
On implications of somatostatin in diabetic retinopathy
2024-01-10 10:13:34YanhongFangQionghuaWangYoujianLiLiZengJianLiuKepengOu
中國神經(jīng)再生研究(英文版) 2024年9期
Yanhong Fang, Qionghua Wang, Youjian Li, Li Zeng, Jian Liu, Kepeng Ou,*
Abstract Somatostatin, a naturally produced neuroprotective peptide, depresses excitatory neurotransmission and exerts anti-proliferative and anti-inflammatory effects on the retina.In this review, we summarize the progress of somatostatin treatment of diabetic retinopathy through analysis of relevant studies published from February 2019 to February 2023 extracted from the PubMed and Google Scholar databases.Insufficient neuroprotection, which occurs as a consequence of declined expression or dysregulation of retinal somatostatin in the very early stages of diabetic retinopathy, triggers retinal neurovascular unit impairment and microvascular damage.Somatostatin replacement is a promising treatment for retinal neurodegeneration in diabetic retinopathy.Numerous preclinical and clinical trials of somatostatin analog treatment for early diabetic retinopathy have been initiated.In one such trial (EUROCONDOR), topical administration of somatostatin was found to exert neuroprotective effects in patients with pre-existing retinal neurodysfunction, but had no impact on the onset of diabetic retinopathy.Overall, we concluded that somatostatin restoration may be especially beneficial for the growing population of patients with early-stage retinopathy.In order to achieve early prevention of diabetic retinopathy initiation, and thereby salvage visual function before the appearance of moderate non-proliferative diabetic retinopathy, several issues need to be addressed.These include the needs to: a) update and standardize the retinal screening scheme to incorporate the detection of early neurodegeneration, b) identify patient subgroups who would benefit from somatostatin analog supplementation, c) elucidate the interactions of somatostatin,particularly exogenously-delivered somatostatin analogs, with other retinal peptides in the context of hyperglycemia, and d) design safe, feasible, low cost, and effective administration routes.
Key Words: diabetes retinopathy; excitotoxicity; growth hormone; insulin like growth factor; irisin;neurodegeneration; neuroinflammation; neuroprotection; neurovascular unit; octreotide; oxidative stress; somatostatin
Introduction
With a multitude of variations linked to geographical, sociodemographic, and ethnic difference, diabetic retinopathy (DR) is not only the most frequent microvascular complication of diabetes mellitus type 1 (T1DM) and type 2(T2DM), it is also the most common retinal vascular disease (Mrugacz et al., 2021; Fung et al., 2022; Oshitari, 2022).Due to the worsening diabetes pandemic and population aging, the global number of adults with DR is predicted to increase by more than 55.6% from 2020 to 2045, according to a meta-analysis of 59 population-based studies around the world (Teo et al., 2021).Apart from genetic heritability and glycemic variability, prolonged high blood glucose levels, hypertension, metabolic dysregulation, chronic inflammation, blood-retinal barrier (BRB) disruption, and progressive retinal microvascular alterations all contribute to retinal damage (Forrester et al.,2020).Depending on the presence and severity of neovascularization, DR can be clinically classified into non-proliferative DR (NPDR; mild, moderate,or severe) and proliferative DR (PDR).The clinical manifestations of earlystage DR which can be detected by fundoscopy, include microaneurysms,hemorrhages, cotton wool spots, venous beading, and hard exudates, while neovascularization, fibrous tissue formation, vitreous hemorrhage, and tractional retinal detachment are features of the advanced stages of DR.In addition, macula swelling or thickening (diabetic macular edema, DMO) can occur when the leakage of hyperpermeable capillaries and microaneurysms compromise the BRB, which can occur independently from the proliferative progression of DR (Nian et al., 2021; Sun et al., 2021).
The underproduction of neuroprotective factors, including somatostatin (SST),substance P, pigment epithelium-derived factor, interstitial retinol-binding protein, and glucagon-like peptide 1, has been implicated in both PDR and DMO (Simó et al., 2002; Carrasco et al., 2007; Amato et al., 2018a; Ou et al.,2019; Mrugacz et al., 2021; Soni et al., 2021; Fragiotta et al., 2022).Among them, SST underproduction is one of the most important indicators of early stage DR.SST, also known as somatotropin release-inhibiting factor, growth hormone (GH) release-inhibiting hormone, and GH-inhibiting hormone, is a cyclic tetradecapeptide, belonging to the group of neuropeptides that modulate autocrine, endocrine, paracrine, and synaptic communication.At the time of its isolation, the name ‘somatostatin’ was coined to indicate‘stagnation of a body,’ which aptly encapsulates its diverse anti-secretory and anti-proliferation actions (Brazeau et al., 1973; Utiger, 2022).The inhibitory effects of SST are facilitated by its selective binding to specific SST receptor subtypes (SSTR1, 2A and B, 3, 4, and 5, of which the SSTR2A splicing product is exclusively found in humans), all members of the G-protein-coupled receptor family.SST suppresses the activity of adenylate cyclase via G-protein signaling,thereby decreasing the accumulation of cyclic adenosine monophosphate, an essential intracellular second messenger universally involved in metabolism and gene expression (Song et al., 2021).
In this review, we discuss the recent findings of studies on the implications of SST in DR and SST-based therapeutics, through the analysis of previous reviews that have comprehensively investigated the association between retinal diseases and neuroprotective peptides such as SST (Simó-Servat et al., 2018; Cervia et al., 2019; Pillar et al., 2020; Mrugacz et al., 2021), Our thoughts for future directions are also discussed.
Search Strategy
A literature search of the PubMed and Google Scholar databases allowed the retrieval of 81 relevant research papers and review articles published in English between February 2019 and February 28, 2023.In addition,nine articles published in 2018, and eight published earlier than 2018 were included based on their applicability.The main keywords used for the search included “somatostatin (and) diabetic retinopathy,” “retinal neurodegeneration,” “somatostatin and growth hormone/IGFs,” and“octreotide and retinopathy.” The article types, experimental subjects in the research papers, and their relevance to this review are summarized in Table 1.
