
Comparison of success rate and intraocular pressure spikes between selective laser trabeculoplasty and micropulse laser trabeculoplasty in African American and Hispanic patients
2023-02-11 08:59:12AlexanderRobinPalwashaSyarDanaDarwishCatherineThomasPfahlerAgniKakouriThomasPatrianakosMichaelGiovingo
Alexander Z Robin, Palwasha Syar, Dana Darwish, Catherine Thomas, N.M. Pfahler, Agni Kakouri, Thomas Patrianakos, Michael Giovingo
1Department of Ophthalmology, John H. Stroger, Jr. Hospital of Cook County, Chicago, IL 60612, USA
2Rosalind Franklin University of Medicine and Science, North Chicago, IL 60064, USA
3Department of Ophthalmology and Visual Science, University of Illinois at Chicago, Chicago, IL 60612, USA
4Department of General Surgery, University of Texas at Houston, Houston, TX 77030, USA
Abstract
● KEYWORDS: selective laser trabeculoplasty; micropulse laser trabeculoplasty; glaucoma; open angle glaucoma;ocular hypertension
INTRODUCTION
Laser trabeculoplasty (LT) is a mainstay of treatment for the management of open angle glaucoma (OAG). Argon laser trabeculoplasty (ALT), introduced in 1979 by Wise and Witter[1], directly applies coagulative thermal energy to the trabecular meshwork (TM) to increase aqueous outflow and thus lower intraocular pressure (IOP). The Glaucoma Laser Trial showed that ALT was as effective as topical beta blockers[2]for controlling IOP, however it was associated with serious post‐procedure complications such as acute and late onset IOP spikes[3], corneal endothelial damage[4]and permanent TM scarring. These complications were attributed mostly to the destructive effects of the thermal energy to surrounding ocular tissue[5]. To avoid these complications, Latina and Park[6]developed a more selective laser trabeculoplasty (SLT)aimed at primarily targeting pigmented TM cells. SLT delivers a photo‐disruptive, shorter duration, energy beam that is selectively absorbed into the pigmented TM cells with minimal risk of heat transfer and damage to the surrounding ocular tissue[6‐7]. SLT proved to be equally effective and safer than ALT[7], but serious complications such as IOP spikes, acute iritis, and retinal side effects such as cystoid macular edema continued to occur at a non‐negligible rate[7‐8]. In particular,SLT has been associated with an increased rate of 1h post procedure pressure spikes in patients with deeply pigmented TM, prior ALT procedures and those taking multiple topical medications[9]. Additionally, both ALT and SLT have been known to exhibit a diminished long‐term effect on IOP control.Schwartzet al[10]followed 72 patients that received ALT for OAG and revealed that the pressure lowering effect of ALT dropped from 72% at 2y to 46% at 5y. Similarly, the success rate of SLT ranges from 67%‐75% at 6mo dropping to 11%‐31% at 5y[11].
Micropulse laser trabeculoplasty (MLT), first described in 2005 by Ingvoldstatet al[12], utilizes a 15% duty cycle of delivered energy as opposed to continuous energy release. This limits the thermal elevation of tissue surrounding the targeted pigmented TM. Microscopically ALT has been shown to cause TM traction and shrinkage and SLT can result in cracking of the pigment granules in pigmented TM cells[13]. These histological findings have not been observed with MLT, an advantage that can clinically result in less inflammation and potentially limit post‐procedure IOP spikes[13].
Given the short amount of time that MLT has been commercially available, there is limited, although quite promising, data that demonstrates its efficacy and safety.SLT and MLT have both separately been reported to have complications of IOP spikes, iritis, hyphema, macular edema,cornel haze, and peripheral anterior synechiae formation[8,14].However, to our knowledge there have only been three studies comparing the outcomes of SLT and MLT[15‐17]. Previous studies have been limited by a small number of participants and limited diversity of participants who were primarily Caucasian or Asian. The aim of this study is to demonstrate the efficacy and safety of MLT in a large cohort that is more representative of the demographic of patients with OAGs.
