
Enhanced recovery nursing and mental health education on postoperative recovery and mental health of laparoscopic liver resection
2023-10-21 01:02:20DongXiaLiWeiYeYiLuYangLeiZhangXiangJunQianPingHuaJiang
Dong-Xia Li, Wei Ye, Yi-Lu Yang, Lei Zhang, Xiang-Jun Qian, Ping-Hua Jiang
Abstract
Key Words: Accelerated surgical rehabilitation; Mental health education; Laparoscopy; Liver metastasis of colorectal cancer;Gastrointestinal function; Mental health
INTRODUCTION
Colorectal cancer is a common gastrointestinal malignant tumor, and the morbidity and mortality of this disease are high.However, the early symptoms are not obvious. When patients gradually develop obvious symptoms such as hematochezia and diarrhea, they are usually in the advanced stage. With the continuous proliferation and differentiation of tumor cells, most patients will have tumor cell metastasis[1]. The liver is the most common organ of distant metastasis in colorectal cancer. Approximately 53% of colon cancer patients will have liver metastasis[2]. Laparoscopic tumor resection is a common surgical treatment method for liver metastasis of colorectal cancer in clinical practice, which reduces the tumor burden of patients by removing liver metastases and has the advantages of a small wound, less bleeding, and quick recovery[3]. However, surgical treatment cannot completely control the disease. Patients will also need to accept chemotherapy and other rehabilitation maintenance, and there is still a risk of postoperative recurrence.Therefore, patients will have negative emotions such as fear and anxiety. The surgical method is in the abdomen of the patient, so it will affect the digestive function after surgery. And therefore, early nursing and psychological intervention are necessary[4,5]. Accelerated rehabilitation surgical nursing is a new nursing concept and rehabilitation model. Based on medical evidence, perioperative intervention is performed to reduce the physiological and psychological traumatic stress of patients and achieve rapid rehabilitation[6,7]. This study analyzed the effect of accelerated rehabilitation surgical nursing combined with mental health education on postoperative recovery and mental health of patients undergoing laparoscopic resection of colorectal cancer liver metastases.
MATERIALS AND METHODS
Data and methods
General information: From March 2021 to March 2023, 120 patients who underwent laparoscopic resection of liver metastases from colorectal cancer in our hospital were selected as subjects. Among them, patients admitted from March 1,2021 to February 28, 2022 were set as the control group, and routine nursing combined with mental health education intervention was given. The group consisted of 30 men and 27 women, aged 31-78 years, with an average age of (62.25 ±9.74) years. In addition, patients admitted from March 1, 2022 to March 31, 2023 were set as the observation group and given accelerated rehabilitation surgical nursing combined with mental health education intervention. This group included 35 men and 28 women, aged 28-80 years, with an average age of (63.26 ± 10.14) years. The general data of the two groups were similar (P> 0.05). See Table 1.
Inclusion and exclusion criteria: Inclusion criteria: (1) Colorectal cancer in line with the 'colorectal cancer diagnosis and treatment norms'[8] standards and underwent radical surgery; postoperative pathology confirmed; (2) Age 18 ≤ 80 years;(3) Abdominal computed tomography or magnetic resonance imaging confirmed liver metastasis, in line with surgical indications; and (4) Complete clinical data.
Exclusion criteria[9]: (1) Laparotomy or conversion to laparotomy; (2) Palliative excision; (3) With colorectal obstruction or perforation; (4) Combination with other serious diseases; and (5) Have comprehension or hearing impairment.
Methods
Mental health education intervention methods: The patients were administered psychological evaluation and intervention according to their existing situation. The goals were to perform mental health education for patients, to encourage patients to express their negative emotions, to take corresponding measures to alleviate them, and to monitor patients' psychological status and emotions in real time.
Routine nursing intervention methods: The patients were given routine preoperative education, routine postoperative treatment according to the doctor's advice, and recommendations of postoperative precautions.
