally advanced,unresectable iCCA receiving neoadjuvant therapy can have good OS after LT [85,89].Per center protocol,patients were eligible for LT if their tumors were radiologically regressing or stable for ≥6 months on neoadjuvant systemic therapy.Patients (n=18) with locally advanced iCCA had OS rates of 100% at 1 year,71% at 3 years,and 57% at 5 years post-LT [89].Thus,selecting patients based on tumor biology and measured by response to neoadjuvant therapy can lead to good post-LT survival rates.
Recent papers have continued to emphasize the importance of combination neoadjuvant therapy.Ito and colleagues from the University of California,Los Angeles reported that patients receiving combination neoadjuvant systemic and locoregional therapy had improved outcomes post-LT relative to use of either single therapy [88].Tumor size did not affect OS or RFS after LT.An analysis of National Cancer Database iCCA data revealed that LT recipients were more likely to receive neoadjuvant and/or adjuvant therapies than patients undergoing resection,emphasizing the importance of combination therapies [44].
Patient selection for LT
As detailed above,initial reports of positive outcomes after LT for iCCA involved either very small or incidentally discovered tumors,with a diameter of 2 cm or less (Table 2) [79,81].Combined with the success of patient selection based on tumor burden for HCC and pCCA,most centers only performed LT for patients with a very small iCCA tumor burden.Additional reports by teams from Mount Sinai Medical Center and Sun Yat-sen University have also supported the efficacy of size-based cutoffs and outcomes [80,92].A recent meta-analysis by Ziogas and others agreed that smaller tumor size was associated with improved survival [93].
However,limiting LT to patients with very small iCCA tumors disqualifies most patients from receiving this potentially lifesaving therapy,including some who may have non-aggressive tumors.Additionally,the landmark study by Sapisochin and colleagues noted that tumor size was not an independent predictor of tumor recurrence [81].Recent studies have also shown that tumor burden is not an accurate predictor of outcomes after transplantation for iCCA [88,94].
Protocols that select patients based on tumor biology have shown promise.For example,reports from Houston Methodist Hospital have shown that tumor response to neoadjuvant therapy is a better predictor of OS than tumor size [85,89].Patients with locally advanced iCCA who respond to neoadjuvant treatment(most frequently gemcitabine/cisplatin chemotherapy) achieved good long-term survival post-LT.Other studies have shown a strong association between post-LT OS and RFS and variables such as microvascular invasion and poor differentiation [39,77,82].Patient selection based on tumor biology may allow for treatment of advanced tumors with excellent,potentially curative outcomes.
Tumor genetic mutations and expression patterns show great promise in identifying iCCA patients amenable to LT.Pre-LT identification of mutations through technologies such as next-generation sequencing of solid tumor biopsies and cell-free DNA,RNA,and/or protein expression could help clinicians select appropriate neoadjuvant therapies and prognosticate patient outcomes [10,95,96].In addition,sequencing explanted tumors may help transplant oncology teams tailor surveillance and select effective therapies to treat recurrence.Studies of LT recipients with iCCA have sequenced explanted tumors and identified mutations in genes such as fibroblast growth factor receptor (FGFR) and isocitrate dehydrogenase 1 (IDH1),which have approved targeted therapies(Table 3) [89,97].Intratumoral heterogeneity has been observed in iCCA [98-100]and has been linked to overall prognosis in iCCA patients [101].Additional research is needed to learn whether such heterogeneity has significant role in prognosticating outcomes in LT candidates and recipients.

Table 3Gene mutations identified in liver transplantation recipients (reported as percent of the total study population) with intrahepatic cholangiocarcinoma that have approved targeted therapies.
Living donor LT for iCCA
Recent studies have begun to examine whether iCCA patients are good living donor liver transplantation (LDLT) candidates.Traditionally,iCCA patients were excluded from LDLT because the benefit to the recipient (OS,RFS) was not large enough to offset the risk to the donor [102].Many reports of outcomes in LDLT recipients with iCCA come from patients with an incidental iCCA diagnosis [87,103].Fortunately,the recent improvements in post-LT outcomes described above have renewed the possibility of LDLT for these patients as double equipoise becomes more achievable.
