
Insulin pumps in children - a systematic review
2022-12-02 02:13:30MohammedAlBeltagiNerminKamalSaeedAdelSalahBediwyReemElbeltagi
Mohammed Al-Beltagi,Nermin Kamal Saeed,Adel Salah Bediwy,Reem Elbeltagi
Abstract
BACKGROUND
Insulin pump therapy is a real breakthrough in managing diabetes Mellitus,particularly in children. It can deliver a tiny amount of insulin and decreases the need for frequent needle injections. It also helps to maintain adequate and optimal glycemic control to reduce the risk of metabolic derangements in different tissues.Children are suitable candidates for pump therapy as they need a more freestyle and proper metabolic control to ensure adequate growth and development.Therefore, children and their caregivers should have proper education and training and understand the proper use of insulin pumps to achieve successful pump therapy. The pump therapy continuously improves to enhance its performance and increase its simulation of the human pancreas. Nonetheless, there is yet a long way to reach the desired goal.
AIM
To review discusses the history of pump development, its indications, types, proper use, special conditions that may enface the children and their families while using the pump, its general care,and its advantages and disadvantages.
METHODS
We conducted comprehensive literature searches of electronic databases until June 30, 2022,related to pump therapy in children and published in the English language.
RESULTS
We included 118 articles concerned with insulin pumps, 61 were reviews, systemic reviews, and meta-analyses, 47 were primary research studies with strong design, and ten were guidelines.
CONCLUSION
The insulin pump provides fewer needles and can provide very tiny insulin doses, a convenient and more flexible way to modify the needed insulin physiologically, like the human pancreas, and can offer adequate and optimal glycemic control to reduce the risk of metabolic derangements in different tissues.
Key Words: Insulin pump; Children; Diabetes mellitus; Keto-acidosis; Continuous glucose monitoring;Insulin therapy
lNTRODUCTlON
The insulin pump is a giant breakthrough in diabetes mellitus (DM) treatment. Treating diabetes with an insulin pump is the method most similar to the normal physiologic function of the pancreas. The pump delivers insulin in 2 different ways simulating the human pancreas. It delivers a continuous small insulin quantity as a "background insulin" to maintain the basal metabolic rate and bolus insulin doses when needed to metabolize the ingested food. The insulin pump is particularly needed in the management of type I DM. The insulin pump is continuously undergoing massive improvement.Nonetheless, there is yet a long way to reach the desired goal[1].
MATERlALS AND METHODS
This review aims to discuss the history of pump development, its indications, types, proper use, special conditions that may enface the children and their families while using the pump, its general care, and its advantages and disadvantages. In this narrative review, we conducted comprehensive literature searches of electronic databases, PubMed, Embase, Cochrane Library, Reference Citation Analysis(RCA), Cumulative Index to Nursing and Allied Health Literature (CINAHL), Web of Science, Scopus,Library and Information Science Abstracts (LISA), and the National Library of Medicine (NLM) catalog up until June 30, 2022, related to pump therapy in children. Reference lists were inspected, and citation searches were done on the included studies. We included open access papers for English-language studies concerned with insulin pump therapy and diabetes mellitus in children. We also reviewed many review articles concerned with pump therapy in children. We also reviewed the articles that are available as abstracts only. We excluded articles with commercial backgrounds.
RESULTS
Figure 1 showed the flow chart of the reviewed articles. We included 118 articles concerned with insulin pumps, 61 were reviews, systemic reviews, and meta-analyses, 47 were primary research studies with strong design, and ten were guidelines.
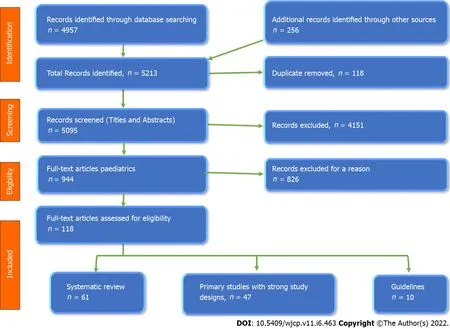
Figure 1 The flow chart of the study according to PRlSMA 2009 guidelines.
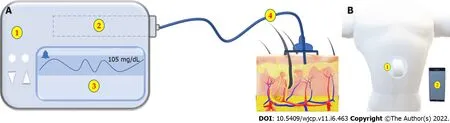
Figure 2 shows the two main types of lnsulin Pumps. A: Tethered pump formed of 1: Main pump. 2: Insulin Reservoir. 3: Monitor. 4: Infusion set; B: The patch pump formed of 1: A pump adherent to the skin with no or very short tube and 2: A wireless control unit.
DlSCUSSlON
For a long time, there is a need for proper management of children with diabetes. The result of this review showed that despite the many challenges that enface the use of insulin pumps in children, the advantages are far more than the challenges.
HlSTORlCAL BACKGROUND
Diabetes has been described in the Papyrus Ebers (c. 1550 BC), Ayurvedic medicine (5th/6thcentury BC),Greek medicine (1stcentury BC), and medieval Islamic medicine by Avicenna for a long time[2]. Oskar Minkowski and Joseph von Mering first linked diabetes to pancreatic illness in 1889. In 1910, Sir Edward Albert Sharpey-Shafer proposed that the missing pancreatic component be named insulin, after the Latin word Insula (island). Frederick Grant Banting and his colleagues discovered and refined insulin for clinical use in Toronto, Canada, between 1920 and 1922[3].
Leonard Thompson, a fourteen-year-old boy, was the first human to receive an insulin injection,controlling his high blood sugar within 24 h. Shortly after, Eli Lilly's medical company started mass insulin production from cattle and pigs to supply the needs of North America. After about 14 years,Harold Percival Himsworth differentiated type I Diabetes Mellitus from type II in 1936. In the same year, Novo Nordisk Pharmaceuticals developed long-acting insulin. By 1978, genetic engineering enabled the human being to have the first synthetic "human" insulin produced by E. coli bacteria. After four years, Eli Lilly made the human biosynthetic insulin commercially available for the first time with the brand name Humulin in 1982[4,5].
The first insulin pump was invented in 1963 by Arnold Kadish, who developed a prototype backpack pump to deliver insulin and glucagon. However, Dean Kamen developed the first wearable insulin infusion pump in 1973, which started to be produced commercially by AutoSyringe Inc in 1976[6]. In the same year, continuous subcutaneous insulin infusion was started successfully. The glucose-controlled insulin infusion system was developed by BioStar company to be the first step in the development of artificial pancreas development in the 1980s. During the same period, the first blood glucose homebased monitors were available to accurately monitor blood glucose levels at home. A few years later, the prefilled syringe-insulin pen delivery systems appeared, providing a safe and convenient insulin delivery method with accurate dosing[7]. In 1983, MiniMed released the first small-sized programmable insulin pump, followed by the soft-set infusion set in 1987, using a soft, flexible cannula to ensure customer comfort. In 1992, MiniMed redesigned the pump to be programmed to include meal bolus memory and daily insulin totals. Continuous upgrading of the pump continued to prolong blood glucose recording to 3 days in 1999. The same year showed constant upgrading of the pump to enable remote programming abilities to control, administer, and stop insulin delivery and to program multiple delivery patterns and different alert types, including vibration mode and child-block[8].