Accelerated rehabilitation surgical nursing methods: (1) Health education and psychological counseling: The nurses were trained on the specific properties of the disease, surgery, and mental health; the patients were then introduced to the disease characteristics and surgical methods in a specific manner, using video, brochures or slides to reduce fear of the disease and surgery. The nurses guided patients in discussions surrounding psychological challenges, encouraged them to vent negative emotions, listened patiently and gave guidance, and established patient confidence in overcoming the disease; (2) Analgesia: Teaching patients to correctly express pain signals to help medical staff to quickly and accurately judge pain symptoms, and inform patients of the rationality of postoperative pain and the importance of reflecting the condition. Nurses guided patients in the use of a self-controlled intravenous analgesia pump, and if necessary,administered oral antipyretic analgesics to enhance the analgesic effect; (3) Diet: After surgery, patients were still not allowed water but if thirsty could dampen their lips with a wet cotton swab. After 6 h, moderate water consumption was allowed, and after 12 h rice soup could be consumed. On the second postoperative day, a number of small semi-liquid meals could be eaten throughout the day. After 3 d of the liquid diet, the principle of consuming numerous small meals throughout the day was continued, while gradually increasing the amount of food, until the patient could return to their normal diet. Patients were advised to eat easily digestible, protein-rich foods that were rich in cellulose, and to avoid spicy foods; (4) Rehabilitation exercise: Nurses informed patients of the necessity of postoperative rehabilitation exercise and strived for the active cooperation of patients and their families. In the early postoperative stage, a semi-reclining position could be assumed, and the patient could be turned onto their back or front every hour. From the third day after surgery, the patients were guided in performing bed exercises such as hip lifting and kicking, which continued daily until they were allowed to get out of bed; and (5) Acupoint massage: Hegu, Zusanli, Weizhong, and other acupoints were massaged to relieve pain, and abdominal massage was performed to promote gastrointestinal motility.
Observation indicators and detection methods
The differences in postoperative recovery-related indices, complications and pain degrees, and mental health-related scores were compared between groups. The T lymphocyte subset levels of the two groups were examined.
Detection method: Fasting fresh blood samples were collected from patients in the morning, using an automatic blood biochemical detector, at a speed of 5500 r/min, centrifugal radius of 10 cm, for a centrifugal processing time of 20 min,allowing separation of serum into the detector, and detection of T lymphocyte subsets.