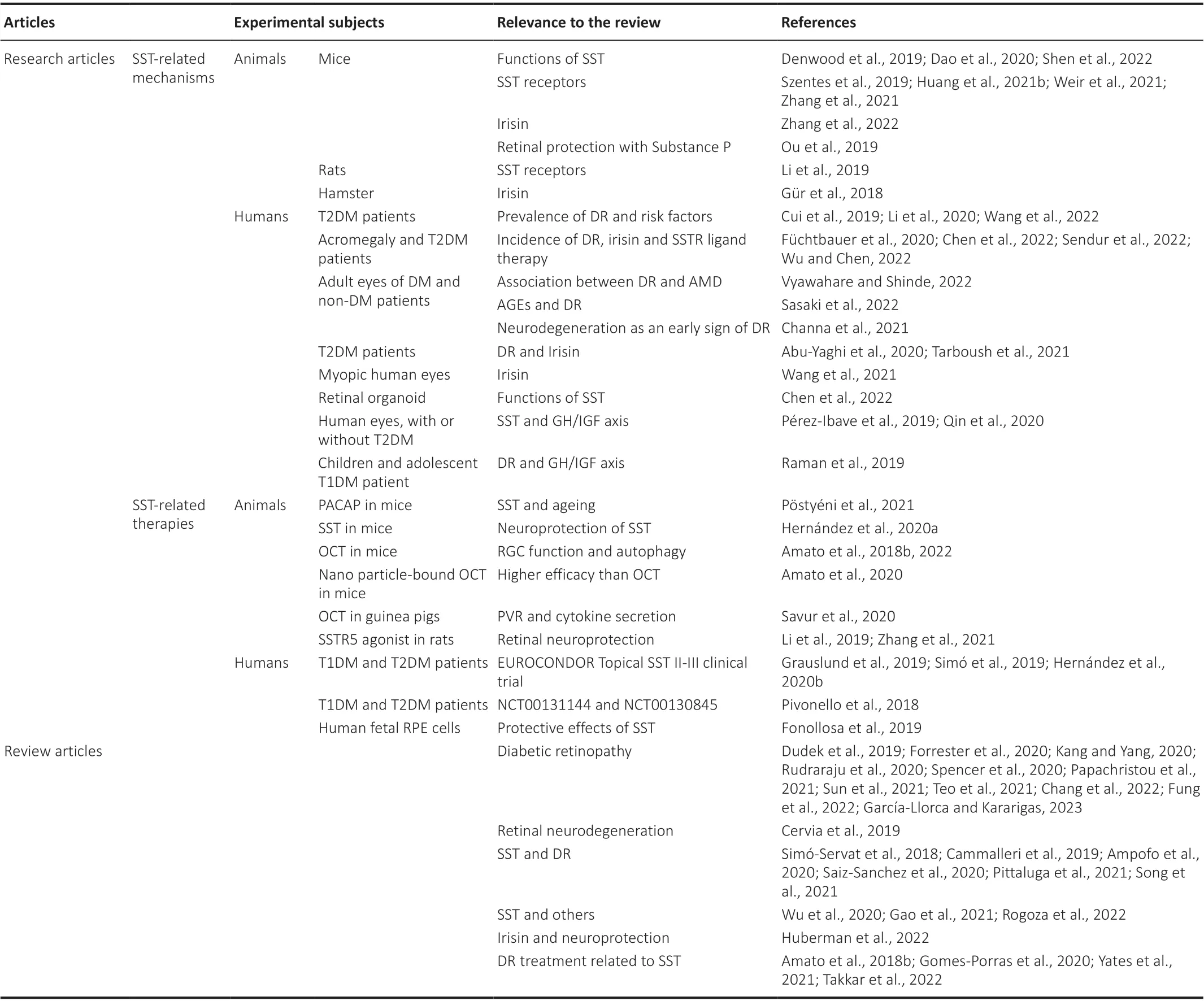
Table 1 | Articles from the literature discussed in the review, published between 2018 and February 2023
Re-Examination of Diabetic Retinopathy through the Lens of the Neurovascular Unit
Although DR primarily manifests as vasculature disorders, and is classically defined as a microcirculatory disease of the retina, blood vessels represent less than 5% of the retinal mass, and there is ample evidence to suggest that neurodegeneration may be the primary pathology that initiates the cascading and intertwining abnormities of metabolic dysregulation, oxidative damage,retinal ischemia, and neuroinflammation associated with DR (Carrasco et al.,2007; Mauricio et al., 2020; Pillar et al., 2020).Retinal neurodegeneration is defined as an increase in neuronal apoptosis in the retina due to inherited gene mutations in the retinal pigment epithelial (Botto et al., 2022), or as a consequence of an array of diseases encompassing glaucoma, age-related macular degeneration, retinitis pigmentosa, and diabetes mellitus (Nian et al., 2021; Maneu et al., 2022).Neural apoptosis and glial activation, both of which are hallmarks of retinal neurodegeneration, have been detected prior to the occurrence of microcirculatory changes in diabetic human donors(Hernández et al., 2013; Simó et al., 2022).Indeed, the morphological and functional deficits of retinal ganglion cells (RGCs), glial cell overactivation, and microglial activation occur as a very early response to the local and systemic metabolic challenges imposed by hyperglycemia (Rolev et al., 2021; Amato et al., 2022).