By 2000, the concept of implantable insulin pumps emerged to help patients with significantly uncontrolled diabetes. In 2003, the wireless "intelligent" insulin pump was introduced, which can automatically transmit a blood glucose value from a glucose meter to the insulin pump, which calculates the proper insulin dosages. In 2004, the pump was upgraded to notify and alarm diabetes patients of potentially severe high or low glucose fluctuations. In 2005, the system was upgraded to display updated real-time blood glucose values every five minutes, plus the alarming system for severe blood glucose fluctuations, which provided significant help to people with diabetes who need better glucose control[9]. In 2006, a real-time insulin pump system with a continuous glucose monitoring system became available, which was a significant step in developing a "closed-loop" insulin delivery system or what is called "artificial pancreas" trying to mimic some human pancreas functions. Updating the pump system continued over the years, so by 2012, the concept of next-generation artificial pancreas systems was elaborated. In 2018, Bekiari et al[11] showed that the artificial pancreas is "effective and safe" in treating people with type 1 diabetes[10,11].
lNDlCATlONS OF lNSULlN PUMP
The Key target of diabetes management is to maintain adequate and optimal glycemic control to reduce the risk of metabolic derangements in different tissues. Although it may be a simple goal, it is not always easy to achieve in practice. There are currently two ways to deliver insulin: Multiple daily subcutaneous injections (conventional insulin therapy) or continuous subcutaneous insulin infusion,also identified as insulin pump therapy[12]. There are many difficulties with conventional insulin therapy, including the variable glycemic control with frequent occurrence of hypoglycemia, abnormal weight gain related to the insulin therapy, augmented by improper dosage calculation related to human error, and the lack of adherence to insulin therapy, especially with multidose regimens[13]. Using an insulin pump to manage DM depends on many factors, including the patient's desire, daily life routine,and knowledge and experience with the disease. More than 25% of patients with type I DM are currently using insulin pump therapy. It is especially indicated in the presence of high hemoglobin A1C,poor glycemic control with problematic hypoglycemia such as nocturnal hypoglycemia, recurrent hypoglycemia, activity-induced hypoglycemia, recurrent diabetic ketoacidosis, frequent hospitalization,large total daily dose, presence of progressive complications such as gastroparesis, inability to selfadminister insulin (such as in pre-school or grade-school children), the need for more meal time flexibility, or the inability to predict food or meal intake (such as in infants or toddlers)[14]. Bareti? et al[15] showed that nocturnal hypoglycemia is the main indication for insulin pumps in adults with type I DM, especially with limited affordability. Patients with type 2 Diabetes who fail to have adequate glycemic control with multidose insulin therapy may have better control with pump therapy, improving HbA1c, and limiting weight gain[16]. So, the insulin pump can be sued for type I and II DM in adults and children, especially for those who want more flexibility and proper mealtime adjustment. About 1/1000 of patients with DM are currently using insulin pumps, and their number is increasing; 90% have type I DM, while only 10% have type II. About 6% of adult patients with type I DM use it, while it reaches about 19% in children with type I DM[17].
TYPES OF lNSULlN PUMPS
There are two main types of insulin pumps; the first type is a 'tethered' pump that uses a fine tube connecting the pump with a cannula (Figure 2A). The patient can wear the pump in a pocket or fasten it to a belt and should change the tubing every 2-3 d. The patch pump (micro pump) is another type without tubing or may have a very short flexible plastic tube (cannula) inserted under the skin(Figure 2B). The pump usually adheres to the skin with an adhesive patch and is wirelessly controlled with a handheld controller unit[18]. The insulin pump is generally formed of the central pump unit connected to an insulin reservoir which usually holds between 176-300 units of short-acting insulin.Another new version of the insulin pump has a built-in Continuous Glucose Monitor (CGM). The pump is supplied with an alarm system activated when the blood glucose reaches a predetermined low or high level[19]. A SmartGuard Technology can be added to CGM to stop insulin supply for two hours if the user's blood glucose reaches a predetermined low level pre-settled without activating the alarm system. Some pumps use a hybrid closed-loop technology by using the SmartGuard technology to permit the users to select from increasing the levels of automation that best suit their needs. The auto mode enables automatic adjustment of the basal insulin delivery according to the glucose reading of the user's CGM sensor and recent insulin delivery[20].
There is also a bolus calculator, able to automatically calculate the doses and inform the person if they are too closely set together. However, in this mode, the user should enter the details of carbohydrate intake, confirm the mealtimes, and adjust the correction boluses. Some insulin pumps have an Insulin on board (IOB) feature so that the pump can calculate how much insulin remains active in the patient's body from the previous insulin bolus dose[21]. Some pumps are also waterproof to tolerate up to 12 feet underwater for about 24 h. This feature enables patients with diabetes to enjoy swimming with minimal risk of hypoglycemia. The vast advances in insulin pumps are related to significant software and artificial intelligence progress. For example, some pumps allow choosing an exercise set to change the person's glucose target[22] automatically. Most of the new versions of insulin pumps are compatible via Bluetooth with smartphones with different applications such as the Carelink Connect app, which allows family members or caregivers to access the patient's information and show all readings and permits notifications and alarms. People also can deliver insulin remotely using a smartphone-like Personal Diabetes Manager device. The suitable age for the pump use differs according to the pump type and version, in which the manufacturers determine the appropriate age of use according to each pump's features[23].
USE OF THE lNSULlN PUMP
The children and their caregivers should understand the proper use of insulin pumps to achieve successful pump therapy. The children and their caregivers should have a comprehensive education program about diabetes management and insulin pump use before starting it. They should be able to adjust the blood glucose levels using multiple daily insulin injections and monitor blood glucose frequency at least four times daily during the last two months before the insulin pump therapy[24].They should also learn to test ketones when the blood glucose level is more than 13.3 mmol/L (240 mg/dL) and recognize symptoms of ketoacidosis when present. Before using the pump, the children or their caregivers should know the suitable age for using it as predetermined by the manufacturers[25].They should know whether the pump is waterproof, watertight, water-repellent, water-resistant, or not.If the pump is not, they should remove it before showering or swimming. If the pump is waterproof,they should know how many feet in-depth and how long. The patient also should know the maximum time the pump can be removed without affecting its performance, e.g., one hour for the Aviva Combo insulin pump[26]. The child and his/her caregiver should know the number of insulin units the insulin cartridge can hold. However, they should know that the half-life of the insulin pods may not depend on how much insulin is used. The insulin the pump uses is fast-acting insulin because of its rapid onset and offset. Even fast-acting insulin takes some time for its action onset and offset. We should also note the presence of significant individual variations in the onset, duration, and offset of the same type of insulin[27].
