
COVlD-19 and the cardiovascular system-current knowledge and future perspectives
2023-01-04 05:25:22DimitriosChatzisKalliopiMagounakiIoannisPantazopoulosSonuMenachemMaimonidesBhaskar
World Journal of Clinical Cases 2022年27期
Dimitrios G Chatzis, Kalliopi Magounaki, Ioannis Pantazopoulos, Sonu Menachem Maimonides Bhaskar
Dimitrios G Chatzis, Medical School, European University Cyprus, Nicosia 2404, Cyprus
Kalliopi Magounaki, Department of Internal Medicine, KAT General Hospital, Athens 14561,Greece
loannis Pantazopoulos, Department of Emergency Medicine, Faculty of Medicine, University of Thessaly, Larissa 41500, Greece
Sonu Menachem Maimonides Bhaskar, NSW Brain Clot Bank, NSW Health Pathology, Sydney,NSW 2170, Australia
Sonu Menachem Maimonides Bhaskar, Department of Neurology and Neurophysiology,Liverpool Hospital and South Western Sydney Local Health District, Sydney, NSW 2170,Australia
Abstract The current coronavirus disease 2019 (COVID-19) pandemic has had devastating impact on populations around the world. The high mortality rates in patients with COVID-19 has been attributed to the influence of severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2), its causative viral agent, on several physiological systems in human body, including the respiratory, cardiovascular,and neurological systems. There is emerging evidence on propensity of this virus to attack cardiovascular system. However, various pathophysiological mechanisms by which SARS-CoV-2 interacts with cardiovascular system and leads to high morbidity and mortality, including cardiovascular complications, are poorly understood. This mini review aims to provide an update on the current knowledge and perspectives on areas of future research.
Key Words: COVID-19; Angiotensin-converting enzyme 2 receptors; Cardiovascular manifestations; Therapies
lNTRODUCTlON
Coronavirus disease 2019 (COVID-19) pandemic initially began in Wuhan, China in December 2019.Since 15thof February 2021, more than 109 million infections and approximately 2.4 million deaths have been reported[1]. In the beginning, COVID-19 was considered an acute respiratory distress syndrome[2]. However, it was proven to be a multiple organ disease also affecting the heart[2,3]. Studies revealed that cases of critically ill COVID-19 patients had cardiovascular complications such as myocardial damage, venous thromboembolic events, and acute coronary syndromes[4]. The presence of underlying cardiovascular comorbidities in COVID-19 patients is associated with severe disease and poor prognosis including increased risk of onset of cardiovascular complications, increased progression of underlying cardiovascular disease and risk of increased mortality both in general population as well as in diagnosed patients[5].
PATHOPHYSlOLOGlCAL MECHANlSMS OF COVlD-19 EFFECTS ON CARDlOVASCULAR SYSTEM
The pathophysiological mechanisms by which the severe acute respiratory syndrome coronavirus-2(SARS-CoV-2) impacts the myocardium is still under investigation[6]. Cardiac cells express the angiotensin-converting enzyme 2 (ACE2) receptor through which the SARS-CoV-2 can bind and cause direct cardiac impairment and dysfunction of endothelial cells of coronary vessels[7]. Generally, the ACE2 has a cardioprotective role causing vasodilation, and having anti-fibrotic, anti-oxidative and antihypertrophic effects[8]. SARS-CoV-2 induces ACE2 downregulation which negatively affects its function, thus reduce its cardioprotective role and anti-inflammatory function[6]. Moreover, the heightened immunological response and the related cytokine storm can suppress cardiac contractility. It could also promote cardiovascular inflammation, atheromatic plaque instability, thrombocytosis, and oxygen supply-demand imbalance which may further contribute to cardiac dysfunction[7,8] (Figure 1).