Some scholars consider diabetic retinal neurodegeneration (DRN) and diabetic retinal vasculopathy as two temporally-divided, but inter-related events of DR (Soni et al., 2021), while others have proposed an umbrella term for diabetic retinal disease to accommodate these two clinical components(Pillar et al., 2020).The structural stability and functionality of the retina are executed by retinal neurovascular units, formed by the interdependent elements of the retina, which include neurons (ganglion, bipolar, horizontal,and amacrine cells), supportive glia (microglia and two types of macroglia,including astrocytes and Müller cells), and vascular cells (endothelial cells(ECs) and pericytes).The loss of integrity of the retinal neurovascular unit may be the triggering event of DR damage (Eleftheriou et al., 2020; Nian et al., 2021).In the eye, specialized neurons and interneurons, including photoreceptors, bipolar cells, horizontal cells, amacrine cells, and RGCs, form the infrastructure of the information pathway to convert light photons into electrochemical signals that can be conveyed to the optic nerve in the brain for interpretation as visual images (Maneu et al., 2022).As part of the brain,the retina is the most metabolically demanding tissue in humans due to its high energy cost.The retinal neuronal network is extremely vulnerable to metabolic fluctuations resulting from unmatched energy supply in diabetic ischemia or hypoxia, and the corresponding production of subsequent cellular stressors (e.g., glucose and O2).
As new insights into the pathogenesis of DR are gained, and imaging modalities continue to advance, the need to update the DR grading system may incur a paradigm shift that underscores potential therapeutic advantage during the early windows before clinical diabetic retinal vasculopathy manifests.For example, a multi-dimensional DR severity scale incorporating assessments of early DRN, retinal neurovascular unit abnormalities, and systemic metabolism has been designed and shown to allow improved stratification of patients, allowing more tailored treatment (Sun et al., 2021).Early intervention would be made possible by quantitative measurements of DRN.Using the large population-based UK Biobank cohort of 74,422 adult individuals, the ganglion-inner plexiform layer was identified as a structural indicator for neuro-retina thickness, and an early predictor of DRN in patients with T1DM or T2DM.Changes in the thickness of the ganglioninner plexiform layer, but not the total retinal or macular retinal nerve fiber layer, were detected before the onset of DR, and were persistently associated with DR development and grade (Channa et al., 2021).Moreover, in addition to multifocal electroretinogram and special-domain optical coherence tomography, fundus-driven microperimetry has been suggested as a better clinical diagnostic approach to evaluate neurodysfunction (Simó et al., 2019;Oshitari, 2021).
The current mainstay treatment for DR only benefits patients with advanced DR.Across patients with moderate to severe NPDR, PDR, and DMO, the latter two pose a major threat to vision, while photocoagulation and anti-vascular endothelial growth factor (VEGF) therapy remain the first-line options to retain visual acuity (Mansour et al., 2020; Yates et al., 2021).However,optimization of general fitness, including systemic control of blood glucose and pressure, is the only countermeasure in the early stages of DR.Several novel therapeutic approaches currently under experimental or preclinical investigation focus on different aspects during DR progression, including neurodegeneration, gut-ocular flow, mitochondrial dysfunction, oxidative stress, inflammation, and lifestyle (Takkar et al., 2022).These factors often involve overlapping or converging mechanisms.The re-establishment of retinal homeostasis requires simultaneous modulation of multiple pathways at a reversible phase of retinopathy.To this end, neuroprotective peptides,including angiotensin, substance P (Ou et al., 2019), neuropeptide Y and SST(Cervia et al., 2019), may serve as good candidates to combat neuronal cell death in DRN.et al., 2019), which is inhibited by free fatty acids and other factors such as palmitate, but enhanced by other amino acids including arginine and leucine.Meanwhile, insulin-induced hypoglycemia and L-glutamate release can stimulate SST secretion to negatively regulate insulin levels, thereby preventing further declines in glucose levels.More than two-thirds of SST in the circulation is produced by gastrointestinal and pancreatic δ-cells, while the rest originates from the central nervous system (Ampofo et al., 2020).SST is released into the circulation through the portal venous system to exert its inhibitory effects on various endocrine effectors including GH, prolactin,thyrotropin, cholecystokinin, gastric inhibitory peptide, neurotensin, motilin,gastrin, secretin, glucagon, insulin, pancreatic polypeptide, and cytokines in immune cells (Ampofo et al., 2020; Rogoza et al., 2022).
The Primary Somatostatin-Involving Mechanisms in Diabetic Retinopathy
In addition to its role as a neuromodulator, functions of SST in the retina include inhibition of ischemic degeneration and inflammation, antiangiogenesis, and regulation of ion/water transport via voltage-gated ion channels (Hernández et al., 2014).From the mechanism network that initiates DR and the following disease progression, we focus on four main pathways which involve SST regulation, as depicted in the diagram in Figure 1: a) excitotoxicity; b) oxidative stress; c) neuroinflammation and abnormal angiogenesis, and d) decline of neuroprotective peptides (Maneu et al.,2022).
Somatostatin in a Nutshell
The two SST isoforms SST-14 and SST-28 are derived by post-translational cleavage of the same prohormone.Both isoforms bind to all SSTRs with a similar affinity.However, isoform SST-14 is predominantly produced in the brain by somatostatinergic neurons that are also GABAergic, and is distributed throughout the neocortex and the periventricular nucleus of the hypothalamus (Song et al., 2021).The spiking activity of SST neuron subtypes displays diverse discharge patterns, contingent on which cortical layers they reside in, suggesting a large repertoire of functions (Song et al., 2021).SST is packaged in dense core vesicles located at nerve endings or interneuronal networks, ready for exocytosis.When projected to the anterior pituitary gland, SST represses the secretion of GH by somatotroph cells by binding to SSTR2 and SSTR5 (Pittaluga et al., 2021).Once released into the synaptic cleft, in a Ca2+-dependent manner or via voltage-gated potassium channels,SST induces synaptic depression by modulating excitatory neurotransmission mediated by other neurotransmitters, such as glutamate and GABAB(Cammalleri et al., 2019; Shen et al., 2022).As an essential part of the regulatory reticulum for energy homeostasis, the secretion of SST is balanced by the stimulation of insulin-like growth factors (IGFs), as well as the feedback effects of high circulating GH levels (Ampofo et al., 2020).
