
Ex vivo liver resection and auto-transplantation as an alternative for the treatment of liver malignancies: Progress and challenges
2024-05-03 09:15:28XinYangLuLuWenWeiZhuYiFengTaoCongHuanShenJinHongChenZhengXinWangLunXiuQin
Xin Yang,Lu Lu,Wen-Wei Zhu,Yi-Feng Tao,Cong-Huan Shen,Jin-Hong Chen,Zheng-Xin Wang,Lun-Xiu Qin
Hepatobiliary Surgery and Liver Transplantation Centers, Department of General Surgery, Huashan Hospital & Cancer Metastasis Institute, Fudan University,Shanghai 200040, China
Keywords: Ex vivo liver resection Liver auto-transplantation Oncology Liver malignancies
ABSTRACT Hepatectomy is still the major curative treatment for patients with liver malignancies.However,it is still a big challenge to remove the tumors in the central posterior area,especially if their location involves the retrohepatic inferior vena cava and hepatic veins.Ex vivo liver resection and auto-transplantation (ELRA),a hybrid technique of the traditional liver resection and transplantation,has brought new hope to these patients and therefore becomes a valid alternative to liver transplantation.Due to its technical difficulty,ELRA is still concentrated in a few hepatobiliary centers that have experienced surgeons in both liver resection and liver transplantation.The efficacy and safety of this technique has already been demonstrated in the treatment of benign liver diseases,especially in the advanced alveolar echinococcosis.Recently,the application of ELRA for liver malignances has gained more attention.However,standardization of clinical practice norms and international consensus are still lacking.The prognostic impact in these oncologic patients also needs further evaluation.In this review,we summarized the principles and recent progresses on ELRA.
Introduction
Surgical treatment is the first choice for liver malignancies [1].Unfortunately,not all patients are suitable for conventional liver resections.Because of the occult nature of liver cancer,70% patients are diagnosed at an advanced stage and therefore,miss the opportunity of surgical treatment.In addition,it is a big challenge to remove some tumors due to their anatomical location such as in central posterior area,in junction to major blood vessels and/or bile ducts which may cause severe bleeding.These liver tumors were categorized as "non-resectable" [2-4].The progress in surgical techniques,such as total hepatic vascular occlusion,portacaval shunting extracorporeal hepatectomy and liver transplantation,has led to the development ofex vivoliver resection and autotransplantation (ELRA).This technique is considered a good solution to the above mentioned problems,allowing also to provide the opportunity for radical treatment (R0) of these liver malignancies [4-6].
ELRA is the combination of “traditional” liver resection (LR) and liver transplantation (LT).This procedure allows to resect liver tumors more accurately,reduce the risk of uncontrollable intraoperative bleeding,increase the operative space for complex vascular reconstructions,and minimize ischemic damage.Moreover,ELRA is an advanced surgical technique which eliminates the need for both a donor allograft and life-long immunosuppression,the risk of disease progression,and waiting time for LT [4,7,8].ELRA implies a high degree of technical difficulties and requirements.Furthermore,ELRA causes postoperative complications and also,ELRA has not been standardized in clinical practice,which might explain why ELRA is not widely applicable in clinical practice.However,the three-dimensional reconstruction of pre-operative images and liver indocyanine green (ICG) clearance allow us to estimate the residual liver volume (RLV) preoperatively [9-11],and the improvement of surgical instruments also facilitates the advances of this procedure,all of which lead to a more widespread recognition of the value of ELRA in the treatment of specific liver diseases,first in the treatment of alveolar hepatic echinococcosis [5,12,13]and very recently also in the treatment of hepatobiliary malignancies.This ELRA technique has gradually matured in several leading hepatobiliary surgery centers in China [2,3,14].