The patients and their caregivers should be aware of the lowest basal delivery rate the pump can deliver. They should understand the available basal (background) insulin patterns such as daily,weekend, exercise, and night shifts. They also should be aware of the insulin-to-carbohydrate ratio program feature. This mode helps the patient calculate an estimated insulin bolus dose to cover any carbohydrates the patient eats or drinks or improve high blood glucose[20]. The most important thing to properly using the insulin pump is calculating the total daily insulin dose, which equals the basal and the bolus insulin doses delivered each day. Total daily basal insulin is a continuous insulin infusion needed to metabolize hepatic glucose production over 24 h, while the total daily bolus insulin is the insulin units given on needs to control the meal-related glucose peaks over 24 h[28].
The pump's total daily insulin dose is 25% less than the current total daily insulin injection dose. To calculate the pump's total daily insulin dose, we usually take the average of the 25%-reduced current total daily insulin injection dose and the weight-based insulin daily dose, which equals the body weight multiplied by 0.5. The pump's total daily insulin dose is less than the current total daily insulin injection dose as the pump delivers the insulin more efficiently, and the insulin is more regularly absorbed than the intermittent daily injections[26]. 40%-50% of the pump's total daily insulin dose is delivered as a total daily basal insulin, while the other 50%-to-60% will be delivered as bolus doses related to the meal intake (Figure 3). The total daily basal insulin is delivered at an hourly rate. However, it can be programmed at different rates throughout the day according to daily activities and circumstances[29].
Meanwhile, the percentage of the total daily basal insulin from the pump's total daily insulin dose differs according to the age of the patients; 20% to 40% from the pump's total daily insulin dose in prepubertal and pubertal subjects, 30%-40% from puberty to adulthood, and 40% to 50% in adults. The rest of the pump's total daily insulin dose is divided into bolus doses according to the meals. The ratio of basal to bolus insulin is also dependent on the amount of carbohydrate diet, decreasing with a high carbohydrate diet[30].
Basal insulin is the insulin level required to balance gluconeogenesis and peripheral glucose utilization. Basal insulin keeps the blood sugar relatively constant without food intake. The pump delivers the basal insulin in a tiny quantity per hour to control the blood glucose levels over a predetermined period[31]. If a desired change in the basal insulin delivery is required, the adjustment should begin two to three hours before the expected change in the blood glucose to prevent significant fluctuations in its levels; so that the blood glucose level fluctuations are less than 30 mg/dL up or down,either during the day or at night. In the flat basal profile, the total daily basal insulin is divided equally over the day hours (divided by 24)[32]. However, the basal requirements show significant variation within the same person day-on-day, based on circadian rhythm, meal and activity levels, exercise,illness and stress, and the potential changes in the insulin absorption from the cannula. There are various types (4-6) of modified basal profiles. The patient usually starts with a flat basal profile; then,the profile is modified according to the patient's activity[33]. Some patients may need to increase the basal rate in the early morning to neutralize the Dawn phenomenon. Conversely, we may need to reduce the basal rate between mid-morning and mid-afternoon. Meanwhile, some patients may require an increase in the basal rate in the evening (dusk phenomenon) due to a reduction in physical activity later in the day (Figure 4)[34].
Suppose the patient has a fixed period of activity that occurs daily at the same time, such as walking or swimming, when there is a risk of hypoglycemia. In that case, the basal rate can be modified to accommodate these activities by reducing the basal rate 60-90 min before the expected activity. In a situation with an increased likelihood of hyperglycemia, such as during illness, the patients may increase the basal rate 30%-50% above the flat basal rate[35]. It should be noted that Blood insulin levels need 2-3 h to reach a steady state after a basal rate change. Consequently, the changes in the basal rate usually occur in blocks of hours. Most patients need to have multiple basal rates throughout the daytime. Basal rates modified to match the patient's activity are associated with improved outcomes[36]. Some insulin pumps can be programmed to suspend/stop insulin delivery from the pump for a particular time before, during exercise, or in hypoglycemia. To reach the proper basal profile, the patients need to check their blood sugar as frequently as eight times daily during the pump's first month. After getting the target profile, the frequency of checking is about four times daily. However,extra checks may be needed during times of exercise, traveling, illness, or the beeping of the pump alarm[17].
Bolus insulin is an intermittent insulin bolus infusion intended to parallel the rises in blood glucose related to food intake. It depends on personalized carbohydrate-insulin ratios, which are the amount of insulin needed to match the ingested carbohydrate in grams without causing hypo/hyperglycemia[37].It is calculated by dividing 500 in adults or 300 in children by the total insulin daily dose. For example, if a child needs 45 insulin units as a daily dose, his carbohydrate-insulin ratio is 300/45 = 6.6. This means that the child needs one Insulin unit for every 6.6-gram carbohydrate. For a meal that contains 120 gm of carbohydrates, the child needs 18 insulin units to maintain the blood glucose levels within the normal range[38]. The insulin pump can deliver various forms of insulin bolus. There are three main types of bolus insulin; the typical bolus, the square-wave bolus, and the dual-wave bolus (Figure 5)[39]. In the typical bolus, the pump delivers the insulin immediately on top of the basal rate for three minutes. The extended bolus delivers the insulin over a longer period than the typical bolus (the insulin dose is not delivered at once). The square wave bolus is an extended bolus that delivers the insulin over a fixed extended duration (2-4 h)[40]. We usually need it when the food is ingested over a longer time, such as during social events, or delayed digestion, such as in gastroparesis. The dual-wave bolus delivers the insulin in two or more waves (dual or multi-waves], 30%-70% of the insulin bolus is delivered as the typical bolus, and the rest of the bolus is delivered over a predetermined fixed duration, such as 2-4 h(biphasic, dual, or multi-wave). The dual/multi-wave bolus is helpful with meals with high protein or fat content (e.g., pizza, pasta, cheese, or fish) as protein and fat usually take longer to increase blood glucose levels than carbohydrates, which immediately affect blood glucose[41].
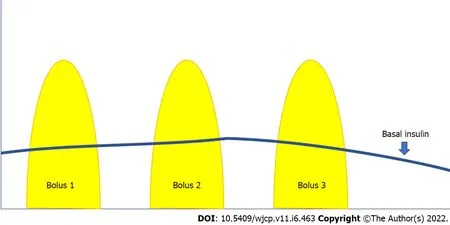
Figure 3 Basal and bolus insulin. Basal insulin is delivered continuously in a small amount as a background to keep the blood glucose levels within the target between meals. The pump can be programmed to deliver at different rates within 24 h. Bolus insulin is a large amount delivered over a short period, which can be given at any time. The pre-meal bolus is given based on the number of carbohydrates in grams. The bolus can also be given to correct high blood glucose levels.

Figure 4 Circadian changes in the basal insulin profile. An example of the circadian changes in the basal insulin profile. Between 12 midnight to 4:0 am,the basal rate is reduced by 20% to increase 20% between 4:0 am to 7:0 am, then will be 100% between 7:0 am to 10:0 am to be reduced by 10% between 10:0 am to 10:0 pm, then it increases again by 10% between 10:0 pm to 12 midnight.