SUBJECTS AND METHODS
Ethical ApprovalThe study protocol was approved by the John H Stroger Hospital of Cook County Healthy (Chicago,IL, USA) Institutional Review Board (No.21‐071X). The research adhered to the tenants of the Declaration of Helsinki.This retrospective study did not require informed consent from participants and no stipend was provided.
Study Design and ParticipantsThis is a single center retrospective comparative cohort review conducted at John H.Stroger Jr. Hospital of Cook County Health and Cook County Health affiliated facilities. Patients who underwent LT for OAG between January 2017 and May 2021 were included.Exclusion criteria included prior LT, uveitic glaucoma, angle‐closure glaucoma, neovascular glaucoma, and non‐standard laser parameters. All MLT treatments included in the study used a power of 1000 mW with a 15% duty cycle, 300ms duration, 300 μm spot size, and 360‐degree treatment with 110 to 130 total spots. SLT treatments were included if the power was 0.3‐1.3 mJ, 3 ns duration, 400 μm spot size, and>180‐degree treatment with at least 20 total spots per quadrant treated.
ParticipantsThe study included patients with OAG or ocular hypertension that received an SLT or MLT procedure. Baselinecharacteristics on age, gender, ethnicity, glaucoma type, central corneal thickness, cup‐to‐disk ratio, number of IOP lowering medications and IOP on the date of procedure measured prior to laser treatment. A comparison of baseline characteristics is listed in Table 1.
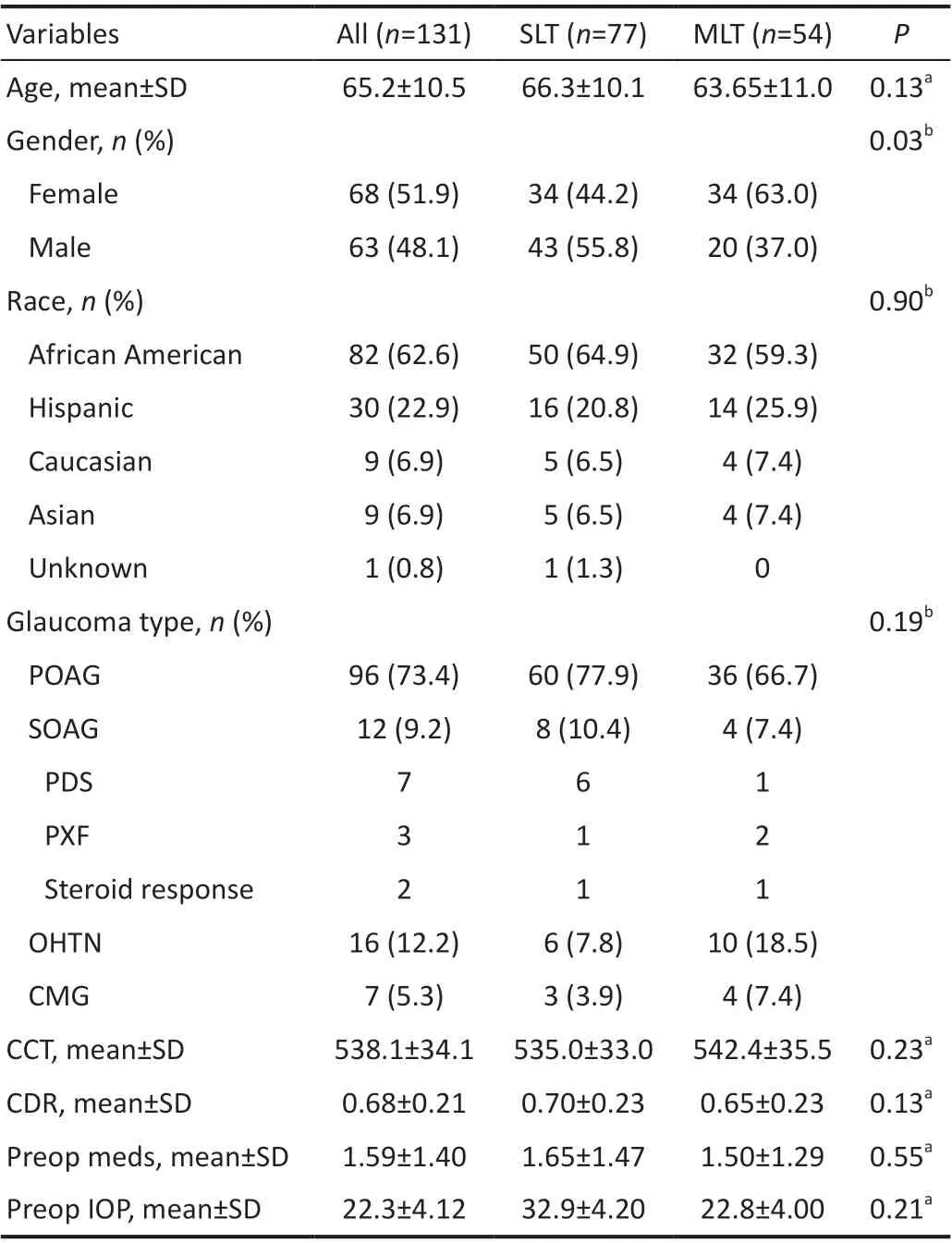
Table 1 Clinical and demographic characteristics in the study population
TreatmentPrior to LT all patients were pretreated with one eye drop of apraclonidine 0.5% and one drop of pilocarpine 1%as is standard procedure at all Cook County Health sites.
SLT was performed with a 532 nm frequency doubled Q‐switched Nd:YAG laser with settings of 400 μm spot size,and 3ns duration, 360 degrees of treatment with >20 spots per quadrant, and varying power titrated to achieve an endpoint of cavitation bubble formation. MLT was performed with a 532 nm laser with standardized settings of 300 μm spot size,300ms duration, 360 degrees of treatment with exactly 30 spots per quadrant (120 total spots), and 1000 mW with a 15%duty cycle. Procedures performed using non‐standard settings,treatment area, or spot number were excluded as they could cloud data. IOP measurements were checked by a physician using Goldmann applanation tonometry immediately prior to and at intervals of 1‐hour and 1‐week post‐procedure. Post‐laser patients were continued on their pre‐procedural IOP lowering medication, no additional planned medications were added. Patients with IOP spikes were treated on an individual basis.