The development of ELRA
The concept and practice ofin vitroand auto-transplantation started in 1963 with autologous kidney transplantation in patients with high ureteral injury [15].In 1980s,the development of transplant techniques such as reduced-size,split and auxiliary liver transplantation [16,17]led to the development of extracorporeal hepatectomy.In 1988,Pichlmayr et al.pioneered this type of surgery;a partial hepatectomy done for large tumor masses was followed by an orthotopic re-implantation of the remaining liver [18].The liver,including retrohepatic inferior vena cava(RHIVC),was removed using extracorporeal veno-venous bypass.The liver was protected from ischemic damage using hypothermicin situperfusion followed by the extra-corporeal resection performed in an iced water bowl.During the resection,the liver was repeatedly perfused using a cold HTK-solution.This operation was applied in patients with hepatocellular carcinoma (HCC) and cholangiocarcinoma (CCC),colorectal liver (CRLM) and leiomyosarcoma metastasis as well as some non-malignant lesions such as giant focal nodular hyperplasia (FNH) and hemangioma [19-22].However,the reported perioperative mortality rate of these pioneering series was as high as 30% (especially in cholestatic patients) and the survival was poor (<2 years) [23].
In 1997,Dong et al.reported the first ELRA in China [24].Since then,several Chinese centers have successfully performed this procedure.In 2010,Wen et al.performed ELRA for the first time in the world to treat the end-stage hepatic alveolar echinococcosis disease (HAED) [25].Subsequently,other centers adopted this technique in this disease.In 2018,Aji et al.[5]reported the largest ELRA series including 69 cases of HAED.The perioperative mortality rate was only 7.24%.Although the effectiveness and safety of ELRA in the case of HAED became well established,the high “technicity” of the procedure,and the still higher morbidity and mortality limited the application of ELRA in the treatment of hepatobiliary malignancies.
Surgical indications
ELRA is performed if the conventionally unresectable tumor invades the RHIVC,the hepatic vein(s) and the hepato-caval venous confluence [26].ELRA allows effectively to solve the problem of poor exposure or very difficult and risky liver resection.Moreover,ELRA raises the rate of curative (R0) resections.In the earlier experiences,the long operative time,the complexity of the procedure,the prolonged venous bypass time,and the realization of the partial hepatectomy under cold perfusion were all responsible for a severe liver ischemia reperfusion injury (IRI) and for a high morbidity and mortality.Until now,there is no widely accepted way to evaluate the applicability of this surgery.The key for success is to accurately evaluate the functional reserve of liver remnant and to refine indications.
ELRA has been reported as a treatment of HAED,CRLM,CCC,HCC,leiomyosarcoma,and some benign diseases including FNH,hemangioma,leiomyoma and solid fibroma [27-30].ELRA is most suitable for large size tumors and/or tumors in a poorly accessible location such as those adjacent to large blood vessels or biliary structures [6,31].It is therefore valuable to consider ELRA as an alternative to a conventional,high risk,hepatectomy or as a rescue after previous unsuccessful resection attempt.The possible indications for ELRA include: (1) complicated hydatid end-stage disease [7,32];(2) malignant,and also some benign,tumors located in caudate lobe and invading the second or third hepatic hilar structures [33-36];and (3) those involving RHIVC and hepatic veins [3,37];(4) complicated liver trauma with laceration of the hepatic vein confluence and inferior vena cava (IVC) and (5)chronic Budd-Chiari syndrome [38].The surgical indications of ELRA are listed in Table 1.

Table 1Comparison of the respective surgical indications for ELRA and non-ELRA.
Preoperative evaluation
ELRA is now an established clinical procedure which should be applied in non-cirrhotic patients with normal liver function because cirrhotic patients may not tolerate this procedure due to the risks of perioperative liver failure and mortality.
Accurate preoperative evaluation of liver function reserve is essential in the candidate of ELRA: (1) normal liver function,Child-Turcotte-Pugh grade A;(2) no severe steatosis (≤30%) and active hepatitis;(3) no cholestasis;and (4) ICG retention rate at 15 min (ICGR15)<20% [27].ELRA is contraindicated in patients of liver dysfunction due to severe cirrhosis,portal hypertension,Budd-Chiari syndrome,anicteric or icteric cholestasis,secondary sclerosing cholangitis or,serious damage to intrahepatic biliary tree [4,12,39-42].Total serum bilirubin should be<twice of normal upper value.Patients with obstructive jaundice should have a biliary drainage aiming at decreasing blood bilirubin [9,32].