In the super bolus (Figure 6), the pump delivers the basal insulin for the next 1-4 h is added to the bolus, followed by temporarily suspending the basal insulin delivery for those hours (basal rate is 0% for the next 1-4 h) without stopping the pump. This super bolus is needed with a diet high in carbohydrates and low in protein and fat, such as white toast, jam, white rice, sugary drinks, jelly sweets, etc. However, if the post-meal blood sugar persists to be high after a super-bolus insulin dose,we should revise the insulin: carbohydrate ratio. If the post-meal blood sugar fluctuates, we should revise carbohydrate counting as it often shows a wide range of variations[42]. A comparison between the different types of insulin boluses is shown in Table 1.
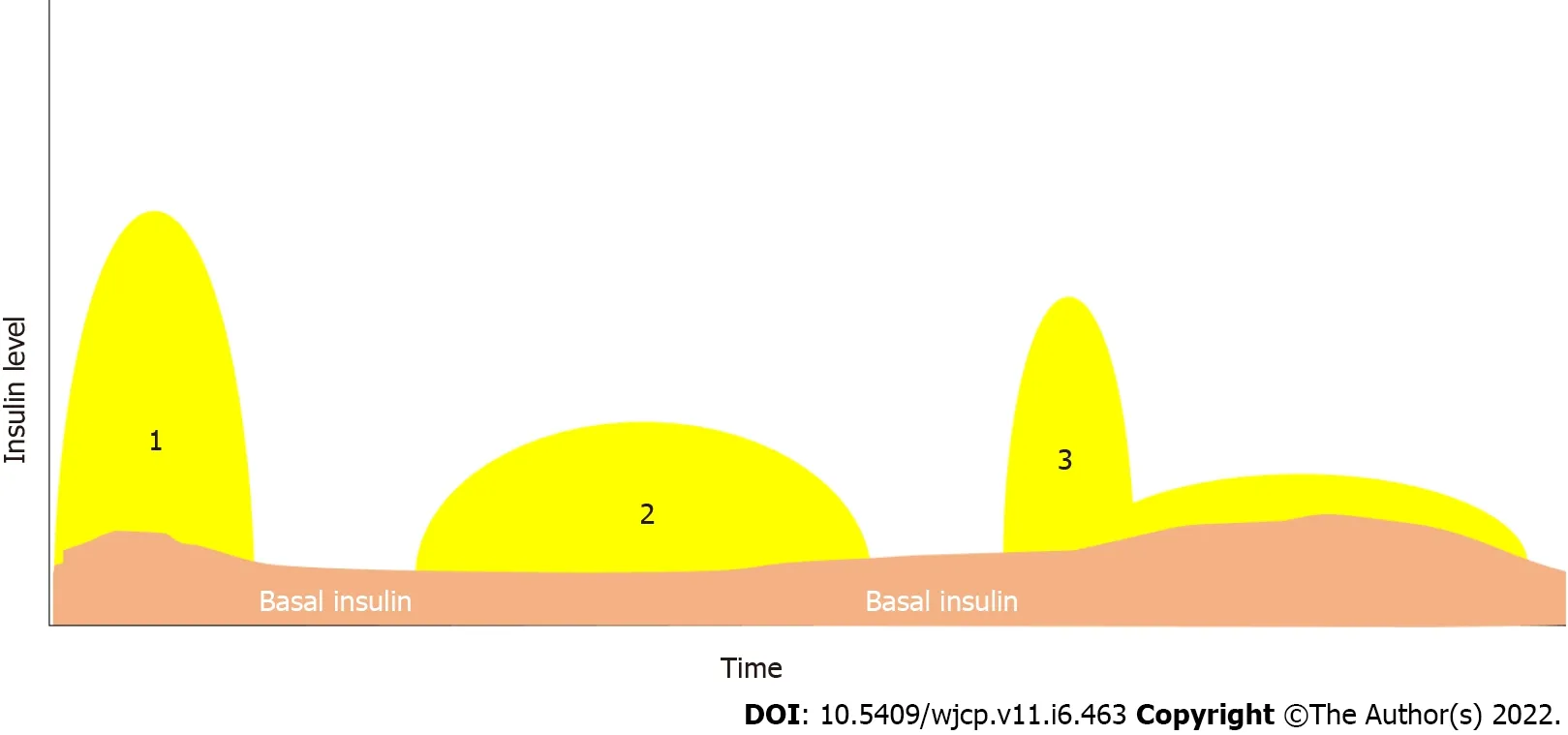
Figure 5 The different insulin bolus types. 1: The typical bolus, 2: The extended bolus, 3: The dual bolus

Figure 6 Different types of insulin bolus. 1: Typical insulin bolus, 2 and 3 super bolus equal to the calculated bolus plus the basal insulin for the coming one to four hours, 4: The basal insulin rate will be 0% for the remaining four hours.

Table 1 Comparison between the different types of insulin boluses
Correction bolus is the number of insulin units delivered by the pump when the blood glucose level is above the target range. It depends on the individual insulin sensitivity factor (ISF), which is the amount of decrease in blood glucose level for every one unit of rapid insulin. It calculates the correction bolus dose, which is the number of insulin units the patient needs to bring the blood glucose into the target range without inducing hypoglycemia[43]. To calculate ISF, we divide 100 by the average total daily insulin dosage over three or four days (TDD) to get the result in mmol/L (100 Rule) or divide 1800 by the average TDD to get the results in mg/dL (1800 Rule). So, when the average TDD is 75 Insulin Units, ISF will be 1.33. Thus, one unit of rapid-acting insulin would reduce the blood sugar by 1.33 mmol/L (24 mg/dL) across the next 2-4 h[43]. The following formula can calculate the correction dose:[(Current Blood Glucose - Target Blood Glucose)/ISF]. However, the Association of British Clinical Diabetologists advises routinely starting with the rule of 130 rather than the 100 rule [ISF = 130/TDD] to achieve the optimal ISF and estimate how much one unit of insulin will decrease the blood glucose level in mmol/L[44]. We should ensure the adequacy of ISF by testing the blood glucose after 4-5 h after the last insulin bolus dose. Carbohydrate was consumed more than three hours ago, and the patient can wait for 4-5 h until the next meal[43].
The caregivers and their child should adequately adjust the pump setting for the IOB and the active insulin time, which is the duration that an insulin dose continues to work after its delivery. Most pumps set this time to be four hours; however, it can be shortened or prolonged in the presence of hypo/hyperglycemia[26]. With short active insulin time, the pump includes the effects of the more recent insulin doses, omitting the impact of the insulin from the previous doses, thus increasing the risk of hypoglycemia[28]. On the other hand, long active insulin time causes overestimation of the insulin on board, and the pump gives smaller boluses which can cause hyperglycemia. Longer active insulin time than four hours is needed in cases with impaired renal functions, as the kidneys clear about 80% of the insulin. Those needing TDD less than or equal to 40 Units/day should reduce active insulin time. In comparison, those receiving a bolus dose of more than 10 Units or TDD of 60 Units/d or more should consider increasing active insulin time[45].