SLT and MLT are both indicated for lowering IOP in patients with OAG. Laser choice depended upon physician preference and availability of the individual laser at the time of procedure.
Outcome MeasuresTwo primary outcomes were investigated in this study. The first metric investigated was the rate of IOP spikes at 1‐hour and 1‐week post‐procedure. IOP spikes were defined as a >5 mm Hg increase in IOP from baseline pre‐procedure IOP. The second metric investigated was the procedure failure rate at 1y. Failure was defined as 1) an IOP decrease <3 mm Hg or <20% on 2 consecutive visits >1mo post‐procedure; 2) increase in the number of IOP lowering medications needed prior to 1y post‐procedure; or 3) additional surgical or procedures intervention needed to control IOP prior to 1y post‐procedure. Patients with fewer than 2 IOP readings between 1mo and 1y post‐procedure were excluded from analysis.
Statistical AnalysisBaseline clinical and demographic characteristics were compared using ANOVA for continuous data and Chi‐square for categorical data. Frequencies of IOP spikes and surgical failure were compared using Chi‐square with Haldane‐Anscombe correction to account for 0 value.Odds ratios with 95% confidence intervals (CIs) were calculated for IOP spikes and surgical failure using univariate and multivariate logistic regression models with adjustments for gender, race, and number of pre‐operative IOP‐lowering medications. Risk factors for IOP spikes and surgical failure were evaluated using binary logistic regression and presented as odds ratios with 95%CIs. Non‐inferiority was evaluated using a Cox proportional hazard regression model for survival data and presented as a hazard ratio with 95%CI. All statistical analyses were performed using Stata Release 17 (StataCorp LLC, College Station, TX, USA).
RESULTS
In total, 131 eyes of 99 patients were analyzed. Totally 77 eyes received SLT and 54 eyes received MLT. The 36 patients had both eyes enrolled in the study (16 patients received SLT in both eyes, 10 patients received MLT in both eyes, and 10 patients received SLT in one eye and MLT in the fellow eye). SLT treatments were performed with total spots ranging from 84‐129 and power ranging from 0.3‐1.3 mJ. MLT was performed with standard parameters as described previously.