The retina is the gateway to the brain and a part of the central nervous system.Retinal neurons form a highly structured neural circuitry, in which SST acts as an inhibitory neurotransmitter to control the synaptic information relayed from the eye to the brain, including vertical connections from photoreceptors to RGCs via bipolar cells, and the lateral modulation of the synaptic transmission by horizontal and amacrine cells (Cammalleri et al.,2019).The retinal pigment epithelium, amacrine cells, and RGCs are the main sources of SST secretion, and all five SSTRs are present in the retina(Carrasco et al., 2007; Li et al., 2019).SSTR1 and SSTR2 primarily exist in the outer retina, while SSTR4 is present in the inner retinal cell types,reflecting the site-specific heterogeneic role of SST in both the regulation of phototransduction, and the adaptation to the metabolic dynamics.The three-dimensional meshwork formed by interwoven varicose fibers of somatostatinergic interneurons and the wide distribution of different SSTR subtypes in the retina suggest a diffuse and diverse action of retinal SST that involves the activities of multiple signaling pathways (Cammalleri et al., 2019).SST (released by RGCs) is one of the neuropeptides dynamically expressed during retinal neurogenesis, which influences neurogenic progenitors and photoreceptor differentiation through binding to SSTR2 (Weir et al., 2021).By studying neurogenesis with three-dimensional retinal organoids, researchers found that SSTR2 is the dominant receptor for SST during retinal development in humans, and is the only SSTR expressed by photoreceptor precursors(Chen et al., 2022).SSTR2 mediates rod photoreceptor differentiation upon SST stimulation, while endogenous SST produced by RGC participates in the generation of photoreceptors, which involves transduction of various signaling pathways, including the protein kinase C/small heterodimer partner and phosphoinositide 3-kinase/ protein kinase B pathways (Chen et al., 2022).
Both SST isoforms can be found in peripheral tissues and in the circulation,but SST-28 is more abundant (Song et al., 2021).SST is secreted by delta cells(δ-cells) located at the pyloric antrum, duodenum, and pancreatic islets,where SST is a potent local inhibitor of the major glucoregulatory hormones insulin and glucagon, secreted by α- and β-cells, respectively.SST secretion and release are also promoted by insulin and glucagon.This hormone trio works together to govern glucose homeostasis, the essence of life (Gao et al., 2021).All five SSTR subtypes are expressed in the islets.With outreaching filopodia, δ-cells are characterized by neuron-like morphology and pan-islet scattering distribution, which together enable the tight coupling required to sense the capricious nutritional input signals to the metabolic regulation by SST.Elevated plasma glucose triggers glucose-induced SST secretion in both membrane potential-dependent or -independent manners (Denwood
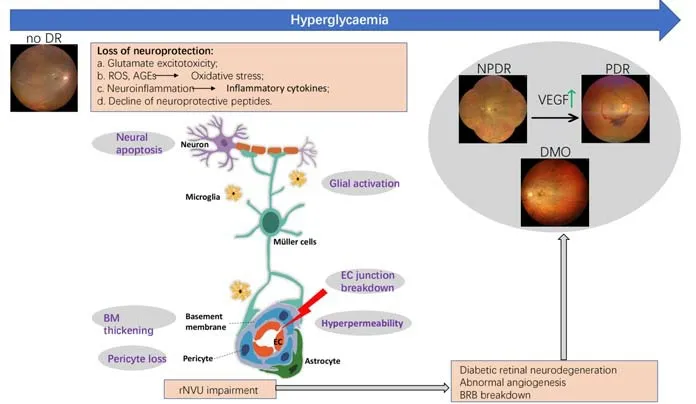
Figure 1 |A simplified diagram illustrating the SST-involving pathogenesis of DR.Impairment of retinal neurovascular units, promoted by chronic hyperglycemia and metabolic disorders in the diabetic milieu, may be the onset event of DR.Under a combined hit of declined neuroprotection by peptides such as SST, glutamate excitotoxicity, oxidative damage, neuroinflammation and altered GH/IGF signaling,and diabetic retinal neurodegeneration occurs, characterized by glial activation and neuron death.Pericyte loss, BM thickening, endothelial cell junction breakdown, and hyperpermeability of the microvasculature collectively contribute to the disruption of the BRB.The resultant fluid leaking into the retina and depositing under the macula are manifestations of DMO.Increased release of inflammatory cytokines and proangiogenic factors such as VEGF stimulates neovascularization to compensate for retinal blood vessel damage.These immature, fragile, and permeable new vessels cause severe complications such as vitreous hemorrhage or tractional retinal detachment, which are features of PDR.Created with CorelDRAW.AGE: Advanced glycation end products; BM:basement membrane; BRB: blood-retinal barrier; DMO: diabetic macular edema; DR:diabetic retinopathy; EC: endothelial cells; GH: growth hormone; IGF: insulin-like growth factor; NPDR: non-proliferative DR; PDR: proliferative DR; rNVU: retinal neurovascular unit; ROS: reactive oxygen species; SST: somatostatin; VEGF: vascular endothelial growth factor.
Glial overactivation and excitotoxicity
Glutamate is the most common excitatory neurotransmitter in the retina.Extracellular glutamate accumulates under hyperglycemic stress, and the subsequent overactivation of ionotropic glutamate receptors, N-methyl-D-aspartate, and α-amino-3-hydroxyl-5-methyl-4-isoxazole-propionate,induces excess Ca2+influx which causes apoptotic neuron death, particularly triggering the loss of RGCs, amacrine and Müller cells, and thinning of the retinal nerve fiber layer (Amato et al., 2018a).The conversion of glutamate into glutamine by the Müller cell-specific enzyme glutamine synthase is essential for extracellular glutamate clearance, which can be impaired under hyperglycemic stress.SST controls glutamate release by preventing Ca2+overload.Activation of the SSTR2 and SSTR5 receptors by synthetic agonists has been shown to reduce T-type Ca+currents through nitric oxide/cyclic guanosine monophosphate/protein kinase G signaling pathway in rat RGCs (Li et al., 2019).The SSTR ligand octreotide (OCT), a long-acting SST derivative which binds preferentially to SSTR2 and SSTR5, has been demonstrated to rescue RGC damage by decreasing excitotoxicity in a steptozotocin-induced hyperglycemia mouse model before overt RGC apoptosis commences (Amato et al., 2022).Intraperitoneal administration of the SSTR5 agonist L-817818 in experimental glaucoma rats could redeem the RGC loss induced by elevated intraocular pressure.This treatment inhibited RGC apoptosis, accumulation of reactive oxygen species (ROS), and malondialdehyde, and rescued the functions of the mitochondrial respiratory chain complex (Zhang et al., 2021).