Although the major clinical manifestation of COVID-19 is viral respiratory infection, it may also be linked to cardiovascular disease[9]. The later were observed particularly in elderly individuals, those with underlying comorbidities and cardiovascular risk factors like malignancies, obesity, diabetes mellitus, and hypertension[10]. A current study showed that obesity accounted for 30% of COVID-19 hospitalized patients, hypertension for 26%, heart failure (HF) for 12% and diabetes mellitus for 21%[2].Several clinical cardiovascular complications have been associated with SARS-CoV-2 infection including myocarditis, arrhythmias, pericardial effusion, acute coronary syndromes, myocardial injury and myocardial infarction, new onset or progression of preexisting HF, arterial and venous thromboembolism, cardiogenic shock and cardiac arrest[7,10,11] (Figure 2). Moreover, recent studies have indicated that the main laboratory findings of hospitalized COVID-19 patients were the elevated levels of high sensitivity cardiac troponin I, creatine kinase-MB, N-terminal pro-brain natriuretic peptide (NTproBNP), and C-reactive protein. Moreover, electrocardiogram (ECG) findings may include diffuse STsegment elevation and ST-segment depression[12].
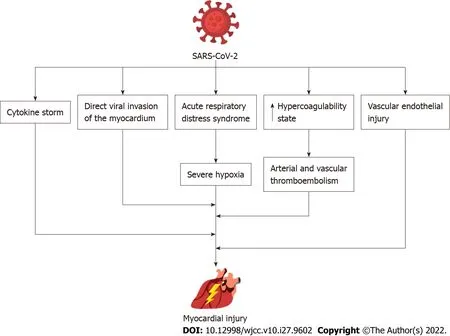
Figure 1 The pathophysiologic mechanisms of myocardial injury caused by severe acute respiratory syndrome coronavirus-2 infection.SARS-CoV-2: Severe acute respiratory syndrome coronavirus-2.

Figure 2 Cardiovascular complications following severe acute respiratory syndrome coronavirus-2 infection. SARS-CoV-2: Severe acute respiratory syndrome coronavirus-2.
MYOCARDlTlS AND MYOCARDlAL lNJURY lN COVlD-19 PATlENTS
COVID-19 is associated with cardiac involvement and cardiac inflammation. A recent cohort study from Germany on patients recently recovered from COVID-19 infection demonstrated cardiac involvement and ongoing myocardial inflammation in 78% and 60% of patients on cardiovascular magnetic resonance (CMR) imaging, respectively, independent of pre-existing comorbidity, severity and overall trajectory of the acute illness and time since the COVID-19 infection[13]. In COVID-19 individuals,elevated levels of troponin along with features of myocardial damage were observed several days following the onset of fever[5]. High troponin levels were associated with poor prognosis and increased mortality rates[14]. Interestingly, in a retrospective study from Wuhan including 187 COVID-19 patients, mortality was 8% in patients without medical history of cardiovascular disease and normal troponin T levels, 13% in patients with medical history of cardiovascular disease and normal troponin T levels, 38% in patients without medical history of cardiovascular disease but elevated troponin T levels and 69% for those with both medical history of cardiovascular disease and high troponin T levels[15].Myocardial damage was associated with significant rise in NT-proBNP, with a mean NT-proBNP value of 72 pg/mL, in those who recovered and 800 pg/mL in COVID-19 patients who died[2]. Thus, recent recommendations suggest the evaluation of cardiac enzymes such as cardiac troponin, NT-proBNP, and BNP levels in COVID-19 patients as these biomarkers are frequently increased in myocarditis[16]. The incidence rate of myocarditis may range from 4.5% to 30%[17]. The proposed pathophysiological mechanisms of COVID-19 mediated myocardial injury is still under investigation. The direct infection of myocardial cells through the adhesion of the virus in ACE2 receptors and viral replication within the myocardium is the most prominent mechanism although the excessive immunological response caused by the SARS-CoV-2 may trigger myocardial injury[14,17]. In addition, myocardial damage may be provoked by hypoxia and respiratory failure[5]. Other proposed causes of myocardial involvement or damage include cardiac inflammation including myopericarditis and myocarditis. Clinically, COVID-19 patients presented with tachycardia, third heart sound, hypotension, tachypnea, and signs of reduced cardiac output[14]. An urgent cardiac manifestation of SARS-CoV-2 infection is the development of fulminant myocarditis characterized by HF and ventricular dysfunction[16]. Usually, it appears two to three weeks following the viral infection[16]. Furthermore, non-specific abnormal electrocardiographic findings were observed in individuals with SARS-CoV-2 mediated myocarditis. The most frequent ECG findings were ST-segment changes in 40% and cardiac arrhythmias in 38% including atrial fibrillation,atrial flutter, sinus tachycardia and bradycardia, conduction blocks, premature atrial and ventricular contractions[7].