DemographicsAs evidenced by Table 1, the SLT and MLT groups were similar with regards to age, race, glaucoma type,central corneal thickness, cup‐to‐disk ratio, baseline glaucoma medications, and baseline IOP. However, the SLT group didhave a higher percentage of male patients when compared to the MLT groups. Both groups had a similarly high percentage of African American patients (SLT 64.9%, MLT 59.3%) and Hispanic patients (SLT 20.8%, MLT 25.9%).
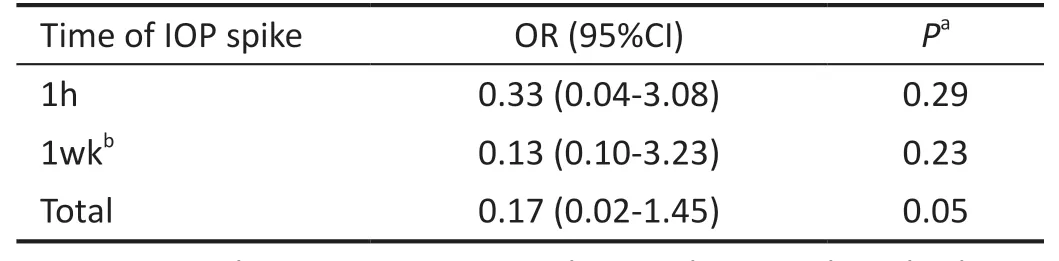
Table 2 Risk of IOP spike using MLT relative to SLT
Intraocular Pressure SpikesAt 1‐hour post‐laser, 4 out of 68 eyes (5.9%) treated with SLT had an IOP spike. In comparison, only 1 out of 49 eyes (2.0%) treated with MLT had a similar IOP spike. At 1‐week post‐laser, 3 out of 54 eyes(5.5%) treated with SLT had an IOP spike, and there were no IOP spikes out of 45 eyes analyzed at 1wk in the MLT group.In the SLT group, 9 eyes at 1h and 24 eyes at 1‐week post‐procedure did not have a recorded IOP. In the MLT group, 5 eyes at 1h and 9 eyes at 1‐week post‐procedure did not have a recorded IOP. All eyes without data at a specific time point were assumed not to have a significant IOP spike at that time.In total, 7 out of 77 eyes in the SLT group (9.1%) and 1 out of 54 eyes in the MLT group (1.9%) had an IOP spike at either 1h or 1wk post treatment (P=0.05, Chi‐squared test with Haldane‐Anscombe correction). Eyes with an IOP spike in the SLT group had an average increase of 7.57 mm Hg (SD 1.59)while the lone eye in the MLT group with an IOP spike had an increase of 5 mm Hg from baseline. This data demonstrates that eyes that received an SLT had a statistically significant increased chance of a post procedure IOP spike compared to eyes that received MLT (Figure 1; Table 2).
Eyes with post‐procedural IOP spikes were treated on an individual basis based on disease severity, amount of IOP increase, and pre‐procedural treatment regimen. The 7 eyes with IOP spikes in the SLT group were treated as follows: 1 was observed with resolution of the IOP spike when rechecked 1d later, 3 were treated with the addition of 1 IOP lowering drop to their pretreatment regimen and rechecked 1wk later at which time all eyes had resolution of their IOP spikes, 3 eyes were on the maximum available IOP lowering drops prior to SLT. One of these patients refused further treatment for the eye with an IOP spike and was monitored with resolution of the IOP spike 1mo later, one eye was treated with 1000 mg oral acetazolamide per day with resolution of the IOP spike 1wk later, and 1 eye required cyclophotocoagulation due to prolonged IOP elevation. In the MLT group, there was only 1 eye with an IOP spike. The IOP was 25 mm Hg at 1‐hour post‐procedure, increased from a pre‐procedure IOP of 20 mm Hg.This eye was observed without treatment and had resolution of the IOP spike 2d later.