The caregivers and their child should recognize the accepted target blood glucose level, which is individualized according to the child's status and is comfortable with it. Some insulin pumps correct the blood glucose level to a single target level but give the correction bolus when a predefined threshold is reached[46]. Other pumps correct to a higher figure in a predefined target range, while others correct to the mid-target range. The target range usually lies between 4.5-5.5 mmol/L (80-100 mg/dL) (± one mmol/L). However, the target level is modified according to the presence of different factors. Those with high HbA1c need a higher target as the setpoint for hypoglycemic symptoms is higher than for more well-regulated patients with diabetes. They frequently have episodes of pseudohypoglycemia until they are used to lower glucose values[47]. Those with HbA1c > 10% should start with high target blood glucose between 9-10 mmol/L (160-180 mg/dL), then reduce the target level monthly until we reach the normal target blood glucose levels. This gradual decrease of the target is particularly indicated in the presence of diabetic retinopathy, which may deteriorate with the rapid lowering of blood glucose levels. To maintain the target glucose blood level, the caregivers and the children need to frequently test the blood glucose levels, especially in the presence of hypo/hyperglycemia, and to know which insulin doses need to be modified, the basal rate, or the bolus insulin[48].
When there is blood glucose variation (hypo/hyperglycemia) during the night, before breakfast, or when a meal is skipped or delayed, the basal rate of insulin needs to be adjusted. However, the insulinto-carbohydrate ratio and ISF should be revised when the blood glucose variation (hypo/hyperglycemia) occurs within four hours of the bolus or meal or after giving a correction insulin bolus. To test the basal rate, we should eliminate the influence of other factors that could affect it by dividing the day into windows, testing the basal rate for each window on different days, and ensuring that the tested person follows his/her usual routine without strenuous activity before the test by 24 h and during the test period[49,50]. Hypoglycemia should not present during the last 12 h before testing, and the patients should be fasting for the tested period except for water. We use the standard basal rate during testing,stop testing with hypoglycemia (< 4 mmol/L or 72 mg/dL), and give a corrective bolus with hyperglycemia of more than 14 mmol/L (252 mg/dL). We should record blood glucose levels, basal rate, and carbohydrate intake. There are four main periods to test the basal rate: Morning testing from 7:00 am to 12:00 noon, after noon testing from 12:00 noon to 18:00, evening basal from 18:00 to 22:00, and overnight testing from 21:00 to 7:00 am[51]. Overnight testing is usually done first, followed by the other periods, each on different daily bases. First, we correct hypoglycemia; then, we correct hyperglycemia with a 10%-20% decrease or increase, i.e., 0.025-0.05 unit/ hour one to hours before the expected change,to keep the blood glucose variation less than 1.5 mmol/L (28 mg/dL)[52].
For bolus adjustment, we try to keep the two-hours post-meals to be 1.6-3.2 mmol/L (29-58 mg/dL)higher than the pre-meal blood glucose levels. If the two-hours post-meal blood glucose level increases to less than 1.6 mmol/L (29 mg/dL), decrease the total bolus by 10%-20%. If the two-hour post-meal blood glucose level increases to more than 3.2 mmol/L (58 mg/dL), increase the total bolus by 10%-20%.Slattery et al[53] suggested that insulin administration 15-20 min before the meal will provide optimum postprandial glucose control. To adjust the correction bolus dose, adjust the insulin sensitivity factor by a 10%-20% increase or decrease to make the two-hours post-meal blood glucose level halfway to the target and reach the target by four-hours post-meal. If the patient uses continuous glucose monitoring(CGM), a retrospective analysis of the time associated with blood sugar fluctuations can help modify the basal rate[54]. Some pumps have a wizard to change the basal rate according to the blood sugar levels.However, CGM should be associated with an event diary to document the meal timing and the carbohydrate intake for accurate assessment. CGM is indicated with frequent or severe hypoglycemia,hypoglycemia unawareness such as in young children, suboptimal glycemic control, or monitoring of young children or beloved ones by family members or friends[55,56].
Suppose the patient needs to change the insulin pump therapy to subcutaneous insulin for any reason. In that case, we need to calculate the total daily basal insulin given by the pump and increase it by 20% for the first few days and by 30% in the following days to calculate how much long-acting basal subcutaneous insulin is needed. This dose can be administered as a single or divided dose depending on the type of long-acting insulin used[57,58]. The bolus pre-meal insulin and the corrective insulin doses are given as usual. The pump should continue working for two hours after starting the first long-acting insulin dose. Doing this shifting in the morning is recommended to avoid troubleshooting at night[59].Alternatively, if we need to resume the pump therapy after subcutaneous therapy, we resume it two hours before the next long-acting insulin dose. Again, we need to reprogram the pump setting and temporarily reduce the basal insulin rate by about 30% for the next 24 h. Blood glucose levels should be checked one to two hours after starting pump therapy[18]. So this shift is better to be in the morning for easy monitoring. Suppose we want to shift the insulin therapy from continuous intravenous infusion to pump therapy. In that case, we can shift without waiting for the coming meal and discontinue the intravenous insulin infusion only 60 min after starting the pump therapy[60].
PUMP THERAPY lN SPEClAL SlTUATlONS
Sports and exercise
Exercise has a long-term beneficial effect on blood glucose regulation regardless of the type of exercise.However, it has a short-term modification on the blood glucose level to be considered during the pump therapy—two significant difficulties enface children with type I diabetes who are willing to exercise regularly. The first problem is controlling the blood glucose level, and the second is the possible occurrence of hypoglycemia during or following exercise[61]. Aerobic exercise reduces blood glucose levels and enhances insulin sensitivity for 16 h following the exercise. On the other side, high-intensity aerobic exercise or that associated with high adrenaline could cause hyperglycemia. Resistance training or anaerobic exercise increases blood glucose levels and insulin resistance, which persist 6-8 h after exercise. Brief periods of anaerobic exercise activity (e.g., short sprints or weight lifting) during moderate-intensity aerobic exercise may decrease the risk of hypoglycemia[62]. However, all types of physical exercises may increase the risk of nighttime and even the next day hypoglycemia, mainly when performed in the afternoon, independent of sex[63].
We can prevent the development of exercise-induced hypoglycemia by reducing the bolus or basal insulin, increasing carbohydrate intake, or adjusting the exercise regimen. The basal insulin can temporarily be reduced one to two hours before and throughout the exercise. The degree of basal rate reduction depends on the intensity of exercise, 30% in low-intensity, 50% in moderate-intensity, and up to 100% reduction in high-intensity exercise. If modification of the basal insulin is not feasible, a fastacting carbohydrate (15-20 gm without bolus insulin dose) can be given immediately before the short,intense exercise. For more extended, moderately intense exercise, a solid snack with slow-release carbohydrates can be given. If an exercise is planned within two hours after a meal, the premeal-bolus insulin dose can be reduced by 25%-75% according to the exercise intensity[64]. If we are anticipating anaerobic exercise-induced hyperglycemia, we can give a 50% extra bolus dose 30-60 min before the exercise to antagonize the expected increase in the blood sugar. Alternatively, we can increase the basal rate by 10%-20%, 30-90 min before the exercise, and continue at this rate when post-exercise hypoglycemia persists. In the case of combined aerobic and anaerobic exercise, hypoglycemia is more frequent but less than pure aerobic exercise. Hypoglycemia can be prevented with a reduction of basal insulin by up to 50%. If these changes are impossible, we should consider the artificial pancreas. The artificial pancreas system appeared to get efficient and secure control of blood glucose levels during exercise and four hours later[65].