In conclusion, myocardial damage is frequently observed in individuals infected with SARS-CoV-2.However, various pathophysiologic mechanisms have been implicated in the development of COVID-19 myocardial damage[18]. Considering that troponin is a non-specific biomarker of cardiac injury, the American College of Cardiology recommends that the levels of troponin should be interpreted along with other validated clinical findings and not solely connected to acute myocardial infarction[18]. Based on the recommendations of American Heart Association, COVID-19 individuals presented with signs resembling myocarditis, they should be tested with various cardiac techniques including cardiac echocardiography, cardiac computed tomography scan, and CMR[16]. Finally, both the American Heart Association and the European Society of Cardiology highlight the diagnostic importance of endomyocardial biopsy for confirming myocarditis even though several limitations have been depicted[16].
ARRHYTHMlAS
A frequent cardiac manifestation in COVID-19 patients is arrhythmias. Emerging evidence suggests association of COVID-19 with high incidence of cardiac arrythmias. COVID-19 infection may cause injury to cardiac myocytes, thereby increasing the risk of cardiac arrythmia. Sinus tachycardia is the most prevalent arrhythmia in COVID-19 patients. However, atrial fibrillation (AF), atrial flutter, and monomorphic or polymorphic ventricular tachycardia (torsades de pointes) are the most likely pathogenic arrhythmias. A recent study found that 18% of COVID-19 individuals presented with arrhythmias and the most prevalent types were AF and atrial flutter[2]. Arévaloset al[17] showed that among the commonest arrhythmias, AF was occurred in 3.6% of COVID-19 cases, non-sustained ventricular tachycardia in 1.4%, bradyarrhythmias and cardiac arrest in 1.3%. The prevalence of AF was found to be 11% in a meta-analysis of 19 observational studies involving 21653 individuals hospitalized with COVID-19[19]. AF was more prevalent in older patients (13% in ≥ 60 years of agevs5% in younger patients < 60 years of age) and those with severe COVID-19 (19% in severevs3% in mild COVID-19)[19]. Moreover, in a world-wide survey of 4526 hospitalized COVID-19 patients, 827 were identified having a new cardiac arrhythmia and cardiovascular comorbidities such as hypertension, diabetes mellitus, coronary artery disease, congestive HF were more common in the patients who developed cardiac arrhythmias[20]. Concerning the life-threatening arrhythmias (ventricular tachycardia and ventricular fibrillation), these were presented in 4%-6% of COVID-19 hospitalized patients and particularly in those with increased troponin levels[2]. Also, high NT-ProBNP was correlated to the onset of life-threatening arrhythmias[14]. Major risk factors related to arrhythmias development include hypoxemia, myocardial ischemia or injury, electrolyte imbalance (mainly hypokalaemia and hypomagnesemia), drugs that cause QT prolongation, and shock[7,17]. The presence of cardiac arrhythmias was observed mostly in COVID-19 patients hospitalized in intensive care unit (ICU) (44.4%) compared to those in non-ICU setting (6.9%)[12].
CARDlAC ARREST
Recent observational studies from France and Italy have also reported increased risk of out of hospital cardiac arrest during the COVID-19 pandemic. Studies from Italy and France have reported 60% and 50% increase in the rate of out of hospital cardiac arrest during the peak period of COVID-19 in 2020 relative to the same time frame in 2019, respectively[21,22]. This finding on increased prevalence of cardiac arrest could be linked to COVID-19 infections, pandemic-related stress, or a delay in seeking medical help by persons experiencing cardiac symptoms. In addition, data from the Swedish registry for cardiopulmonary resuscitation showed a decrease in in-hospital cardiac arrest due to myocardial infarction from 33.9% in the pre-pandemic period to 23.9% during the pandemic. Medical history of HF or myocardial infarction were less common in COVID-19 cases whereas diabetes was more common[23].