Oxidative stress
Oxidative stress cont ributes to DR by disturbing both ends of the redox balance, i.e., exposure to oxidizing agents or excessive generation of free radicals such as ROS, and inadequate antioxidant defense mechanisms such as autophagy (Taurone et al., 2022).Sitting on the frontline of oxidative attack from ROS-producing light sources, the retina is also an organ with intrinsic hypermetabolic oxygen consumption.The outer photoreceptor segment membranes of the retina are rich in polyunsaturated fatty acids, which are prone to oxidative degradation and act as major sources of retinal damage through the production of lipid peroxidation products (Kang and Yang, 2020).Exposure to prolonged hyperglycemia leads to both mitochondria-derived ROS overproduction and impairments in ROS scavenging by suppression of antioxidant machinery.Excessive accumulation of ROS is involved in almost all aspects of retinal abnormalities associated with DR, including mitochondrial damage, inflammation, apoptosis, cellular senescence, and endothelial hyperpermeability (Kang and Yang, 2020).High glucose disrupts the biochemical pathways of glycolysis, the Krebs cycle, and oxidative phosphorylation to trigger the overproduction of glycolytic intermediates,which are shunted into pathways leading to the accumulation of reactive intermediate molecules such as 3-deoxyglucosone, a highly potent glycating agent (Yumnamcha et al., 2020).The excess production of pro-oxidant advanced glycation end products (AGEs) from non-enzymatic glycation by 3-deoxyglucosone subsequently activates advanced end glycation products-AGE receptors ubiquitously expressed in the retina.The AGE/receptor for advanced end glycation product activity and the downstream oxidative stressrelated pathways are strong indicators of DR development (Papachristou et al., 2021; Sasaki et al., 2022).The oxidation products of ROS also inhibit autophagy, the critical housekeeping bioprocess which eliminates damaged or harmful cellular components in response to various stress conditions.For example, re-activating autophagy by mechanistic inhibition of rapamycin complex 1 has been shown to delay DR progression (Chang et al., 2022).Inex vivomouse retinal explants exposed to high glucose, treatment with OCT increased neuron survival through inhibition of mammalian target of rapamycin activity, thereby re-equilibrating autophagy and apoptosis activities(Amato et al., 2018b).
Neuroinflammation and abnormal angiogenesis
The normal function of the retinal microvasculature is maintained by its two major constitutive components: perivascular pericytes and ECs.The physical connection between pericytes and ECs in the niche of the vascular basement membrane allows their intimate interaction and cooperation.Pericytes exert both anti-apoptotic and anti-proliferative effects on ECs via paracrine and juxtacrine communications, which are critical for microvascular resistance against stressors such as hyperglycemia (Spencer et al., 2020).Prolonged local and systemic subclinical inflammation provokes a polarization switch of microglia from the anti-inflammatory (M2, neuro-protective) to the proinflammatory (M1) phenotype, which triggers a deviation of the survivalapoptosis balance of retinal pericytes toward death (Yin et al., 2022; Kaur and Singh, 2023).In vitroexperiments have shown that LPS-treated murine microglial BV-2 cells exhibited lower proliferation, enhanced apoptosis, and higher expression of proinflammatory cytokines such as inducible nitric oxide synthase, tumor necrosis factor-α, interleukin (IL)-1β, IL-4, IL-6, IL-10, and IL-13, which could be prevented by pre-treatment of the cells with SST.The associated mechanisms included a direct and rapid activation of p38α mitogen-activated protein kinase phosphorylation (Hernández et al.,2020a; Tang et al., 2023).Moreover, a hyperglycemia-induced decrease of platelet-derived growth factor B (PDGF-B)/beta-type platelet-derived growth factor receptor signaling of glial cells also contributes to the disappearance of capillary pericytes.However, whether SST is involved in the PDGF-B pathway in the eye remains unclear, although one study on rat hepatic stellate cells did find that OCT enhanced PDGF-induced hepatic stellate cell proliferation (Klironomos et al., 2014).In a guinea pig model of dispaseinduced proliferative vitreoretinopathy, intravitreal administration of OCT demonstrated both anti-proliferation and anti-inflammation effects.The retinal levels of the cytokines TNF-a, IL-1, IL-6, and PDGF, which participate in cellular modulation in the context of retinal inflammation, were found to be significantly downregulated (Savur et al., 2020).
Other consequences of pericyte damage include endothelial proliferation,excess synthesis of basement membrane components, and BRB breakdown(Spencer et al., 2020).The high metabolic rate in the retina renders it vulnerable to an undersupply of oxygen in the diabetic milieu.Complex adaptive metabolic reprogramming is initiated in response to hypoxic ischemic conditions, and may include the switch from mitochondrial oxidative phosphorylation to anaerobic glycolysis and upregulation of VEGF, ultimately resulting in VEGF-induced vessel leakage and loss of BRB integrity (Rudraraju et al., 2020).Pre-treatment of fetal human retinal pigment epithelium with SST was shown to protect the cells from VEGF- and hypoxia-induced hyperpermeability, by promoting the recovery of occludin and zonula occludens-1, which are the key integral tight junction proteins that provide the structural stability of both inner and outer BRB (Fonollosa et al., 2019).