Troubleshooting hypoglycemia
If severe hypoglycemia is present, the patient should not stop the pump but keep it running and check blood glucose levels. When confirmed, the patient is advised to take 15 gm of fast-acting carbohydrates and to recheck blood glucose after 10-15 min. If hypoglycemia persists, another dose of fast-acting carbohydrates is given, and the basal insulin could be temporarily reduced by 10%-20%. As the insulin type used in pump therapy is short-acting, long-acting carbohydrate is not a valid option to treat hypoglycemia with pump therapy. Patients with type I DM on pump therapy should be well trained to recognize and manage the episodes of hypoglycemia they may encounter. The patients should not rely on the hypoglycemia symptoms. Pseudohypoglycemia may occur in patients with diabetes with the typical symptoms of hypoglycemia with blood glucose levels of more than 3.9 mmol/L (70 mg/dL)[66].
Disabling hypoglycemia occurs when repeated episodes of hypoglycemia result in persistent anxiety and impaired quality of life. It usually occurs with tight DM control and with an increasing duration of diabetes. Severe hypoglycemia is that associated with the patient's inability to self-treat with marked impairment of cognitive functions, contrary to non-severe hypoglycemia in which the patient can selftreat and mild cognitive function impairment. Therefore, all children and adolescents with type I DM should have annual screening for impaired hypoglycemia awareness using a valid screening tool such as Gold Score or Clarke Score[67]. These tools can identify the increased risk of severe hypoglycemic events. CGM can detect when more than 10% of the reading is less than four mmol/L (72 mg/dL) or when there are more than three readings with less than three mmol/L (54 mg/dL) per week, which increases the risk of severe hypoglycemic events[68]. It is crucial to investigate the underlying cause of disabling hypoglycemia, such as cortisol, a Growth Hormone, Coeliac disease, insulin Antibodies, etc. If no reason is detected, we should start an intensive education program for the family and the child. Then we can update the pump to sensor augment pump {SAP} without low glucose suspend (LGS). If not improved, we can shift to SAP with LGS. Islet cell or pancreas transplant could be the last option[69].The child should be reassessed every 3-6 mo.
Sick child
Children with diabetes and adequate metabolic control should not encounter more infections or illnesses than children without diabetes. However, when a child with type I DM gets sick, we should rule out the presence of uncontrolled or symptomatic hyperglycemia, ketoacidosis, dehydration, and hypoglycemia[70]. The most crucial point to be emphasized is never to stop insulin; it is a prevalent mistake that leads to the development of ketoacidosis. When a child with diabetes has vomiting, we should consider insulin deficiency till proven otherwise. Consequently, the insulin dose may need to be increased or decreased according to the blood glucose level and the presence or absence of ketosis. The blood glucose should be monitored more frequently, at least every 3-4 h, particularly during the night and occasionally every 1-2 h. we also need to monitor for ketosis[70]. We should not depend on urinary ketones' presence to diagnose ketoacidosis as there is a long time lag between the pump stoppage and appearance of the ketone bodies in the urine and the lack of association between the ketones in the urine and the ketones in the blood. Blood beta-hydroxybutyrate monitoring is beneficial in too young children or when urine collection is hard to get[71].
In the presence of hyperglycemia, we need to check for ketosis. If the urine ketones are absent or small or the blood ketones are less than 0.6 mmol/L (11 mg/dL), we give a pump correction bolus by drinking extra low-carbohydrate fluids and hourly checking of the blood glucose. If the blood glucose starts to decrease, then continue monitoring and accordingly decide to give another bolus dose or not. If the blood glucose fails to decrease after one hour from the corrective dose, then we supplement with a syringe or pen injection. Suppose the urine ketones are moderately or severely increased, or the blood ketones are equal to or more than 0.6 mmol/L (11 mg/dL). In that case, we should check for a pump delivery failure or a significant medical problem, e.g., severe infection. Accordingly, we can shift to insulin therapy by pen or syringe according to the severity of hyperglycemia and degree of ketonuria/ketonemia[70]. The pump should be checked for mechanical or catheter difficulties by replacing the insulin in the pump, the infusion set, and the cannula while continuing to give bolus doses with a pen or syringe until the hyperglycemia is controlled. Then, we must resume the pump therapy with a temporary basal rate of 120%, hourly blood glucose monitoring, and extra low-carbohydrate diet fluids[72].
If the child exhibits signs of diabetic ketoacidosis (DKA), the pump therapy should be discontinued due to the altered tissue perfusion in DKA, which impairs insulin absorption and affects the reliability of the pump therapy. The pump should be temporarily discontinued; the cannula should be removed,then follow the standard protocol to manage DKA. Once DKA is fixed, pump therapy is resumed at the patient's standard basal rate, but the patient should maintain intravenous insulin infusion till he receives a meal bolus[73]. Wang et al[74] showed that using nano-insulin pumps in children with DKA can quickly correct children's blood glucose and ketone body levels. If there is ketosis with low blood glucose, the child should drink extra high-carbohydrate fluids with continuous blood glucose monitoring. In case of persistent vomiting or failure of the previous attempt to control the disorder, the child should be hospitalized[75].
Insulin pump use in a hospitalized child
When hospitalized with a severe medical condition, children with type I DM need aggressive management of diabetes. Adequate and meticulous control of diabetes is associated with significant morbidity and mortality improvement in children and adults with diabetes[76]. However, intensive insulin therapy is associated with an increased hypoglycemia rate and complications without a significant mortality reduction. Therefore, continuous monitoring of the blood glucose level is crucial to prevent hypo/hyperglycemia[77]. Non-critically ill children hospitalized for elective and non-acute hospitalizations who can operate their insulin pumps are allowed to continue using them. Fasting prior to elective surgical procedure is allowed with proper adjustment of the basal insulin rate to prevent the development of hypoglycemia. However, if the children cannot operate their pump, they can transition to the basal-bolus regimen[78]. If the child is expected to go into a minor procedure with general anesthesia for less than two hours and is expected to eat or drink within 2-3 h, check the blood glucose levels hourly and adjust the insulin pump accordingly (Figure 7)[79].

Figure 7 A flow chart for a minor procedure with general anesthesia for less than two hours.
It is acceptable that hospitalized patients continue to self-control their DM using an insulin pump except if they are unconscious, confused, or have severe pain, undergo major surgery or procedure under general anesthesia lasting more than two hours, or develop DKA. However, if children are hospitalized due to a critically ill condition or surgery that needs anesthesia for more than two hours and will miss more than one meal, they need to shift to intravenous insulin therapy. The patients should remove the insulin pump and keep it safe to be resumed once the procedure finishes unless being critically ill. Frequent blood glucose monitoring (or CGM) offers safe insulin delivery control[80]. Care should be taken while doing specific procedures in the hospital to avoid damage to the insulin pump.The insulin pump should be covered by a lead apron while doing an X-ray, computerized tomography scan, cardiac catheterization, or insertion of a pacemaker/automatic implantable defibrillator.Ultrasonography can be done when needed, but the operator should avoid direct pointing the transducer to the pump. On the other hand, the pump should be removed while doing magnetic resonance imaging. Upper or lower gastrointestinal endoscopies do not require the removal of the pump[81].