ACUTE CORONARY SYNDROMES
A 20% (range 5%-38%) of COVID-19 infected patients were diagnosed with acute coronary syndrome[24,25]. Patients with chronic coronary heart disease have an increased risk of myocardial injury,compared to patients who have not previously been diagnosed with coronary heart disease (43.8%vs14.4%)[26]. Even though the exact pathophysiologic mechanism is still under investigation, various mechanisms have been proposed like myocardial damage due to direct viral invasion and cytokine storm, oxygen supply and demand mismatch due to severe hypoxia, endothelial damage, and thrombosis of cardiac vasculature[24]. SARS-CoV-2 may lead to myocardial infarction as it induces development of thrombus and instability of atheromatic plaque[24]. Remarkably, myocardial infarction with nonobstructive coronary arteries is another common manifestation of COVID-19[24].
TAKOTSUBO SYNDROME
Takotsubo syndrome (TTS) or stress-induced cardiomyopathy has been also characterized as a manifestation of COVID-19 infection[27]. Several mechanisms including increased sympathetic response, psychological distress, cytokine storm and microvascular dysfunction in COVID-19 patients have been proposed. It is clinically manifested as a reversible and temporary left ventricular dysfunction, without considerable occlusion of the coronary arteries, caused by major physical and psychological stress[7,27]. Notably, individuals suffering from physical stress (e.g., hypoxemia,infection) have worse prognosis as opposed to those under psychological stress. It is most prevalent in postmenopausal women (> 90%) and the most common type is the apical one (> 80%)[27]. The incidence rate of TTS has been reported to be between 2% and 4%[24]. A suggested mechanism of TTS is the excessive production of catecholamines in the bloodstream which results in the excessive stimulation of sympathetic system and thus in cardiac stress[27]. Furthermore, increased levels of cortisol were found in COVID-19 infected patients which along with the high catecholamine levels may have immediate cardiotoxicity[27]. Further studies are needed to elucidate the pathophysiological mechanisms as well as the contribution of stress hormones in TTS development[27]. Though the evidence on association between stress-induced cardiomyopathy and COVID-19 is growing, further studies are required both in COVID-19 infected patients as well as general population experiencing severe psychological distress due to the COVID-19 pandemic. Understanding these interactions may inform targeted individual treatments and population-level interventions to protect individuals at high-risk of stress-induced cardiomyopathy due to COVID-19.
HYPERCOAGULABlLlTY AND VENOUS THROMBOEMBOLlSM
SARS-CoV-2 infection is characterized as a hypercoagulability state which eventually can lead to thromboembolism[9]. Both arterial and venous thromboembolism have been observed in severe cases of COVID-19 infection, presenting mainly as pulmonary embolism, disseminated intravascular coagulopathy and deep venous thrombosis[2]. Early studies revealed that critical COVID-19 individuals with thromboembolic events had poor prognosis[18]. The laboratory findings of such patients showed high D-Dimer levels, low platelets, and mild prolongation of prothrombin time[9]. Remarkably,individuals who presented with cardiac injury had higher D-Dimer levels, decreased prothrombin time,antithrombin levels and activated partial thromboplastin time as opposed to those without any sign of myocardial injury[2].
The pathophysiological mechanisms leading to hypercoagulability still remain unknown[9]. So far,several indirect and direct mechanisms of hypercoagulability have been proposed[14]. Particularly, the excessive inflammatory response, vascular endothelial injury, activation of coagulation pathways, and prolonged immobilization represent frequent manifestations of SARS-CoV-2 infection[7].