Decline of neuroprotective peptides such as SST
In the study of human diabetic post-mortem eyes without microvascular abnormalities, the level of SST production was found to be inversely associated with the degree of retinal neurodegeneration, indicated by glial activation and neuronal death (Carrasco et al., 2007).SST depletion identified in the early stages of DR suggests a major contribution to DRN (Soni et al.,2021), although a definitive conclusion about whether the downregulation of SST is causal or consequential to retinal neurodegeneration is currently lacking.Many degenerative and ischemic complications of diabetes, such as DR and myocardial ischemia, converge with the physiological changes during chronological aging.In addition to DR, the neuroprotective role of SST has been evidenced in many age-related memory and cognition dysfunctions, neuropsychiatric disorders, and metabolic disorders (Song et al., 2021).The association between SST and early neuropathological changes has also previously been emphasized (Saiz-Sanchez et al., 2020).Age itself,accompanied by systemic metabolic drifting, is an independent risk factor for T2DM and DR (Li et al., 2020).Many common symptoms are evident in DR and age-related retinal diseases, including age-related macular degeneration,and patients with DR showed a four-fold increase of age-related macular degeneration risk than those without (Vyawahare and Shinde, 2022).Early onset of T2DM may accelerate retinal aging, thereby increasing the prevalence of DR and DMO (Wang et al., 2022).In the human thymus, an inverse relationship between aging and the number of binding sites for SST to its three receptors, SSTR1, SSTR2, and SSTR3, has been reported, which may contribute to the age-related thymus involution and altered cellular immunity (Ferone et al., 2000).A significant reduction of hypothalamic SST neurons in the periventricular nuclei was also found in diabetic BBZ/WpR rats and db/db mice (Huang et al., 2021a).Loss of endogenous hypothalamic somatostatinergic neurons leads to systemic hypothalamic inflammation and sympathetic nerve hyperactivity, which can precede or even drive systemic immunity and peripheral metabolic dysregulations in diabetes, as well as instigate the positive feedback loops that aggravate immune infiltration in the hypothalamus.Eliminating SST neurons by stereotactic injection of a floxed diphtheria toxin into the mouse hypothalamus induced persistent hypothalamus inflammation and a panel of metabolic and inflammatory alterations mimicking diabetic or pre-diabetic symptoms, without the development of disrupted glucose homeostasis (Huang et al., 2021a).Preventing the inhibition of the hypothalamic SST could directly hyperactivate the sympathetic nerve in richly innervated tissues including mesenteric adipose, bone marrow, and retina.As a result, treated mice exhibited a reduction in catecholamine-induced lipolysis in mesenteric adipose,expanded myeloid lineage hematopoiesis in bone marrow, and the earliest signs of DR characteristics such as higher level of monocyte infiltration in the retina, reduced special acuity and scrambled timing of oscillatory potentials on electroretinogram (Huang et al., 2021a).In addition to the hypothalamic decline of SST expression during aging, the density of SST-ergic amacrine cells in the retina was also found to be downregulated in aged transgenic mice,but could be restored by intravitreal injection of pituitary adenylate cyclaseactivation polypeptide, a fellow neuropeptide enhancing SST activity (P?styéni et al., 2021).
In addition, new data have shed light on the seemingly obsolete mechanism involving GF/IGF-1 signaling.Despite the established angiogenic effects of GH/IGF-1, the association between GH/IGF-1 production and DR remains unclear.Retinal expression of both GH and its receptors have been identified(Pérez-Ibave et al., 2019), while GH-releasing hormone and GH, but not IGF-1, was detected in the vitreous and aqueous humor of the eyes of T2DM patients with PDR.The intensive expression of GH-releasing hormone and its receptor in polymorphonuclear leukocytes, vascular ECs, and fibrocytes in FVM isolated from PDR patients suggested the participation of GH-releasing hormone/GH-releasing hormone receptor signaling in fibrinous inflammation and FVM formation in DR (Qin et al., 2020).Overexpression of GH selectively caused inner retinal damage in transgenic mice, while both neuroprotective and neuroregenerative effects of GH were identified in chick retinal cells(Cervia et al., 2019).Acromegaly patients with excessive GH/IGF-1 activity have a high risk of diabetes and an increased number of vascular branching points in the retina, but not a higher prevalence of DR (Füchtbauer et al.,2020).Elevated GH/IGF-1 signaling may be associated with a more severe form of DR, as high PDR prevalence was identified, but no link with NPDR was reported in patients with acromegaly (Wu and Chen, 2018).What role SST plays in aberrant GH/IGF-1 signaling and whether the angio-proliferative action of IGF-1 is opposed by exogenous SST remains unknown.Experimental attempts targeting IGF-1 at the systemic or local level did not yield therapeutic benefits to delay DR progression, and the neuroprotective role of SST was deemed to be unrelated to IGF-1 (Simó-Servat et al., 2018).However, in other studies, subcutaneous infusion of the SST analog SMS 201–995 or OCT was beneficial in arresting DR progression via inhibition of GH secretion in T1DM patients (Mallet et al., 1992; Gomes-Porras et al., 2020).This may indicate that in certain subgroups of DR patients, systemic SST treatment may exert a therapeutic benefit through regulation of the GH/IGF-1 axis.This previously ignored population-specific variance may explain some between-study discrepancies.Hormonal changes during puberty, particularly IGF-1 levels,have been associated with the incidence rate of DR in T1DM prepubescent or adolescent children.An inverse relationship between serum IGF-1 levels and DR severity was also found in pubescent T1DM patients, according to a cross-sectional study (Raman et al., 2019).A high level of GH/IGF-1 has also been indicated to accelerate DR progression from NPDR to PDR, as observed in patients with comorbid T1DM and acromegaly, in comparison to diabetic patients with a similar level of glycated hemoglobin and glucose control (Wu and Chen, 2022).