Degrees of pain: The visual analogue scale score was used to evaluate pain at different time points after surgery[10].Pain was scored out of 10, where 0 was no discomfort, and 10 was the most severe pain; the score was positively correlated with the degree of pain.
Mental health: The self-rating depression scale (SDS)[11] and self-rating anxiety scale (SAS)[12] that were used to evaluate the mental health of patients included 20 items, and the critical values were 53 and 50 respectively; the higher the score, the worse the mental health of patients.
Medical coping style (MCMQ) score[13]: A total of 20 items, covering the face (8 items), avoidance (7 items), and yield(5 items). For each of these three aspects, a single item was given a score of 1-4 points; the higher the score, the greater the patient was adopting the coping style.
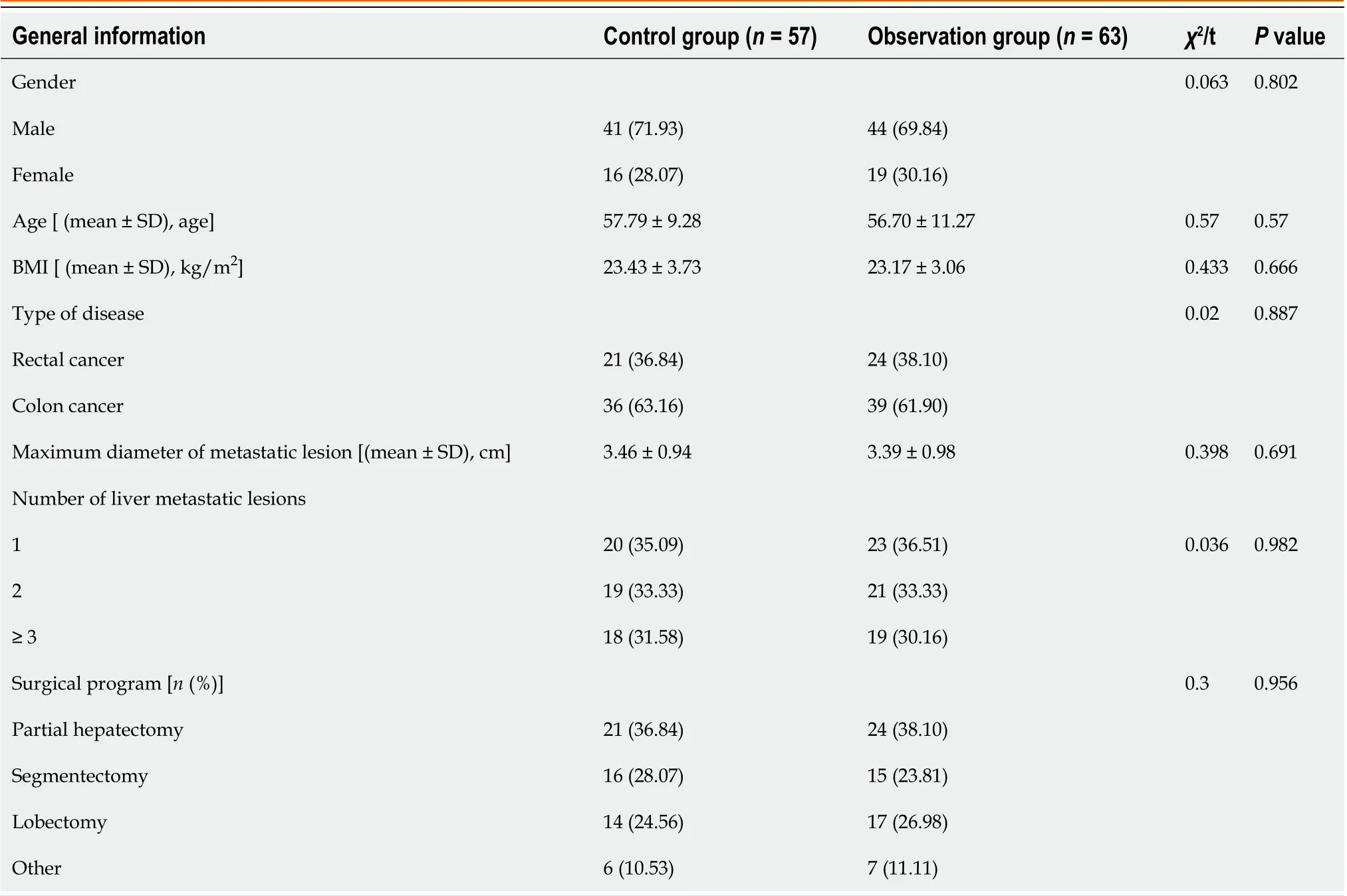
Table 1 Comparison of general data of two groups, n (%)
Cancer patients living function index scale (FLIC) score[14]: This consisted of a total of 22 items covering physical condition, psychological state, cancer-related difficulties, social well-being, and nausea. For each of these 5 aspects, a single item was given a score of 1-7 points; the higher the score, the better the quality of life.
Nursing satisfaction: The self-made satisfaction score table of the department was used to evaluate the 0-10 points with the patient when the treatment was completed, 0-4 points were dissatisfied, 5-8 points were satisfied, and 9-10 points were very satisfied.
Statistical processing
SPSS 26.0 software was used to process the data. FLIC score, MCMQ score, and other measurement data that conformed to normal or approximate distribution were described by (`c ± s), and a t-test was used for comparison. Countable data such as those for the surgical plan and number of liver metastases were described by the number of patients (%), and aχ2test was used for comparison.
RESULTS
Comparison of postoperative recovery between two groups
The postoperative exhaust, drainage, defecation and eating time in the observation group were shorter than those in the control group (P< 0.05). See Table 2.
Comparison of T lymphocyte subsets between two groups
T lymphocyte subsets were similar between the two groups (P> 0.05). At 3 d after operation, CD4+ in the two groups and CD3+ and CD4+/CD8+ in the control group were lower than before, while CD8+ in the control group was higher than before, and CD3+, CD8+ and CD4+/CD8+ in the observation group were similar with those before operation (P> 0.05).CD4+/CD8+ in the observation group was higher than that in the control group at 3 d after operation, and CD3+, CD4+and CD8+ were compared with the control group (P> 0.05). See Table 3.