Use of corticosteroid with pump therapy
As DM type I is an autoimmune disease, it is frequently associated with other autoimmune disorders,such as autoimmune thyroid disease[82]. Corticosteroids are frequently used in high doses to treat these autoimmune disorders such as asthma and inflammatory bowel diseases. Steroids usually increase insulin resistance, insulin requirement, and the risk of hyperglycemia. Hyperglycemia is predicted to occur approximately four to eight hours following oral steroids administration and sooner following intravenous steroids[83]. On the contrary, blood glucose levels may return to pre-steroid levels 24 h following intravenous steroids discontinuation. If oral steroids are withdrawn gradually over many weeks, glucose levels may decrease dose-dependently[84,85].
Interestingly, the daily timing of steroid-induced hyperglycemia depends on the type of steroid use.For example, prednisolone, usually given in the morning, induces hyperglycemia in the late morning and persists into the evening with a gradual fall of blood glucose back overnight, often reaching baseline levels the following morning[86]. Therefore, children on pump therapy need to increase the basal insulin rate to 130%-150% during the expected times of maximal hyperglycemia. However, we may occasionally need to increase the basal insulin rate to 200%-300% of the standard rate. Other management options are adjusting ICR or giving corrective insulin bolus when needed. Frequent blood glucose monitoring every 4 h should be done. Once steroid therapy is reduced or stopped, the insulin requirement can be decreased back to pre-steroid levels; therefore, readjusting insulin rates may be needed[87].
Improving insulin absorption at the insertion sites
Warming the injection site increases the blood flow, increasing the subcutaneous insulin absorption rate.Warming can be done by massaging or using special warming devices, which is particularly helpful in managing postprandial hyperglycemia[88,89]. Local application of recombinant human hyaluronidase increases the subcutaneous insulin dispersion and absorption rate at the injection site, conferring both ultrafast insulin absorption and action[90]. Using silicon microneedles integrated within the insulin pump trans-dermally delivers insulin efficiently, safely, and painlessly. It also helps decrease the insulin pump size[91].
Insulin pump and school days
School life occupies an integral part of children's daily life. Consequently, children using an insulin pump should be able to manage it and have a good education about the proper use of the pump and the management of different problems that they may enface. This awareness is crucial for young children who may need continuous supervision of the pump data and settings, especially for carbohydrate intake, blood glucose monitoring, and insulin administration. The responsible teachers or the school healthcare worker should be well trained in the different scenarios the child using an insulin pump may encounter to allow rapid interference when needed. A clear school health plan to manage students with Type I DM should be available and practiced in recognizing and managing specific acute emergencies such as hypo/hyperglycemia with/without ketonemia[87].
Puberty in children using an insulin pump
Puberty is associated with increased sex hormone levels which increase the degree of insulin resistance and, consequently, increase the insulin requirement during puberty. Puberty is associated with higher hemoglobin A1c levels and rates of diabetes complications[92]. Adolescence is also associated with an increased risk of alcohol consumption and considerably increases the diabetes risk in young adulthood and makes diabetes control more difficult. Alcohol consumption in the evening increases the risk of hypoglycemia, especially at night and after the next breakfast, which needs frequent blood glucose monitoring, particularly at night and early morning[93,94].
Menstrual cycle in an adolescent female with Type I DM
Menses is associated with high fluctuations of the glycaemic control with an increased risk of hyperglycemia and increased insulin resistance during periovulation and early luteal phases (premenstrual period), possibly due to the rising oestradiol levels that occur before ovulation, which may need a temporary increase in the basal insulin rate[95]. On the contrary, when menses start, the progesterone level begins to drop, causing a sharp decline in the insulin requirement, which may increase the hypoglycemia risk steeply[96]. If the adolescent girl has a disturbed menstrual cycle and needs to use contraceptive pills to regulate the cycle, care should be taken while using them as an increase in the basal insulin requirement may occur, especially with high-dose contraceptive pills or with long-acting progesterone injections[97].
Traveling with an insulin pump
Despite traveling being a welcome retreat from our everyday life difficulties, it is associated with an extraordinary increase in daily activity, which could increase the risk of hypoglycemia and becomes a real challenge in patients with diabetes. It is particularly challenging in the presence of time zone differences > 3 h, significant variations in the basal rates, such as the marked Dawn phenomenon,recurrent or severe episodes of hypoglycemia, or reduced hypoglycemia awareness. The pump basal rate is reduced by 10%-20% during traveling for the first 24 h and gradually changes the pump timing setting to the new local time upon arrival at the destination by 2-3 h each day. This change should be associated with frequent blood glucose monitoring. Disconnecting the pump during take-off and landing is also essential to avoid pressure effects on the pump delivery mechanism[98].
GENERAL CARE FOR CHlLDREN WlTH DM WHO REQUlRE lNSULlN PUMP THERAPY
Skin care and prevention of insertion site infection
Skin changes occur in one-third of patients with diabetes. Children with high glucose levels tend to have dry skin[99]. Therefore, they need adequate blood sugar control and proper skin hydration with specific lotions for diabetes following site change, especially in pump care. Itching is frequent at the insertion site; the child is advised to gently rub and avoid scratching the affected area to avoid skin breakage[100]. The insertion set should be applied to dry, unwet, non-broken skin. The insertion site should be rotated ideally every three days, over 6-10 sites, to long-term preserve skin integrity. Certain areas are advised more than others due to their superior insulin-absorptive capabilities, more comfort, and better convenience. The most common sites suitable for insertion are the abdomen (two-centimetre radius around and away from the navel), upper buttocks, upper thigh (medial and lateral areas, at least 5 cm away from hip or knee joints), upper buttocks (flank), upper arm, and rarely forearm (Figure 8A). The area with the least hair should be chosen as the hair decreases the longevity of the insertion site. Every site should take at least one week for recovery and should be away from the next site by at least one to two inches. Different patterns of insertion site rotations are demonstrated in Figure 8B[101].

Figure 8 Approved insertion sites and different types of insertion site rotation. A: There are four approved sites for the subcutaneous injection of insulin: Insulin Absorption Rate Fluctuation Depending on Injection Site; B: shows different types of insertion site rotation. Note that all the rotation patterns keep away from the umbilicus by at least one inch.
Vaccination
Patients with DM, especially those requiring insulin pump therapy, need intense vaccination programs.They should receive an annual flu vaccination. They also should consider having Streptococcus pneumoniae vaccines, and the coronavirus disease 2019 (COVID-19) vaccination is strongly recommended[102].
The use of insulin pumps in special situations such as traveling, swimming, bathing, imaging, and other procedures is summarized in Table 2.

Table 2 Special situations with insulin pumps
CT: Computed tomography; MDT: Multidose therapy; MRI: Magnetic resonance imaging.