In 2005 a case series by Jonas and colleagues reported outcomes in 2 iCCA patients undergoing LDLT [104].Both patients had experienced recurrence at 31 months but were alive at 46 and 35 months post-LDLT,respectively.Hafeez Bhatti et al.identified a combined cohort of 16 incidentally diagnosed iCCA and pCCA patients undergoing LDLT for presumed diagnosis of HCC in a large retrospective review of their center’s data [103].They reported an overall 3-year RFS of 47%.Importantly,patients with well-or moderately-differentiated tumors had a 3-year RFS of 64%,suggesting that outcomes may improve with careful patient selection.A multicenter study from Japan by Hara et al.yielded RFS rates of 79%,45%,and 45% at 1,3,and 5 years post-LDLT in patients incidentally diagnosed with iCCA in explant pathology [87].Post-LDLT OS rates were 79%,63%,and 46% at 1,3,and 5 years,respectively.A recent systematic review by Rauchfu? et al.identified 6 patients undergoing LDLT for iCCA;3 LDLT recipients recurred.Patients who were still alive had a median follow-up of 30.5 months [102].
Transplantation vs.resection: direct comparisons
Comparisons between resection and LT for iCCA are difficult to make since there has not been a trial directly comparing them in similar patient cohorts.For example,in 1995 Pichlmayr et al.[13]reported a 1-year OS rate of 13.9% in LT recipients,versus 80% in patients with stage II tumors undergoing resection [32].However,in this study,patients with advanced tumors were not excluded from LT: 72% (13/18) of LT recipients had stage IV iCCA,compared to 41% (13/32) of resected patients.It is therefore unsurprising that such papers have reported worse survival in LT recipients relative to those undergoing resection [17,34,42].
Some authors have assessed outcomes after resection and LT in patients treated under a single protocol (Table 4).A subset of these papers matched LT recipients to patients undergoing resection.For example,Jung et al.compared the outcomes of 16 LT iCCA recipients to 100 propensity-matched patients undergoing resection [34].The OS (P=0.082) or RFS (P=0.121) were similar between the two groups of patients.Hue and colleagues also compared iCCA patients undergoing LT or resection using data from the United States National Cancer Database (NCDB) [41].OS rates were similar for LT recipients and both unmatched (P=0.34) and matched (P=0.57) resection patients.Similarly,an NCDB analysis by Kim et al.found that propensity-matched resection recipients had similar OS to LT recipients (P=0.53) [44].Lee et al.also conducted a multivariate analysis of NCDB data;LT recipients were at a significantly reduced risk of dying relative to matched resected patients (adjusted hazard ratio=0.33,95% CI: 0.16-0.68;P=0.04) [45].
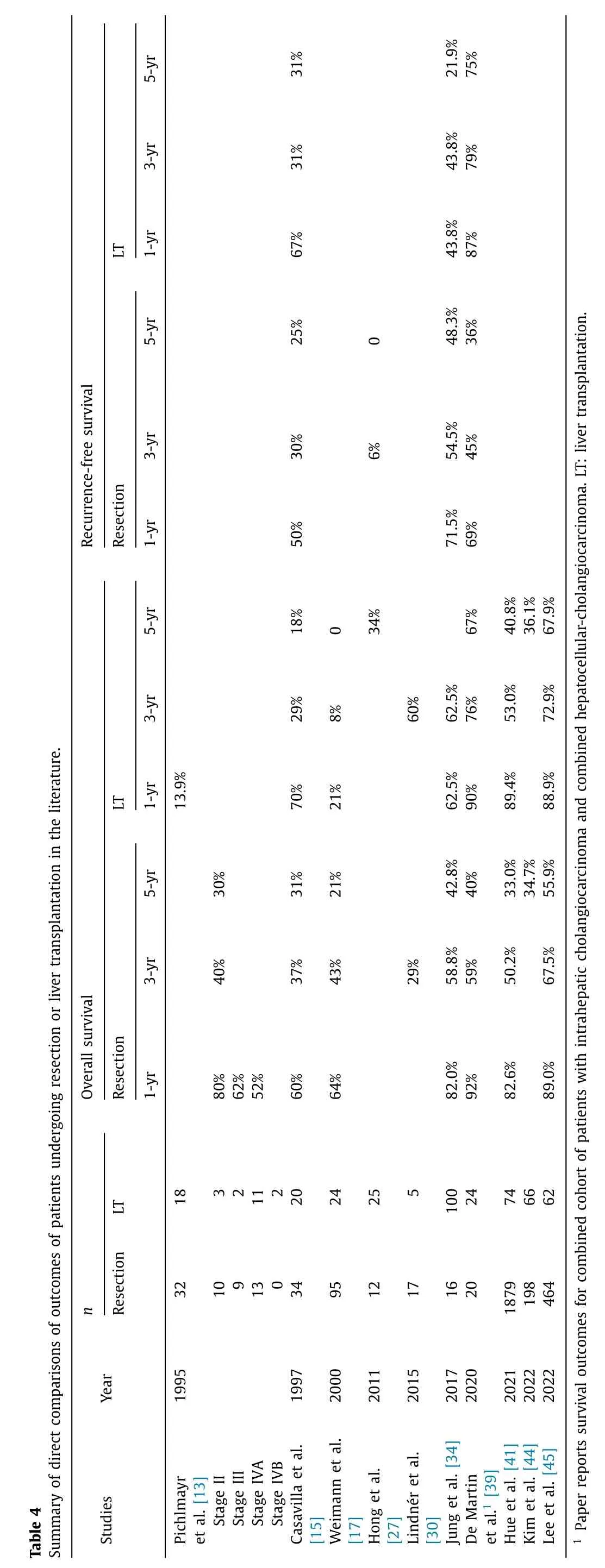
As described above,patients who are good candidates for resection are clinically different from good candidates for LT.LT is a more aggressive approach,generally for sicker patients with locally advanced iCCA and underlying liver disease.Resection is often for patients with early,localized iCCA lesions.However,there is a growing body of evidence showing that LT has similar or improved outcomes compared to resection for iCCA,despite these differences in the patient populations.These data support the efficacy and importance of LT for iCCA,affirming the continued utilization of donor grafts in these patients.