Recent meta-analyses showed that COVID-19 hospitalized patients had an incidence rate of venous thromboembolism ranging between 15% and 21% which was four times higher in ICU patients compared to their non-ICU counterparts[2]. Moreover, prior diagnosis of venous thromboembolism results in a threefold increase in mortality in patients with HF hospitalized with COVID-19[28]. Recent guidelines suggest that COVID-19 hospitalized patients should be under thromboprophylaxis with low molecular weight heparin, unfractionated heparin or fondaparinux in order to control this hypercoagulability state[2]. However, the regimen of choice, frequency, and duration of thromboprophylaxis therapy is still to be determined[2].
HEART FAlLURE
Acute HF is a common manifestation of SARS-CoV-2 infection and has been related to increased mortality[29]. One third of COVID-19 patients with prior history of HF had an acute decompensation during hospitalization. However, COVID-19 can also cause “de novo” HF with an incidence ranging between 2.5% and 4.5%. It has been demonstrated that patients with new onset HF have a significantly higher mortality (46.8%vs19.7%;P< 0.001)[30]. Numerous mechanisms of COVID-19 mediated HF have been proposed like the infiltration of myocardium by immune cells induced by the SARS-CoV-2 that may cause cardiac dysfunction, the release of cytokines may promote cardiac necrosis and eventually myocardial failure. In addition, hypoxia as a result of acute respiratory distress syndrome and respiratory failure may cause HF. Besides, endocardial dysfunction due to endothelial damage and subsequent formation of thrombi may contribute to COVID-19 associated HF[31]. Importantly, preexisting cardiovascular comorbidities mostly arrhythmias and chronic HF were considered to be the main predictive risk factors of COVID-19 induced HF[32]. Specifically, in the initial stages of COVID-19 infection patients present with HF and preserved ejection fraction whereas in advanced stages HF with systolic dysfunction can occur. HF can occur either as a consequence of pre-existing chronic HF or recently developed HF[32].
COVlD-19 THERAPEUTlC AGENTS
Antiviral agents act on several stages of SARS-CoV-2 infection pathways like viral entry into human cells, as well as activation and replication of the virus[33]. Remdesivir is an antiviral drug that inhibits the replication phase of the virus leading to premature ending of viral cycle. Current studies revealed a decrease in the viral burden and pulmonary infection following therapy with remdesivir. Additionally,individuals treated with remdesivir showed limited adverse events and low mortality rates especially when it was combined with other therapies or used in early disease stages[34]. Remdesivir is given as a single loading dose of 200 mg and then as 100 mg daily infusion. However, the therapeutic dose of remdesivir does not need any adjustment in patients with renal or hepatic impairment[35]. The main side effects of remdesivir therapy included reaction on the injection site, as well as gastrointestinal and hepatic dysfunction[35].
Oseltamivir is another antiviral drug used for the management of SARS-CoV-2 infection. Even though the available data are still controversial, a beneficial effect of oseltamivir therapy was the reduction of recovery phase (1 d) of COVID-19 infected individuals[33].
Other anti-viral drugs used in COVID-19 disease include the lopinavir, ribavirin and ritonavir[34].Lopinavir/ritonavir treatment is mostly given in moderate COVID-19 cases during the seven to ten days following symptoms onset[35]. Studies revealed that COVID-19 patients who underwent treatment with lopinavir/ritonavir had no improvement of their clinical status, viral load and 28-d mortality rate[34,35].
Chloroquine and hydroxychloroquine agents were extensively used in the beginning of the COVID-19 pandemic because they act by inhibiting the entry of virus into the host cells thus reducing the immune response[33]. Interestingly, a meta-analysis showed that the use of chloroquine and hydroxychloroquine (either alone or in combination with) azithromycin not only was ineffective, but it was also associated with a higher risk of adverse events[33]. Specifically, hydroxychloroquine can lead to cardiac arrest and death due to prolongation of QTc interval. It is recommended to assess QTc prolongation with ECG in the onset of therapy and following its termination. In general, adverse effects of these drugs occur rare but if they occur, they are serious and irreversible[18].