Tangible Somatostatin Replacement for Early Diabetic Retinopathy
The current diagnosis and staging of DR is based on the presence of microangiopathies of the retina, as detected by ophthalmic fundus examination, including the formation of microaneurysms, venous beading,intraretinal hemorrhages, and cotton wool spots for NPDR, and PDR characteristics of extensive ischemia, neovascularization of the disk or elsewhere, and tractional retinal detachment (Nian et al., 2021).Approved therapies targeting these lesions, including laser photocoagulation, intravitreal injection of corticosteroids and anti-VEGF agents, and vitreoretinal surgery,are usually expensive, invasive, technically demanding, and carry the risk of various side effects.Meanwhile, consequences of retinal neurodegeneration,such as inner retinal thinning, delayed dark adaptation, decreased contrast sensitivity, and visual field deficit, not only greatly blunt patients’ functioning and well-being, but are also identifiable early signs which could facilitate DR prevention (Sachdeva, 2021; Fragiotta et al., 2022).
The therapeutic value of synthetic SST analogs (SSAs), exemplified by OCT,which exhibits a much-extended half-life compared to native SST, has been intensively investigated as a treatment for a panel of diseases involving endocrine dysfunction or neurodegeneration, including acromegaly, digestive diseases, endocrine tumors, and solid tumors in breast and prostate, etc.Excellent tolerability of the drug in DR patients was confirmed by a safety assessment of long-acting OCT treatment, through pooling two randomized,double-blind, and placebo-controlled clinical trials, NCT00131144 and NCT00130845.This study showed that, except for a transient slight elevation of liver transaminase, long-term administration of OCT (median duration of exposure > 3.5 years) was not associated with increased risk of cardiac,hepatic, or renal damage.In addition, the treatment seemed to improve cardiac ischemia and peripheral neuropathy (Pivonello et al., 2018).
Intravitreal injection of SSAs, combined with other conventional treatments such as laser photocoagulation, has been applied in patients with PDR and DMO (Gomes-Porras et al., 2020).Despite convincing evidence indicating the therapeutic potential of SST or OCT for the treatment of DR, identification of an administration modality to achieve the desired drug efficacy remains an obstacle for clinical translation.Furthermore, adverse side effects can occur during long-term systemic administration of OCT or SST due to their versatile functions in neuroendocrine regulation, and the access of the drug to the retina is largely limited by the BRB that remains intact in the very early stages of DR.Local delivery by intravitreal injection is too invasive to treat patients without evident DR, while frequent intraocular injection carries too high of a risk of severe injury.Therefore, the topical use of SSA eye drops has attracted significant attention (Simó-Servat et al., 2018).In a db/db mouse model,administration of SST-14 eye drops directly onto the superior corneal surface,twice daily for 15 days, ameliorated Müller glial and microglial activation,as indicated by improvements in glial fibrillar acidic protein score and Iba-1 immunofluorescence staining, respectively (Hernández et al., 2020a).Similar treatment of steptozotocin-induced diabetic rats with SST eye drops prevented apoptosis in all retinal layers, EGR abnormalities, and glutamate accumulation by replenishing glutamate transporter (Hernández et al.,2013).A phase II-III randomized-controlled clinical trial from EUROCONDOR(European Consortium for the Early Treatment of Diabetic Retinopathy)was conducted to assess the efficacy of topical administration of SST or brimonidine, a selective α2-receptor agonist, for DR prevention or early treatment in T2DM patients.During this study, more than 400 patients were enrolled, and eye drops of the drug or placebo were administered twice daily in one eye.Although no prevention of the development of neurodegeneration was observed, the treatment was effective at arresting the ongoing neurodegenerative progress and halting the implicit time worsening in the subset of patients with pre-existing retinal neurodysfunction, as indicated by multifocal electroretinogram implicit time (Simó et al., 2019).Meanwhile,both SST and brimonidine induced significant dilation of retinal arteriolar and venular vascular caliber in patients with pre-existing mild DR (Grauslund et al., 2019).Under the pressure of the hypoxic microenvironment in diabetes mellitus, vasodilation may be an adaptive response to augment blood flow to meet the high metabolic demand of the retina.This observation may indicate a beneficial effect of the drug in improving the insufficient vasodilation resulting from neurovascular unit damage in early DR.
Nevertheless, the multi-layer permeation barriers between the administration site to the inner retina microenvironment, as well as the stresses in the eye evoked by long-term topical treatment, still restrict its usage.Novel biocompatible and non-antigenic polymeric nanoparticles, such as magnetic nanoparticles, have been tested as drug carriers to treat retinal diseases such as DR, with their pros and cons being analyzed elsewhere (Amato et al., 2018a).Prior research has shown that while the bioactivity of OCT is not affected by binding to functionalized magnetic nanoparticles, magnetic nanoparticle-bound OCT demonstrated improved drug stability, sustained post-injection release, and extended efficacy in inhibition of VEGF-induced human retinal EC proliferation, oxidative stress-induced apoptosis in mouse retinal explants (Amato et al., 2020).
Beyond DR, pathological secretion of SST has been identified in both neuroendocrine tumors and solid organ tumors, including melanoma, prostate cancer, and gastrointestinal cancers.SSAs targeting SSTR2 overexpression,including OCT, lanreotide, and pasireotide, have been successfully used as first-line treatment for neuroendocrine tumors, neuroendocrine neoplasms,and meningioma (Wu et al., 2020; Harrow et al., 2022).SSA therapy has also been shown to suppress tumor growth and immune modulation through the inhibition of certain hormones associated with tumorigenesis, such as insulin for insulinoma and thyrotropin for pituitary adenoma (Fani et al.,2022).SST receptor ligands, OCT and lanreotide autogel, are also mainstays of acromegaly treatment.