Future directions
Although research and clinical advances have improved outcomes after LT for iCCA,additional studies are still needed.Early work has shown that biomarkers have the potential to identify patients likely to survive after LT and respond to neoadjuvant treatment,leading to better post-surgical outcomes.Additional research is needed to identify non-invasive predictors of post-LT outcomes that can be measured prior to evaluation for transplantation.These biomarkers would allow clinicians to identify aggressive tumors,regardless of size,and prioritize LT in patients with the lowest risk of recurrence.
Similarly,advances in adjunctive therapies have the potential to further improve transplant outcomes for iCCA.Neoadjuvant and adjuvant targeted therapies tailored to a patient’s tumor genetic profile can work in concert with LT to increase post-transplant survival even further.Drug development is an area of active basic and translational research to create new therapies for iCCA tumors that do not respond to current therapies [105].Effective neoadjuvant therapies are particularly important given the effectiveness of LT candidate selection strategies based on response to neoadjuvant therapy.
Conclusions
iCCA patients have a poor prognosis without treatment but may be cured with combinations of surgery and systemic and/or locoregional therapy.Resection is the preferred surgical treatment when feasible,but LT can yield excellent long-term outcomes in wellselected patients with unresectable tumors.Post-LT outcomes depend on patient selection,which can be either size-based and/or tumor biology-based.Selection based on tumor aggressiveness has the potential to expand lifesaving treatment to patients with large but indolent tumors.Post-LT survival rates are anticipated to increase with the development of non-invasive biomarkers and better selection criteria.Improvements in post-LT outcomes will also depend on the introduction of further neoadjuvant and adjuvant therapies for iCCA.
Acknowledgments
Fig.1 was created using BioRender software (BioRender.com).
CRediT authorship contribution statement
Sudha Kodali:Conceptualization,Data curation,Formal analysis,Investigation,Supervision,Validation,Writing -original draft,Writing -review &editing.Ashton A Connor:Conceptualization,Data curation,Formal analysis,Investigation,Supervision,Validation,Writing -original draft,Writing -review &editing.Souhail Thabet:Conceptualization,Data curation,Writing -original draft.Elizabeth W Brombosz:Conceptualization,Data curation,Formal analysis,Investigation,Project administration,Visualization,Writing -original draft,Writing -review &editing.R Mark Ghobrial:Conceptualization,Investigation,Supervision,Resources,Validation,Writing -review &editing.
Funding
None.
Ethical approval
Not needed.
Competing interest
R Mark Ghobrial is a member of the advisory board for Trans-Medics and has received stock in the company.For the rest authors,no benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
 Hepatobiliary & Pancreatic Diseases International2024年2期
Hepatobiliary & Pancreatic Diseases International2024年2期
- Hepatobiliary & Pancreatic Diseases International的其它文章
- Editors
- Information for Readers
- Meetings and Courses
- Liver transplantation and liver resection as alternative treatments for primary hepatobiliary and secondary liver tumors: Competitors or allies?
- Laparoscopic anatomical liver resection of segment 7 using a sandwich approach to the right hepatic vein (with video)
- Severe liver injury and clinical characteristics of occupational exposure to 2-amino-5-chloro-N,3-dimethylbenzamide: A case series