No second eyes were treated while the first eye was still undergoing treatment for an IOP spike. While second eyes of patients who had an IOP spike was not specifically one of our exclusion criteria, no second eyes of such patients were included in this study. During our data collection there were no second eyes of patients who had an IOP spike in their first eye identified, this is likely because an LT was avoided in these patients.
Additional ComplicationsThis analysis did not specifically
aim to evaluate the rate of additional complications such as iritis, hyphema, macular edema, corneal haze and peripheral anterior synechia (PAS) formation. On chart review we identified one case of symptomatic iritis in the SLT group and zero case in the MLT group. No patients were identified as having hyphema, macular edema, corneal haze, or PAS formation. Patients did not receive routine gonioscopy or ocular coherence tomography of the macula during follow up visits.
Treatment FailureFailure rate at one‐year post‐procedure in the SLT group was 50% (22/44) compared to 48% (23/48)in the MLT group with a hazard ratio of 1.34 (95%CI 0.76‐2.36). TheP‐value of 0.31 on Cox regression represents non‐inferiority for MLT compared to the standard of care treatment of SLT at 1y (Table 3).
Risk factorsRisk factors for IOP spikes and treatment failure were investigated. We analyzed age, gender, race, type of glaucoma, central corneal thickness, cup‐to‐disk ratio, baseline IOP, and number of baseline medications. Eyes with a higher number of baseline glaucoma medications were found to be more at risk of IOP spikes (P=0.02) while eyes with lower baseline IOP were more at risk for treatment failure (P=0.004;Table 4).
DISCUSSION
This retrospective, comparative cohort study demonstrates that MLT may be a safer alternative to SLT with regards to post‐procedure IOP spikes while maintaining a similar 1‐year efficacy. Although there is a relative dearth of data comparingSLT and MLT, this study confirms the limited previous investigations that have shown MLT is likely equivalent to SLT with regards to IOP lowering.
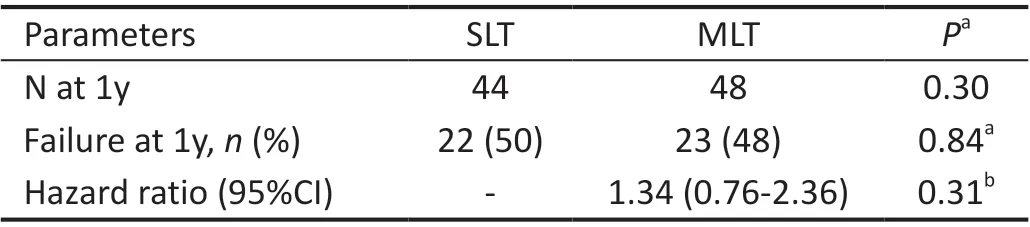
Table 3 Failure rates and non-inferiority analysis
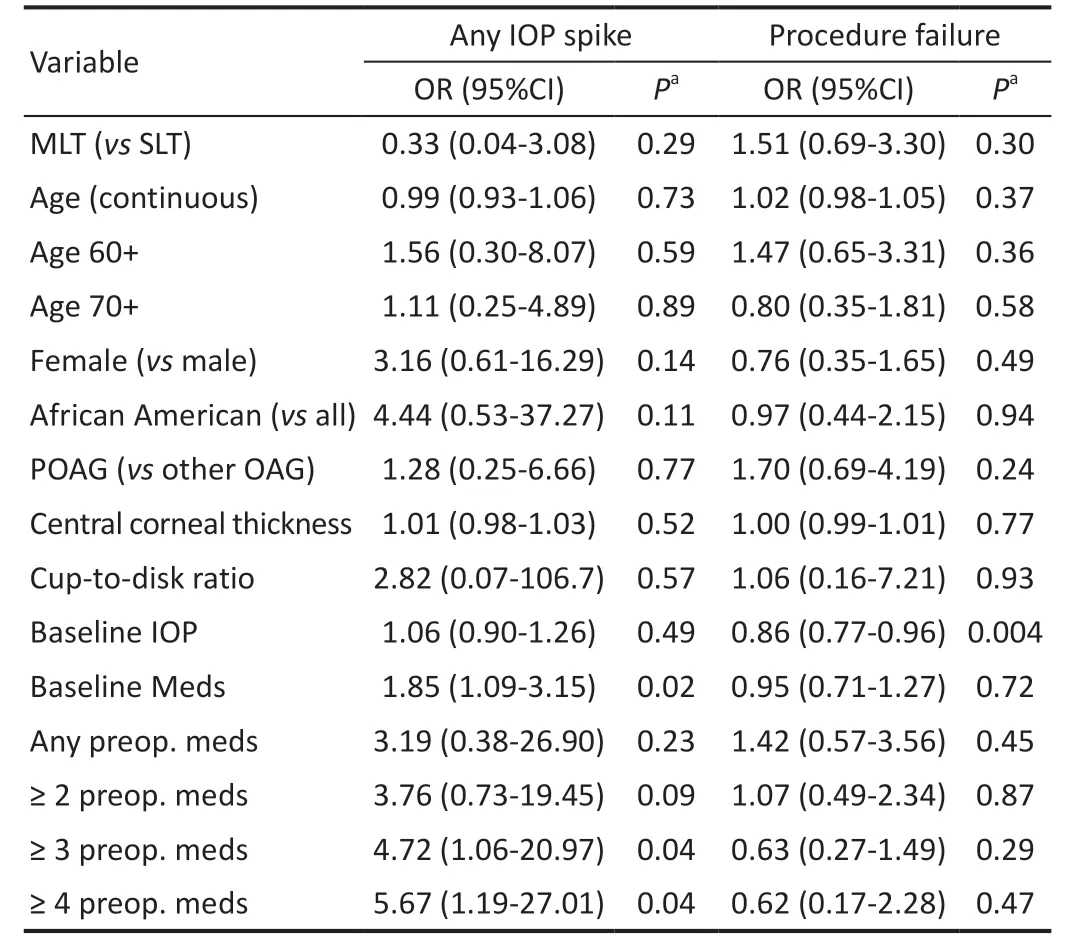
Table 4 Risk factors for IOP spikes and failures