Comparison of pain degree between two groups
The pain scores of the observation group were lower than those of the control group at 6 h, 12 h, 24 h, 48 h and 72 h after operation (P< 0.05). See Figure 1.

Table 2 Comparison of postoperative recovery between two groups (mean ± SD)

Table 3 Comparison of T lymphocyte subsets between the two groups (mean ± SD)

Figure 1 Comparison of pain degree between two groups. VAS: Visual analogue scale.
Comparison of mental health related scores between two groups
The mental health related scores of the two groups were similar before intervention (P> 0.05). After intervention, the SAS and SDS scores of the two groups were lower than those before intervention, and the observation group was lower (P<0.05). See Figures 2 and 3.
Comparison of MCMQ scores between two groups
MCMQ scores of the two groups were similar before intervention (P> 0.05). After intervention, the face scores of the two groups were higher than those before intervention, and the observation group was higher (P< 0.05). The avoidance and yield scores of the two groups were lower than those before intervention, and the observation group was lower (P< 0.05).See Table 4.
Comparison of FLIC scores between two groups
The FLIC scores of the two groups were similar before intervention (P> 0.05). After intervention, the total scores of FLIC and good psychology in the two groups and the scores of good body and good society in the observation group were higher than those before intervention. The scores of good body, difficulty due to cancer, good society and nausea in the control group were compared with those before intervention (P> 0.05). The scores of good body, good psychology, good society and the total score of FLIC in the observation group were higher (P< 0.05). See Table 5.

Table 4 Comparison of medical coping style scores between two groups [ (mean ± SD), fraction]
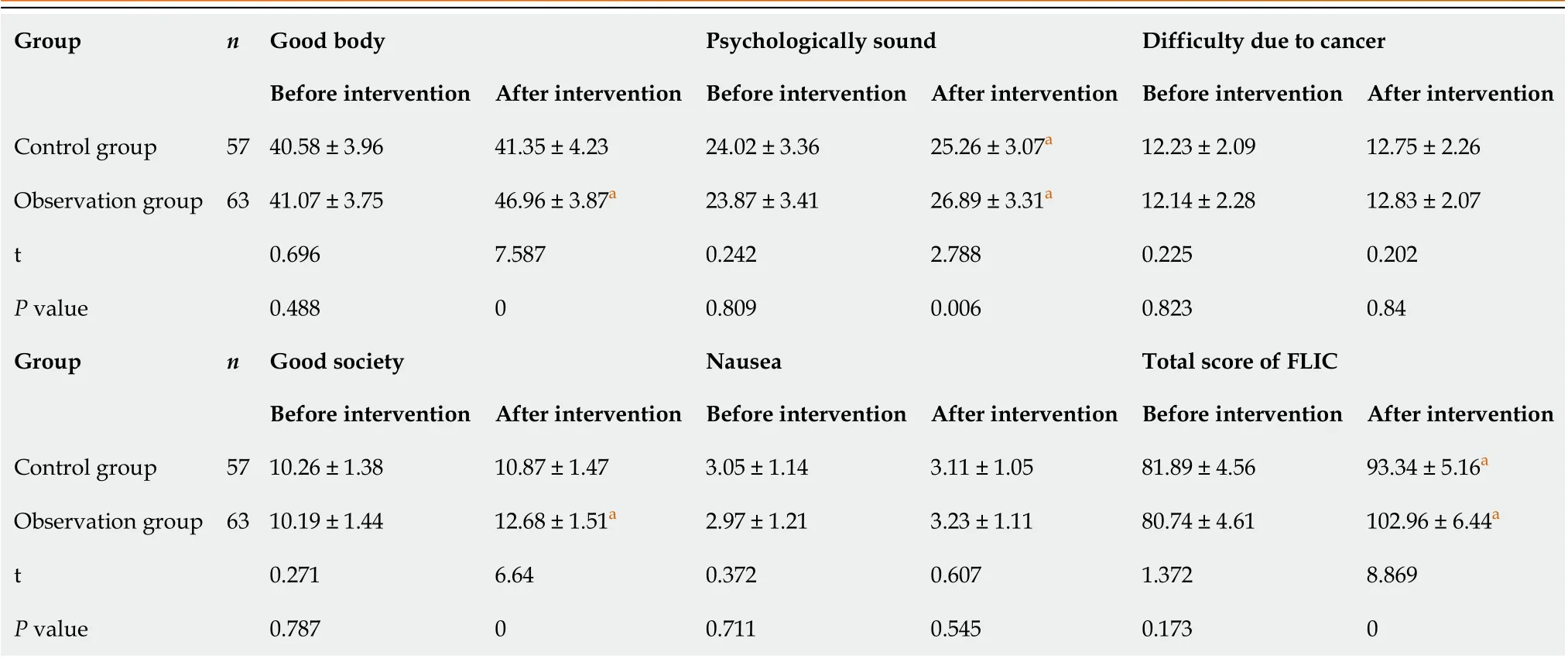
Table 5 Comparison of the life function index scale scores between two groups [ (mean ± SD), fraction]

Figure 2 Comparison of self-rating anxiety scale scores between two groups. SAS: Self-rating anxiety scale.