The preoperative evaluation is to ensure a sufficient RLV.The measurement of RLV mainly relies on computed tomography (CT)-based 3-D imaging which has applied routinely for more than 10 years.This technique has been evolved from empirical to the 3-D,real-time navigated anatomical hepatectomy [43].3-D reconstruction help surgeons understand the course and variation of each vessel in the liver as well as the adjacent relationship between the lesion and the surrounding vessels.Preoperative surgical planning requires calculating the scope of the hepatectomy and its implication on the RLV and to repeatedly simulate the surgical procedure in order to maximize the preserved liver volume.The advantages of the 3-D reconstruction technique have been valued by many surgical teams [44,45].For some huge tumors,residual 3-D reconstruction needs to be perfected further when large vascular structures are extensively invaded,and when the RLV/standard liver volume ratio is insufficient (<40%),RLV should also always be evaluated both quantitatively (liver mass) and qualitatively (liver function),before surgery to avoid small for size liver syndrome and to ensure maintenance of a postoperative liver function [46].Once all these investigations are done and critically analyzed,the most suitable resection plane has to be chosen aiming at avoiding major complications.
The introduction of the “precision liver surgery principle” has promoted the modularization,simplification,standardization and operational risk control of liver surgery [24].The advances on evaluation and surgery allow ELRA to gradually become a more wildly accepted procedure [24].
Technical issues
ELRA is one of the most technically demanding procedure,involving a series of complicated processes,such as hepatic blood flow interruption,total hepatectomy,extracorporeal venous bypass,extracorporeal organ perfusion and resection,and reconstruction of the involved major blood vessels and hilar ducts,reperfusion and re-implantation of a very modified liver remnant [24,47].All these elements require the “construction” of a surgical team including members all having experiences with both conventional liver resection and transplantation techniques.
Intraoperative ultrasound (IOUS) is used to further specify the relationship between the lesion(s) and the hepatic artery,portal,and hepatic veins,and IVC;and to exclude extrahepatic lesions.The procedure first needs a cholecystectomy,a dissection of the common bile duct,proper hepatic artery and portal vein,then,IVC,proper hepatic artery,and portal vein need to be clamped and the liver removeden blocwith the RHIVC.If the hepatic veins are found to be invaded,they need to be separated.The removed liver will be put in an ice bath and immediately perfused through the portal vein using cold UW-solution [4 8,4 9].The lesion is carefully dissected together with the invaded hilar portion and the corresponding vascular segments.Reconstructions of blood vessels or bile duct are performed as needed (Fig.1A).
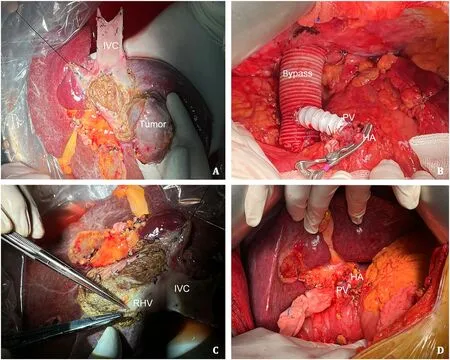
Fig.1. Ex vivo liver resection and auto-transplantation.A: The liver tumor is resected using bipolar coagulation;small short hepatic veins,hepatic arteries,and portal vein branches are suture-ligated;B: the IVC has been replaced with prosthesis and a temporary portacaval shunt has been constructed;C: ex vivo surgery with ex situ reconstruction of the blood vessels and bile ducts before re-implanting the liver;D: after anastomosing the portal vein,the portal blood flow is restored followed by rearterialisation.IVC: inferior vena cava;PV: portal vein;HA: hepatic artery;RHV: right hepatic vein.
Compared to liver transplantation,auto-transplantation is more complicated,including partial hepatectomy,repair and reconstruction of hepatic blood vessels and bile ducts,operation and anhepatic time are therefore evidently much longer.The management of the anhepatic phase is another key issue that determines whether the operation can proceed smoothly.Previously veno-venous bypass (VVB) was routinely used in ELRA to preserve hemodynamic stability during the anhepatic phase and to reduce pressure in the venous and visceral vascular systems [50,51].Unfortunately,VVB also has many disadvantages such as increasing operative and warm ischemia time,increasing complications such as pulmonary thromboembolism,vascular and neurological injuries,and post-reperfusion syndrome [52-54].In the early 1990s,temporary portacaval shunt (PCS) was added to avoid intestinal congestion,thereby improving intestinal edema and IRI [55].Some studies indeed showed that PCS reduces surgical and warm ischemic time,and liver injury,improves postoperative renal function,and finally,improves overall survival (OS) and graft survival [56,57].In a systematic review and meta-analysis,there were differences in patients undergoing VVB and temporary PCS.There was no statistical difference in intraoperative variables and complication rate,but compared to the VVB group,the 90-day mortality was significantly lower in the PCS group (23% vs.12%,P=0.03).It has been proposed that all patients should undergo routine temporary IVC reconstruction combined with temporary PCS surgery,ensuring hemodynamic stability,and reducing the incidence of postoperative infections due to bacterial translocation [37,58].We routinely perform a prosthetic vessel to connect the IVC cuffs above and below the liver to restore the systemic circulation,together with endto-side anastomosis of the portal vein with artificial IVC to avoid obstruction of mesentery and renal congestion (Fig.1B).After resection of the tumor,blood vessels and bile ducts are reconstructedex situ(Fig.1C).Normal saline is used to check the leakage of the blood vessels and bile duct.