This study is unique in that we have a larger sample size that is more representative of the real‐world demographics of patients with OAGs than previous studies. Prior studies have had a majority Caucasian and Asian patients while this study is novel it analyzed data from predominantly Hispanic and Black patients, who are at a higher risk of developing glaucoma[18‐19]. Prior studies have demonstrated differences in both the efficacy and safety of SLT when comparing between Black and Caucasian patients[20]. These results likely originate from differences in TM pigmentation as SLT was designed to selectively target pigmented tissue[11]. SLT has been shown previously to produce significant inflammation and pressure spikes in patients with more deeply pigmented trabecular meshwork[9]. MLT also works by selectively targeting pigmented tissue as well[16], however significantly even in our patient population we had a very low rate of post‐MLT pressure spikes.In addition, patients on a higher number of baseline IOP lowering eye drops in our study had a statistically higher rate of IOP spikes at both 1‐hour and 1‐week post‐procedure possibly because these eyes had a baseline reduced outflow capacity. This is important as these patients also have fewer non‐invasive treatment options available to lower IOP in the event of an IOP spike.
Other studies have also shown that MLT has a decreased incidence of post‐laser IOP spikes when compared to SLT. The findings by Sunet al[15]showed 1h IOP spikes of 16% post‐SLT treatmentvs5% post‐MLT treatment in predominantly Caucasian and Asian patients. Hirabayashiet al[16]conducted a 6‐month follow‐up of Caucasian patients to find that 10% of patients had a 1h IOP spike in the SLT group versus none in the MLT group. The present study showed that 9.1% of eyes that underwent SLT versus 1.9% of eyes that underwent MLT had a post‐procedural IOP spike which is in line with previous studies.
Several studies have been conducted to explore the severity of inflammation that occurs after LT procedures[17]and the efficacy and benefits of MLT compared to SLT[15‐17]. In 2008,a histological study was conducted to compare the tissue effects of ALT, SLT and MLT on the TM[14]. The researchers found that MLT was the least likely to cause structural damage to the TM, attributing it to the ability of the laser to minimize its thermal spread and therefore avoid coagulative damage.It has been further noted that MLT patients experience significantly less pain during and after the LT[17], making it superior over the other trabeculoplasty procedure for patient comfort.