The Way Forward
The existing research has extensively established that SST replacement therapy cannot be applied in all patients with T1DM or T2DM, which raises the question as to who this treatment should be targeted towards.Biomarkers or clinical indications need to be identified to filter patient subsets who would benefit from treatment with neuroprotective agents such as SST.In the EUROCONDOR study, serum N-epsilon-carboxy methyl lysine, the most abundant AGE in circulation, was suggested not only as a biomarker for changes in implicit time and retinal thickness in early DR, but also as an indicator to monitor the effectiveness of DR treatment with SSAs (Hernández et al., 2020b).The importance of the central or peripheral regulation of neuropeptides on the sex-specific response to T2DM has spurred consideration of gender-specific therapeutics, a heavily under-researched area (Dudek et al., 2019).Whether sexual dimorphism is a factor in the levels of retinal SST and SSTR under physiological conditions or hyperglycemic stress currently remains unclear.Although lower retinal expression of immunoreactive SST in male rats compared to females was reported in a prior study (Peinado et al.,1990), and sex-dependent differences in behavior modulation of SST neurons have been documented (Szentes et al., 2019; Dao et al., 2020; Jefferson et al., 2020; Suresh Nair et al., 2022), whether or not gender is an independent risk factor for DR remains controversial.Some studies previously identified a higher prevalence and risk of DR in male adults than females, while women were found to be more likely to suffer a proliferative form of DR; however,other studies have reported that these differences were either insignificant or opposite (Cui et al., 2019; Li et al., 2020).Recent data have indicated that sex differences may play a fundamental role in the disease progression and treatment responses of metabolic syndrome-related diseases such as DR.Disrupted metabolism, pro-inflammatory cytokine secretion, and ROS production are all associated with sex-biased impairment of gut microbiota composition (García-Llorca and Kararigas, 2023).
Another important question to consider is how peptides with seemingly similar protective effects interact or override each other.Unfortunately,nothing is currently known about this topic.Current SST-based approaches are limited by the ignorance of potential antagonism or competition between different neuroprotective peptides.Combination therapies acting on multiple pathways of neuroprotection have been discussed in the treatment of DR, due to the possible benefits of synergistic effects, lower doses of a single drug, and hence reduced side effects or drug resistance (Maneu et al., 2022).Parallel to the retinal neuroprotection by SST, our previous work uncovered that Substance P, a constitutive neurotransmitter of amacrine and ganglion cells,inhibited N-methyl-D-aspartate-mediated RGC apoptosis and VEGF-induced vascular hyperpermeability in mice (Ou et al., 2019).Another example is irisin, known as an anti-diabetes hormone.Although originally discovered as a myokine produced by skeletal muscles, irisin immunoreactivity was identified in the pineal and neural retina of crested porcupines (Gen?er Tarak?? et al., 2016), most retinal layers of dwarf hamsters (Gür et al., 2018), and the aqueous humor of eyes from high myopic patients (Wang et al., 2021).Irisin is believed to exert a neuroprotective effect in the brain by regulating cerebral metabolism and inflammation (Huberman et al., 2022).However, how irisin influences GH synthesis and secretion in humans is not clear, although some new evidence in DR development raises an interesting question regarding whether SST inhibits the function of irisin, or there is a competing role between them.Functional antagonism between irisin and SSAR2/5 activation by administration of pasireotide, an approved SSA treatment for acromegaly,was previously reported (NATALICCHIO et al., 2020).In addition, irisin was found to be strongly correlated with DR initiation and stage.Recent studies in T2DM patients and mice with oxygen-induced retinopathy suggested that reduced circulating or vitreous irisin concentrations and elevated serum VEGF levels could be an indicator of early DR.Administration of irisin mitigated retinal neovascularization by suppressing VEGF expression and inflammation in mouse retinae (Abu-Yaghi et al., 2020; Tarboush et al., 2021; Zhang et al.,2022).Furthermore, in a cohort of patients with acromegaly, SSTR ligand therapy was found to be the only independent factor correlated with reduced serum irisin levels (Sendur et al., 2022).
Conclusion
DRN at the levels of neurovascular units precedes clinically manifest microangiopathy during DR initiation and development.The neuropeptide SST protects the retina from the metabolic pressure imposed by hyperglycemia by inhibiting excitatory neurotransmission and neuronal apoptosis, redressing autophagy, and suppressing neuroinflammation.The restoration of retinal structure and function is only possible if non-invasive interventions are adopted at the early stages, or even before vasculopathy manifests, when the local system still retains its resilience and plasticity.To improve the therapeutic potential of SST, it may be necessary to stratify target patients and to establish a better understanding of its crosstalk with other peptides in the context of diabetes mellitus.We regret that the depth and breadth of this review were constrained by the article volume and the need for focus.Unfortunately, the orchestrating neuroprotective action played by multiple molecules such as SST,which may direct DR research and treatment into a new paradigm highlighting neuroprotection, could not be sufficiently scrutinized.
Acknowledgments:The authors are grateful to Mr.Dou-Dou Liu (University of Oxford), a native English speaker, for the help in language editing.
Author contributions:All authors made a significant contribution to the work,whether that is the conception, literature search, drafting, or critical reviewing of the article.All authors gave final approval of the version to be submitted and published and agree to be accountable for all aspects of the manuscript.Conflicts of interest:The authors declare no conflict of interest.
Data availability statement:Not applicable.
Open access statement:This is an open access journal, and articles are distributed under the terms of the Creative Commons AttributionNonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.

- 中國神經(jīng)再生研究(英文版)的其它文章
- Does MgSO4 protect the preterm brain? Dissecting its role in the pathophysiology of hypoxic ischemic encephalopathy
- Exosomes derived from microglia overexpressing miR-124-3p alleviate neuronal endoplasmic reticulum stress damage after repetitive mild traumatic brain injury
- Rebuilding insight into the pathophysiology of Alzheimer’s disease through new blood-brain barrier models
- The functions of exosomes targeting astrocytes and astrocyte-derived exosomes targeting other cell types
- Post-transcriptional mechanisms controlling neurogenesis and direct neuronal reprogramming
- Hypothalamic circuits and aging: keeping the circadian clock updated