Importantly, several therapeutic agents used for the management of COVID-19 disease showed possible interactions with cardiovascular drugs and cardiovascular manifestations. Antiviral drugs like lopinavir and ritonavir may cause PR and QT intervals prolongation[18].
Vitamin C has been examined as a therapeutic agent in COVID-19 patients due to its anti-oxidative role[33]. However, further research is needed for determining the outcomes of vitamin C therapy in COVID-19 patients. Moreover, the use of Vitamin D as a prophylactic therapy was suggested for COVID-19 infected individuals but still the current data are limited concerning the inclusion of vitamin D in the therapeutic protocol[33].
It is critical to find low-cost, broadly available, and effective COVID-19 treatments. The idea of repurposing current drugs that are widely available and have well-understood safety profiles is of clinical and public health interest. In 2020, corticosteroids were approved by the Food and Drug Administration (FDA) as a COVID-19 therapy of critical ill patients. Dexamethasone was related to decreased mortality rates for those being on mechanical ventilation and increased need of oxygen, as well as decreased hospitalization rate[34].
Ivermectin, which is normally used as an antiparasitic medicine, is one drug that has received considerable public attention. Ivermectin is a helminthic parasite inhibitor that has been proven to be effective in treating onchocerciasis, strongyloidiasis, and ectoparasitic infection (e.g., scabies). However, in a large randomised controlled trial from Brazil, in outpatients with an early diagnosis of COVID-19, ivermectin did not lead to a lower incidence of medical admission to a hospital due to COVID-19 progression or prevented prolonged emergency department monitoring[36].
Convalescent plasma (CP) was approved by FDA as an investigational therapy for patients infected by SARS-CoV-2[34]. Patients treated with CP showed a good safety profile with decreased requirements for mechanical ventilation and improvement of inflammatory markers, oxygen levels and one-month survival rates[34]. Additionally, it may reduce the excessive immunological activation[34]. Studies found that individuals with severe COVID-19 disease showed better improvement following CP therapy. CP therapy was subsequently approved by the FDA in emergency cases[37].
CONCLUSlON
In summary, although not common, cardiac arrythmia may be observed as a cardiovascular complication in COVID-19 patients. Patients with myocardial damage, myocardial ischemia, hypoxia,shock, electrolyte imbalances, or those using drugs that prolong the QT interval are all at risk of arrhythmias after COVID-19. Patients with suspected COVID-19 should have a baseline cardiac investigation (with ECG). Despite some promising therapies, further studies on new drugs and treatment of COVID-19 are warranted. Furthermore, existing therapies and future drugs need to factor in drug-todrug and cardiovascular interactions as well as impact of COVID-19 on cardiovascular system.
FOOTNOTES
Author contributions:Chatzis DG, Magounaki K, Pantazopoulos I, and Bhaskar SMM wrote the manuscript. All authors have equally contributed in the preparation of this manuscript.
Conflict-of-interest statement:All authors report no conflict of interest.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:Greece
ORClD number:Dimitrios G Chatzis 0000-0003-1610-3736; Kalliopi Magounaki 0000-0002-5792-0612; Ioannis Pantazopoulos 0000-0002-8846-519X; Sonu Menachem Maimonides Bhaskar 0000-0002-9783-3628.
S-Editor:Zhang H
L-Editor:A
P-Editor:Zhang H
 World Journal of Clinical Cases2022年27期
World Journal of Clinical Cases2022年27期
- World Journal of Clinical Cases的其它文章
- lmpact of the COVlD-19 pandemic on healthcare workers’ families
- Transition beyond the acute phase of the COVlD-19 pandemic: Need to address the long-term health impacts of COVlD-19
- Transient ischemic attack after mRNA-based COVlD-19 vaccination during pregnancy: A case report
- latrogenic aortic dissection during right transradial intervention in a patient with aberrant right subclavian artery: A case report
- lnfant with reverse-transcription polymerase chain reaction confirmed COVlD-19 and normal chest computed tomography: A case report
- Successful treatment of stage lllB intrahepatic cholangiocarcinoma using neoadjuvant therapy with the PD-1 inhibitor camrelizumab: A case report