In addition to having a lower complication rate, our study also demonstrates that MLT is non‐inferior to SLT in terms of efficacy through a 1‐year time point. The only factor that was identified as being associated with a higher treatment failure was a lower baseline IOP. This is consistent with previous studies that show that patients with a higher baseline IOP have better IOP lowering outcomes after SLT[21‐22]. At least one previous study demonstrated that fewer laser spots was associated with high treatment failure[14]. All of our MLTs were performed on 360 degrees of TM, as is standard practice at John H Stroger Hospital of Cook County Health, due to this earlier finding.Our success rate was in line with previous studies which showed a success rate of 29%‐73%[15‐17].
Cost is of concern when considering both SLT and MLT.Seideyet al[23]demonstrated that SLT is less costly than most brand name glaucoma drops within one‐year of procedure and likely less expensive than most generic medications within 13‐40mo. The CPT code for MLT is the same as SLT so the cost savings for the patient with MLT are likely similar. The initial cost to the physicians for both lasers is expensive however multi procedural use is important to consider. In addition to MLT, the IQ 532 nmTMlaser (Iridex Corporation, Mountain View, CA, USA) can be used for stimulation of the retinal pigment epithelium, retinal photocoagulation, laser peripheral iridoplasty, and laser suturolysis[17,24]. Ultimately the most cost‐effective laser likely depends on which additional procedures an individual practice is performing.
The main limitation of this study is its retrospective nature which may have resulted in selection bias. Key baseline characteristics that have been hypothesized or previously shown to be related to procedure success or complications such as age, race, type of glaucoma, central corneal thickness,baseline IOP, and baseline IOP lowering medications were all similar between groups. An additional limitation is that TM pigmentation was not routinely recorded and as such is not included in our analysis. TM pigmentation may significantly affect the rate of IOP spikes and as such could be looked at in future studies. The only difference in demographics between groups was gender. The SLT group had a higher percentage of male patients than the MLT group however we did not find any relationship between gender and procedural complications of success nor have previous studies. Some eyes did not have data for all of the follow up time points. Significantly at 1wk post‐procedure only 54/77 eyes (70.1%) in the SLT group versus 45/54 eyes (83.3%) in the MLT group had IOP values.All eyes without data at a specific time point were assumed not to have a significant IOP spike at that time. It is possible that some IOP spikes were not accounted for, however as the SLT group had more patients without IOP data it is more likely that this would have resulted in additional IOP spikes in the SLT group which would improve the significance of the data.The relatively small sample size of this study limited some potential multivariate analyses. A larger population analyzed in a prospective fashion would be beneficial for follow‐up studies. Additionally, a more complex statistical model could be used adjusting for some subjects having both eyes enrolled in the study.
In conclusion, MLT is an effective procedure to lower IOP in OAG and has a lower chance of post‐procedural IOP spikes than SLT[17,25‐26]. The rate of procedure failure at 1y was similar between eyes that received SLT and eyes the received MLT,however a significantly lower incidence of pressure spikes were seen with MLT. These results provide support for MLT as an alternative to SLT in treating patients with OAG and ocular hypertension.
ACKNOWLEDGEMENTS
Conflicts of Interest: RobinAZ,None;Syar P,None;Darwish D, None;Thomas C,None;Pfahler NM,None;Kakouri A,None;Patrianakos T,None;Giovingo M, Iridex speaker, consultant.
 International Journal of Ophthalmology2023年1期
International Journal of Ophthalmology2023年1期
- International Journal of Ophthalmology的其它文章
- Instructions for Authors
- Morphological and functional changes in the macular area in diabetic macular edema after a single intravitreal injection of aflibercept
- Macular vascularisation changes analysed using OCT angiography after successful rhegmatogenous retinal detachment repair
- Efficacy of custom-made soft keratoconus lenses on corneal aberrations and photic phenomena in patients with keratoconus: a corneal topography imaging based study
- Clinical observation of recombinant human nerve growth factor in the treatment of neurotrophic keratitis
- Destructive effects on endothelial cells of grafts in cytomegalovirus DNA-positive patients after keratoplasty