Comparison of complications between two groups
The cumulative complication rate of the observation group was 3.17% (2/63), which was lower than 14.04% (8/57) of the control group (P< 0.05). See Table 6.
The nursing satisfaction of the observation group was 93.65%, which was higher than that of the control group(80.70%) (P< 0.05). See Table 7.

Table 6 Comparison of complications between the two groups, n (%)

Table 7 Comparison of nursing satisfaction between the two groups, n (%)

Figure 3 Comparison of self-rating depression scale scores between two groups. SDS: Self-rating depression scale.
DISCUSSION
Surgical resection is the best treatment for long-term survival of patients with colorectal cancer and liver metastasis.Simultaneously, one-stage resection of primary and metastatic lesions has become widely accepted[15]. The minimally invasive, safe, and effective characteristics of laparoscopic surgery give it unique advantages in simultaneous resection of colorectal liver metastases[16]. The implementation of targeted nursing and psychological intervention during the perioperative period can further promote the postoperative recovery of patients and help to achieve better therapeutic effects[17]. Accelerated rehabilitation surgical nursing is an innovative treatment revolution, and it is mainly patient centered.Through the cooperation of surgery, anesthesia, nursing, nutrition, and other disciplines, it achieves win-win results for doctors and patients' families[18].
In this study, the postoperative recovery-related indicators of the two groups were compared. The results showed that the postoperative exhaust, defecation, eating, drainage, and hospitalization time of the observation group were shorter than those of the control group, indicating that accelerated rehabilitation surgical nursing combined with mental health education can accelerate the recovery of gastrointestinal function. The reason is that accelerated rehabilitation surgical nursing provides targeted nursing for patients on postoperative diet. According to the recovery guidelines for postoperative gastrointestinal function, a phased diet plan is formulated to avoid spicy and other stimulating foods and reduce the hyperstimulation of gastrointestinal function. At the same time, the patient's abdomen is massaged to promote gastrointestinal peristalsis and accelerate the recovery of postoperative gastrointestinal function[19-21].
In this study, the degrees of pain experienced by the two groups were compared. The pain score of the observation group was lower than that of the control group at 6, 12, 24, 48, and 72 h after surgery, indicating that education can reduce the degree of postoperative pain in patients. The reason is that education promotes the understanding of the importance of surgery and postoperative precautions. The diversification of education methods can enable patients to understand the operation process and treatment principle in different aspects; this may reduce patients' fear of postoperative pain and improve compliance[22]. Simultaneously, accelerated rehabilitation surgical nursing, combined with the use of a self-controlled intravenous analgesia pump, and non-steroidal anti-inflammatory drugs for analgesia treatment, can reduce incision pain[23]. Massage of the Hegu, Zusanli, Weizhong, and other acupoints also helps to reduce the degree of pain and reduce the pain score[24].