Reconstruction of the hepatic venous outflow tract during ELRA is a technical difficulty.In contrast to LT,the venous reconstruction is limited by the patient’s own vascular conditions.Reconstruction of large blood vessels usually needs bridging veins to extend the venous outflow tract,to ensure the integrity of the reconstructed vascular bed and the permeability after re-implantation.To obtain a successful reconstruction,the relationship,the length,and the internal diameter of anastomosis between outflow tract and vena cava,should be well evaluated based on experiences gathered in vascular and transplantation surgery [8].To repair and reconstruct the defective vessel,autologous or allogeneic vessels can be used.Presently,commonly used autologous veins include portal,hepatic,great saphenous,umbilical,and iliac veins.Before the autologous re-implantation,it is necessary to ensure that the hepatic veins of future liver remnant (FLR) are widely open.Similar to the experiences in living donor liver transplantation (LDLT),congestion,stretching,or anastomotic stenosis of the hepatic vein orifice(s)should be avoided when reconstructing the outflow tract [24,59].If the defect of the IVC or hepatic vein behind the autologous liver is too large,this defect must be repaired using autologous or allogeneic vascular patches.Sometimes,autologous,allogeneic,or prosthetic vessels are needed to reconstruct,lengthen,or replace adequately the blood vessels.
The reconstructed hepatic vein and the artificial IVC are anastomosed.If the IVC is reconstructed,the artificial IVC needs to be removed,and the autologous reconstructed blood vessels anastomosed to IVC.Afterwards the procedure is the same as conventional LT (Fig.1D).
Compared to HAED,some important specific modifications are needed when apply ELRA to hepatobiliary malignancies (Table 2).

Table 2Key issues for successful ELRA in case of hepatobiliary malignancies.
Zhang et al.evaluated the role of hepatic vein stenting as a bridge therapy in improving hepatic venous outflow and thereby the FLR quality in patients with HAED presenting Budd-Chiari syndrome [60].They demonstrated that hepatic vein stenting increases hepatic vein outflow and improves long-term prognosis.
A newly designed technique of the cavo-portal hemitransposition is based on two anastomoses: an IVC-sparing hepatectomy and large latero-lateral cavo-caval,and end-toside cavo-portal anastomoses [61].This technique may also be applicable in ELRA.
Outcomes
In 2010,Wen et al.[25]first applied ELRA to treat end-stage HAED.Qiu et al.reported 228 patients treated with ELRA between 2014 and 2020 [14].The 5-year OS rate in the ELRA group was significantly higher than that in the non-ELRA group (82.1% vs.19.1%,P <0.001).The patients with a predicted 12-month mortality risk of>75% did significantly benefit from ELRA.