ADVANTAGES OF lNSULlN PUMP THERAPY
The insulin pump provides fewer needle injections as there is no need to inject insulin every time needed. It also can provide small insulin doses down to ten times less (0.05-0.1 Units) than an insulin pen or syringe, which is particularly useful in insulin-sensitive young children. Meanwhile, the insulin pump provides a convenient and more flexible way to modify the needed insulin more physiologically,relatively similar to the human pancreas[103]. Hence basal insulin can be programmed to match the person's activity, the changing daily requirement, hormonal changes, pubertal spurts, stress, illness,traveling, and any other situations. At the same time, insulin bolus can be delivered in different ways considering various conditions such as gastroparesis, malabsorption, or even to match the ingested foods. On the other hand, insulin delivery can be temporarily reduced or suspended in certain situations, such as hypoglycemia[32].
This incredible flexibility in the insulin delivery system and the marked less in blood glucose fluctuations allow a better quality of life. Using rapid-acting insulin delivered in a low volume tailored to the individual needs allows the insulin pump to overcome the variation in insulin absorption that is usually observed with long-acting insulin, resulting in more consistent and reliable insulin absorption and consequently less fluctuation of both insulin profile and blood glucose level[104]. This feature also helps to decrease the need for snacks, especially before exercise, consequently decreasing the rate of weight gain[105]. However, Boucher-Berry et al[106] found that lower bolus to basal insulin ratios increases the risk of excess weight gain. Hence, proper bolus and basal insulin dose adjustments are mandatory during insulin therapy. Pump therapy also improves the patient experience and satisfaction due to technology motivation and improved self-management. Pumps can also integrate easily with the new technology, so they can link easily with blood glucose measuring technology, bolus advisors, and wizards for diabetes management, forming a closed-loop system similar to an artificial pancreas which significantly improves the patient's quality of life[107].
DlSADVANTAGES OF lNSULlN PUMP THERAPY
There are some disadvantages to insulin pump therapy that may limit its use. Being worn all the time(24 h a day/7 days a week), even during sleep, showering, and sports, with continuous reminders of being diabetic, can influence body image and self-confidence. Luckily, numerous accessories are accessible to make wearing the pump hidden and convenient[108]. Because insulin pumps use only rapid-acting insulin without a long-acting insulin depot, there is a high risk of rapid development of DKA with technical failure or interruption of insulin flow such as air in the tubing, a damaged infusion set, or infection at the insertion site. Therefore, the patient should monitor blood glucose levels more frequently, at least four times daily, and a specialized well-trained interdisciplinary care team should be accessible in case of emergency. The pump also should not be disconnected for a long time (short-actinginsulin). This limitation could affect the child's daily activities, such as swimming. However, many pump types are waterproof and fit for swimming[109].
Insulin pump setup occasionally is complicated and difficult to proceed with compared to pen or syringe use. Therefore, adequate training and education are mandatory for both the child and the caregiver. It also needs a high level of motivation, understanding, and education to achieve the best benefit of the pump and avoid complications. In addition, the insertion set, including the infusion set and cannula, requires to be replaced every 2-3 d. In addition, the infusion set may be prone to incorrect priming, air bubbles, tubing breakdown, and kinking or slippage of the cannula, which can interrupt insulin delivery[110].
Infection of the insertion site occurs in 17% of patients on insulin pumps over a period of three years,especially when the infusion set is left for longer than it should[111]. Risk factors for insertion site infections include large insulin doses, poor patient selection, inadequate patient education, lack of hygienic measures, infrequent changes of the infusion set as requested by the manufacturer, and incorrect cannula insertion[112]. Staphylococcal or streptococcal bacterial infections are the most common infection at the insertion site, followed by Rhizomucor pusillus fungal cellulitis[113].Occasionally the infection may progress to cellulitis or collect into an abscess requiring surgical drainage. Primary tuberculous infection of the insulin injection site is rare but reported complications of insulin therapy[114]. Changing the insertion set should be done according to the manufacturer's guidelines or pump educator to diminish the chance of infection. It is also imperative that the patient follow proper hygienic measures, especially washing the hands and periodically changing the site to decrease infection chances. The cost of the pump is not only limited to the device but also running costs for accessories, cartridge syringes, batteries, skin preparation items, cannulas, and infusion sets, which are significantly higher than the regular insulin pens and syringes. Because insulin is a lifesaving essential medicine, every effort should be made to minimize the cost to the patient and his family[115].
DlSCONTlNUATlON OF lNSULlN PUMP THERAPY
About 3% of the pump user discontinue pump therapy within one year. The most frequent causes,according to Wong et al[116], include difficulties in pump insertion/adhesive (60%), interference with sports activities (42%), discomfort with wearing the pump (38%), interference with intimacy (34%),pump dysfunction (28%), and problematic hyperglycemia (28%). Beato-Víbora et al[117] 2015 showed that pump therapy improves glycaemic control and hypoglycemia awareness, decreases hypoglycemia frequency, and can be sustained for many years. However, 5% of the users discontinued the pump therapy due to a lack of clinical advantage, technical problems, safety issues, or user choice.
The pump therapy should be discontinued for recurrent DKA as it affects the local absorption of insulin due to altered tissue perfusion. It should also be discontinued when there is a pump failure or mismanagement, inadequate blood glucose monitoring (less than four times/day), recurrent injection site infection, intentional overdosing, failure to meet the objective of pump therapy, or with the parents'or the child's wishes. Pump therapy should be discontinued if the patient becomes unconscious,confused, and unable to self-management, such as severe pain or illness. It should also be discontinued if the patient goes for major surgery with general anesthesia for more than two hours[118]. Limitation of the study: some of the included articles were in favor of using insulin pumps which may carry the risk of bias. However, we tried to include most of the available studies to minimize the risk of bias.
CONCLUSlON
The insulin pump is a giant breakthrough in DM management, especially in the pediatric age. The insulin pump provides fewer needles and can provide very tiny insulin doses. It provides a convenient and more flexible way to modify the needed insulin physiologically, like the human pancreas. It can offer adequate and optimal glycemic control to reduce the risk of metabolic derangements in different tissues. However, there are some disadvantages to insulin pump therapy that do not necessarily prevent its use. It should be discontinued with recurrent diabetic ketoacidosis.
ARTlCLE HlGHLlGHTS

ACKNOWLEDGEMENTS
We thank the anonymous referees for their valuable suggestions.
FOOTNOTES
Author contributions: Al-Biltagi M, Saeed NK, Bediwy AS, and Elbeltagi R collected the data and wrote and revised the manuscript.
Conflict-of-interest statement: All authors declare no conflict of interest.
PRlSMA 2009 Checklist statement: The authors have read the PRISMA 2009 Checklist, and the manuscript was prepared and revised according to the PRISMA 2009 Checklist.
Open-Access: This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin: Bahrain
ORClD number: Mohammed Al-Beltagi 0000-0002-7761-9536; Nermin Kamal Saeed 0000-0001-7875-8207; Adel Salah Bediwy 0000-0002-0281-0010.
S-Editor: Liu JH
L-Editor: A
P-Editor: Liu JH