This study compared the mental health-related scores of the two groups. The SAS and SDS scores of the two groups were lower than those before the intervention, and the postoperative observation group score was lower than that of the control group. The MCMQ scores of the two groups were compared. The scores of the two groups were higher than those before the intervention, and the observation group score was higher than that of the control group after surgery. The avoidance and yield scores of the two groups were lower than those before the intervention, and the observation group scores were lower than those of the control group after surgery. These results show that accelerated rehabilitation surgical nursing combined with mental health education can more effectively alleviate patients' negative emotions such as anxiety and depression, improve patients' psychological state, and help patients actively face the disease. This is because mental health education through the psychological assessment of patients and use of the full range of psychological interventions, prompting patients to vent their negative emotions, help patients to resolve bad mood and establish a good mentality[25]. Accelerated rehabilitation surgical nursing reduces patients’ fear of disease and surgery, by improving the professional and psychological nursing level of staff, allowing the timely psychological counseling of patients, and conveying knowledge of the disease to patients in an accessible manner, so as to better improve their psychological state[26,27].
After the intervention, the physical, psychological, social well-being, and FLIC in the observation group were higher than those in the control group, and the incidence of complications was lower. The nursing satisfaction of the observation group was better than that of the control group, indicating that accelerated rehabilitation surgical nursing combined with mental health education can help reduce complications and improve the quality of life of patients and nursing satisfaction. As mentioned above, accelerated rehabilitation surgical nursing can promote the recovery of gastrointestinal function and improve the psychological state of patients. Concurrently, through postoperative rehabilitation training,accelerated rehabilitation surgical nursing guides patients to promote physical recovery. The hip lifting and kicking exercises are used to exercise the patients’ lower limbs, thereby promoting their functional recovery, and reducing complications such as intestinal obstruction and incision infection, improving patient activities of daily life and quality of life[28-30]. The prevention of various complications can improve the postoperative comfort of patients, and pay more attention to psychological nursing in the nursing process, timely help patients solve difficulties, and establish a good doctor-patient relationship.
The patients included in this study were from the same center, and the number of patients was also limited. The results of this study need to be confirmed by large cohort study in the future.
CONCLUSION
In summary, enhanced recovery after surgical nursing combined with mental health education can promote the recovery of gastrointestinal function, improve patients’ mental health and quality of life, and reduce the incidence of complications after laparoscopic resection of liver metastases from colorectal cancer.
ARTICLE HIGHLIGHTS

FOOTNOTES
Author contributions:Li DX and Ye W contributed equally to this work; Li DX, Ye W, and Jiang PH designed the research study; Li DX,Yang YL, Zhang L and Qian XJ performed the research; Li DX, Jiang PH and Yang YL analyzed the data and wrote the manuscript; All authors have read and approved the final manuscript.
Supported byNational Key Clinical Discipline; and the National Science Foundation of China, No. 82002587.
Institutional review board statement:The study was reviewed and approved by the Institutional Review Board of The Sixth Affiliated Hospital of Sun Yat-sen University, No. 2023ZSLYEC-046.
Informed consent statement:The ethics committee reviewed and approved the waiver of informed consent/informed consent signing.
Conflict-of-interest statement:All the authors report no relevant conflicts of interest for this article.
Data sharing statement:Technical appendix, statistical code, and dataset are available from the corresponding author at jiangph3@mail.sysu.edu.cn.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORCID number:Dong-Xia Li 0009-0004-4799-8805; Xiang-Jun Qian 0000-0001-6485-0731; Ping-Hua Jiang 0009-0001-2336-163X.
S-Editor:Li L
L-Editor:A
P-Editor:Wu RR
 World Journal of Gastrointestinal Surgery2023年8期
World Journal of Gastrointestinal Surgery2023年8期
- World Journal of Gastrointestinal Surgery的其它文章
- Is endoscopic mucosal resection-precutting superior to conventional methods for removing sessile colorectal polyps?
- Knowledge, attitude, and practice of monitoring early gastric cancer after endoscopic submucosal dissection
- Changing trends in gastric and colorectal cancer among surgical patients over 85 years old: A multicenter retrospective study, 2001-2021
- Effects of ultrasound monitoring of gastric residual volume on feeding complications, caloric intake and prognosis of patients with severe mechanical ventilation
- Risk factors and their interactive effects on severe acute pancreatitis complicated with acute gastrointestinal injury
- Regional differences in islet amyloid deposition in the residual pancreas with new-onset diabetes secondary to pancreatic ductal adenocarcinoma