It is still controversial if patients with liver malignancies may benefit from ELRA.In a meta-analysis,Zawistowski et al.included 53 studies from four different databases,the R0 resection rate was 93.4%,the incidence of major surgical complications was 24.5%,the 30-day mortality rate was 9.5%,and the one-year survival rate was 78.4% [27].According to the data of a 244-patient cohort [27]the R0 resection rate was 98.6%,the 30-day mortality rate was 7.9%,and the one-year survival rate was 82.1%;the 30-day mortality rates of the patients presenting malignant and benign lesions were 11.3% and 6.3% (P=0.181),the one-year survival rates were 65.0% and 89.7% (P <0.001),and the incidence rates of major surgical complications were 50.0% and 21.0% (P <0.001),respectively.Regression analysis showed that the prognosis of patients with benign tumors was better.ELRA is very satisfactory in the radical resection of tumors in livers with a normal function.Although results of ELRA are still unsatisfactory in the treatment of malignant tumors,some reports indicate that this procedure can also be a valuable treatment for patients presenting unresectable liver and abdominal malignancies.Kato et al.retrospectively analyzed the outcome of 46 patients with various liver tumors including cancer (n=20),sarcoma (n=20),and benign to low grade tumors (n=6) who received ELRA during the period 2008-2019 [3].Their median follow-up was 3.1 years (range:12 days-11.5 years).Based on tumor location and vascular involvement,the ELRA surgeries consisted ofex situhepatectomy (n=18),ex situhepatectomy combined with bowel transplantation (n=12),ex situhepato-duodeno-pancreatectomy (n=8),andex situmultiple organ-surgery (n=7).R0-surgery was obtained in 91% of patients.The 1-,3-and 5-year survival rates of patients with benign to low grade tumors,sarcomas,and cancers are 100%/100%/100%,65%/60%/50%,and 65%/45%/40%,respectively.Weiner et al.[15]retrospectively analyzed the prognosis of 35 patients having ELRA.Their 1-,3-,and 5-year OS rates were 67%,39%,28%,respectively;with the median survival period of 710 days (range: 22-4824)and with a median follow-up of 1200 days (range: 210-4992).The 1-,3-,and 5-year OS rates of patients with low,moderate,and high invasive tumors were 100%/100%/100%,67%/40%/22%,and 61%/33%/23%,respectively,with a median survival of 1825,4 4 4,and 577 days.These suggest a more widespread use of ELRA in centers having LT experience.
Both Tomoaki Kato and Joshua Weiner and other researchers show that ELRA may indeed be an alternative treatment in well selected (low malignancy) patients [3,15,62,63].
Challenges and prospectives
ELRA,as a technical fusion of conventional hepatectomy and liver transplantation techniques,provides the opportunity of radical surgical resection for patients with liver tumors that are difficult to remove by conventionalin vivoresection methods due to their specific localization.The outcomes of this complex procedure are acceptable,particularly in case of benign or lower grade of malignancies [6,7,25,32-37].In addition,more precise extracorporeal resection of ELRA maximizes the preservation of the remaining liver volume and allows to raise the R0 resectability.Thein situvascular reconstructions,independent of ischemia time constraints [64],avoids prolonged and risky conventional hepatectomy.Moreover,ELRA represents an important means to over-
come liver allograft shortage and long waiting time on the transplant lists,as well as many complications and costs,linked to the chronic use of immunosuppressive drugs.Despite these advantages,ELRA still faces many challenges,such as the difficulties of appropriate venous reconstruction,the management of short-term and long-term complications,the better identification of indications,the evaluation of long-term outcome,and finally the more widespread application of this technique especially in cancer patients [3,4,14].The joined effort of involved disciplines (surgery,anesthesiology,oncology,hepatology,and intensive care) will further advance ELRA.The clinical improvement and long-term effects of ELRA still need further investigation [65].
Acknowledgments
None.
CRediT authorship contribution statement
Xin Yang:Writing -original draft.Lu Lu:Conceptualization.Wen-Wei Zhu:Data curation,Formal analysis.Yi-Feng Tao:Data curation,Formal analysis.Cong-Huan Shen:Investigation,Methodology.Jin-Hong Chen:Supervision,Validation.Zheng-Xin Wang:Resources,Software.Lun-Xiu Qin:Writing -review &editing.
Funding
None.
Ethical approval
Not needed.
Competing interest
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
 Hepatobiliary & Pancreatic Diseases International2024年2期
Hepatobiliary & Pancreatic Diseases International2024年2期
- Hepatobiliary & Pancreatic Diseases International的其它文章
- Editors
- Information for Readers
- Meetings and Courses
- Liver transplantation and liver resection as alternative treatments for primary hepatobiliary and secondary liver tumors: Competitors or allies?
- Laparoscopic anatomical liver resection of segment 7 using a sandwich approach to the right hepatic vein (with video)
- Severe liver injury and clinical characteristics of occupational exposure to 2-amino-5-chloro-N,3-dimethylbenzamide: A case series